
Performance of Two Commercial Assays for the Detection of Serum Aspergillus Galactomannan in Non-Neutropenic Patients

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
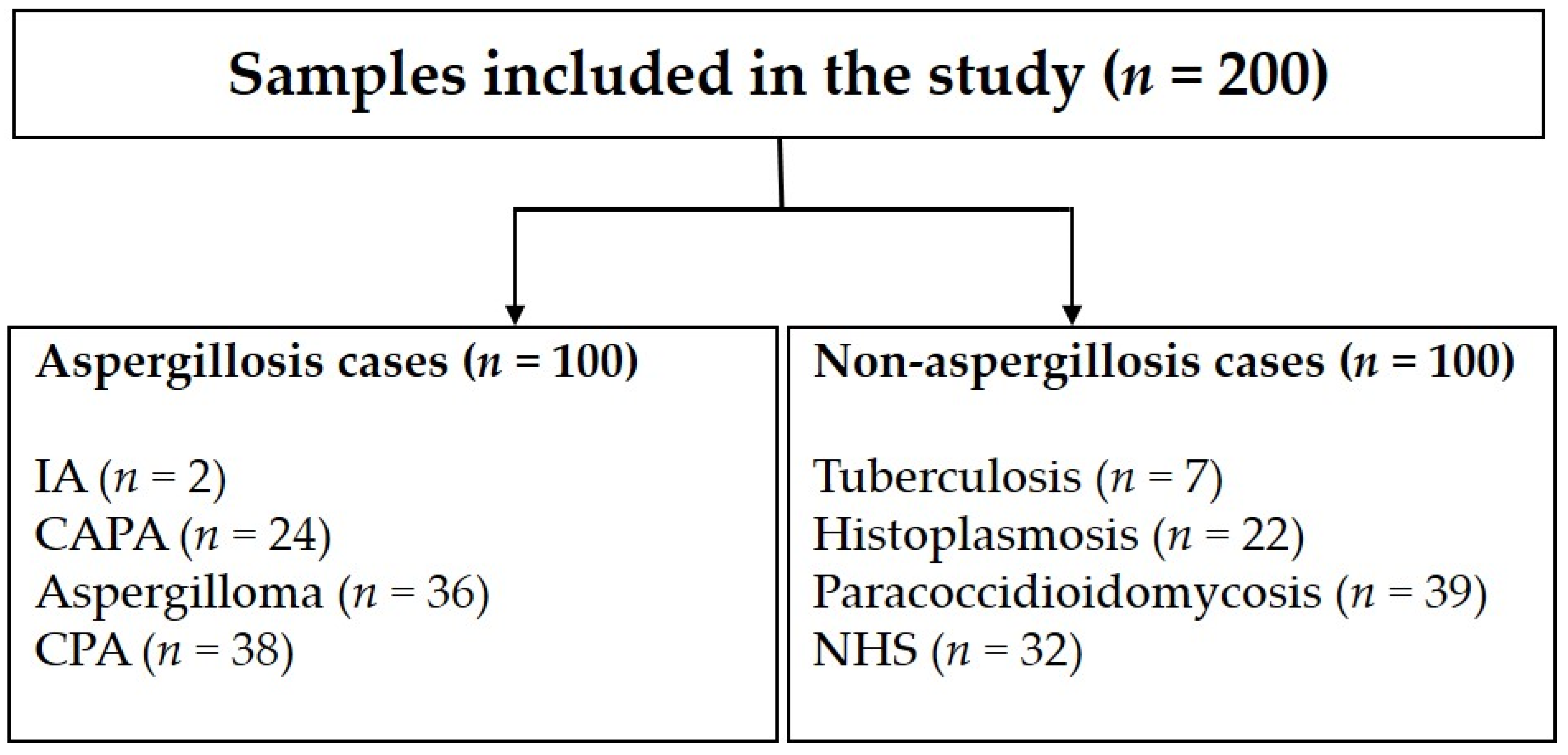
2.1. Study Design, Patients, and Sera
2.2. Case Definitions
2.3. IMMY Sōna AGM Lateral Flow Assay
2.4. Bio-Rad Platelia Sandwich ELISA
2.5. Statistical Analyses
3. Results
3.1. Overall Performance of Individual Assays
3.2. Performance of the Assays in Individuals with Aspergillosis
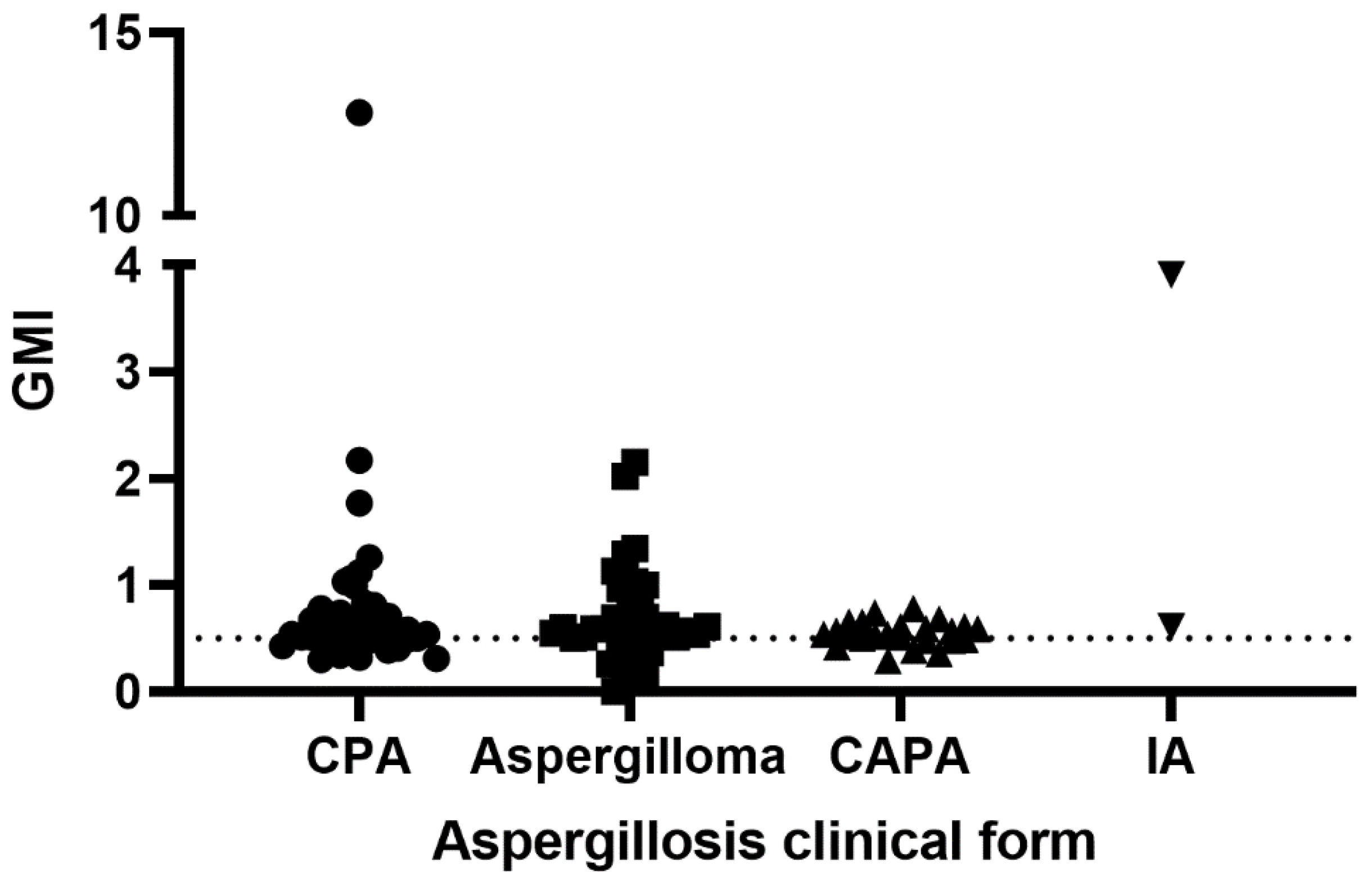
3.2.1. IMMY Sōna AGM Lateral Flow Assay
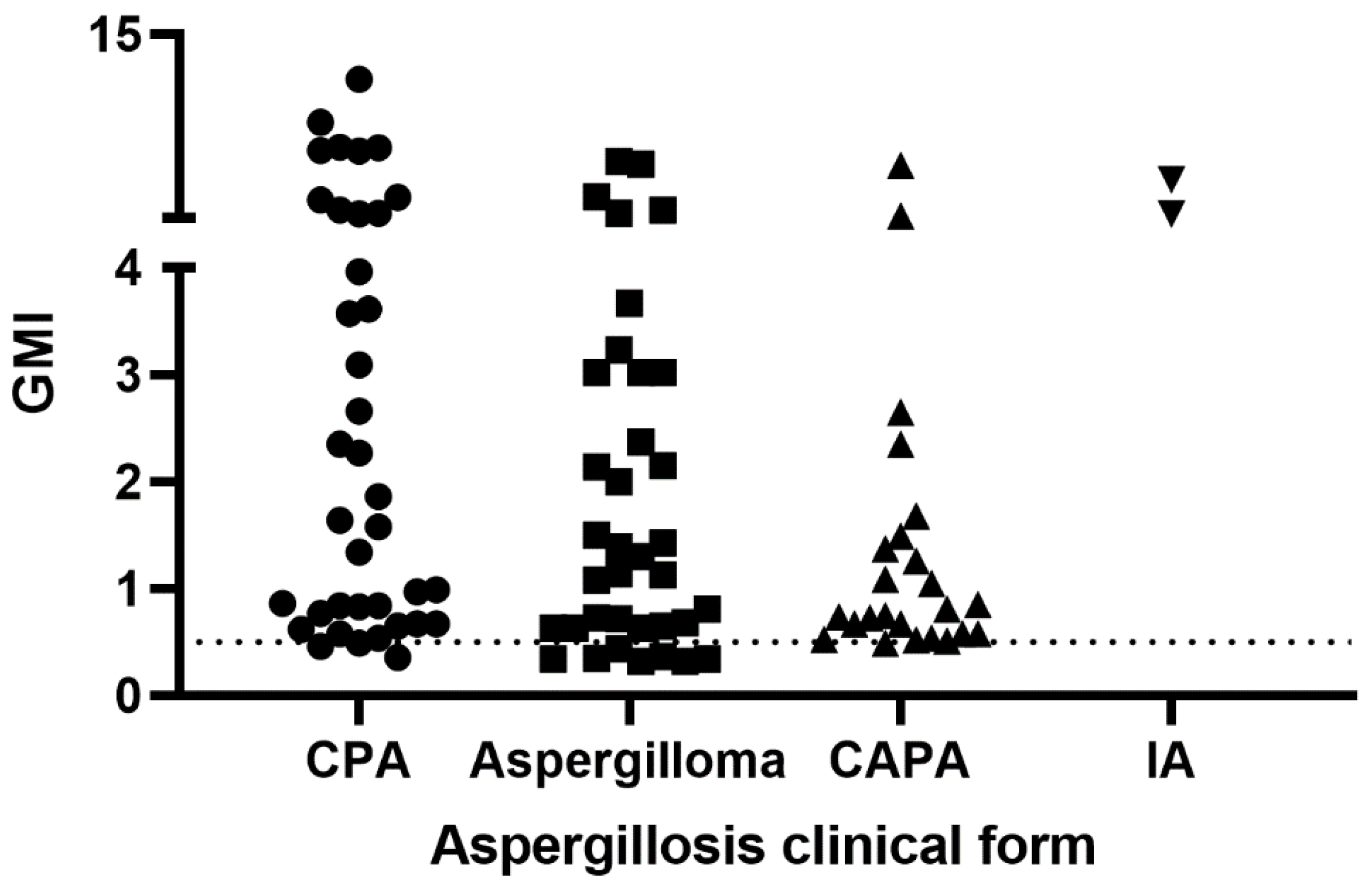
3.2.2. Bio-Rad Platelia Sandwich ELISA
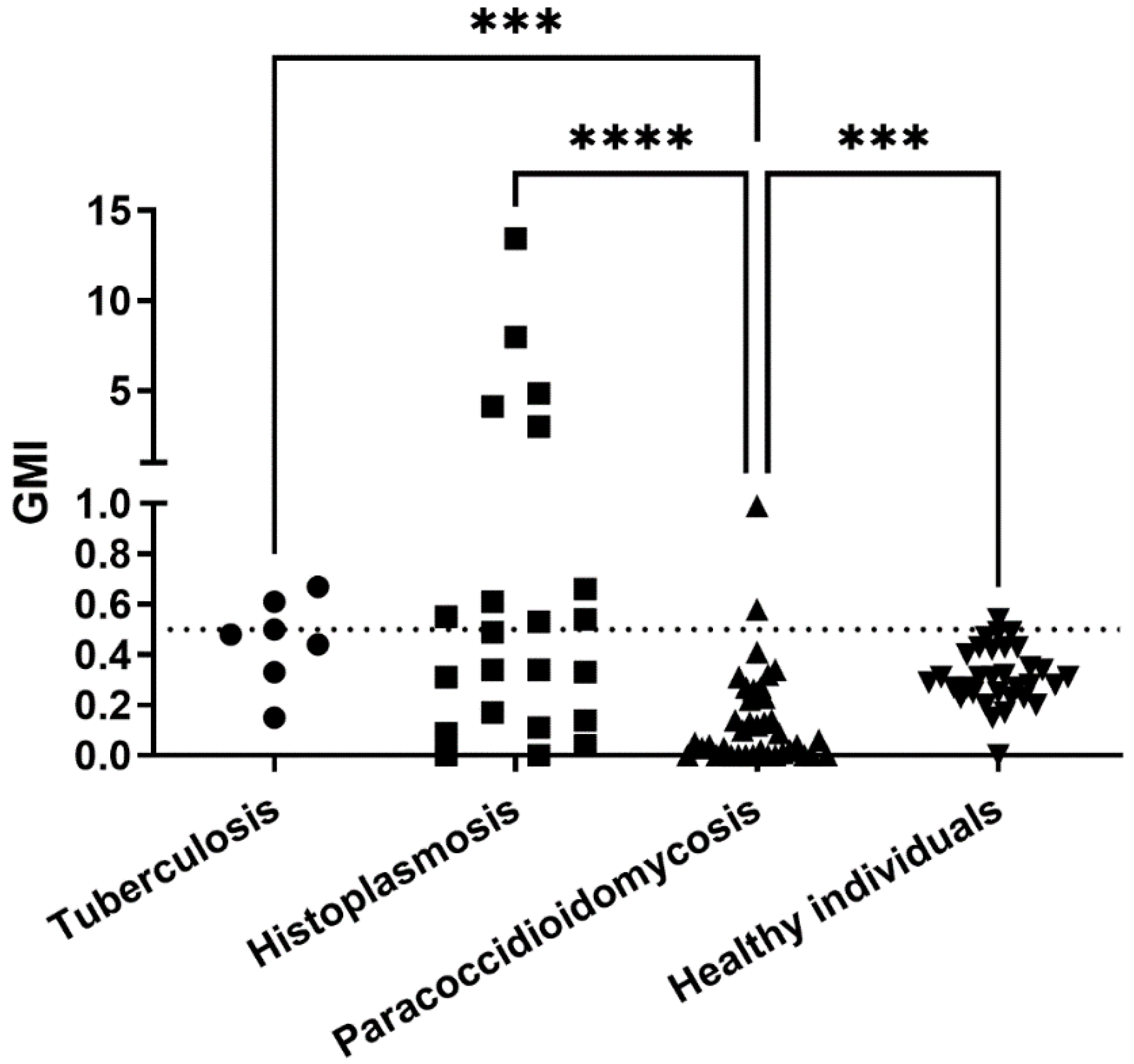
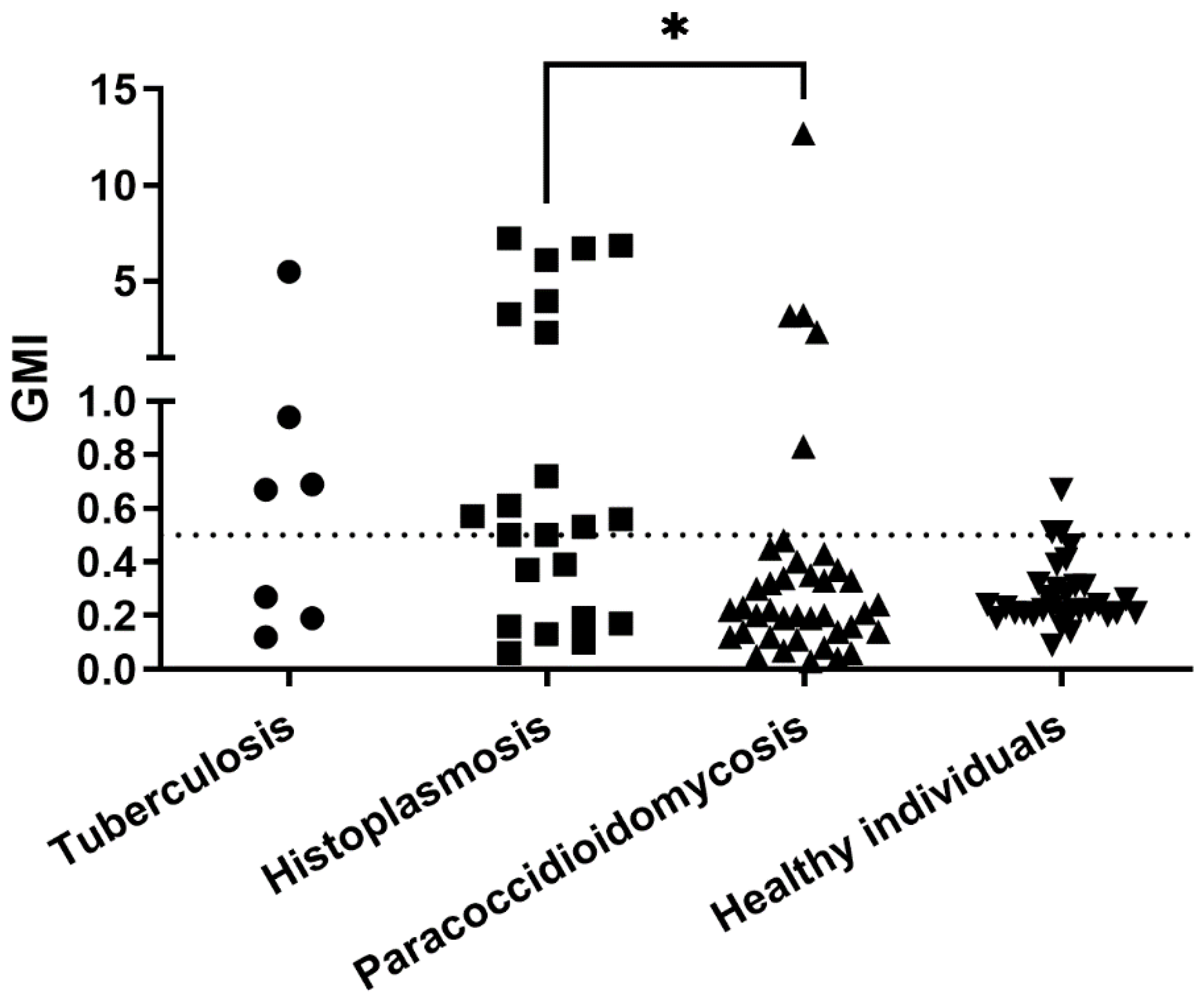
3.3. Performance of the Assays in Individuals without Aspergillosis
3.3.1. IMMY Sōna AGM Lateral Flow Assay
3.3.2. Bio-Rad Platelia Sandwich ELISA
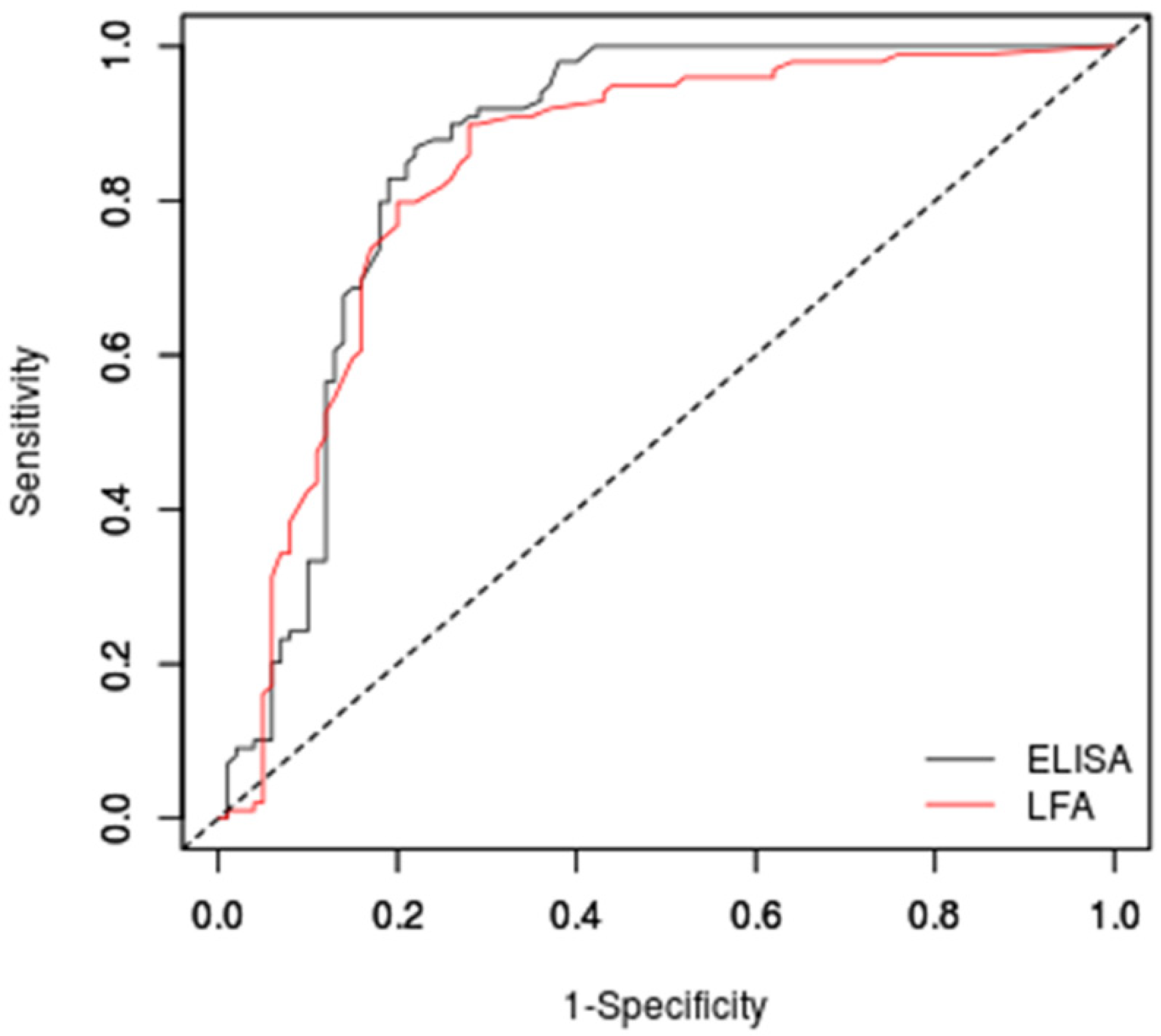
3.4. Receiver Operator Characteristic (ROC)-Based Cut-Off Calculations
3.5. Comparison between Assays
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Latgé, J.-P.; Chamilos, G. Aspergillus fumigatus and Aspergillosis in 2019. Clin. Microbiol. Rev. 2019, 33, e00140-18. [Google Scholar] [CrossRef] [PubMed]
