
Novel Hypertrophic Cardiomyopathy Diagnosis Index Using Deep Features and Local Directional Pattern Techniques

 , , , and
, , , and
Abstract
:1. Introduction
- Established databanks of four-chamber US images of normal and HCM subjects;
- Created deep features by combining local texture featured images with deep neural networks; and
- Generated an integrated index to categorize normal versus HCM using a distinctive number.
2. Materials
3. Methodology
3.1. Preprocessing
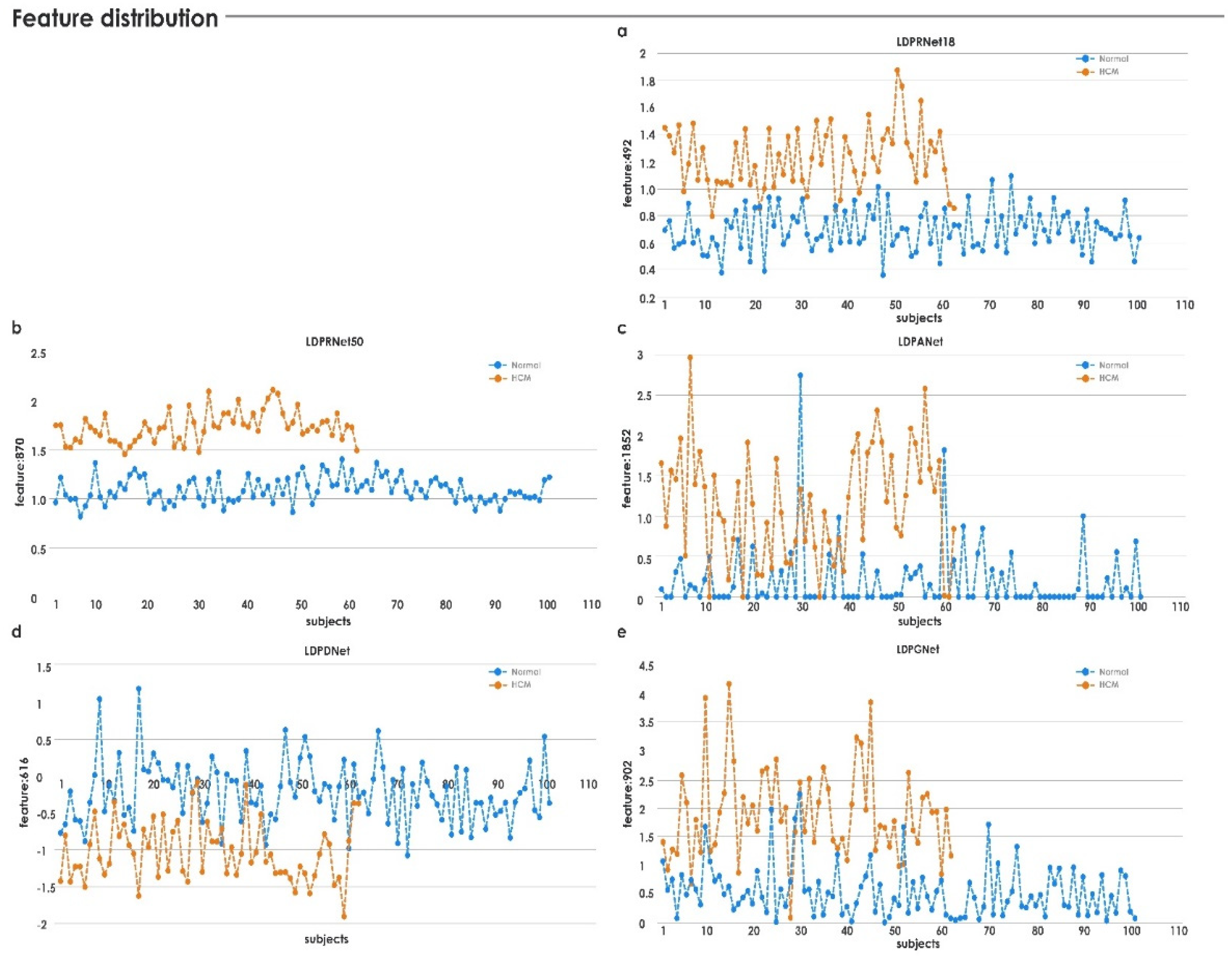
3.2. Feature Generation
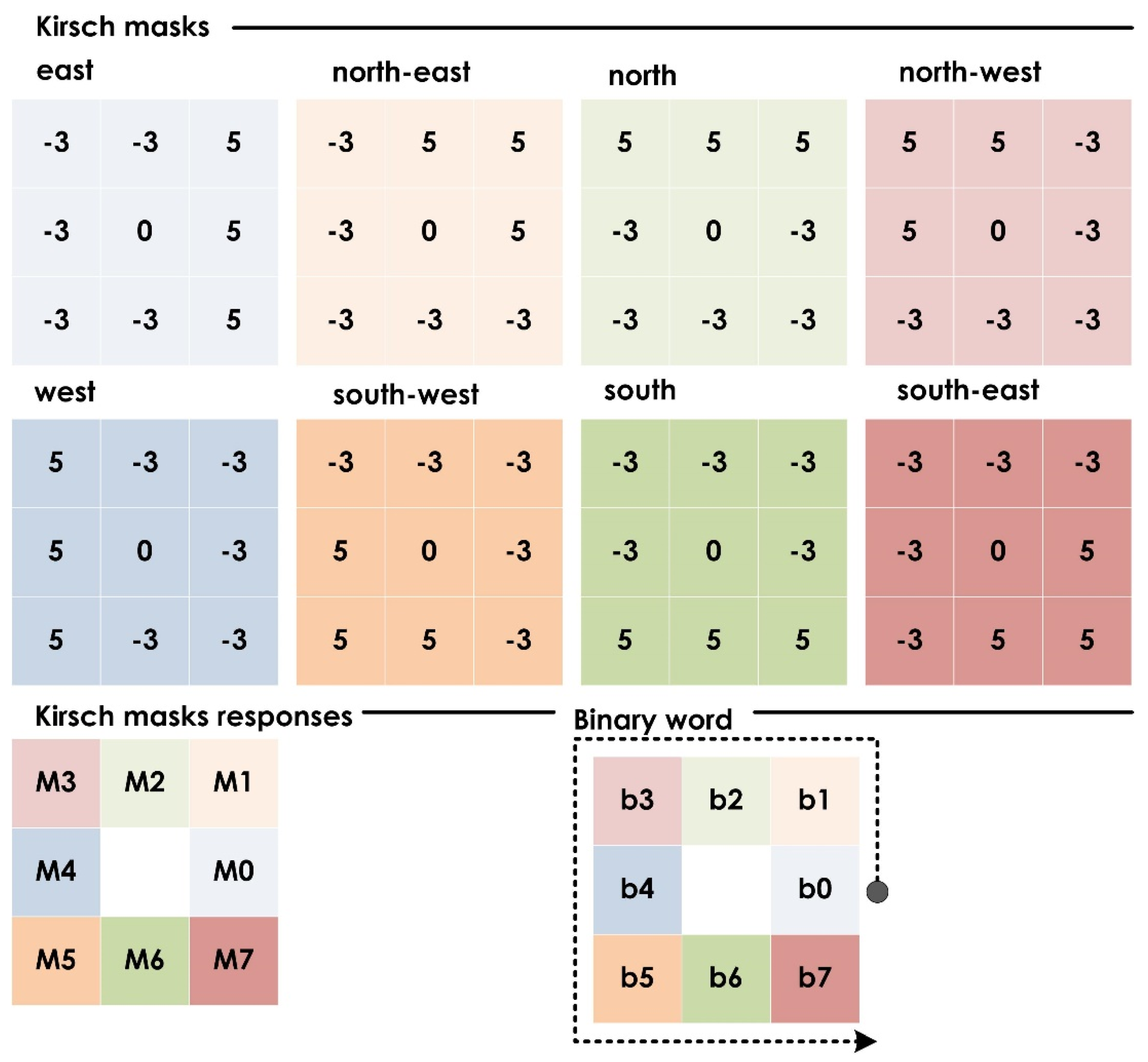
3.2.1. Local Directional Pattern (LDP)
3.2.2. Deep-Learning Model
3.3. Feature Selection
3.4. Classification
4. Experimental Results
Comparative Study
5. Discussion
- An integrated index based on heart US image features was developed that could effectively discriminate for HCM subjects.
- The use of a single distinct value simplified the classification and should garner early clinical adoption, especially in rural and semiurban areas where access to experienced US operators may be limited.
- The proposed framework can be generalized to image analysis of other imaging modalities and/or other anatomical regions; e.g., fundus images, brain magnetic resonance imaging, etc.
