
Procedure-Related Differences and Clinical Outcomes in Patients Treated with Percutaneous Coronary Intervention Assisted by Optical Coherence Tomography between New and Earlier Generation Software (Ultreon™ 1.0 Software vs. AptiVue™ Software)

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
2.1. Patients
2.2. Optical Coherence Tomography—Image Attainment and Processing
2.3. Minimal Mean Stent Expansion
2.4. Study Endpoints
2.5. Statistical Analysis
3. Results
3.1. General Characteristics and Concomitant Disease at Baseline (Before Index Procedure)
3.2. Biochemical Indices at Baseline (Before Index Procedure)
3.3. Procedural Indices (Index Procedure)
3.4. OCT Parameters (Index Procedure)
3.5. Pharmacotherapy (After Index Procedure)
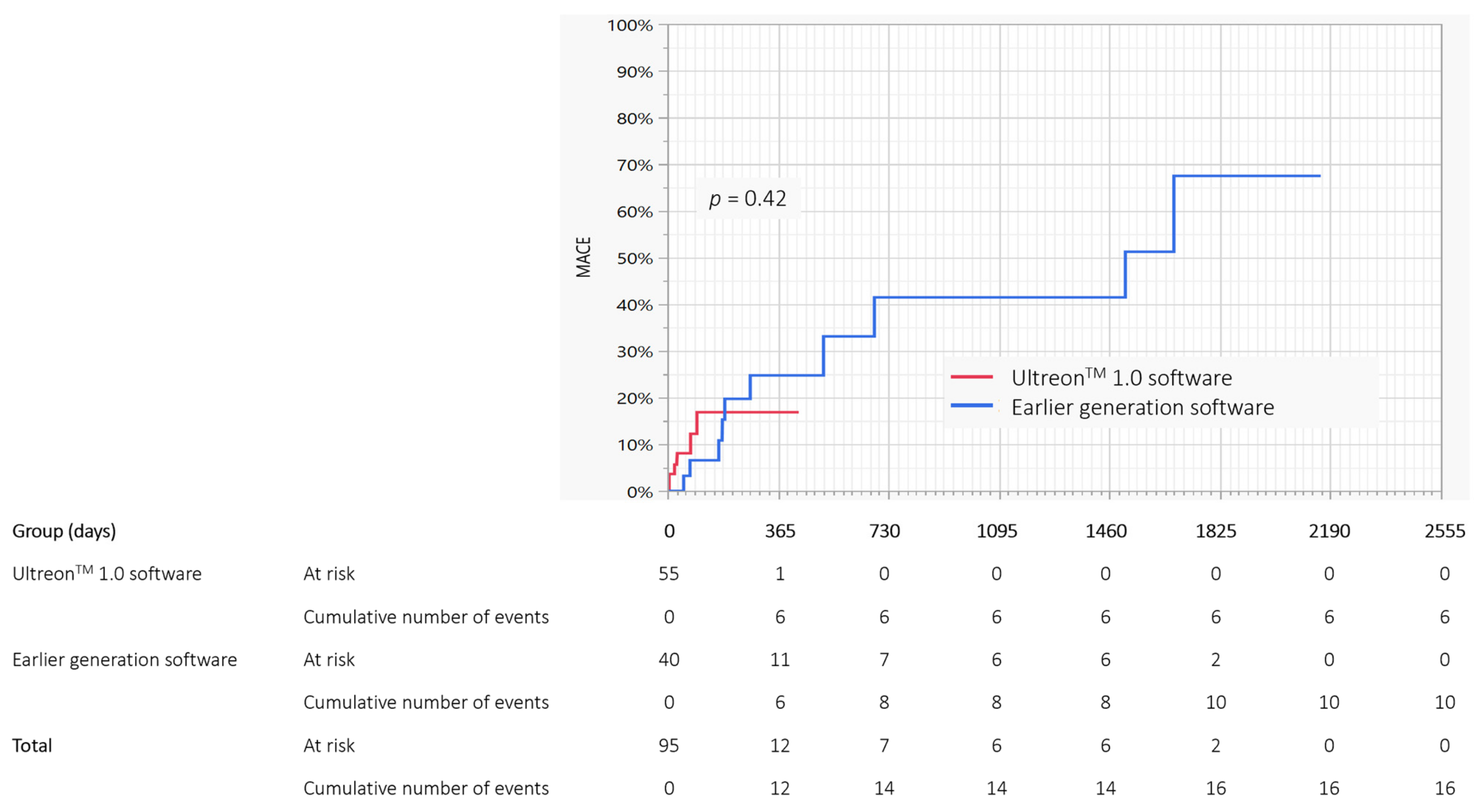
3.6. Clinical Outcomes
3.7. Predictors of Stent Expansion—Univariable Analysis
3.8. Predictors of Stent Expansion—Multivariable Analysis
4. Discussion
4.1. Predictors of Stent Expansion
4.2. Follow-Up
4.3. Issues Related to the Procedure and Stent Expansion
5. Conclusions
6. Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Prati, F.; Di Vito, L.; Biondi-Zoccai, G.; Occhipinti, M.; La Manna, A.; Tamburino, C.; Burzotta, F.; Trani, C.; Porto, I.; Ramazzotti, V.; et al. Angiography alone versus angiography plus optical coherence tomography to guide decision-making during percutaneous coronary intervention: The Centro per la Lotta contro l’Infarto-Optimisation of Percutaneous Coronary Intervention (CLI-OPCI) study. EuroIntervention 2012, 8, 823–829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prati, F.; Romagnoli, E.; Burzotta, F.; Limbruno, U.; Gatto, L.; La Manna, A.; Versaci, F.; Marco, V.; Di Vito, L.; Imola, F.; et al. Clinical impact of OCT findings during PCI: The CLI-OPCI II study. JACC Cardiovasc. Imaging 2015, 8, 1297–1305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kubo, T.; Akasaka, T.; Shite, J.; Suzuki, T.; Uemura, S.; Yu, B.; Kozuma, K.; Kitabata, H.; Shinke, T.; Habara, M.; et al. OCT compared with IVUS in a coronary lesion assessment: The OPUS-CLASS study. JACC Cardiovasc. Imaging 2013, 6, 1095–1104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wijns, W.; Shite, J.; Jones, M.R.; Lee, S.W.; Price, M.J.; Fabbiocchi, F.; Barbato, E.; Akasaka, T.; Bezerra, H.; Holmes, D. Optical coherence tomography imaging during percutaneous coronary intervention impacts physician decision-making: ILUMIEN I study. Eur. Heart J. 2015, 36, 3346–3355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maehara, A.; Ben-Yehuda, O.; Ali, Z.; Wijns, W.; Bezerra, H.G.; Shite, J.; Généreux, P.; Nichols, M.; Jenkins, P.; Witzenbichler, B.; et al. Comparison of stent expansion guided by optical coherence tomography versus intravascular ultrasound: The ILUMIEN II study (Observational Study of Optical Coherence Tomography [OCT] in patients undergoing Fractional Flow Reserve [FFR] and percutaneous coronary intervention). JACC Cardiovasc. Interv. 2015, 8, 1704–1714. [Google Scholar] [PubMed] [Green Version]
