
Multidetector Computed Tomography (MDCT) Findings of Complications of Acute Cholecystitis. A Pictorial Essay

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. Background
1.2. Objective
2. Pathophysiology
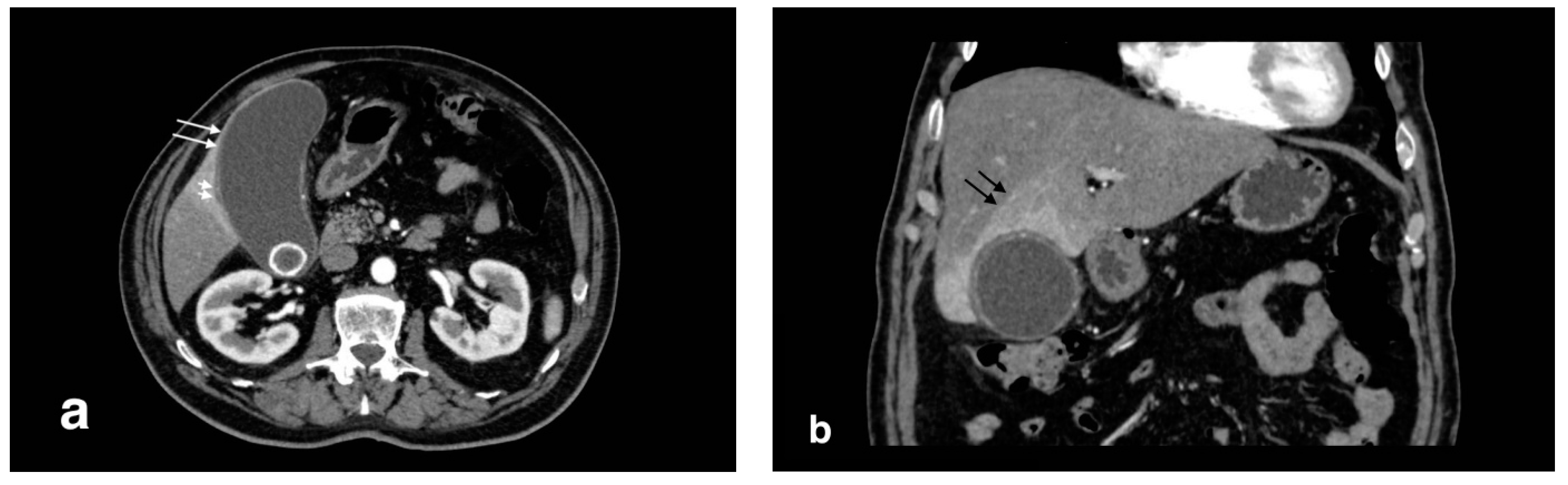
2.1. CT Findings in Acute Cholecystitis
