

Validation of Left Atrial Volume Correction for Single Plane Method on Four-Chamber Cine Cardiac MRI
 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Cohort
2.2. Ethics Approval and Consent to Participate
2.3. Cardiac Magnetic Resonance Protocol
2.4. CMR Analysis
2.5. Statistical Analysis
3. Results
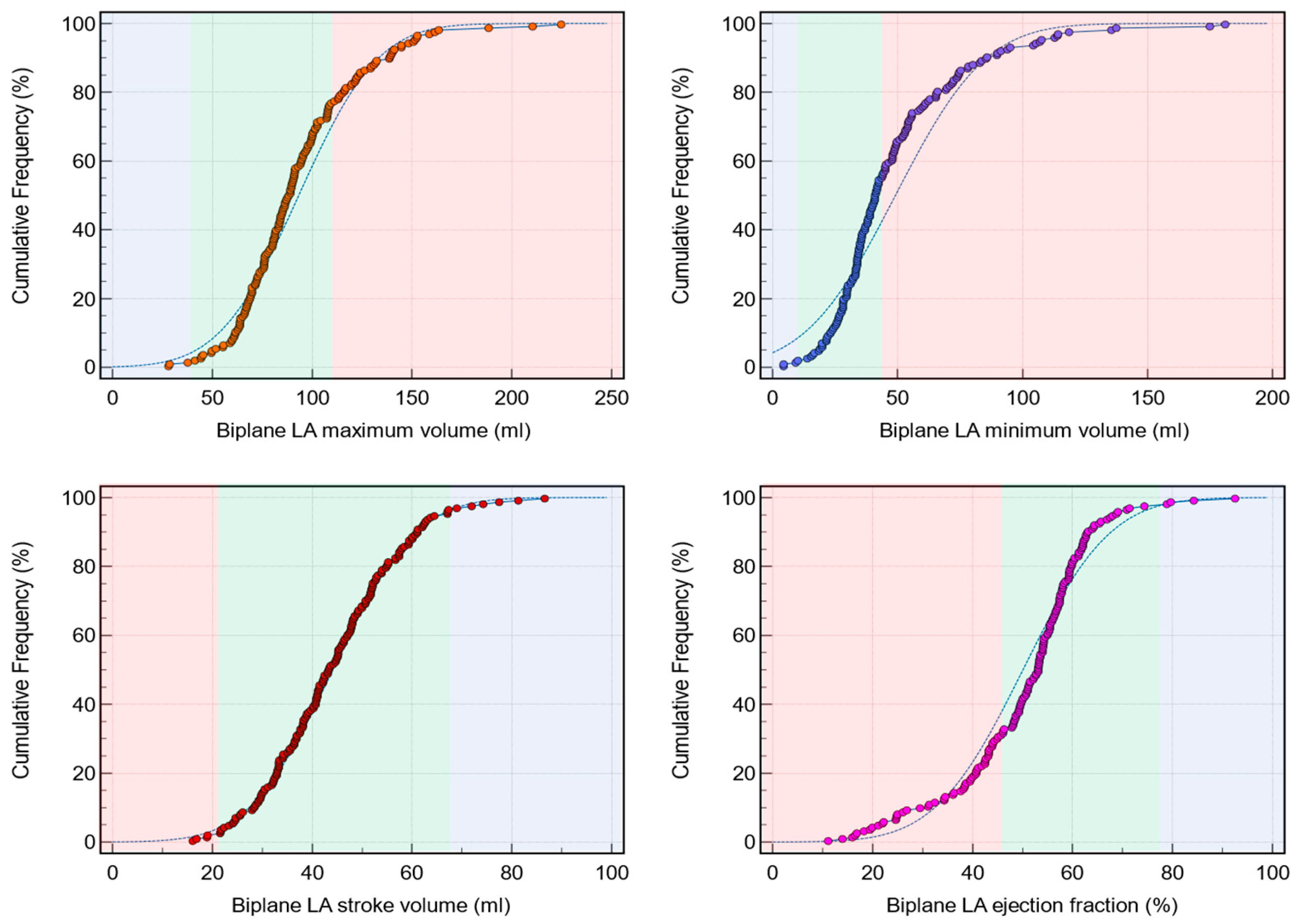
3.1. Left Atrial Biplanar Volume Assessment in the Whole Cohort
3.2. Derivation Cohort (n = 100)
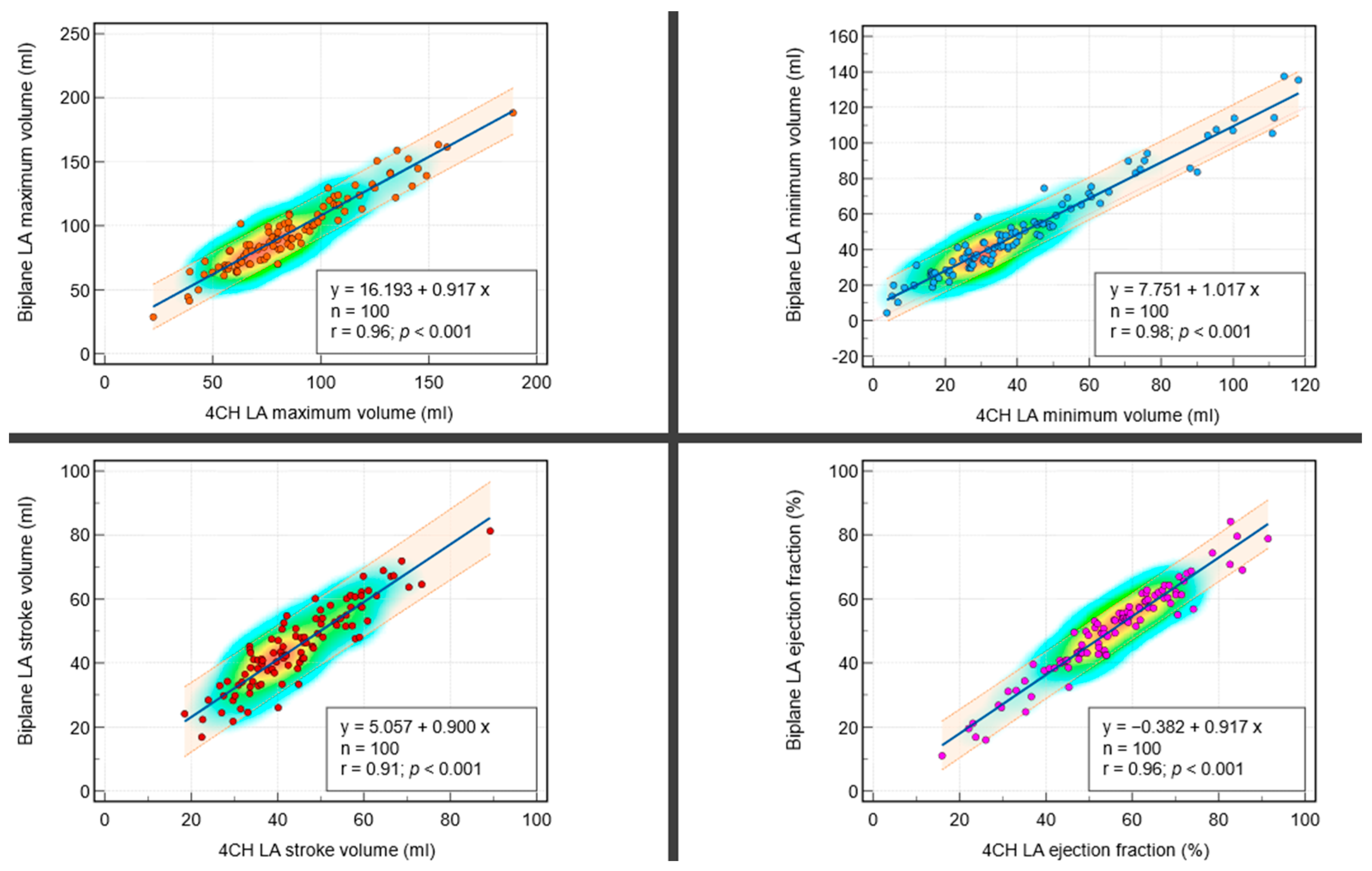
3.2.1. Correlations between Biplanar and Single Planar Methods
3.2.2. Bland–Altman Plots and Bias Investigation
3.3. Validation Cohort (n = 79)
3.3.1. Left Atrial Volumetric Assessment
3.3.2. Correlations between Biplanar and Single-Planar after Bias Correction
3.3.3. Bland–Altman Plots and Bias Investigation after Bias Correction
3.3.4. Receiver Operator Characteristics
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AF | atrial fibrillation |
| AUC | area under the curve |
| CMR | cardiovascular magnetic resonance |
| EF | ejection fraction |
| LA | left atrium |
| LVFP | left ventricular filling pressure |
| ROC | receiver operator curve |
| SD | standard deviation |
| SV | stroke volume |
References
- Hoit, B.D. Left atrial size and function: Role in prognosis. J. Am. Coll. Cardiol. 2014, 63, 493–505. [Google Scholar] [CrossRef]
- Rossi, A.; Temporelli, P.L.; Quintana, M.; Dini, F.L.; Ghio, S.; Hillis, G.S.; Klein, A.L.; Marsan, N.A.; Prior, D.L.; Yu, C.M.; et al. Independent relationship of left atrial size and mortality in patients with heart failure: An individual patient meta-analysis of longitudinal data (MeRGE Heart Failure). Eur. J. Heart Fail. 2009, 11, 929–936. [Google Scholar] [CrossRef]
- Raisi-Estabragh, Z.; McCracken, C.; Condurache, D.; Aung, N.; Vargas, J.D.; Naderi, H.; Munroe, P.B.; Neubauer, S.; Harvey, N.C.; Petersen, S.E. Left atrial structure and function are associated with cardiovascular outcomes independent of left ventricular measures: A UK Biobank CMR study. Eur. Heart J. Cardiovasc. Imaging 2022, 23, 1191–1200. [Google Scholar] [CrossRef]