- Ali, Z.A.; Karimi Galougahi, K.; Maehara, A.; Shlofmitz, R.A.; Fabbiocchi, F.; Guagliumi, G.; Alfonso, F.; Akasaka, T.; Matsumura, M.; Mintz, G.S.; et al. Outcomes of optical coherence tomography compared with intravascular ultrasound and with angiography to guide coronary stent implantation: One-year results from the ILUMIEN III: OPTIMIZE PCI trial. EuroIntervention 2021, 16, 1085–1091. [Google Scholar] [CrossRef]
- Ali, Z.A.; Maehara, A.; Généreux, P.; Shlofmitz, R.A.; Fabbiocchi, F.; Nazif, T.M.; Guagliumi, G.; Meraj, P.M.; Alfonso, F.; Samady, H.; et al. Optical coherence tomography compared with intravascular ultrasound and with angiography to guide coronary stent implantation (ILUMIEN III: OPTIMIZE PCI): A randomised controlled trial. Lancet 2016, 388, 2618–2628. [Google Scholar] [CrossRef]
- Meneveau, N.; Souteyrand, G.; Motreff, P.; Caussin, C.; Amabile, N.; Ohlmann, P.; Morel, O.; Lefrançois, Y.; Descotes-Genon, V.; Silvain, J.; et al. Optical coherence tomography to optimize results of percutaneous coronary intervention in patients with non-ST-elevation acute coronary syndrome: Results of the multicenter, randomized DOCTORS study (Does Optical Coherence Tomography Optimize the Results of Stenting?). Circulation 2016, 134, 906–917. [Google Scholar]
- Collet, J.P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef]
- Neumann, F.J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [PubMed] [Green Version]
- Writing Committee Members; Lawton, J.S.; Tamis-Holland, J.E.; Bangalore, S.; Bates, E.R.; Beckie, T.M.; Bischoff, J.M.; Bittl, J.A.; Cohen, M.G.; DiMaio, J.M.; et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2022, 79, 197–215. [Google Scholar]
- Morris, A.H. Treatment algorithms and protocolized care. Curr. Opin. Crit. Care 2003, 9, 236–240. [Google Scholar] [CrossRef] [PubMed]
- Shlofmitz, E.; Shlofmitz, R.A.; Galougahi, K.K.; Rahim, H.M.; Virmani, R.; Hill, J.M.; Matsumura, M.; Mintz, G.S.; Maehara, A.; Landmesser, U.; et al. Algorithmic Approach for Optical Coherence Tomography-Guided Stent Implantation During Percutaneous Coronary Intervention. Interv. Cardiol. Clin. 2018, 7, 329–344. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, S.S.; Wilk, M.B. An Analysis of Variance Test for Normality (Complete Samples). Biometrika 1965, 52, 591–611. [Google Scholar] [CrossRef]
- Kobayashi, Y.; Okura, H.; Kume, T.; Yamada, R.; Kobayashi, Y.; Fukuhara, K.; Koyama, T.; Nezuo, S.; Neishi, Y.; Hayashida, A.; et al. Impact of target lesion coronary calcification on stent expansion. Circ. J. 2014, 78, 2209–2214. [Google Scholar]
- Fujii, K.; Carlier, S.G.; Mintz, G.S.; Yang, Y.M.; Moussa, I.; Weisz, G.; Dangas, G.; Mehran, R.; Lansky, A.J.; Kreps, E.M.; et al. Stent underexpansion and residual reference segment stenosis are related to stent thrombosis after sirolimus-eluting stent implantation: An intravascular ultrasound study. J. Am. Coll. Cardiol. 2005, 45, 995–998. [Google Scholar] [CrossRef] [Green Version]