- Hohl, T.M. Immune responses to invasive aspergillosis: New understanding and therapeutic opportunities. Curr. Opin. Infect. Dis. 2017, 30, 364–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ledoux, M.-P.; Guffroy, B.; Nivoix, Y.; Simand, C.; Herbrecht, R. Invasive Pulmonary Aspergillosis. Semin. Respir. Crit. Care Med. 2020, 41, 80–98. [Google Scholar] [CrossRef]
- Costantini, C.; van de Veerdonk, F.L.; Romani, L. Covid-19-Associated Pulmonary Aspergillosis: The Other Side of the Coin. Vaccines 2020, 8, 713. [Google Scholar] [CrossRef]
- Chong, W.H.; Neu, K.P. Incidence, diagnosis and outcomes of COVID-19-associated pulmonary aspergillosis (CAPA): A systematic review. J. Hosp. Infect. 2021, 113, 115–129. [Google Scholar] [CrossRef] [PubMed]
- Patterson, T.F.; Thompson, G.R.; Denning, D.W.; Fishman, J.A.; Hadley, S.; Herbrecht, R.; Kontoyiannis, D.P.; Marr, K.A.; Morrison, V.A.; Nguyen, M.H.; et al. Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2016, 63, e1–e60. [Google Scholar] [CrossRef]
- Miceli, M.H.; Maertens, J. Role of Non-Culture-Based Tests, with an Emphasis on Galactomannan Testing for the Diagnosis of Invasive Aspergillosis. Semin. Respir. Crit. Care Med. 2015, 36, 650–661. [Google Scholar] [CrossRef] [PubMed]
- Xavier, M.O.; Pasqualotto, A.C.; Cardoso, I.C.E.; Severo, L.C. Cross-reactivity of Paracoccidioides brasiliensis, Histoplasma capsulatum, and Cryptococcus species in the commercial Platelia Aspergillus enzyme immunoassay. Clin. Vaccine Immunol. CVI 2009, 16, 132–133. [Google Scholar] [CrossRef] [Green Version]