- Bombelli, M.; Facchetti, R.; Cuspidi, C.; Villa, P.; Dozio, D.; Brambilla, G.; Grassi, G.; Mancia, G. Prognostic Significance of Left Atrial Enlargement in a General Population. Hypertension 2014, 64, 1205–1211. [Google Scholar] [CrossRef]
- Inciardi, R.M.; Giugliano, R.P.; Claggett, B.; Gupta, D.K.; Chandra, A.; Ruff, C.T.; Antman, E.M.; Mercuri, M.F.; Grosso, M.A.; Braunwald, E.; et al. Left atrial structure and function and the risk of death or heart failure in atrial fibrillation. Eur. J. Heart Fail. 2019, 21, 1571–1579. [Google Scholar] [CrossRef]
- Di Tullio, M.R.; Sacco, R.L.; Sciacca, R.R.; Homma, S. Left atrial size and the risk of ischemic stroke in an ethnically mixed population. Stroke 1999, 30, 2019–2024. [Google Scholar] [CrossRef]
- Hosseini Farahabadi, M.; Milani-Nejad, S.; Liu, S.; Yu, W.; Shafie, M. Left Atrial Dilatation and Reduced Left Ventricular Ejection Fraction Are Associated with Cardioembolic Stroke. Front. Neurol. 2021, 12, 680651. [Google Scholar] [CrossRef] [PubMed]
- Welles, C.C.; Ku, I.A.; Kwan, D.M.; Whooley, M.A.; Schiller, N.B.; Turakhia, M.P. Left atrial function predicts heart failure hospitalization in subjects with preserved ejection fraction and coronary heart disease: Longitudinal data from the Heart and Soul Study. J. Am. Coll. Cardiol. 2012, 59, 673–680. [Google Scholar] [CrossRef] [PubMed]
- Kawel-Boehm, N.; Hetzel, S.J.; Ambale-Venkatesh, B.; Captur, G.; Francois, C.J.; Jerosch-Herold, M.; Salerno, M.; Teague, S.D.; Valsangiacomo-Buechel, E.; van der Geest, R.J.; et al. Reference ranges (‘normal values’) for cardiovascular magnetic resonance (CMR) in adults and children: 2020 update. J. Cardiovasc. Magn. Reson. Off. J. Soc. Cardiovasc. Magn. Reson. 2020, 22, 87. [Google Scholar] [CrossRef] [PubMed]
- Kowallick, J.T.; Kutty, S.; Edelmann, F.; Chiribiri, A.; Villa, A.; Steinmetz, M.; Sohns, J.M.; Staab, W.; Bettencourt, N.; Unterberg-Buchwald, C.; et al. Quantification of left atrial strain and strain rate using Cardiovascular Magnetic Resonance myocardial feature tracking: A feasibility study. J. Cardiovasc. Magn. Reson. 