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tsoutsman, T.; Lam, L.; Semsarian, C. Genes, Calcium and Modifying Factors in Hypertrophic CardiomyopathY. Clin. Exp. Pharmacol. Physiol. 2006, 33, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Marian, A. Pathogenesis of diverse clinical and pathological phenotypes in hypertrophic cardiomyopathy. Lancet 2000, 355, 58–60. [Google Scholar] [CrossRef]
- Elliott, P.; Charron, P.; Blanes, J.R.G.; Tavazzi, L.; Tendera, M.; Konté, M.; Laroche, C.; Maggioni, A.P. European Cardiomyopathy Pilot Registry: EURObservational Research Programme of the European Society of Cardiology. Eur. Heart J. 2015, 37, 164–173. [Google Scholar] [CrossRef]
- Tucholski, T.; Cai, W.; Gregorich, Z.R.; Bayne, E.F.; Mitchell, S.D.; McIlwain, S.J.; de Lange, W.J.; Wrobbel, M.; Karp, H.; Hite, Z.; et al. Distinct hypertrophic cardiomyopathy genotypes result in convergent sarcomeric proteoform profiles revealed by top-down proteomics. Proc. Natl. Acad. Sci. USA 2020, 117, 24691–24700. [Google Scholar] [CrossRef]
- Rowin, E.J.; Maron, M.S.; Chan, R.H.; Hausvater, A.; Wang, W.; Rastegar, H.; Maron, B.J. Interaction of Adverse Disease Related Pathways in Hypertrophic Cardiomyopathy. Am. J. Cardiol. 2017, 120, 2256–2264. [Google Scholar] [CrossRef]
- Maron, B.J.; Thompson, P.D.; Ackerman, M.J.; Balady, G.; Berger, S.; Cohen, D.; Dimeff, R.; Douglas, P.S.; Glover, D.W.; Hutter, A.M.; et al. Recommendations and Considerations Related to Preparticipation Screening for Cardiovascular Abnormalities in Competitive Athletes: 2007 Update. Circulation 2007, 115, 1643–1655. [Google Scholar] [CrossRef] [Green Version]
- Elliott, P.M.; Anastasakis, A.; Borger, M.A.; Borggrefe, M.; Cecchi, F.; Charron, P.; Hagege, A.A.; Lafont, A.; Limongelli, G.; Mahrholdt, H.; et al. 2014 ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy: The Task Force for the Diagnosis and Management of Hypertrophic Cardiomyopathy of the European Society of Cardiology (ESC). Eur. Heart J. 2014, 35, 2733–2779. [Google Scholar] [CrossRef]
- O’Mahony, C.; Jichi, F.; Pavlou, M.; Monserrat, L.; Anastasakis, A.; Rapezzi, C.; Biagini, E.; Gimeno, J.R.; Limongelli, G.; McKenna, W.J.; et al. A novel clinical risk prediction model for sudden cardiac death in hypertrophic cardiomyopathy (HCM Risk-SCD). Eur. Heart J. 2013, 35, 2010–2020. [Google Scholar] [CrossRef]
- Pantazis, A.; Vischer, A.S.; Perez-Tome, M.C.; Castelletti, S. Diagnosis and management of hypertrophic cardiomyopathy. Echo Res. Pract. 2015, 2, R45–R53. [Google Scholar] [CrossRef] [Green Version]
- Antunes, M.D.O.; Scudeler, T.L. Hypertrophic cardiomyopathy. IJC Heart Vasc. 2020, 27, 100503. [Google Scholar] [CrossRef]
- Shetty, R. Evaluation of Subtle Left Ventricular Systolic Abnormalities in Adult Patients with Hypertrophic Cardiomyopathy. J. Clin. Diagn. Res. 2014, 8, MC05–MC09. [Google Scholar] [CrossRef] [PubMed]
- Jahmunah, V.; Oh, S.L.; Wei, J.K.E.; Ciaccio, E.J.; Chua, K.; San, T.R.; Acharya, U.R. Computer-aided diagnosis of congestive heart failure using ECG signals—A review. Phys. Medica 2019, 62, 95–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sudarshan, V.; Acharya, U.R.; Ng, E.Y.-K.; Meng, C.S.; Tan, R.S.; Ghista, D.N. Automated Identification of Infarcted Myocardium Tissue Characterization Using Ultrasound Images: A Review. IEEE Rev. Biomed. Eng. 2014, 8, 86–97. [Google Scholar] [CrossRef] [PubMed]
- Kusunose, K. Radiomics in Echocardiography: Deep Learning and Echocardiographic Analysis. Curr. Cardiol. Rep. 2020, 22, 89. [Google Scholar] [CrossRef]
- Raghavendra, U.; Acharya, U.R.; Gudigar, A.; Shetty, R.; Krishnananda, N.; Pai, U.; Samanth, J.; Nayak, C. Automated screening of congestive heart failure using variational mode decomposition and texture features extracted from ultrasound images. Neural Comput. Appl. 2017, 28, 2869–2878. [Google Scholar] [CrossRef]
