
Low Prevalence of Cardiomyopathy in Patients with Mitochondrial Disease and Neurological Manifestations


Abstract
:1. Introduction
2. Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nissanka, N.; Moraes, C.T. Mitochondrial DNA damage and reactive oxygen species in neurodegenerative disease. FEBS Lett. 2018, 592, 728–742. [Google Scholar] [CrossRef] [PubMed]
- Alston, C.L.; Rocha, M.C.; Lax, N.Z.; Turnbull, D.M.; Taylor, R.W. The genetics and pathology of mitochondrial disease. J. Pathol. 2017, 241, 236–250. [Google Scholar] [CrossRef] [PubMed]
- Lightowlers, R.N.; Taylor, R.W.; Turnbull, D.M. Mutations causing mitochondrial disease: What is new and what challenges remain? Science 2015, 349, 1494. [Google Scholar] [CrossRef] [PubMed]
- Kanungo, S.; Morton, J.; Neelakantan, M.; Ching, K.; Saeedian, J.; Goldstein, A. Mitochondrial disorders. Ann. Transl. Med. 2018, 6, 475. [Google Scholar] [CrossRef]
- DiMauro, S.; Schon, E.A. Mitochondrial respiratory-chain diseases. N. Engl. J. Med. 2003, 348, 2656–2668. [Google Scholar] [CrossRef]
- Stewart, J.B.; Chinnery, P.F. The dynamics of mitochondrial DNA heteroplasmy: Implications for human health and disease. Nat. Rev. Genet. 2015, 16, 530–542. [Google Scholar] [CrossRef] [PubMed]
- Wahbi, K.; Bougouin, W.; Behin, A.; Stojkovic, T.; Becane, H.M.; Jardel, C.; Berber, N.; Mochel, F.; Lombes, A.; Eymard, B.; et al. Long-term cardiac prognosis and risk stratification in 260 adults presenting with mitochondrial diseases. Eur. Heart J. 2015, 36, 2886–2893. [Google Scholar] [CrossRef] [Green Version]
- Anan, R.; Nakagawa, M.; Miyata, M.; Higuchi, I.; Nakao, S.; Suehara, M.; Osame, M.; Tanaka, H. Cardiac involvement in mitochondrial diseases. A study on 17 patients with documented mitochondrial DNA defects. Circulation 1995, 91, 955–961. [Google Scholar] [CrossRef]
- Scaglia, F.; Towbin, J.A.; Craigen, W.J.; Belmont, J.W.; Smith, E.O.; Neish, S.R.; Ware, S.M.; Hunter, J.V.; Fernbach, S.D.; Vladutiu, G.D.; et al. Clinical spectrum, morbidity, and mortality in 113 pediatric patients with mitochondrial disease. Pediatrics 2004, 114, 925–931. [Google Scholar] [CrossRef]
- Finsterer, J.; Stöllberger, C.; Blazek, G.; Kunafer, M.; Prager, E. Cardiac involvement over 10 years in myotonic and Becker muscular dystrophy and mitochondrial disorder. Int. J. Cardiol. 2007, 119, 176–184. [Google Scholar] [CrossRef]