2014, 16, 60. [Google Scholar] [CrossRef] [PubMed]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E.; Drazner, M.H.; Fonarow, G.C.; Geraci, S.A.; Horwich, T.; Januzzi, J.L.; et al. 2013 ACCF/AHA guideline for the management of heart failure: A report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation 2013, 128, e240–e327. [Google Scholar] [CrossRef] [PubMed]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, e895–e1032. [Google Scholar] [CrossRef]
- Kawel-Boehm, N.; Maceira, A.; Valsangiacomo-Buechel, E.R.; Vogel-Claussen, J.; Turkbey, E.B.; Williams, R.; Plein, S.; Tee, M.; Eng, J.; Bluemke, D.A. Normal values for cardiovascular magnetic resonance in adults and children. J. Cardiovasc. Magn. Reson. Off. J. Soc. Cardiovasc. Magn. Reson. 2015, 17, 29. [Google Scholar] [CrossRef] [PubMed]
- Petersen, S.E.; Khanji, M.Y.; Plein, S.; Lancellotti, P.; Bucciarelli-Ducci, C. European Association of Cardiovascular Imaging expert consensus paper: A comprehensive review of cardiovascular magnetic resonance normal values of cardiac chamber size and aortic root in adults and recommendations for grading severity. Eur. Heart J. Cardiovasc. Imaging 2019, 20, 1321–1331. [Google Scholar] [CrossRef]
- Garg, P.; Gosling, R.; Swoboda, P.; Jones, R.; Rothman, A.; Wild, J.M.; Kiely, D.G.; Condliffe, R.; Alabed, S.; Swift, A.J. Cardiac magnetic resonance identifies raised left ventricular filling pressure: Prognostic implications. Eur. Heart J. 2022, 43, 2511–2522. [Google Scholar] [CrossRef]
- Assadi, H.; Matthews, G.; Chambers, B.; Grafton-Clarke, C.; Shabi, M.; Plein, S.; Swoboda, P.P.; Garg, P. Cardiac Magnetic Resonance Left Ventricular Filling Pressure Is Associated with NT-proBNP in Patients with New Onset Heart Failure. Medicina 2023, 59, 1924. [Google Scholar] [CrossRef]
- Tao, S.; Ciuffo, L.A.; Lima, J.A.C.; Wu, K.C.; Ashikaga, H. Quantifying left atrial structure and function using single-plane tissue-tracking cardiac magnetic resonance. Magn. Reson. Imaging 2017, 42, 130–138. [Google Scholar] [CrossRef]
- Mitchell, C.; Rahko, P.S.; Blauwet, L.A.; Canaday, B.; Finstuen, J.A.; Foster, M.C.; Horton, K.; Ogunyankin, K.O.; Palma, R.A.; Velazquez, E.J. Guidelines for Performing a Comprehensive Transthoracic Echocardiographic Examination in Adults: Recommendations from the American Society of Echocardiography. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2019, 32, 1–64. [Google Scholar] [CrossRef] [PubMed]