- Sonoda, S.; Morino, Y.; Ako, J.; Erashima, M.; Hassan, A.H.; Bonneau, H.N.; Leon, M.B.; Moses, J.W.; Yock, P.G.; Honda, Y.; et al. Impact of final stent dimensions on long-term results following sirolimus-eluting stent implantation: Serial intravascular ultrasound analysis from the sirius trial. J. Am. Coll. Cardiol. 2004, 43, 1959–1963. [Google Scholar] [CrossRef] [Green Version]
- Fujii, K.; Mintz, G.S.; Kobayashi, Y.; Carlier, S.G.; Takebayashi, H.; Yasuda, T.; Moussa, I.; Dangas, G.; Mehran, R.; Lansky, A.J.; et al. Contribution of stent underexpansion to recurrence after sirolimus-eluting stent implantation for in-stent restenosis. Circulation 2004, 109, 1085–1088. [Google Scholar] [CrossRef] [Green Version]
- Fujino, A.; Mintz, G.; Matsumura, M.; Yamamoto, M.H.; Lee, C.; Hoshino, M.; Usui, E.; Kanaji, Y.; Murai, T.; Yonetsu, T.; et al. TCT-28 a new optical coherence tomography-based calcium scoring system to predict stent underexpansion. J. Am. Coll. Cardiol. 2017, 70, B12–B13. [Google Scholar] [CrossRef]
- Karimi Galougahi, K.; Maehara, A.; Mintz, G.S.; Shlofmitz, R.A.; Stone, G.W.; Ali, Z.A. Update on intracoronary optical coherence tomography: A review of current concepts. Curr. Cardiovasc. Imaging. Rep. 2016, 9, 16. [Google Scholar] [CrossRef]
- Barbato, E.; Shlofmitz, E.; Milkas, A.; Shlofmitz, R.; Azzalini, L.; Colombo, A. State of the art: Evolving concepts in the treatment of heavily calcified and undilatable coronary stenoses—From debulking to plaque modification, a 40-year-long journey. EuroIntervention 2017, 13, 696–705. [Google Scholar] [CrossRef] [PubMed]
- Kubo, T.; Shimamura, K.; Ino, Y.; Yamaguchi, T.; Matsuo, Y.; Shiono, Y.; Taruya, A.; Nishiguchi, T.; Shimokado, A.; Teraguchi, I.; et al. Superficial calcium fracture after PCI as assessed by OCT. JACC Cardiovasc. Imaging 2015, 8, 1228–1229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maejima, N.; Hibi, K.; Saka, K.; Akiyama, E.; Konishi, M.; Endo, M.; Iwahashi, N.; Tsukahara, K.; Kosuge, M.; Ebina, T.; et al. Relationship between thickness of calcium on optical coherence tomography and crack formation after balloon dilatation in calcified plaque requiring rotational atherectomy. Circ. J. 2016, 80, 1413–1419. [Google Scholar] [CrossRef] [Green Version]
- Ali, Z.A.; Brinton, T.J.; Hill, J.M.; Maehara, A.; Matsumura, M.; Karimi Galougahi, K.; Illindala, U.; Götberg, M.; Whitbourn, R.; Van Mieghem, N.; et al. Optical coherence tomography characterization of coronary lithoplasty for treatment of calcified lesions: First description. JACC Cardiovasc. Imaging 2017, 10, 897–906. [Google Scholar] [CrossRef]