- Holmgren, D.; Wåhlander, H.; Eriksson, B.O.; Oldfors, A.; Holme, E.; Tulinius, M. Cardiomyopathy in children with mitochondrial disease; clinical course and cardiological findings. Eur. Heart J. 2003, 24, 280–288. [Google Scholar] [CrossRef]
- Limongelli, G.; Tome-Esteban, M.; Dejthevaporn, C.; Rahman, S.; Hanna, M.G.; Elliott, P.M. Prevalence and natural history of heart disease in adults with primary mitochondrial respiratory chain disease. Eur. J. Heart Fail. 2010, 12, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Quadir, A.; Pontifex, C.S.; Lee Robertson, H.; Labos, C.; Pfeffer, G. Systematic review and meta-analysis of cardiac involvement in mitochondrial myopathy. Neurol. Genet. 2019, 5, e339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bates, M.G.; Bourke, J.P.; Giordano, C.; d’Amati, G.; Turnbull, D.M.; Taylor, R.W. Cardiac involvement in mitochondrial DNA disease: Clinical spectrum, diagnosis, and management. Eur. Heart J. 2012, 33, 3023–3033. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, Y.H.; Yogasundaram, H.; Parajuli, N.; Valtuille, L.; Sergi, C.; Oudit, G.Y. MELAS syndrome and cardiomyopathy: Linking mitochondrial function to heart failure pathogenesis. Heart Fail. Rev. 2016, 21, 103–116. [Google Scholar] [CrossRef] [PubMed]
- Bittles, A.H. Evidence for and against the causal involvement of mitochondrial DNA mutation in mammalian ageing. Mutat. Res. 1992, 275, 217–225. [Google Scholar] [CrossRef]
- McFarland, R.; Taylor, R.W.; Turnbull, D.M. A neurological perspective on mitochondrial disease. Lancet Neurol. 2010, 9, 829–840. [Google Scholar] [CrossRef]
- Pankuweit, S.; Richter, A. Mitochondrial disorders with cardiac dysfunction: An under-reported aetiology with phenotypic heterogeneity. Eur. Heart J. 2015, 36, 2894–2897. [Google Scholar] [CrossRef]
- Anderson, T.J.; Gregoire, J.; Pearson, G.J.; Barry, A.R.; Couture, P.; Dawes, M.; Francis, G.A.; Genest, J., Jr.; Grover, S.; Gupta, M.; et al. 2016 Canadian Cardiovascular Society Guidelines for the Management of Dyslipidemia for the Prevention of Cardiovascular Disease in the Adult. Can. J. Cardiol. 2016, 32, 1263–1282. [Google Scholar] [CrossRef]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E., Jr.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 2018, 71, 1269–1324. [Google Scholar]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool For Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Yancy Clyde, W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey Donald, E.; Colvin Monica, M.; Drazner Mark, H.; Filippatos Gerasimos, S.; Fonarow Gregg, C.; Givertz Michael, M.; et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation 2017, 136, e137–e161. [Google Scholar]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–270. [Google Scholar] [CrossRef] [PubMed]
