
The Prediction and Prognosis of Fungal Infection in Lung Transplant Recipients—A Retrospective Cohort Study in South Korea

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.3. Lung Transplantation Protocol
2.4. Definition
2.5. Statistical Analyses
3. Results
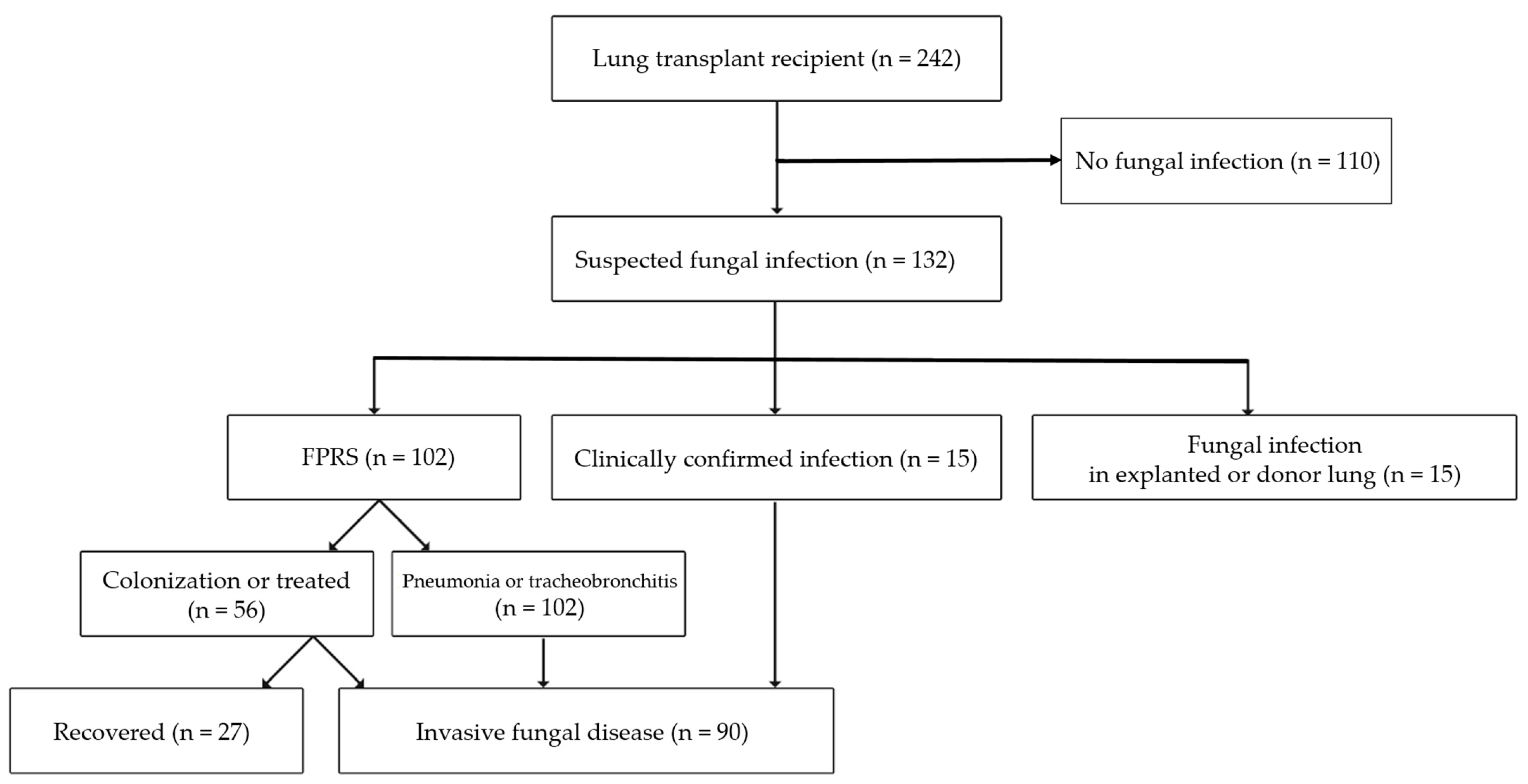
3.1. Study Population
3.2. Fungus-Positive Respiratory Samples
3.3. Characteristics of Patients with Invasive Fungal Diseases
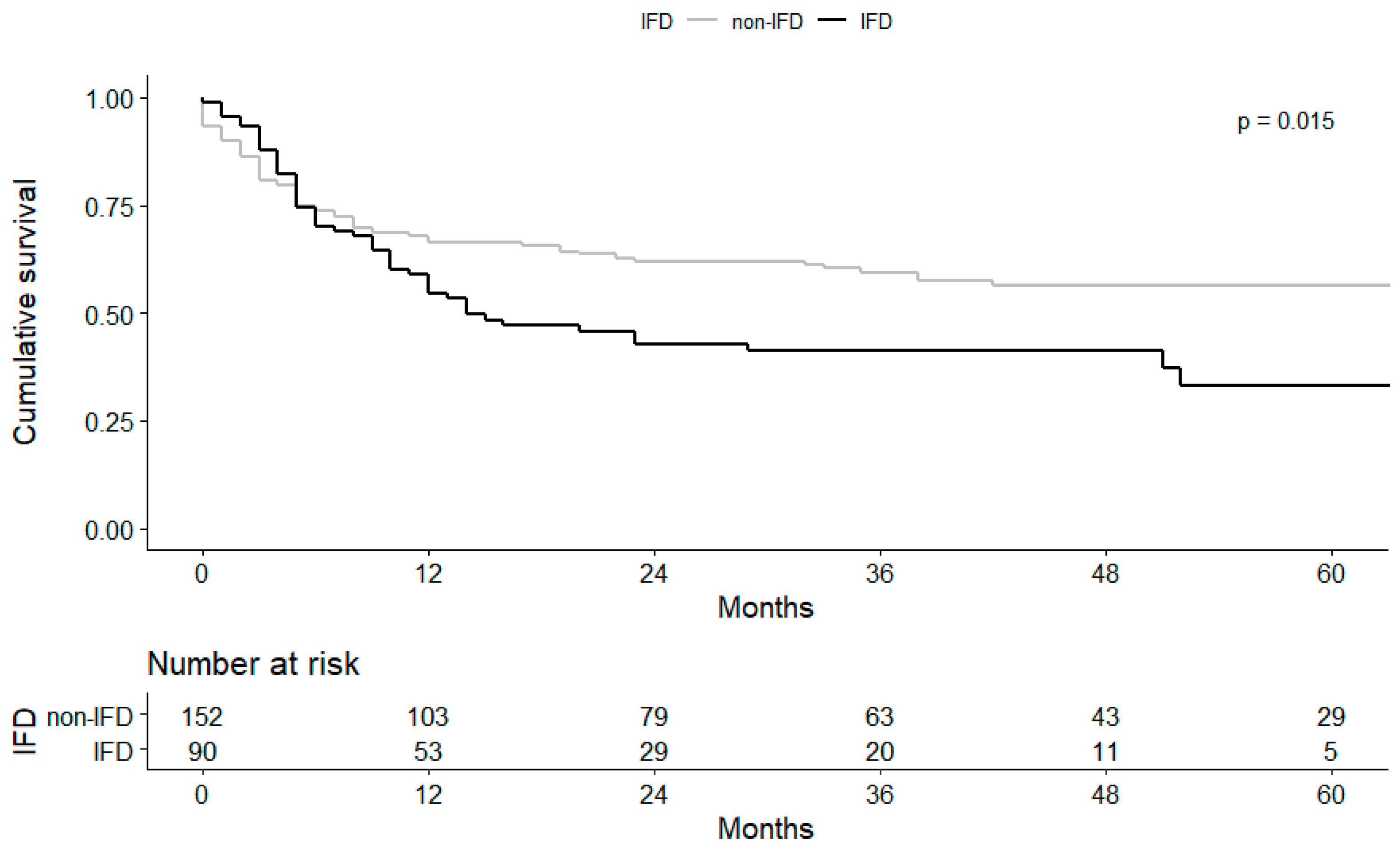
3.4. Clinical Course and Prognosis of Fungal Infection
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Kennedy, C.C.; Razonable, R.R. Fungal infections after lung transplantation. Clin. Chest Med. 2017, 38, 511–520. [Google Scholar] [CrossRef]
- Paik, H.C. Current perspective of lung transplantation. J. Korean Med. Assoc. 2016, 59, 119–124. [Google Scholar] [CrossRef] [Green Version]
- Pappas, P.G.; Alexander, B.D.; Andes, D.R.; Hadley, S.; Kauffman, C.A.; Freifeld, A.; Anaissie, E.J.; Brumble, L.M.; Herwaldt, L.; Ito, J. Invasive fungal infections among organ transplant recipients: Results of the transplant-associated infection surveillance network (transnet). Clin. Infect. Dis. 2010, 50, 1101–1111. [Google Scholar] [CrossRef]
- Arthurs, S.K.; Eid, A.J.; Deziel, P.J.; Marshall, W.F.; Cassivi, S.D.; Walker, R.C.; Razonable, R.R. The impact of invasive fungal diseases on survival after lung transplantation. Clin. Transplant. 2010, 24, 341–348. [Google Scholar] [CrossRef] [PubMed]
- Solé, A.; Salavert, M. Fungal infections after lung transplantation. Transplant. Rev. 2008, 22, 89–104. [Google Scholar] [CrossRef]
- Silveira, F.P.; Husain, S. Fungal infections in solid organ transplantation. Med. Mycol. 2007, 45, 305–320. [Google Scholar] [CrossRef]
- Doligalski, C.T.; Benedict, K.; Cleveland, A.A.; Park, B.; Derado, G.; Pappas, P.G.; Baddley, J.W.; Zaas, D.W.; Harris, M.T.; Alexander, B.D. Epidemiology of invasive mold infections in lung transplant recipients. Arab. Archaeol. Epigr. 2014, 14, 1328–1333. [Google Scholar] [CrossRef] [PubMed]