- Habara, M.; Nasu, K.; Terashima, M.; Kaneda, H.; Yokota, D.; Ko, E.; Ito, T.; Kurita, T.; Tanaka, N.; Kimura, M.; et al. Impact of frequency-domain optical coherence tomography guidance for optimal coronary stent implantation in comparison with intravascular ultrasound guidance. Circ. Cardiovasc. Interv. 2012, 5, 193–201. [Google Scholar] [CrossRef] [Green Version]
- Ali, Z.A.; Karimi Galougahi, K.; Maehara, A.; Shlofmitz, R.A.; Ben-Yehuda, O.; Mintz, G.S.; Stone, G.W. Intracoronary optical coherence tomography 2018: Current status and future directions. JACC Cardiovasc. Interv. 2017, 10, 2473–2487. [Google Scholar] [CrossRef]
- Liu, X.; Doi, H.; Maehara, A.; Mintz, G.S.; de Costa, J.R., Jr.; Sano, K.; Weisz, G.; Dangas, G.D.; Lansky, A.J.; Kreps, E.M.; et al. A volumetric intravascular ultrasound comparison of early drug-eluting stent thrombosis versus restenosis. JACC Cardiovasc. Interv. 2009, 2, 428–434. [Google Scholar] [CrossRef] [Green Version]
- Choi, S.Y.; Witzenbichler, B.; Maehara, A.; Lansky, A.J.; Guagliumi, G.; Brodie, B.; Kellett, M.A., Jr.; Dressler, O.; Parise, H.; Mehran, R.; et al. Intravascular ultrasound findings of early stent thrombosis after primary percutaneous intervention in acute myocardial infarction: A Harmonizing Outcomes with Revascularization and Stents in Acute Myocardial Infarction (HORIZONS-AMI) substudy. Circ. Cardiovasc. Interv. 2011, 4, 239–247. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.; Maehara, A.; Mintz, G.S.; Weissman, N.J.; Yu, A.; Wang, H.; Mandinov, L.; Popma, J.J.; Ellis, S.G.; Grube, E.; et al. An integrated TAXUS IV, V, and VI intravascular ultrasound analysis of the predictors of edge restenosis after bare metal or paclitaxel-eluting stents. Am. J. Cardiol. 2009, 103, 501–506. [Google Scholar] [CrossRef]
- Kang, S.J.; Cho, Y.R.; Park, G.M.; Ahn, J.M.; Kim, W.J.; Lee, J.Y.; Park, D.W.; Lee, S.W.; Kim, Y.H.; Lee, C.W.; et al. Intravascular ultrasound predictors for edge restenosis after newer generation drug-eluting stent implantation. Am. J. Cardiol. 2013, 111, 1408–1414. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, N.; Mintz, G.S.; Witzenbichler, B.; Metzger, D.C.; Rinaldi, M.J.; Duffy, P.L.; Weisz, G.; Stuckey, T.D.; Brodie, B.R.; Parvataneni, R.; et al. Prevalence, features, and prognostic importance of edge dissection after drug-eluting stent implantation: An ADAPT-DES intravascular ultrasound sub-study. Circ. Cardiovasc. Interv. 2016, 9, e003553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calvert, P.A.; Brown, A.J.; Hoole, S.P.; Obaid, D.R.; West, N.E.; Bennett, M.R. Geographical miss is associated with vulnerable plaque and increased major adverse cardiovascular events in patients with myocardial infarction. Catheter. Cardiovasc. Interv. 2016, 88, 340–347. [Google Scholar] [CrossRef] [PubMed]