- Messroghli, D.R.; Moon, J.C.; Ferreira, V.M.; Grosse-Wortmann, L.; He, T.; Kellman, P.; Mascherbauer, J.; Nezafat, R.; Salerno, M.; Schelbert, E.B.; et al. Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: A consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI). J. Cardiovasc. Magn. Reson. 2017, 19, 75. [Google Scholar] [PubMed] [Green Version]
- Kabunga, P.; Lau, A.K.; Phan, K.; Puranik, R.; Liang, C.; Davis, R.L.; Sue, C.M.; Sy, R.W. Systematic review of cardiac electrical disease in Kearns-Sayre syndrome and mitochondrial cytopathy. Int. J. Cardiol. 2015, 181, 303–310. [Google Scholar] [CrossRef]
- Weber, K.T.; Janicki, J.S. The metabolic demand and oxygen supply of the heart: Physiologic and clinical considerations. Am. J. Cardiol. 1979, 44, 722–729. [Google Scholar] [CrossRef]
- Lim, A.Z.; Jones, D.M.; Bates, M.G.D.; Schaefer, A.M.; Sullivan, J.; Feeney, C.; Farrugia, M.E.; Bourke, J.P.; Turnbull, D.M.; Gorman, G.S.; et al. Risk of cardiac manifestations in adult mitochondrial disease caused by nuclear genetic defects. Open Heart 2021, 8, e001510. [Google Scholar] [CrossRef]
- Mancini, G.B.J.; Gosselin, G.; Chow, B.; Kostuk, W.; Stone, J.; Yvorchuk, K.J.; Abramson, B.L.; Cartier, R.; Huckell, V.; Tardif, J.C.; et al. Canadian Cardiovascular Society Guidelines for the Diagnosis and Management of Stable Ischemic Heart Disease. Can. J. Cardiol. 2014, 30, 837–849. [Google Scholar] [CrossRef]
- Apabhai, S.; Gorman, G.S.; Sutton, L.; Elson, J.L.; Plötz, T.; Turnbull, D.M.; Trenell, M.I. Habitual physical activity in mitochondrial disease. PLoS ONE 2011, 6, e22294. [Google Scholar] [CrossRef]
- Imamura, T.; Sumitomo, N.; Muraji, S.; Mori, H.; Osada, Y.; Oyanagi, T.; Kojima, T.; Yoshiba, S.; Kobayashi, T.; Ono, K. The necessity of implantable cardioverter defibrillators in patients with Kearns-Sayre syndrome-systematic review of the articles. Int. J. Cardiol. 2019, 279, 105–111. [Google Scholar] [CrossRef]
- Nikhanj, A.; Yogasundaram, H.; Kimber, S.; Siddiqi, Z.A.; Oudit, G.Y. Clinical utility of 12-lead electrocardiogram in evaluating heart disease in patients with muscular dystrophy: Assessment of left ventricular hypertrophy, conduction disease, and cardiomyopathy. Ann. Noninvasive Electrocardiol. 2021, 26, e12876. [Google Scholar] [CrossRef] [PubMed]