2.2. Complications
2.3. Complicated Acute Forms
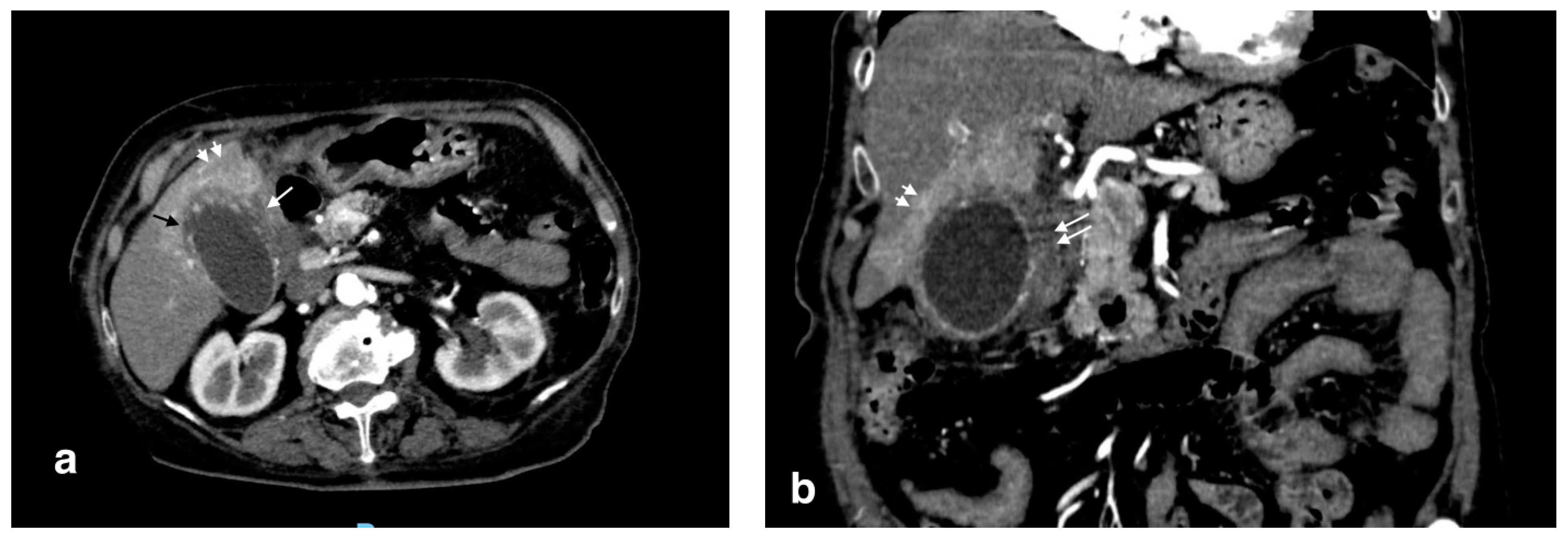
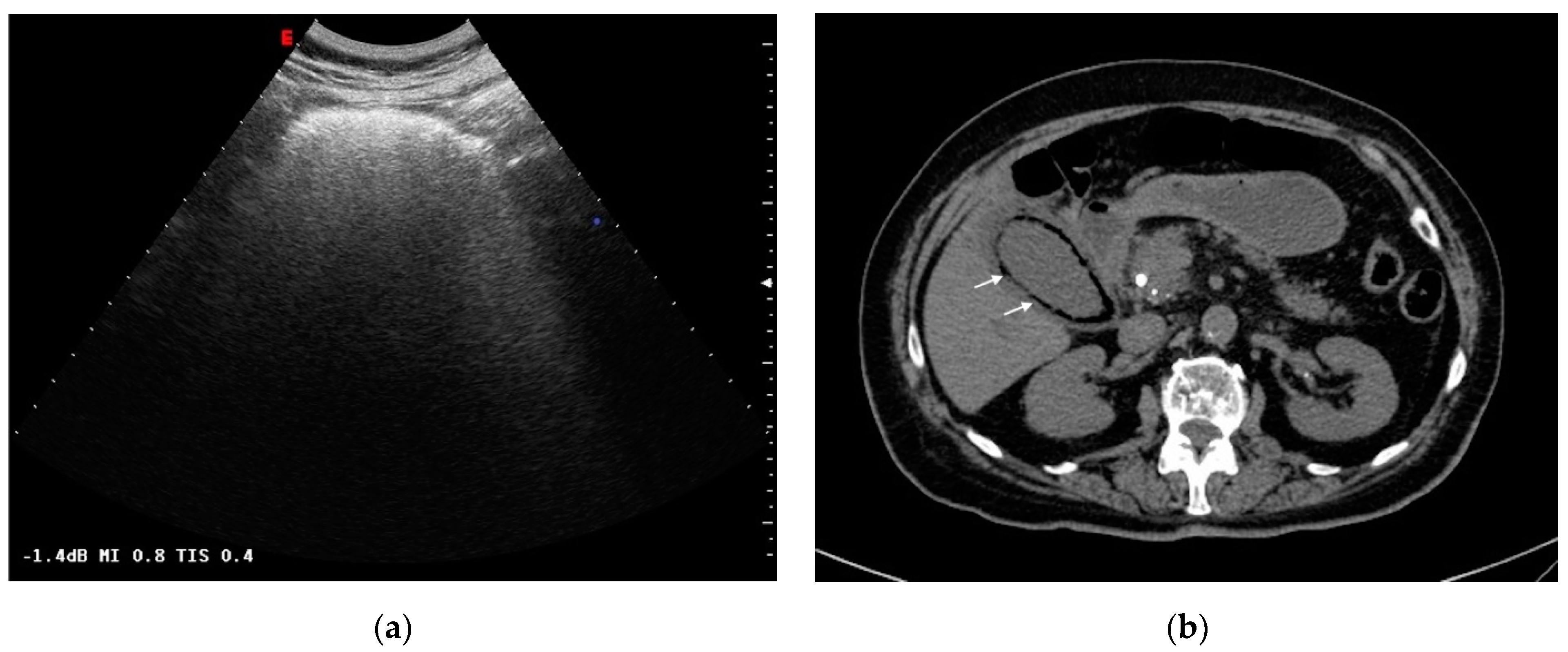