- Stynen, D.; Goris, A.; Sarfati, J.; Latgé, J.P. A new sensitive sandwich enzyme-linked immunosorbent assay to detect galactofuran in patients with invasive aspergillosis. J. Clin. Microbiol. 1995, 33, 497–500. [Google Scholar] [CrossRef] [Green Version]
- White, P.L.; Price, J.S.; Posso, R.; Cutlan-Vaughan, M.; Vale, L.; Backx, M. Evaluation of the Performance of the IMMY sona Aspergillus Galactomannan Lateral Flow Assay When Testing Serum To Aid in Diagnosis of Invasive Aspergillosis. J. Clin. Microbiol. 2020, 58, e00053-20. [Google Scholar] [CrossRef]
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2020, 71, 1367–1376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koehler, P.; Bassetti, M.; Chakrabarti, A.; Chen, S.C.A.; Colombo, A.L.; Hoenigl, M.; Klimko, N.; Lass-Flörl, C.; Oladele, R.O.; Vinh, D.C.; et al. Defining and managing COVID-19-associated pulmonary aspergillosis: The 2020 ECMM/ISHAM consensus criteria for research and clinical guidance. Lancet Infect. Dis. 2021, 21, e149–e162. [Google Scholar] [CrossRef]
- Goksuluk, D.; Korkmaz, S.; Zararsiz, G.; Karaağaoğlu, A.E. easyROC: An Interactive Web-tool for ROC Curve Analysis Using R Language Environment. R J. 2016, 8, 213–230. [Google Scholar] [CrossRef] [Green Version]