- Duchnowski, P.; Hryniewiecki, T.; Kuśmierczyk, M.; Szymański, P. The usefulness of selected biomarkers in aortic regurgitation. Cardiol. J. 2019, 26, 477–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nikhanj, A.; Miskew Nichols, B.; Wang, K.; Siddiqi, Z.A.; Oudit, G.Y. Evaluating the diagnostic and prognostic value of biomarkers for heart disease and major adverse cardiac events in patients with muscular dystrophy. Eur. Heart J. Qual. Care Clin. Outcomes 2021, 7, 564–573. [Google Scholar] [CrossRef] [PubMed]
- Nikhanj, A.; Yogasundaram, H.; Miskew Nichols, B.; Richman-Eisenstat, J.; Phan, C.; Bakal, J.A.; Siddiqi, Z.A.; Oudit, G.Y. Cardiac Intervention Improves Heart Disease and Clinical Outcomes in Patients with Muscular Dystrophy in a Multidisciplinary Care Setting. J. Am. Heart Assoc. 2020, 9, e014004. [Google Scholar] [CrossRef]
- Nikhanj, A.; Sivakumaran, S.; Yogasundaram, H.; Becher, H.; Kimber, S.; Siddiqi, Z.A.; Oudit, G.Y. Comparison of Usefulness of Cardiac Resynchronization Therapy in Patients with Type 1 Myotonic Dystrophy with Versus without Left Bundle Branch Block. Am. J. Cardiol. 2019, 124, 1770–1774. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
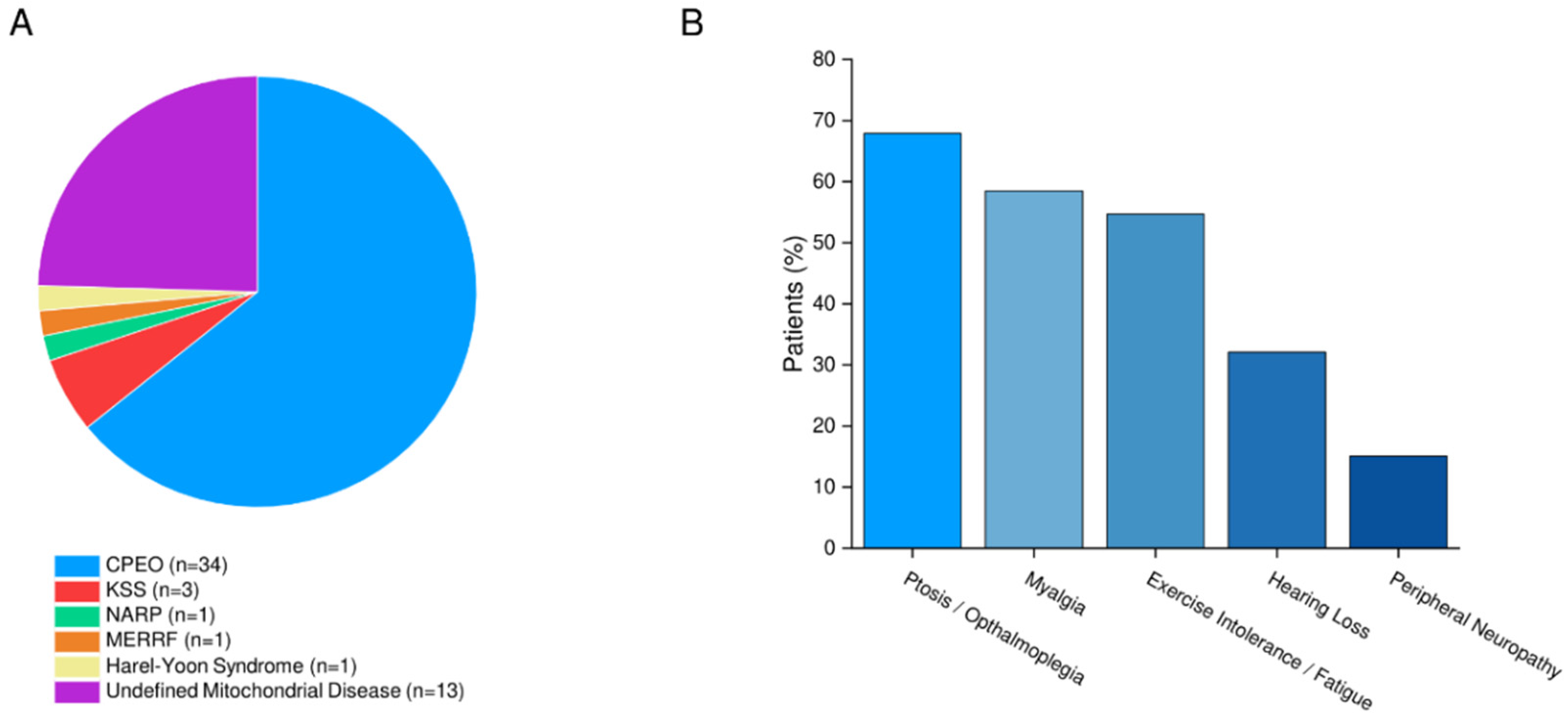
| Variable | Mitochondrial Disease (n = 53) |
|---|---|
| Men/Women, No. | 19 (35.8%)/34 (64.2%) |
| Age, Yrs. | 50.0 (33.0–61.0) |
| Height, cm | 165.1 (160.0–175.4) |
| Weight, kg | 73.0 (59.8–82.0) |
| Body Surface Area, m2 | 1.80 (1.60–2.03) |
| Current/Former Smoker, No. | 17 (32.1%) |
| Ambulatory Aids, No. | 5 (9.43%) |
| Comorbidities, No. | |
| Diabetes | 5 (9.43%) |
| Dyslipidemia * | 9 (17.0%) |
| Hypertension † | 7 (13.2%) |
| Respiratory Disease | 20 (37.7%) |
| Sleep Disordered Breathing | 11 (20.8%) |
| Respiratory Therapies, No. | |
| Lung Volume Recruitment | 5 (9.43%) |
| Non-Invasive Ventilation | 5 (9.43%) |
| Vitals, median | |
| Heart Rate, bpm | 80.0 (65.0–87.5) |
| Systolic Blood Pressure, mmHg | 125.0 (116.5–135.5) |
| Diastolic Blood Pressure, mmHg | 75.0 (66.5–82.0) |
| Biomarkers, median | |
| B-Type Natriuretic Peptide | 14.0 (7.00–37.0) |
| Creatine Kinase | 99.0 (72.8–218.5) |
| Creatinine | 63.0 (50.0–79.5) |
| C-Reactive Protein | 3.00 (1.40–8.80) |
| Potassium | 4.40 (4.10–4.70) |