2.3.1. Gangrenous Cholecystitis
2.3.2. Emphysematous Cholecystitis
3. Cholecystic Complications
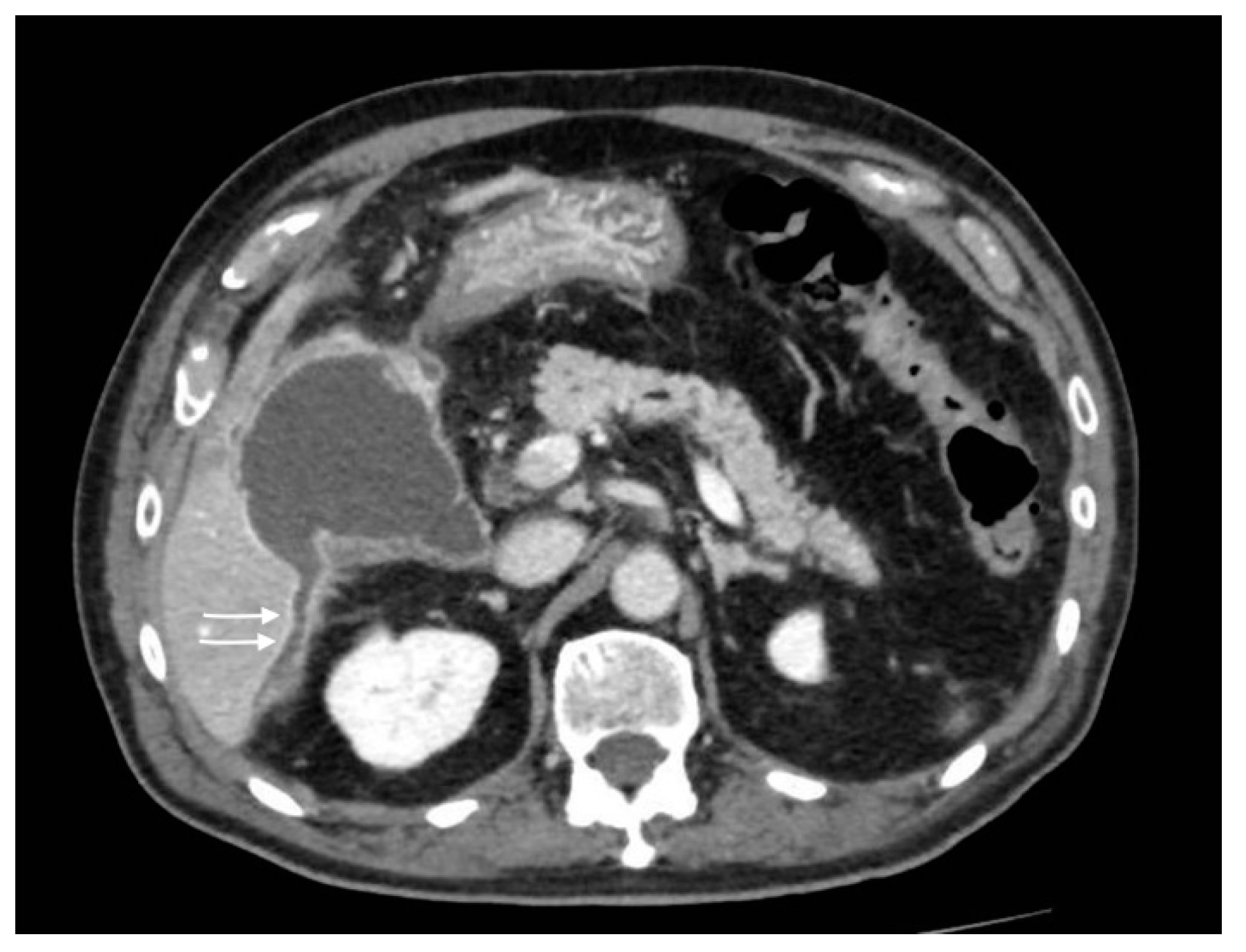
Gallbladder Perforation