- Raghavendra, U.; Fujita, H.; Gudigar, A.; Shetty, R.; Nayak, K.; Pai, U.; Samanth, J.; Acharya, U. Automated technique for coronary artery disease characterization and classification using DD-DTDWT in ultrasound images. Biomed. Signal Process. Control 2018, 40, 324–334. [Google Scholar] [CrossRef]
- Gudigar, A.; Raghavendra, U.; Devasia, T.; Nayak, K.; Danish, S.M.; Kamath, G.; Samanth, J.; Pai, U.M.; Nayak, V.; Tan, R.S.; et al. Global weighted LBP based entropy features for the assessment of pulmonary hypertension. Pattern Recognit. Lett. 2019, 125, 35–41. [Google Scholar] [CrossRef]
- Gudigar, A.; Samanth, J.; Raghavendra, U.; Dharmik, C.; Vasudeva, A.; Padmakumar, R.; Tan, R.-S.; Ciaccio, E.J.; Molinari, F.; Acharya, U.R. Local Preserving Class Separation Framework to Identify Gestational Diabetes Mellitus Mother Using Ultrasound Fetal Cardiac Image. IEEE Access 2020, 8, 229043–229051. [Google Scholar] [CrossRef]
- Balaji, G.; Subashini, T.; Chidambaram, N. Detection and diagnosis of dilated cardiomyopathy and hypertrophic cardiomyopathy using image processing techniques. Eng. Sci. Technol. Int. J. 2016, 19, 1871–1880. [Google Scholar] [CrossRef] [Green Version]
- Sharon, J.J.; Anbarasi, L.J.; Raj, B.E. DPSO-FCM based segmentation and Classification of DCM and HCM Heart Diseases. In Proceedings of the 2018 Fifth HCT Information Technology Trends (ITT), Dubai, United Arab Emirates, 28–29 November 2018; pp. 41–46. [Google Scholar] [CrossRef]
- Zhang, J.; Gajjala, S.; Agrawal, P.; Tison, G.H.; Hallock, L.A.; Beussink-Nelson, L.; Lassen, M.H.; Fan, E.; Aras, M.A.; Jordan, C.; et al. Fully automated echocardiogram interpretation in clinical practice:feasibility and diagnostic accuracy. Circulation 2018, 138, 1623–1635. [Google Scholar] [CrossRef]
- Yu, F.; Huang, H.; Yu, Q.; Ma, Y.; Zhang, Q.; Zhang, B. Artificial intelligence-based myocardial texture analysis in etiological differentiation of left ventricular hypertrophy. Ann. Transl. Med. 2021, 9, 108. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Agrawal, M.; Roy, S.D.; Gupta, V.; Vashisht, P.; Sidhu, T. Deep learning to diagnose Peripapillary Atrophy in retinal images along with statistical features. Biomed. Signal Process. Control 2020, 64, 102254. [Google Scholar] [CrossRef]
- Raghavendra, U.; Fujita, H.; Bhandary, S.V.; Gudigar, A.; Tan, J.H.; Acharya, U.R. Deep convolution neural network for accurate diagnosis of glaucoma using digital fundus images. Inf. Sci. 2018, 441, 41–49. [Google Scholar] [CrossRef]
- Acharya, U.R.; Fujita, H.; Oh, S.L.; Raghavendra, U.; Tan, J.H.; Adam, M.; Gertych, A.; Hagiwara, Y. Automated identification of shockable and non-shockable life-threatening ventricular arrhythmias using convolutional neural network. Futur. Gener. Comput. Syst. 2018, 79, 952–959. [Google Scholar] [CrossRef]
- Tan, J.H.; Bhandary, S.; Sivaprasad, S.; Hagiwara, Y.; Bagchi, A.; Raghavendra, U.; Rao, A.K.; Raju, B.; Shetty, N.S.; Gertych, A.; et al. Age-related Macular Degeneration detection using deep convolutional neural network. Future Gener. Comput. Syst. 2018, 87, 127–135. [Google Scholar] [CrossRef]
- Pan, S.J.; Yang, Q. A Survey on Transfer Learning. IEEE Trans. Knowl. Data Eng. 2010, 22, 1345–1359. [Google Scholar] [CrossRef]
- Jabid, T.; Kabir, H.; Chae, O. Gender Classification Using Local Directional Pattern (LDP). In Proceedings of the 2010 20th International Conference on Pattern Recognition, Istanbul, Turkey, 23–26 August 2010; pp. 2162–2165. [Google Scholar] [CrossRef]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016. [Google Scholar]
- Keys, R. Cubic convolution interpolation for digital image processing. IEEE Trans. Acoust. Speech Signal Process. 1981, 29, 1153–1160. [Google Scholar] [CrossRef] [Green Version]
- ImageNet. Available online: http://www.image-net.org/ (accessed on 17 March 2021).