- Räber, L.; Ueki, Y. Optical coherence tomography vs. intravascular ultrasound-guided percutaneous coronary intervention. J. Thorac. Dis. 2017, 9, 1403–1408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Jaegere, P.; Mudra, H.; Figulla, H.; Almagor, Y.; Doucet, S.; Penn, I.; Colombo, A.; Hamm, C.; Bartorelli, A.; Rothman, M.; et al. Intravascular ultrasound-guided optimized stent deployment. Immediate and 6 months clinical and angiographic results from the Multicenter Ultrasound Stenting in Coronaries Study (MUSIC Study). Eur. Heart J. 1998, 19, 1214–1223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, S.J.; Kim, B.K.; Shin, D.H.; Nam, C.M.; Kim, J.S.; Ko, Y.G.; Choi, D.; Kang, T.S.; Kang, W.C.; Her, A.Y.; et al. Effect of Intravascular Ultrasound-Guided vs. Angiography-Guided Everolimus-Eluting Stent Implantation: The IVUS-XPL Randomized Clinical Trial. JAMA 2015, 314, 2155–2163. [Google Scholar] [CrossRef]
- Guo, N.; Maehara, A.; Mintz, G.S.; He, Y.; Xu, K.; Wu, X.; Lansky, A.J.; Witzenbichler, B.; Guagliumi, G.; Brodie, B.; et al. Incidence, mechanisms, predictors, and clinical impact of acute and late stent malapposition after primary intervention in patients with acute myocardial infarction: An intravascular ultrasound sub-study of the Harmonizing Outcomes with Revascularization and Stents in Acute Myocardial Infarction (HORIZONS-AMI) trial. Circulation 2010, 122, 1077–1084. [Google Scholar]
- Steinberg, D.H.; Mintz, G.S.; Mandinov, L.; Yu, A.; Ellis, S.G.; Grube, E.; Dawkins, K.D.; Ormiston, J.; Turco, M.A.; Stone, G.W.; et al. Long-term impact of routinely detected early and late incomplete stent apposition: An integrated intravascular ultrasound analysis of the TAXUS IV, V, and VI and TAXUS ATLAS workhorse, long lesion, and direct stent studies. JACC Cardiovasc. Interv. 2010, 3, 486–494. [Google Scholar] [CrossRef] [Green Version]
- Souteyrand, G.; Amabile, N.; Mangin, L.; Chabin, X.; Meneveau, N.; Cayla, G.; Vanzetto, G.; Barnay, P.; Trouillet, C.; Rioufol, G.; et al. Mechanisms of stent thrombosis analysed by optical coherence tomography: Insights from the national PESTO French registry. Eur. Heart J. 2016, 37, 1208–1216. [Google Scholar] [CrossRef] [Green Version]
- Adriaenssens, T.; Joner, M.; Godschalk, T.C.; Malik, N.; Alfonso, F.; Xhepa, E.; De Cock, D.; Komukai, K.; Tada, T.; Cuesta, J.; et al. Optical coherence tomography findings in patients with coronary stent thrombosis: A report of the PRESTIGE consortium (Prevention of Late Stent Thrombosis by an Interdisciplinary Global European Effort). Circulation 2017, 136, 1007–1021. [Google Scholar] [CrossRef]
- Radu, M.D.; Raber, L.; Heo, J.; Gogas, B.D.; Jørgensen, E.; Kelbæk, H.; Muramatsu, T.; Farooq, V.; Helqvist, S.; Garcia-Garcia, H.M.; et al. Natural history of optical coherence tomography-detected nonflow-limiting edge dissections following drug-eluting stent implantation. EuroIntervention 2014, 9, 1085–1094. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Total N = 95 | Ulteron™ 1.0 Software N = 55 | Earlier Generation Software N = 40 | p-Value | |
|---|---|---|---|---|