- Weigt, S.S.; Elashoff, R.M.; Huang, C.; Ardehali, A.; Gregson, A.L.; Kubak, B.; Fishbein, M.C.; Saggar, R.; Keane, M.P.; Saggar, R. Aspergillus colonization of the lung allograft is a risk factor for bronchiolitis obliterans syndrome. Am. J. Transplant. 2009, 9, 1903–1911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pasupneti, S.; Manouvakhova, O.; Nicolls, M.; Hsu, J. Aspergillus-related pulmonary diseases in lung transplantation. Med. Mycol. 2016, 55, 96–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pilarczyk, K.; Haake, N.; Heckmann, J.; Carstens, H.; Haneya, A.; Cremer, J.; Jakob, H.; Pizanis, N.; Kamler, M. Is universal antifungal prophylaxis mandatory in adults after lung transplantation? A review and meta-analysis of observational studies. Clin. Transplant. 2016, 30, 1522–1531. [Google Scholar] [CrossRef] [PubMed]
- Husain, S.; Sole, A.; Alexander, B.D.; Aslam, S.; Avery, R.; Benden, C.; Billaud, E.M.; Chambers, D.; Danziger-Isakov, L.; Fedson, S. The 2015 international society for heart and lung transplantation guidelines for the management of fungal infections in mechanical circulatory support and cardiothoracic organ transplant recipients: Executive summary. J. Heart Lung Transplant. 2016, 35, 261–282. [Google Scholar] [CrossRef] [Green Version]
- De Mol, W.; Bos, S.; Beeckmans, H.; Lagrou, K.; Spriet, I.; Verleden, G.M.; Vos, R. Antifungal prophylaxis after lung transplantation: Where are we now? Transplantation 2021. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H. Revision and update of the consensus definitions of invasive fungal disease from the european organization for research and treatment of cancer and the mycoses study group education and research consortium. Clin. Infect. Dis. 2019, 71, 1367–1376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.Y.; Jeong, S.J.; Lee, J.G.; Park, M.S.; Paik, H.C.; Na, S.; Kim, J. Critical care after lung transplantation. Acute Crit. Care 2018, 33, 206. [Google Scholar] [CrossRef] [PubMed]
- Hadjiliadis, D.; Howell, D.; Davis, R.; Lawrence, C.; Rea, J.; Tapson, V.; Perfect, J.; Palmer, S. Anastomotic infections in lung transplant recipients. Ann. Transplant. 2000, 5, 13. [Google Scholar]
- Cornely, O.A.; Hoenigl, M.; Lass-Flörl, C.; Chen, S.C.A.; Kontoyiannis, D.P.; Morrissey, C.O.; Thompson, G.R., 3rd. Mycoses Study Group Education and Research Consortium; European Confederation of Medical Mycology. Defining breakthrough invasive fungal infection–position paper of the mycoses study group education and research consortium and the european confederation of medical mycology. Mycoses 2019, 62, 716–729. [Google Scholar] [PubMed]