- Acharya, U.R.; Oh, S.L.; Hagiwara, Y.; Tan, J.H.; Adeli, H. Deep convolutional neural network for the automated detection and diagnosis of seizure using EEG signals. Comput. Biol. Med. 2018, 100, 270–278. [Google Scholar] [CrossRef]
- Chu, Y.; Yue, X.; Yu, L.; Sergei, M.; Wang, Z. Automatic Image Captioning Based on ResNet50 and LSTM with Soft Attention. Wirel. Commun. Mob. Comput. 2020, 2020, 8909458. [Google Scholar] [CrossRef]
- Chougrad, H.; Zouaki, H.; Alheyane, O. Deep Convolutional Neural Networks for breast cancer screening. Comput. Methods Programs Biomed. 2018, 157, 19–30. [Google Scholar] [CrossRef]
- Theckedath, D.; Sedamkar, R.R. Detecting Affect States Using VGG16, ResNet50 and SE-ResNet50 Networks. SN Comput. Sci. 2020, 1, 79. [Google Scholar] [CrossRef] [Green Version]
- Altaf, F.; Islam, S.M.S.; Janjua, N.K. A novel augmented deep transfer learning for classification of COVID-19 and other thoracic diseases from X-rays. Neural Comput. Appl. 2021, 33, 14037–14048. [Google Scholar] [CrossRef] [PubMed]
- Al-Antari, M.A.; Han, S.-M.; Kim, T.-S. Evaluation of deep learning detection and classification towards computer-aided diagnosis of breast lesions in digital X-ray mammograms. Comput. Methods Programs Biomed. 2020, 196, 105584. [Google Scholar] [CrossRef] [PubMed]
- Luo, W.; Liu, J.; Huang, Y.; Zhao, N. An effective vitiligo intelligent classification system. J. Ambient Intell. Humaniz. Comput. 2020, 1–10. [Google Scholar] [CrossRef]
- Hong, J.; Cheng, H.; Zhang, Y.-D.; Liu, J. Detecting cerebral microbleeds with transfer learning. Mach. Vis. Appl. 2019, 30, 1123–1133. [Google Scholar] [CrossRef]
- Tajbakhsh, N.; Shin, J.Y.; Gurudu, S.R.; Hurst, R.T.; Kendall, C.B.; Gotway, M.B.; Liang, J. Convolutional Neural Networks for Medical Image Analysis: Full Training or Fine Tuning? IEEE Trans. Med. Imaging 2016, 35, 1299–1312. [Google Scholar] [CrossRef] [Green Version]
- Jason, Y.; Jeff, C.; Bengio, Y.; Lipson, H. How transferable are features in deep neural networks? Adv. Neural Inf. Processing Syst. (NIPS) 2014, 27. [Google Scholar]
- Zhou, N.; Wang, L. A Modified T-test Feature Selection Method and Its Application on the HapMap Genotype Data. Genom. Proteom. Bioinform. 2007, 5, 242–249. [Google Scholar] [CrossRef] [Green Version]
- Aslam, M.W.; Zhu, Z.; Nandi, A.K. Feature generation using genetic programming with comparative partner selection for diabetes classification. Expert Syst. Appl. 2013, 40, 5402–5412. [Google Scholar] [CrossRef]
- Glen, S. T Test (Student’s T-Test): Definition and Examples. 2020. Available online: https://www.statisticshowto.com/probability-and-statistics/t-test/ (accessed on 6 December 2020).