| Age, years | 66.1 ± 12.9 67.7 (61.3; 75.1) | 68.4 ± 10.8 68.3 (62.4; 75.8) | 63 ± 14.9 65.8 (57.8; 70.6) | 0.07 |
| Gender, male | 74 (77.9) | 44 (80) | 30 (75) | 0.62 |
| Euroscore II, % | 3 ± 2.5 2.1 (1.2; 4.1) | 2.9 ± 2.3 2 (1.2; 4.2) | 3.2 ± 2.7 2.3 (1.4; 3.7) | 0.58 |
| STS score | 2 ± 1.8 1.5 (0.7; 2.8) | 2 ± 1.8 1.3 (0.6; 2.8) | 2.1 ± 1.7 1.6 (0.7; 3.3) | 0.76 |
| Syntax I | 15.2 ± 9.2 13 (8; 21) | 16 ± 9.4 13.5 (8; 24) | 14.2 ± 9.1 13 (7.2; 19) | 0.35 |
| Syntax II PCI 4-year mortality, % | 18.2 ± 18 10 (5.3; 23.9) | 19.2 ± 18.2 13.9 (5.9; 23.6) | 16.9 ± 17.8 9.2 (4.2; 27.6) | 0.54 |
| Syntax II CABG 4-year mortality, % | 12 ± 10.4 9.1 (4.1; 17.2) | 12.3 ± 10.1 9.1 (4.8; 17.4) | 11.7 ± 11.1 8.5 (3.1; 16.8) | 0.4 |
| Diabetes mellitus | 33 (34.7) | 22 (40) | 11 (27.5) | 0.27 |
| Hypercholesterolemia | 56 (58.9) | 29 (52.7) | 27 (67.5) | 0.2 |
| Arterial hypertension | 79 (83.2) | 46 (83.6) | 33 (82.5) | 0.88 |
| Kidney failure | 7 (7.4) | 5 (9.1) | 2 (5) | 0.69 |
| Dialysotherapy | 1 (1) | 1 (1.8) | 0 (0) | 0.3 |
| Prior PCI | 58 (61) | 36 (65.4) | 22 (55) | 0.39 |
| Prior CABG | 6 (6.3) | 1 (1.8) | 5 (12.5) | 0.95 |
| COPD/Bronchial asthma | 14 (14.7) | 8 (14.5) | 6 (15) | 0.95 |
| Smoking | 26 (27.4) | 14 (25.4) | 12 (30) | 0.79 |
| Family history of CVD | 14 (14.7) | 5 (9.1) | 9 (22.5) | 0.08 |
| Heart failure | 47 (49.5) | 29 (52.7) | 18 (45) | 0.53 |
| LVEF, % | 42 ± 16.4 45 (29.5; 55) | 40.5 ± 16 42.5 (28.5; 55) | 44 ± 16.9 47 (32.5; 55) | 0.33 |
| Peripheral artery disease | 13 (13.7) | 5 (9.1) | 8 (20) | 0.14 |
| Prior PTCA | 3 (3.2) | 1 (1.8) | 2 (5) | 0.57 |
| Prior stroke | 7 (7.4) | 5 (9.1) | 2 (5) | 0.69 |
| Total N = 95 | Ulteron™ 1.0 Software N = 55 | Earlier Generation Software N = 40 | p-Value | |
|---|---|---|---|---|
| LMCA | 27 (28.4) | 17 (30.9) | 10 (25) | 0.52 |
| LAD | 69 (72.6) | 43 (78.2) | 26 (65) | 0.15 |
| Diagonal branch | 13 (13.7) | 11 (20) | 2 (5) | 0.03 |
| Circumflex branch | 27 (28.4) | 15 (27.3) | 12 (30) | 0.77 |
| Marginal branch | 5 (5.3) | 2 (3.6) | 3 (7.5) | 0.64 |
| Right coronary artery | 30 (31.6) | 15 (27.3) | 15 (37.5) | 0.28 |
| Chronic total occlusion | 8 (8.4) | 5 (9.1) | 3 (7.5) | 1.0 |
| PCI + stent | 87 (91.6) | 52 (94.5) | 35 (87.5) | 0.27 |
| Drug-eluting balloon | 4 (4.2) | 2 (3.6) | 2 (5) | 1.0 |
| Drug-eluting stent | 82 (86.3) | 52 (94.5) | 30 (75) | 0.006 |
| Bioresorbable scaffold | 6 (6.3) | 0 (0) | 6 (15) | 0.004 |
| Type of antimitotic agent: | ||||
| Everolimus | 72 (76.6) | 45 (81.8) | 27 (69.2) | 0.17 |
| Sirolimus | 18 (18.9) | 7 (12.7) | 11 (27.5) | 0.07 |
| Zotarolimus | 2 (2.1) | 2 (3.6) | 0 (0) | 0.5 |
| Number of stents | 1.8 ± 1.1 2 (1; 2) | 1.9 ± 1.1 2 (1; 2) | 1.7 ± 1.2 1 (1; 3) | 0.22 |
| Number of stents: | 0.03 | |||
| 0 | 8 (8.4) | 3 (5.4) | 5 (12.5) | |
| 1 | 35 (36.8) | 17 (30.9) | 18 (45) | |
| 2 | 30 (31.6) | 24 (43.6) | 6 (15) | |
| 3 | 14 (14.7) | 7 (12.7) | 7 (17.5) | |