- Nucci, M.; Perfect, J.R. When primary antifungal therapy fails. Clin. Infect. Dis. 2008, 46, 1426–1433. [Google Scholar] [CrossRef]
- Sole, A.; Salavert, M. Fungal infections after lung transplantation. Curr. Opin. Pulm. Med. 2009, 15, 243–253. [Google Scholar] [CrossRef]
- Atchade, E.; Desmard, M.; Kantor, E.; Genève, C.; Tebano, G.; De Tymowski, C.; Tran-Dinh, A.; Zappella, N.; Houzé, S.; Mal, H. Fungal Isolation in Respiratory Tract after Lung Transplantation: Epidemiology, Clinical Consequences, and Associated Factors. Transplant. Proc. 2020, 52, 326–332. [Google Scholar] [CrossRef]
- Weder, W.; Inci, I.; Korom, S.; Kestenholz, P.B.; Hillinger, S.; Eich, C.; Irani, S.; Lardinois, D. Airway complications after lung transplantation: Risk factors, prevention and outcome. Eur. J. Cardio-Thorac. Surg. 2009, 35, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Baker, A.W.; Maziarz, E.K.; Arnold, C.J.; Johnson, M.D.; Workman, A.D.; Reynolds, J.M.; Perfect, J.R.; Alexander, B.D. Invasive fungal infection after lung transplantation: Epidemiology in the setting of antifungal prophylaxis. Clin. Infect. Dis. 2020, 70, 30–39. [Google Scholar] [CrossRef]
- Chong, P.P.; Kennedy, C.C.; Hathcock, M.A.; Kremers, W.K.; Razonable, R.R. Epidemiology of invasive fungal infections in lung transplant recipients on long-term azole antifungal prophylaxis. Clin. Transplant. 2015, 29, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Aguilar, C.A.; Hamandi, B.; Fegbeutel, C.; Silveira, F.P.; Verschuuren, E.A.; Ussetti, P.; Chin-Hong, P.V.; Sole, A.; Holmes-Liew, C.; Billaud, E.M. Clinical risk factors for invasive aspergillosis in lung transplant recipients: Results of an international cohort study. J. Heart Lung Transplant. 2018, 37, 1226–1234. [Google Scholar] [CrossRef]
- Forsberg, K.; Woodworth, K.; Walters, M.; Berkow, E.L.; Jackson, B.; Chiller, T.; Vallabhaneni, S. Candida auris: The recent emergence of a multidrug-resistant fungal pathogen. Med. Mycol. 2019, 57, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arendrup, M.C.; Patterson, T.F. Multidrug-resistant candida: Epidemiology, molecular mechanisms, and treatment. J. Infect. Dis. 2017, 216, S445–S451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beyda, N.D.; John, J.; Kilic, A.; Alam, M.J.; Lasco, T.M.; Garey, K.W. Fks mutant candida glabrata: Risk factors and outcomes in patients with candidemia. Clin. Infect. Dis. 2014, 59, 819–825. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Candida Strains | Cases (n = 85) |