- Specht, D.F. Probabilistic neural networks. Neural. Netw. 1990, 3, 109–118. [Google Scholar] [CrossRef]
- Kecman, V. Learning and Soft Computing; MIT Press: Cambridge, UK, 2001. [Google Scholar]
- Hastie, T.; Tibshirani, R.; Friedman, J. The Elements of Statistical Learning, 2nd ed.; Springer: New York, NY, USA, 2008. [Google Scholar]
- Christianini, N.; Shawe-Taylor, J. An introduction to Support Vector Machines and Other Kernel-Based Learning Methods; Cambridge University Press: Cambridge, UK, 2000. [Google Scholar]
- Han, J.; Pei, J.; Kamber, M. Data Mining: Concepts and Techniques; Elsevier: Amsterdam, The Netherland, 2011. [Google Scholar]
- Acharya, U.R.; Fujita, H.; Sudarshan, V.K.; Sree, V.S.; Eugene, L.W.J.; Ghista, D.N.; Tan, R.S. An integrated index for detection of Sudden Cardiac Death using Discrete Wavelet Transform and nonlinear features. Knowl.-Based Syst. 2015, 83, 149–158. [Google Scholar] [CrossRef]
- Ghista, D.N. Nondimensional physiological indices for medical assessment. J. Mech. Med. Biol. 2009, 9, 643–669. [Google Scholar] [CrossRef]
- Acharya, U.R.; Raghavendra, U.; Fujita, H.; Hagiwara, Y.; Koh, J.E.; Hong, T.J.; Sudarshan, V.K.; Vijayananthan, A.; Yeong, C.H.; Gudigar, A.; et al. Automated characterization of fatty liver disease and cirrhosis using curvelet transform and entropy features extracted from ultrasound images. Comput. Biol. Med. 2016, 79, 250–258. [Google Scholar] [CrossRef] [PubMed]
- Fujita, H.; Acharya, U.R.; Sudarshan, V.K.; Ghista, D.N.; Sree, S.V.; Eugene, L.W.J.; Koh, J.E. Sudden cardiac death (SCD) prediction based on nonlinear heart rate variability features and SCD index. Appl. Soft Comput. 2016, 43, 510–519. [Google Scholar] [CrossRef]
- Acharya, U.R.; Fujita, H.; Sudarshan, V.K.; Mookiah, M.R.K.; Koh, J.E.; Tan, J.H.; Hagiwara, Y.; Chua, C.K.; Junnarkar, S.P.; Vijayananthan, A.; et al. An integrated index for identification of fatty liver disease using radon transform and discrete cosine transform features in ultrasound images. Inf. Fusion 2016, 31, 43–53. [Google Scholar] [CrossRef]
- Raghavendra, U.; Acharya, U.R.; Ng, E.Y.K.; Tan, J.-H.; Gudigar, A. An integrated index for breast cancer identification using histogram of oriented gradient and kernel locality preserving projection features extracted from thermograms. Quant. Infrared Thermogr. J. 2016, 13, 195–209. [Google Scholar] [CrossRef]
- Sharma, R.; Pachori, R.B.; Acharya, U.R. An Integrated Index for the Identification of Focal Electroencephalogram Signals Using Discrete Wavelet Transform and Entropy Measures. Entropy 2015, 17, 5218–5240. [Google Scholar] [CrossRef] [Green Version]
- Raghavendra, U.; Acharya, U.R.; Gudigar, A.; Tan, J.H.; Fujita, H.; Hagiwara, Y.; Molinari, F.; Kongmebhol, P.; Ng, K.H. Fusion of spatial gray level dependency and fractal texture features for the characterization of thyroid lesions. Ultrasonics 2017, 77, 110–120. [Google Scholar] [CrossRef]
- Pham, T.-H.; Raghavendra, U.; Koh, J.E.W.; Gudigar, A.; Chan, W.Y.; Hamid, M.T.R.; Rahmat, K.; Fadzli, F.; Ng, K.H.; Ooi, C.P.; et al. Development of breast papillary index for differentiation of benign and malignant lesions using ultrasound images. J. Ambient Intell. Humaniz. Comput. 2020, 12, 2121–2129. [Google Scholar] [CrossRef]
- Acharya, U.R.; Mookiah, M.R.K.; Koh, J.E.; Tan, J.H.; Noronha, K.; Bhandary, S.; Rao, A.K.; Hagiwara, Y.; Chua, C.K.; Laude, A. Novel risk index for the identification of age-related macular degeneration using radon transform and DWT features. Comput. Biol. Med. 2016, 73, 131–140. [Google Scholar] [CrossRef]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. Imagenet classification with deep convolutional neural networks. NIPS 2012, 60, 84–90. [Google Scholar] [CrossRef]
- Redmon, J. 2013–2016 “Darknet: Open Source Neural Networks in C”. Available online: https://pjreddie.com/darknet (accessed on 13 October 2021).