- Robin, C.; Cordonnier, C.; Sitbon, K.; Raus, N.; Lortholary, O.; Maury, S.; Peffault de la Tour, R.; Bretagne, S.; Bastuji-Garin, S.; SAIF (Surveillance des Aspergilloses Invasives en France) and the SFGM-TC (Société Francophone de Greffe de Moelle et de Thérapie Cellulaire) Aspergillus Group. Mainly Post-Transplant Factors Are Associated with Invasive Aspergillosis after Allogeneic Stem Cell Transplantation: A Study from the Surveillance des Aspergilloses Invasives en France and Société Francophone de Greffe de Moelle et de Thérapie Cellulaire. Biol. Blood Marrow Transplant. J. Am. Soc. Blood Marrow Transplant. 2019, 25, 354–361. [Google Scholar] [CrossRef] [Green Version]
- Pazos, C.; del Palacio, A. Diagnóstico temprano de aspergilosis invasiva en pacientes neutropénicos con detección seriada quincenal de galactomanano circulante por Platelia Aspergillus. Rev. Iberoam. Micol. 2003, 20, 99–102. [Google Scholar]
- Jenks, J.D.; Hoenigl, M. Point-of-care diagnostics for invasive aspergillosis: Nearing the finish line. Expert Rev. Mol. Diagn. 2020, 20, 1009–1017. [Google Scholar] [CrossRef]
- Dobias, R.; Jaworska, P.; Tomaskova, H.; Kanova, M.; Lyskova, P.; Vrba, Z.; Holub, C.; Svobodová, L.; Hamal, P.; Raska, M. Diagnostic value of serum galactomannan, (1,3)-β-d-glucan, and Aspergillus fumigatus-specific IgA and IgG assays for invasive pulmonary aspergillosis in non-neutropenic patients. Mycoses 2018, 61, 576–586. [Google Scholar] [CrossRef]