- Crandon, S.; Westenberg, J.J.M.; Swoboda, P.P.; Fent, G.J.; Foley, J.R.J.; Chew, P.G.; Brown, L.A.E.; Saunderson, C.; Al-Mohammad, A.; Greenwood, J.P.; et al. Impact of Age and Diastolic Function on Novel, 4D flow CMR Biomarkers of Left Ventricular Blood Flow Kinetic Energy. Sci. Rep. 2018, 8, 14436. [Google Scholar] [CrossRef] [PubMed]
- Garg, P.; Crandon, S.; Swoboda, P.P.; Fent, G.J.; Foley, J.R.J.; Chew, P.G.; Brown, L.A.E.; Vijayan, S.; Hassell, M.E.C.J.; Nijveldt, R.; et al. Left ventricular blood flow kinetic energy after myocardial infarction—Insights from 4D flow cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. Off. J. Soc. Cardiovasc. Magn. Reson. 2018, 20, 61. [Google Scholar] [CrossRef] [PubMed]
- Alandejani, F.; Alabed, S.; Garg, P.; Goh, Z.M.; Karunasaagarar, K.; Sharkey, M.; Salehi, M.; Aldabbagh, Z.; Dwivedi, K.; Mamalakis, M.; et al. Training and clinical testing of artificial intelligence derived right atrial cardiovascular magnetic resonance measurements. J. Cardiovasc. Magn. Reson. Off. J. Soc. Cardiovasc. Magn. Reson. 2022, 24, 25. [Google Scholar] [CrossRef] [PubMed]
- Alfuhied, A.; Marrow, B.A.; Elfawal, S.; Gulsin, G.S.; Graham-Brown, M.P.; Steadman, C.D.; Kanagala, P.; McCann, G.P.; Singh, A. Reproducibility of left atrial function using cardiac magnetic resonance imaging. Eur. Radiol. 2021, 31, 2788–2797. [Google Scholar] [CrossRef] [PubMed]
- Zareian, M.; Ciuffo, L.; Habibi, M.; Opdahl, A.; Chamera, E.H.; Wu, C.O.; Bluemke, D.A.; Lima, J.A.C.; Venkatesh, B.A. Left atrial structure and functional quantitation using cardiovascular magnetic resonance and multimodality tissue tracking: Validation and reproducibility assessment. J. Cardiovasc. Magn. Reson. Off. J. Soc. Cardiovasc. Magn. Reson. 2015, 17, 52. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, C.; Bricknell, K.; Marwick, T.H. Use of real-time three-dimensional echocardiography to measure left atrial volume: Comparison with other echocardiographic techniques. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2005, 18, 991–997. [Google Scholar] [CrossRef]