|---|---|
| C. albicans | 18 (21.2) |
| Non-albicans strains | |
| C. glabrata1 | 31 (36.5) |
| C. tropicalis | 10 (11.8) |
| C. parapsilosis | 6 (7.1) |
| C. guilliermondii2 | 4 (4.7) |
| C. lusitaniae3 | 1 (1.2) |
| C. inconspicua4 | 1 (1.2) |
| C. auris | 1 (1.2) |
| Unknown (yeast) | 13 (15.3) |
| Variable | IFDs (n = 90) | Non-IFDs (n = 137) | p-Value |
|---|---|---|---|
| Age, years | 55.8 ± 11.8 | 51.8 ± 12.9 | 0.019 |
| Sex, male | 56 (62.2) | 88 (64.2) | 0.779 |
| BMI | 21.21 ± 4.2 | 20.86 ± 3.9 | 0.521 |
| Disease leading to LTx | |||
| Idiopathic pulmonary fibrosis | 43 (47.8) | 80 (58.4) | 0.135 |
| CTD-ILD | 18 (20.0) | 3 (2.3) | <0.001 |
| Pulmonary tuberculosis | 15 (16.7) | 30 (21.9) | 0.396 |
| COPD | 11 (12.2) | 13 (9.5) | 0.660 |
| Other ILD | 9 (10.0) | 19 (13.9) | 0.648 |
| Obliterative bronchiolitis | 7 (7.8) | 13 (9.5) | 0.812 |
| Emphysema & bronchiectasis | 6 (6.7) | 9 (6.6) | 0.977 |
| Pulmonary hypertension | 6 (6.7) | 11 (8.0) | 0.800 |
| Lymphangioleiomyomatosis | 2 (2.2) | 2 (1.5) | 0.65 |
| Acute interstitial pneumonia | 2 (2.2) | 2 (1.5) | 0.65 |
| ARDS | 1 (1.1) | 6 (4.4) | 0.249 |
| Underlying disease | |||
| DM | 25 (27.8) | 28 (25.7) | 0.750 |
| Connective tissue disease | 22 (24.4) | 17 (16) | 0.155 |
| Cancer | 18 (20.0) | 15 (14.4) | 0.303 |
| CAOD | 10 (11.1) | 6 (13.3) | 0.780 |
| Previous SCT | 6 (6.7) | 11 (8.1) | 0.800 |
| Previous SOT | 1 (1.1) | 6 (4.4) | 0.483 |
| Previous history within 3 months | |||
| Hospitalization, yes | 68 (75.6) | 94 (68.6) | 0.295 |
| Hospitalization days before LTx | 8 [0–33] | 0 [0–16] | 0.011 |
| Antibiotics use | 55 (61.1) | 80 (58.4) | 0.782 |
| Antifungal agent use 1 | 25 (27.8) | 19 (13.9) | 0.011 |
| Immunosuppressant use 2 | 52 (57.8) | 77 (56.2) | 0.891 |
| Prior ECMO use | 32 (35.6) | 34 (24.8) | 0.100 |
| Transplantation type | |||
| Single LTx | 5 (5.4) | 6 (4.4) | 0.757 |
| Surgery | |||
| Operation time, minutes | 412 [362–453] | 392 [356–455] | 0.480 |