- Zhou, W.; Li, H.; Zhang, Y.; Huang, M.; He, Q.; Li, P.; Zhang, F.; Shi, Y.; Su, X. Diagnostic Value of Galactomannan Antigen Test in Serum and Bronchoalveolar Lavage Fluid Samples from Patients with Nonneutropenic Invasive Pulmonary Aspergillosis. J. Clin. Microbiol. 2017, 55, 2153–2161. [Google Scholar] [CrossRef] [Green Version]
- Takazono, T.; Saijo, T.; Ashizawa, N.; Oshima, K.; Nishimura, K.; Tashiro, M.; Yamamoto, K.; Imamura, Y.; Miyazaki, T.; Yanagihara, K.; et al. Clinical features and cause analysis of false positive results of Aspergillus galactomannan assay in pulmonary cryptococcosis patients. Eur. J. Clin. Microbiol. Infect. Dis. Off. Publ. Eur. Soc. Clin. Microbiol. 2019, 38, 735–741. [Google Scholar] [CrossRef]
- Tortorano, A.M.; Esposto, M.C.; Prigitano, A.; Grancini, A.; Ossi, C.; Cavanna, C.; Cascio, G.L. Cross-reactivity of Fusarium spp. in the Aspergillus Galactomannan enzyme-linked immunosorbent assay. J. Clin. Microbiol. 2012, 50, 1051–1053. [Google Scholar] [CrossRef] [Green Version]
- Van Der Veer, J.; Lewis, R.J.; Emtiazjoo, A.M.; Allen, S.D.; Wheat, L.J.; Hage, C.A. Cross-reactivity in the PlateliaTM Aspergillus enzyme immunoassay caused by blastomycosis. Med. Mycol. 2012, 50, 396–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ranque, S.; Pelletier, R.; Michel-Nguyen, A.; Dromer, F. Platelia Aspergillus assay for diagnosis of disseminated histoplasmosis. Eur. J. Clin. Microbiol. Infect. Dis. Off. Publ. Eur. Soc. Clin. Microbiol. 2007, 26, 941–943. [Google Scholar] [CrossRef] [PubMed]