- Nagueh, S.F.; Khan, S.U. Left Atrial Strain for Assessment of Left Ventricular Diastolic Function: Focus on Populations with Normal LVEF. JACC Cardiovasc. Imaging 2023, 16, 691–707. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Derivation Cohort | Biplane Method | Single Plane Method | Bias | SD of Bias | p |
|---|---|---|---|---|---|
| LA maximum volume, mL | 96 ± 29 | 86 ± 30 | −9 | 9 * | <0.01 |
| LA minimum volume, mL | 50 ± 27 | 42 ± 26 | −8 | 6 * | <0.01 |
| LA stroke volume, mL | 45 ± 13 | 45 ± 13 | −1 | 6 | 0.27 |
| LA ejection fraction, % | 50 ± 14 | 55 ± 15 | −5 | 4 * | <0.01 |
| Validation Cohort | Biplane Method | Single Plane | Bias | p |
|---|---|---|---|---|
| LA maximum volume, mL | 90 ± 34 | 92 ± 34 | −2 | 0.06 |
| LA minimum volume, mL | 48 ± 30 | 47 ± 30 | 0.5 | 0.47 |
| LA stroke volume, mL | 43 ± 14 | 42 ± 13 | 0.5 | 0.47 |
| LA ejection fraction, % | 50 ± 14 | 50 ± 15 | −0.2 | 0.69 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Assadi, H.; Sawh, N.; Bailey, C.; Matthews, G.; Li, R.; Grafton-Clarke, C.; Mehmood, Z.; Kasmai, B.; Swoboda, P.P.; Swift, A.J.; et al. Validation of Left Atrial Volume Correction for Single Plane Method on Four-Chamber Cine Cardiac MRI. Tomography 2024, 10, 459-470. https://0-doi-org.brum.beds.ac.uk/10.3390/tomography10040035
Assadi H, Sawh N, Bailey C, Matthews G, Li R, Grafton-Clarke C, Mehmood Z, Kasmai B, Swoboda PP, Swift AJ, et al. Validation of Left Atrial Volume Correction for Single Plane Method on Four-Chamber Cine Cardiac MRI. Tomography. 2024; 10(4):459-470. https://0-doi-org.brum.beds.ac.uk/10.3390/tomography10040035
Chicago/Turabian StyleAssadi, Hosamadin, Nicholas Sawh, Ciara Bailey, Gareth Matthews, Rui Li, Ciaran Grafton-Clarke, Zia Mehmood, Bahman Kasmai, Peter P. Swoboda, Andrew J. Swift, and et al. 2024. "Validation of Left Atrial Volume Correction for Single Plane Method on Four-Chamber Cine Cardiac MRI" Tomography 10, no. 4: 459-470. https://0-doi-org.brum.beds.ac.uk/10.3390/tomography10040035