| Blood loss, L | 2.45 [1.4–4.5] | 2.00 [1.1–3.2] | 0.057 |
| Total ICU length of stay, days | 19 [7–32] | 11 [5–24] | 0.020 |
| Hospitalization days after LTx | 62 [37.5–102.5] | 35 [23.5–60.5] | <0.001 |
| Post-surgery event in hospitalization period | |||
| Acute renal failure 3 | 16 (17.8) | 31 (22.6) | 0.407 |
| Weaning failure 4 | 54 (60.0) | 64 (46.7) | 0.058 |
| Reoperation 5 | 26 (28.9) | 27 (19.7) | 0.148 |
| Variable | Adjusted Odds Ratio (95% CI) | p-Value |
|---|---|---|
| Previous use of AFA | 2.32 (1.07–5.02) | 0.033 |
| Age (by 10-year) | 1.38 (1.07–1.79) | 0.014 |
| hospitalization days after LTx (by 30 days) | 1.24 (1.08–1.42) | 0.002 |
| CTD-ILD | 10.55 (2.85–39.10) | <0.001 |
| Survivors (n = 41) | Non-Survivors (n = 58) | p-Value | |
|---|---|---|---|
| Time from surgery to an episode (d) | 37 [21.5–133] | 55.5 [19.5–131.3] | 0.402 |
| Post-surgery event in hospitalization period | |||
| Acute renal failure 1 | 6 (35.3) | 11 (64.7) | 0.787 |
| Weaning failure 2 | 22 (35.5) | 40 (64.5) | 0.143 |
| Reoperation 3 | 11 (40.7) | 16 (59.3) | 1.000 |
| Genus | |||
| Aspergillus sp. | 16 (40) | 24 (60) | 0.978 |
| Candida sp. | 17 (39.5) | 26 (60.5) | 0.899 |
| Treatment failure | 11 (21.2) | 41 (78.8) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baek, Y.-J.; Cho, Y.-S.; Kim, M.-H.; Hyun, J.-H.; Sohn, Y.-J.; Kim, S.-Y.; Jeong, S.-J.; Park, M.-S.; Lee, J.-G.; Paik, H.-C. The Prediction and Prognosis of Fungal Infection in Lung Transplant Recipients—A Retrospective Cohort Study in South Korea. J. Fungi 2021, 7, 639. https://0-doi-org.brum.beds.ac.uk/10.3390/jof7080639
Baek Y-J, Cho Y-S, Kim M-H, Hyun J-H, Sohn Y-J, Kim S-Y, Jeong S-J, Park M-S, Lee J-G, Paik H-C. The Prediction and Prognosis of Fungal Infection in Lung Transplant Recipients—A Retrospective Cohort Study in South Korea. Journal of Fungi. 2021; 7(8):639. https://0-doi-org.brum.beds.ac.uk/10.3390/jof7080639
Chicago/Turabian StyleBaek, Yae-Jee, Yun-Suk Cho, Moo-Hyun Kim, Jong-Hoon Hyun, Yu-Jin Sohn, Song-Yee Kim, Su-Jin Jeong, Moo-Suk Park, Jin-Gu Lee, and Hyo-Chae Paik. 2021. "The Prediction and Prognosis of Fungal Infection in Lung Transplant Recipients—A Retrospective Cohort Study in South Korea" Journal of Fungi 7, no. 8: 639. https://0-doi-org.brum.beds.ac.uk/10.3390/jof7080639