- BVLC GoogLeNet Model. Available online: https://github.com/BVLC/caffe/tree/master/models/bvlc_googlenet (accessed on 13 October 2021).
- Raghavendra, U.; Gudigar, A.; Rao, T.N.; Rajinikanth, V.; Ciaccio, E.J.; Yeong, C.H.; Satapathy, S.C.; Molinari, F.; Acharya, U.R. Feature-versus deep learning-based approaches for the automated detection of brain tumor with magnetic resonance images: A comparative study. Int. J. Imaging Syst. Technol. 2021, 32, 501–516. [Google Scholar] [CrossRef]
- Vafaeezadeh, M.; Behnam, H.; Hosseinsabet, A.; Gifani, P. A deep learning approach for the automatic recognition of prosthetic mitral valve in echocardiographic images. Comput. Biol. Med. 2021, 133, 104388. [Google Scholar] [CrossRef] [PubMed]
- He, H.; Bai, Y.; Garcia, E.A.; Li, S. ADASYN: Adaptive synthetic sampling approach for im-balanced learning. In Proceedings of the 2008 IEEE International Joint Conference on Neural Networks (IEEE World Congress on Computational Intelligence), Hong Kong, China, 1–6 June 2008; pp. 1322–1328. [Google Scholar]
- van der Maaten, L.; Hinton, G. Visualizing Data using t-SNE. J. Mach. Learn. Res. 2008, 9, 2579–2605. [Google Scholar]
- Theodoridis, S.; Koutroumbas, K. Pattern Recognition; Academic Press: San Diego, CA, USA, 1999; pp. 341–342. [Google Scholar]
- Liu, H.; Motoda, H. Feature Selection for Knowledge Discovery and Data Mining. Kluwer International Series in Engineering and Computer Science 454; Kluwer Academic Publishers: Boston, MA, USA, 1998. [Google Scholar]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Features | Normal | HCM | p-Value | t-Value | ||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| LDPRes870 | 1.0906 | 0.1285 | 1.7401 | 0.1585 | 5.1 × 10−65 | 28.6105 |
| LDPRes1731 | 1.6194 | 0.3706 | 2.7880 | 0.3472 | 1.58 × 10−45 | 20.0121 |
| LDPRes1313 | 2.121 | 0.3118 | 1.3068 | 0.2749 | 1.57 × 10−37 | 16.9102 |
| LDPRes1701 | 0.8078 | 0.1347 | 0.4998 | 0.0998 | 6.62 × 10−34 | 15.5594 |
| LDPRes1100 | 0.9853 | 0.1107 | 1.2622 | 0.1160 | 5.59 × 10−33 | 15.2183 |
| LDPRes54 | 0.0675 | 0.0336 | 0.1584 | 0.0438 | 4.1 × 10−32 | 14.9010 |
| LDPRes110 | 1.1768 | 0.2628 | 1.8776 | 0.3561 | 9.59 × 10−31 | 14.4011 |
| LDPRes1351 | 0.7101 | 0.2133 | 0.3076 | 0.1133 | 7.92 × 10−29 | 13.7051 |
| LDPRes223 | 0.1786 | 0.0606 | 0.0634 | 0.0351 | 1.58 × 10−28 | 13.5969 |
| LDPRes770 | 2.4266 | 0.2920 | 1.8258 | 0.2951 | 4.83 × 10−26 | 12.6988 |
| Parameters | RNet50 | RNet18 | ANet | DNet | GNet |
|---|---|---|---|---|---|
| Input image size | 224 × 224 × 3 | 224 × 224 × 3 | 227 × 227 × 3 | 256 × 256 × 3 | 224 × 224 × 3 |
| No. of deep layers | 50 | 18 | 8 | 19 | 22 |
| Output layer | ‘avg pool’ | ‘pool5′ | ‘pool5′ | ‘avg1′ | ‘pool5-7 × 7′ |
| No. of features | 1 × 2048 | 1 × 512 | 1 × 4096 | 1 × 1000 | 1 × 1024 |
| Methods | Acc. (%) | Sen. (%) | Spe. (%) | PPV (%) | F-Score |
|---|---|---|---|---|---|
| LDP-RNet18 | 95.12 | 98.38 | 94.05 | 91.04 | 0.9456 |
| LDP-RNet50 | 100 | 100 | 100 | 100 | 1 |
| LDP-ANet | 87.11 | 82.25 | 90.09 | 83.60 | 0.8291 |