| Modality | Mitochondrial Disease |
|---|---|
| 12-Lead Electrocardiogram | (n = 53) |
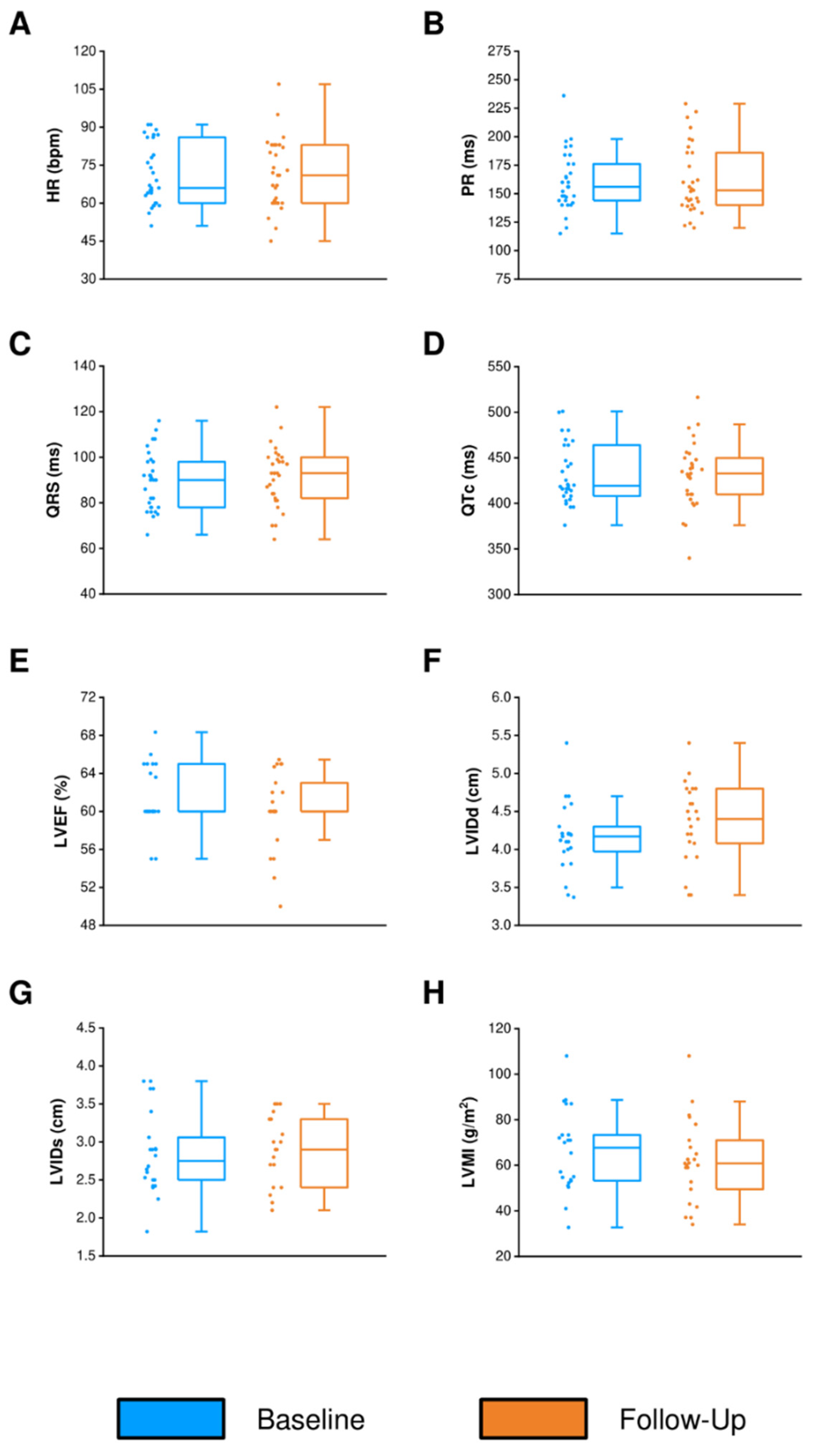
| Heart Rate, bpm | 71.0 (62.0–82.5) |
| PR Interval, ms | 155.5 (144.0–171.3) |
| QRS Duration, ms | 90.0 (79.0–98.0) |
| QT Interval, ms | 396.0 (372.0–415.5) |
| QTc Bazett, ms | 425.5 (414.3–443.0) |
| Advanced Atrioventricular Block | 0 |
| Left Anterior Fascicular Block | 1 (1.89%) |
| Echocardiogram | (n = 40) |
| Left Atrial Volume Index (mL/m2) | 20.2 (16.5–25.1) |
| Left Ventricular Internal Dimension at End-Diastole (cm) | 4.30 (4.10–4.70) |
| Left Ventricular Internal Dimension at End-Systole (cm) | 2.80 (2.52-3.03) |
| Left Ventricular Posterior Wall Thickness at End-Diastole (cm) | 0.88 (0.77–0.99) |
| Left Ventricular Ejection Fraction (%) | 59.0 (58.0–61.8) |
| Left Ventricular Mass Index (g/m2) | 67.0 (56.1–76.3) |
| E/e’ | 7.55 (6.40–8.93) |
| Mitral Valve E/A | 1.30 (0.99–1.47) |
| Mitral Valve Deceleration Time (ms) | 186.0 (168.0–262.0) |
| Tricuspid Annular Plane Systolic Excursion (mm) | 2.24 (1.98–2.53) |
| Right Ventricular Systolic Pressure (mmHg) | 25.0 (23.3–26.1) |
| Right Ventricle Size | Normal |
| Right Ventricular Systolic Function | Normal |
| Cardiac Magnetic Resonance Imaging | (n = 13) |
| Left Atrial Volume Index (mL/m2) | 27.0 (22.0–33.4) |
| Left Ventricular End Diastolic Volume Index (mL/m2) | 66.0 (54.5–74.5) |
| Left Ventricular End Systolic Volume Index (mL/m2) | 27.0 (25.5–28.0) |
| Left Ventricular Ejection Fraction (%) | 62.0 (56.0–64.0) |
| Left Ventricular Mass Index (g/m2) | 44.0 (34.0–51.0) |
| Right Ventricular End Diastolic Volume Index (mL/m2) | 70.0 (60.5–79.5) |
| Right Ventricular End Systolic Volume Index (mL/m2) | 34.0 (26.0–38.0) |
| Right Ventricular Ejection Fraction (%) | 55.0 (52.0–58.0) |
| Patient/Diagnosis | Age (yrs)/Sex | Clinical History and Comorbidities | Cardiac Abnormality | HR (bpm) | sBP (mmHg)/dBP (mmHg) | ECG Findings (ms) | TTE Findings | Before Assessment | After Assessment | |
|---|---|---|---|---|---|---|---|---|---|---|
| Cardiac Medication and Daily Dose (mg) | Cardiac Medication and Daily dose (mg) | Cardiac Device | ||||||||
| 1/Harel–Yoon Syndrome | 21/M | Spastic paraplegia (spasticity, weakness, ataxia), neuropathy, seizures | Moderate LV systolic dysfunction | 133 | 117/75 | PR: 131; QRS: 80 QTc: 421 Sinus tachycardia | LVEF: 38.0% LVMI: 50.7 g/m2 LVIDd: 3.90 cm LVIDs: 3.40 cm LAVI: 9.00 mL/m2 | Perindopril 2 mg, Bisoprolol 1.25 mg | Perindopril 4 mg, Bisoprolol 2.5 mg | NA |