| 4 | 6 (6.3) | 2 (3.6) | 4 (10) | |
| 5 | 2 (2.1) | 2 (3.6) | 0 (0) | |
| Total stent length, mm | 46.1 ± 28.6 41 (24; 66) | 48.8 ± 25.2 48 (28; 66) | 42.4 ± 32.7 38 (18; 72.7) | 0.12 |
| Maximum stent diameter, mm | 3.4 ± 3.2 3.5 (3; 3.5) | 3.7 ± 4.1 3.5 (3; 3.5) | 2.9 ± 1.2 3.5 (3; 3.5) | 0.31 |
| Minimum stent diameter, mm | 2.7 ± 1 3 (2.5; 3.5) | 2.8 ± 0.9 3 (2.5; 3.5) | 2.6 ± 1.1 2.6 (2.5; 3.4) | 0.27 |
| Maximum balloon diameter, mm | 4.1 ± 0.9 4 (3.5; 5) | 4.1 ± 1 4 (3.5; 5) | 4.1 ± 0.9 3.7 (3.5; 4.5) | 0.7 |
| Maximum balloon pressure, atm. | 21.4 ± 6.3 20 (18; 24) | 22.1 ± 6.9 20 (18; 25) | 20.6 ± 5.3 20 (16; 24) | 0.19 |
| Rotablation | 22 (23.2) | 14 (25.4) | 8 (20) | 0.53 |
| IVL | 8 (8.4) | 5 (9.1) | 3 (7.5) | 1.0 |
| Impella pump | 25 (26.3) | 14 (25.4) | 11 (27.5) | 0.82 |
| IABP | 3 (3.2) | 1 (1.8) | 2 (5) | 0.57 |
| Total N = 95 | Ulteron™ 1.0 Software N = 55 | Earlier Generation Software N = 40 | p-Value | |
|---|---|---|---|---|
| Before PCI | ||||
| Type of plaque: | 0.63 | |||
| - Lipidic | 8 (9.4) | 5 (9.1) | 3 (10) | |
| - Fibrotic | 14 (16.5) | 8 (14.5) | 6 (20) | |
| - Mild/moderate calcium | 21 (24.7) | 12 (21.8) | 9 (30) | |
| - Severe calcium | 42 (49.4) | 30 (54.5) | 12 (40) | |
| Maximum calcium angle, ° | 170.2 ± 122.7 181 (0; 289) | 174.7 ± 121.8 183 (59; 296) | 162.2 ± 125.9 180 (0; 261) | 0.71 |
| Maximum calcium thickness, mm | 0.9 ± 0.6 1.1 (0; 1.4) | 0.9 ± 0.6 1.1 (0.5; 1.4) | 0.9 ± 0.7 1 (0; 1.3) | 0.51 |
| Total calcium length, mm | 11 ± 13.7 5 (0; 19) | 11.6 ± 13.3 5 (2; 20) | 9.9 ± 14.5 3 (0; 13.5) | 0.27 |
| Minimum lumen diameter, mm | 1.5 ± 0.44 1.4 (1.2; 1.7) | 1.46 ± 0.4 1.38 (1.1; 1.6) | 1.6 ± 0.5 1.52(1.2; 2) | 0.18 |
| Distal EEL reference diameter, mm | 3.39 ± 0.76 3.26 (2.9; 3.8) | 3.25 ± 0.7 3 (2.84; 3.75) | 3.72 ± 0.82 3.56 (3.2; 4.1) | 0.02 |
| Distal EEL reference to minimum stent diameter ratio | 1.13 ± 0.2 1.09 (1.01; 1.2) | 1.08 ± 0.15 1.08 (1; 1.14) | 1.26 ± 0.25 1.2 (1.1; 1.34) | 0.003 |
| Distal lumen diameter, mm | 2.56 ± 0.8 2.43 (2; 2.95) | 2.5 ± 0.74 2.36 (1.94; 2.94) | 2.67 ± 0.82 2.7 (2.1; 3.2) | 0.31 |
| Distal lumen to minimum stent diameter ratio | 0.84 ± 0.2 0.82 (0.7; 0.94) | 0.82 ± 0.2 0.8 (0.7; 0.93) | 0.9 ± 0.25 0.9 (0.7; 1) | 0.1 |
| After PCI | ||||
| Medial dissection | 2 (2.35) | 1 (1.82) | 1 (3.33) | 0.66 |
| Malapposition | 1 (1.18) | 1 (1.82) | 0 (0) | 1.0 |
| Minimum stent expansion, % | 96 ± 16.7 95 (86; 106) | 96.2 ± 16.2 94 (86.5; 105) | 95.8 ± 17.9 96.5 (85; 108) | 0.91 |
| Minimum lumen diameter, mm | 2.7 ± 0.6 2.7 (2.3; 3.1) | 2.64 ± 0.6 2.6 (2.2; 3) | 2.8 ± 0.6 2.7 (2.4; 3.2) | 0.32 |
| Minimum lumen to minimum stent diameter ratio | 0.92 ± 0.16 0.9 (0.84; 0.97) | 0.89 ± 0.14 0.89 (0.82; 0.97) | 0.96 ± 0.18 0.94 (0.9; 1) | 0.06 |
| Total N = 95 | Ulteron™ 1.0 Software N = 55 | Earlier Generation Software N = 40 | p-Value | |
|---|---|---|---|---|
| Completed follow-up | 94 (98.9) | 54 (98.2) | 40 (100) | 1.0 |