| LDP-DNet | 84.04 | 83.87 | 84.15 | 76.47 | 0.7999 |
| LDP-GNet | 93.25 | 90.32 | 95.04 | 91.80 | 0.9105 |
| Features | Normal | HCM | p-Value | t-Value | ||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| LDP-RNet18 | ||||||
| LDPRes492 | 0.696662 | 0.155103 | 1.216885 | 0.231307 | 2.98 × 10−38 | 17.18295 |
| LDP-RNet50 | ||||||
| LDPRes870 | 1.0906 | 0.1285 | 1.7401 | 0.1585 | 5.1 × 10−65 | 28.6105 |
| LDP-ANet | ||||||
| LDPAlex1852 | 0.194477 | 0.393206 | 1.13497 | 0.689104 | 1.31 × 10−21 | 11.09695 |
| LDP-DNet | ||||||
| LDPDark616 | −0.21708 | 0.421096 | −1.02086 | 0.402245 | 3.41 × 10−24 | 12.03204 |
| LDP-GNet | ||||||
| LDPGoogLe902 | 0.547527 | 0.457099 | 1.890254 | 0.790567 | 6.12 × 10−29 | 13.74575 |
| Features Using Various Methods | Normal | HCM | |||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | p-Value | |
| Entropy | |||||
| LDPRes17 | 0.000195 | 0.001399 | 0 | 0 | 0.274759 |
| Bhattacharyya | |||||
| LDPRes17 | 0.000195 | 0.001399 | 0 | 0 | 0.274759 |
| ROC | |||||
| LDPRes28 | 0 | 0 | 0.000952 | 0.004895 | 0.052053 |
| Wilcoxon | |||||
| LDPRes870 | 1.090677 | 0.128562 | 1.740115 | 0.158587 | 5.1 × 10−65 |
| Paper | Method | Result | Dataset |
|---|---|---|---|
| [19] | PCA + BPNN | Accuracy = 92.04% (normal and abnormal (DCM and HCM)) | Echocardiogram videos: 60 |
| [20] | DPSO-FCM + GLCM and DCT + SVM | For segmentation accuracy: 95% For classification accuracy: 90% | Echocardiogram videos: DCM: 40, HCM: 40, normal: 10 |
| [21] | Multilayer CNN | C statistics: 0.93 (for HCM) | HCM: 495 studies to train the model |
| [22] | First-order statistics + GLCM + SVM | Studied possible texture myocardial features with p-value < 0.05 | Transthoracic echocardiography images: HCM, uremic cardiomyopathy, and hypertensive heart disease (50 cases for each group) |
| Ours | LDP + ResNet-50 + ADASYN + IIHCM | Accuracy: 100% | Echocardiography images Normal: 101 HCM: 97 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gudigar, A.; Raghavendra, U.; Samanth, J.; Dharmik, C.; Gangavarapu, M.R.; Nayak, K.; Ciaccio, E.J.; Tan, R.-S.; Molinari, F.; Acharya, U.R. Novel Hypertrophic Cardiomyopathy Diagnosis Index Using Deep Features and Local Directional Pattern Techniques. J. Imaging 2022, 8, 102. https://0-doi-org.brum.beds.ac.uk/10.3390/jimaging8040102
Gudigar A, Raghavendra U, Samanth J, Dharmik C, Gangavarapu MR, Nayak K, Ciaccio EJ, Tan R-S, Molinari F, Acharya UR. Novel Hypertrophic Cardiomyopathy Diagnosis Index Using Deep Features and Local Directional Pattern Techniques. Journal of Imaging. 2022; 8(4):102. https://0-doi-org.brum.beds.ac.uk/10.3390/jimaging8040102
Chicago/Turabian StyleGudigar, Anjan, U. Raghavendra, Jyothi Samanth, Chinmay Dharmik, Mokshagna Rohit Gangavarapu, Krishnananda Nayak, Edward J. Ciaccio, Ru-San Tan, Filippo Molinari, and U. Rajendra Acharya. 2022. "Novel Hypertrophic Cardiomyopathy Diagnosis Index Using Deep Features and Local Directional Pattern Techniques" Journal of Imaging 8, no. 4: 102. https://0-doi-org.brum.beds.ac.uk/10.3390/jimaging8040102