| 2/CPEO | 61/F | Dyslipidemia, respiratory disease (exertional dyspnea, SDOB) | Mild LV systolic and diastolic dysfunction | 65 | 117/70 | PR: 160; QRS: 105 QTc: 449 | LVEF: 53.0% LVMI: 78.0 g/m2 LVIDd: 4.80 cm LVIDs: 3.50 cm LAVI: 27.0 mL/m2 | NA | Perindopril 2 mg, Bisoprolol 2.5 mg | NA |
| 3/CPEO | 78/M | Syncope, respiratory disease (oropharyngeal dysphagia) | Mild LV systolic dysfunction, Non-sustained VT | 60 | 124/72 | PR: 232; QRS: 108 QTc: 456 1st degree AVB, 2 PVCs | LVEF: 45.0% LVMI: 108.0 g/m2 LVIDd: 5.40 cm LVIDs: 3.40 cm LAVI: 40.6 mL/m2 | Metoprolol 25 mg | Perindopril 4 mg, Metoprolol 100 mg | Dual-chamber ICD |
| 4/CPEO | 26/F | Severe fatigue, migraines, myalgia | Secundum ASD, RV dilation, RV hypertrophy | 70 | 118/80 | PR: 164; QRS: 89 QTc: 374 | LVEF: 60.0% LVMI: 49.6 g/m2 LVIDd: 3.40 cm LVIDs: 2.60 cm LAVI: 15.0 mL/m2 | NA | NA | NA |
| 5/CPEO | 59/M | Smoker, TIA Angina | Atrial Fibrillation (Wolff–Parkinson–White Syndrome) | 103 | 90/62 | PR: 155; QRS: 95 QTc: 377 | LVEF: 55.0% LVMI: 66.2 g/m2 LVIDd: 4.50 cm LVIDs: 3.30 cm LAVI: 16.8 mL/m2 | NA | Apixaban 10 mg | NA |
| 6/CPEO | 52/M | Syncope, falls, dysautonomia, neuropathy, seizures | LV hypertrophy, LA enlargement | 71 | 144/83 | PR: 176; QRS: 106 QTc: 513 LV hypertrophy, P mitrale | LVEF: 60.0% LVMI: 115.5 g/m2 LVIDd: 4.40 cm LVIDs: 3.30 cm LAVI: 45.0 mL/m2 | Perindopril 4 mg | Perindopril 8 mg | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nikhanj, A.; Bautista, J.; Siddiqi, Z.A.; Phan, C.L.; Oudit, G.Y. Low Prevalence of Cardiomyopathy in Patients with Mitochondrial Disease and Neurological Manifestations. J. Cardiovasc. Dev. Dis. 2022, 9, 221. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9070221
Nikhanj A, Bautista J, Siddiqi ZA, Phan CL, Oudit GY. Low Prevalence of Cardiomyopathy in Patients with Mitochondrial Disease and Neurological Manifestations. Journal of Cardiovascular Development and Disease. 2022; 9(7):221. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9070221
Chicago/Turabian StyleNikhanj, Anish, Jesi Bautista, Zaeem A. Siddiqi, Cecile L. Phan, and Gavin Y. Oudit. 2022. "Low Prevalence of Cardiomyopathy in Patients with Mitochondrial Disease and Neurological Manifestations" Journal of Cardiovascular Development and Disease 9, no. 7: 221. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9070221