- Iriart, X.; Blanchet, D.; Menard, S.; Lavergne, R.-A.; Chauvin, P.; Adenis, A.; Cassaing, S.; Fillaux, J.; Magnaval, J.-F.; Demar, M.; et al. A complementary tool for management of disseminated Histoplasma capsulatum var. capsulatum infections in AIDS patients. Int. J. Med. Microbiol. IJMM 2014, 304, 1062–1065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Macedo, P.M.; Freitas, A.D.; Bártholo, T.P.; Bernardes-Engemann, A.R.; de Almeida, M.A.; Almeida-Silva, F.; Zancopé-Oliveira, R.M.; Almeida-Paes, R. Acute Pulmonary Histoplasmosis Following COVID-19: Novel Laboratorial Methods Aiding Diagnosis. J. Fungi 2021, 7, 346. [Google Scholar] [CrossRef] [PubMed]
- Vergidis, P.; Walker, R.C.; Kaul, D.R.; Kauffman, C.A.; Freifeld, A.G.; Slagle, D.C.; Kressel, A.B.; Wheat, L.J. False-positive Aspergillus galactomannan assay in solid organ transplant recipients with histoplasmosis. Transpl. Infect. Dis. Off. J. Transplant. Soc. 2012, 14, 213–217. [Google Scholar] [CrossRef] [Green Version]
- Hosseini, M.; Shakerimoghaddam, A.; Ghazalibina, M.; Khaledi, A. Aspergillus coinfection among patients with pulmonary tuberculosis in Asia and Africa countries; A systematic review and meta-analysis of cross-sectional studies. Microb. Pathog. 2020, 141, 104018. [Google Scholar] [CrossRef]
- Shah, A. Allergic bronchopulmonary and sinus aspergillosis: The roentgenologic spectrum. Front. Biosci. J. Virtual Libr. 2003, 8, e138–e146. [Google Scholar] [CrossRef] [Green Version]