| TLR: | 3 (3.5) | 0 (0) | 3 (9.4) | 0.01 |
| - In-stent restenosis | 3 (100) | 0 (0) | 3 (100) | |
| - In-stent thrombosis | - | - | - | |
| TVR | 6 (7.1) | 0 (0) | 6 (18.7) | 0.001 |
| Myocardial infarction | 2 (2.3) | 0 (0) | 2 (6.2) | 0.04 |
| Stroke | 2 (2.3) | 1 (1.9) | 1 (3.1) | 0.71 |
| Re-PCI | 6 (7.1) | 1 (1.9) | 5 (15.6) | 0.02 |
| CABG | 0 (0) | 0 (0) | 0 (0) | - |
| Cardiac death | 3 (3.5) | 3 (5.6) | 0 (0) | 0.09 |
| TV-MI | 1 (1.2) | 0 (0) | 1 (3.1) | 0.16 |
| MACE | 16 (18.4) | 6 (10.9) | 10 (31.2) | 0.01 |
| Death overall | 5 (5.7) | 5 (9.1) | 0 (0) | 0.03 |
| Mean follow-up duration, days | 252.3 ± 479.2 98 (31; 196) | 82.5 ± 76.6 56 (26; 126) | 485.7 ± 670 189 (67; 467) | <0.001 |
| Variable | Estimate | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Ultreon 1.0 vs. older software | 2.29 | −4.207–8.788 | 0.5 |
| History of CVD, yes vs. no | −13.387 | −22.722–(−4.052) | 0.008 |
| Sirolimus, yes vs. no | −10.893 | −19.226–(−2.56) | 0.01 |
| Insulinotherapy, yes vs. no | 8.299 | 0.369–16.228 | 0.053 |
| Inhalators, yes vs. no | −10.93 | −21.896–0.035 | 0.06 |
| Age, years | −0.206 | −0.462–0.05 | 0.13 |
| Hemoglobin, g/dL | 1.904 | 0.026–3.783 | 0.06 |
| Maximum stent length, mm | −0.851 | −1.781–0.078 | 0.09 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Januszek, R.; Siłka, W.; Sabatowski, K.; Malinowski, K.P.; Heba, G.; Surowiec, S.; Chyrchel, M.; Rzeszutko, Ł.; Bryniarski, L.; Surdacki, A.; et al. Procedure-Related Differences and Clinical Outcomes in Patients Treated with Percutaneous Coronary Intervention Assisted by Optical Coherence Tomography between New and Earlier Generation Software (Ultreon™ 1.0 Software vs. AptiVue™ Software). J. Cardiovasc. Dev. Dis. 2022, 9, 218. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9070218
Januszek R, Siłka W, Sabatowski K, Malinowski KP, Heba G, Surowiec S, Chyrchel M, Rzeszutko Ł, Bryniarski L, Surdacki A, et al. Procedure-Related Differences and Clinical Outcomes in Patients Treated with Percutaneous Coronary Intervention Assisted by Optical Coherence Tomography between New and Earlier Generation Software (Ultreon™ 1.0 Software vs. AptiVue™ Software). Journal of Cardiovascular Development and Disease. 2022; 9(7):218. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9070218
Chicago/Turabian StyleJanuszek, Rafał, Wojciech Siłka, Karol Sabatowski, Krzysztof Piotr Malinowski, Grzegorz Heba, Sławomir Surowiec, Michał Chyrchel, Łukasz Rzeszutko, Leszek Bryniarski, Andrzej Surdacki, and et al. 2022. "Procedure-Related Differences and Clinical Outcomes in Patients Treated with Percutaneous Coronary Intervention Assisted by Optical Coherence Tomography between New and Earlier Generation Software (Ultreon™ 1.0 Software vs. AptiVue™ Software)" Journal of Cardiovascular Development and Disease 9, no. 7: 218. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9070218