- Binder, R.E.; Faling, L.J.; Pugatch, R.D.; Mahasaen, C.; Snider, G.L. Chronic necrotizing pulmonary aspergillosis: A discrete clinical entity. Medicine 1982, 61, 109–124. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Performance Parameter | Lateral Flow Assay | Sandwich ELISA | ||
|---|---|---|---|---|
| Value | 95% CI a | Value | 95% CI | |
| Sensitivity | 74% | 64.27–82.26% | 89% | 81.17–94.38% |
| Specificity | 84% | 75.32–90.57% | 75% | 65.34–83.12% |
| Accuracy | 79% | 72.69–84.43% | 82% | 75.96–87.06% |
| Positive Likelihood Ratio | 4.62 | 2.91–7.35 | 3.56 | 2.52–5.03 |
| Negative Likelihood Ratio | 0.31 | 0.22–0.44 | 0.15 | 0.08–0.26 |
| Performance Parameter | ROC Based Cut-Off Value | ||
|---|---|---|---|
| 0.36 | 0.48 | 0.48 | |
| Sensitivity (95% CI) | 90% (82.2–95%) | 80% (70.8–87.3%) | 80% (70.8–87.3%) |
| Specificity (95% CI) | 72% (62.1–80.5%) | 80% (70.8–87.3%) | 80% (70.8–87.3%) |
| Accuracy (95% CI) | 81% (74.9–86.2%) | 80% (73.8–85.3%) | 80% (73.8–85.3%) |
| Positive Likelihood Ratio (95% CI) | 3.211 (2.329–4.427) | 3.990 (2.663–5.978) | 3.990 (2.663–5.978) |
| Negative Likelihood Ratio (95% CI) | 0.140 (0.077–0.256) | 0.253 (0.169–0.378) | 0.253 (0.169–0.378) |
| Performance Parameter | ROC Based Cut-Off Value | ||
|---|---|---|---|
| 0.52 | 0.58 | 0.61 | |
| Sensitivity (95% CI) | 87% (78.8–92.9%) | 83% (74.2–89.8%) | 80% (70.8–87.3%) |
| Specificity (95% CI) | 78% (68.6–85.7%) | 81% (71.9–88.2%) | 81% (71.9–88.2%) |
| Accuracy (95% CI) | 82.5% (76.5–87.5%) | 82% (76–87.1%) | 80,5% (74.3–85.8%) |
| Positive Likelihood Ratio (95% CI) | 3.955 (2.713–5.764) | 4.368 (2.887–6.611) | 4.211 (2.777–6.385) |
| Negative Likelihood Ratio (95% CI) | 0.167 (0.099–0.280) | 0.210 (0.135–0.327) | 0.247 (0.165–0.370) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almeida-Paes, R.; Almeida, M.d.A.; de Macedo, P.M.; Caceres, D.H.; Zancopé-Oliveira, R.M. Performance of Two Commercial Assays for the Detection of Serum Aspergillus Galactomannan in Non-Neutropenic Patients. J. Fungi 2022, 8, 741. https://0-doi-org.brum.beds.ac.uk/10.3390/jof8070741
Almeida-Paes R, Almeida MdA, de Macedo PM, Caceres DH, Zancopé-Oliveira RM. Performance of Two Commercial Assays for the Detection of Serum Aspergillus Galactomannan in Non-Neutropenic Patients. Journal of Fungi. 2022; 8(7):741. https://0-doi-org.brum.beds.ac.uk/10.3390/jof8070741
Chicago/Turabian StyleAlmeida-Paes, Rodrigo, Marcos de Abreu Almeida, Priscila Marques de Macedo, Diego H. Caceres, and Rosely Maria Zancopé-Oliveira. 2022. "Performance of Two Commercial Assays for the Detection of Serum Aspergillus Galactomannan in Non-Neutropenic Patients" Journal of Fungi 8, no. 7: 741. https://0-doi-org.brum.beds.ac.uk/10.3390/jof8070741