4. Biliary and Intrahepatic Complications
4.1. Acute Cholangitis
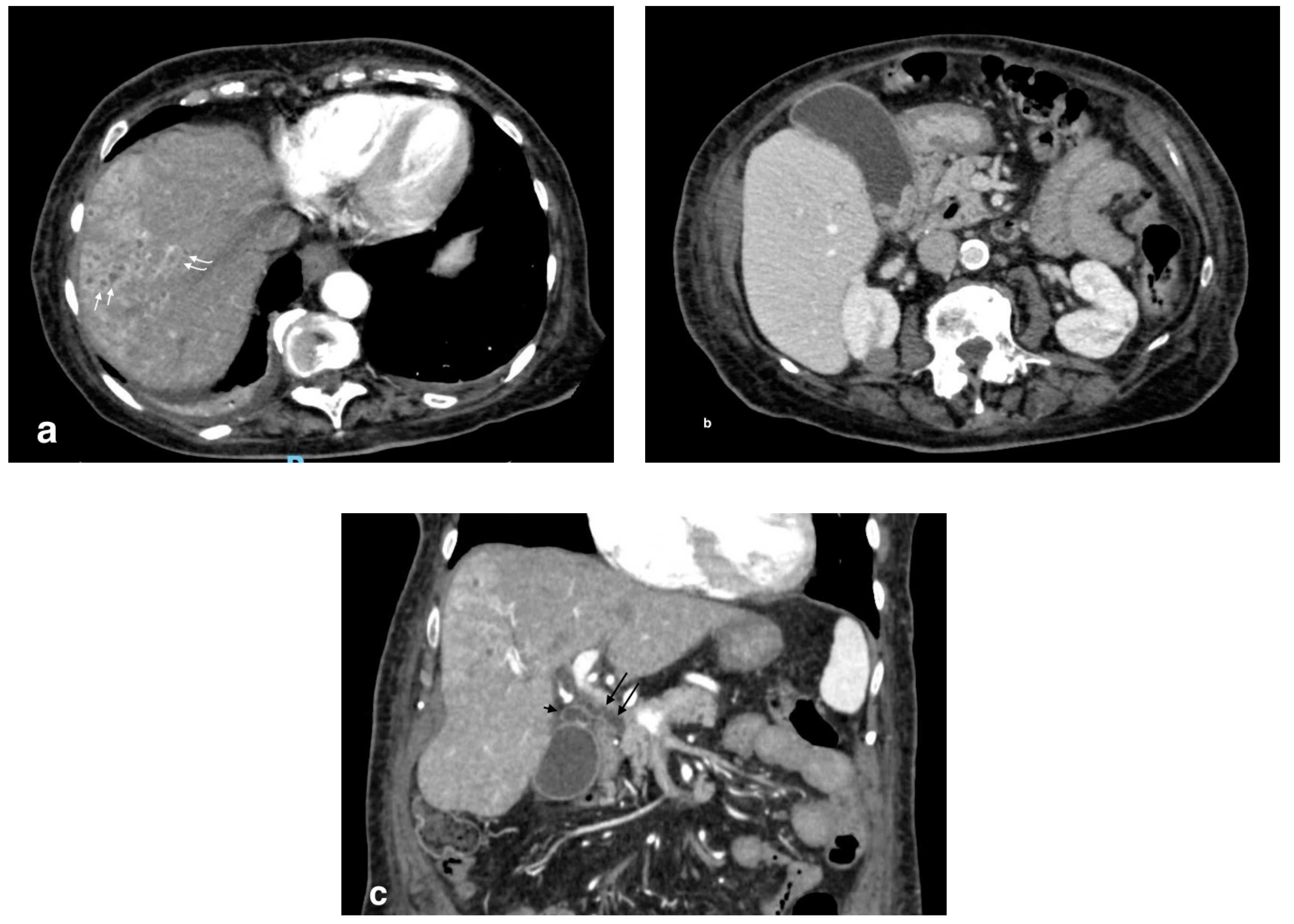
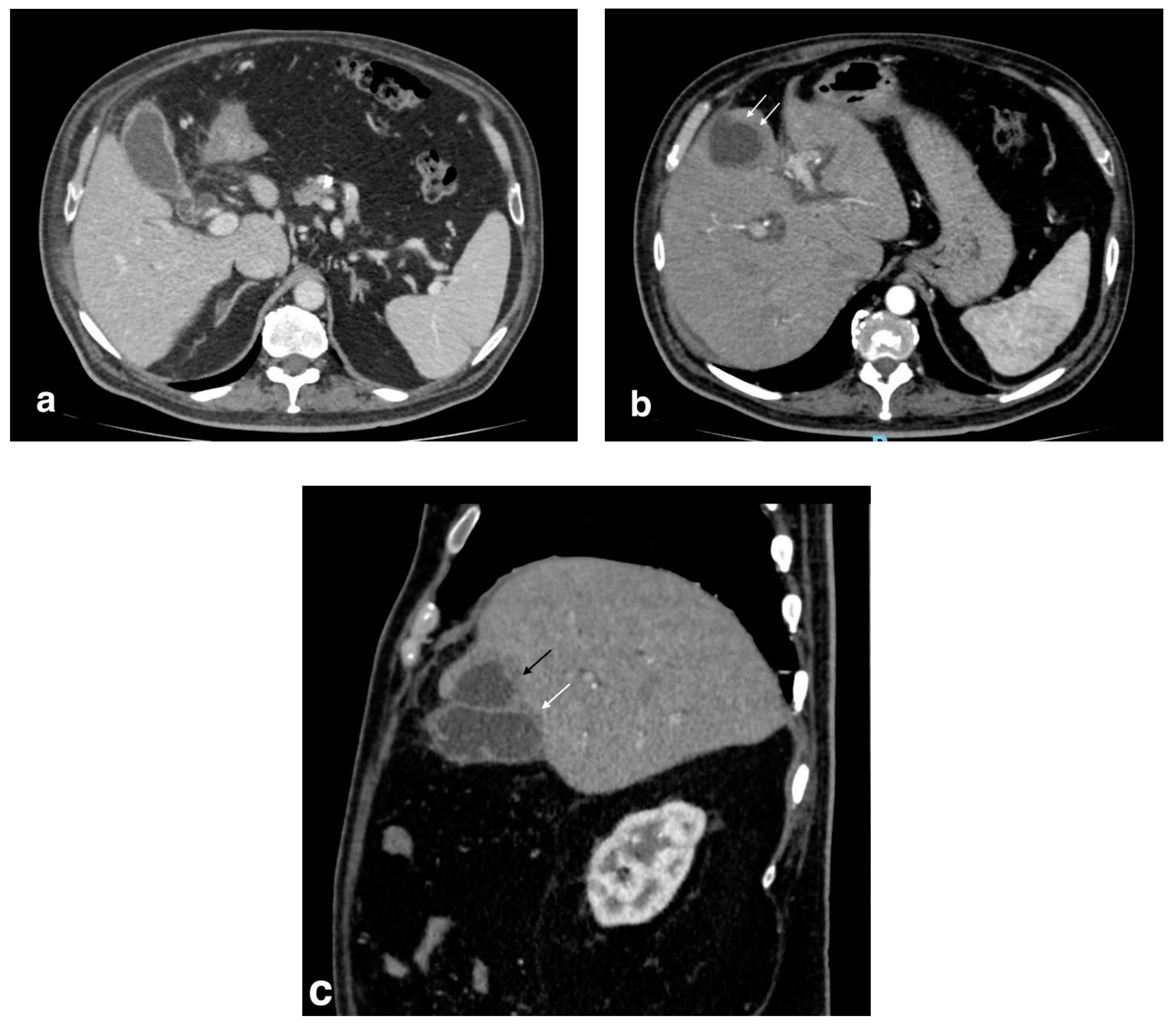
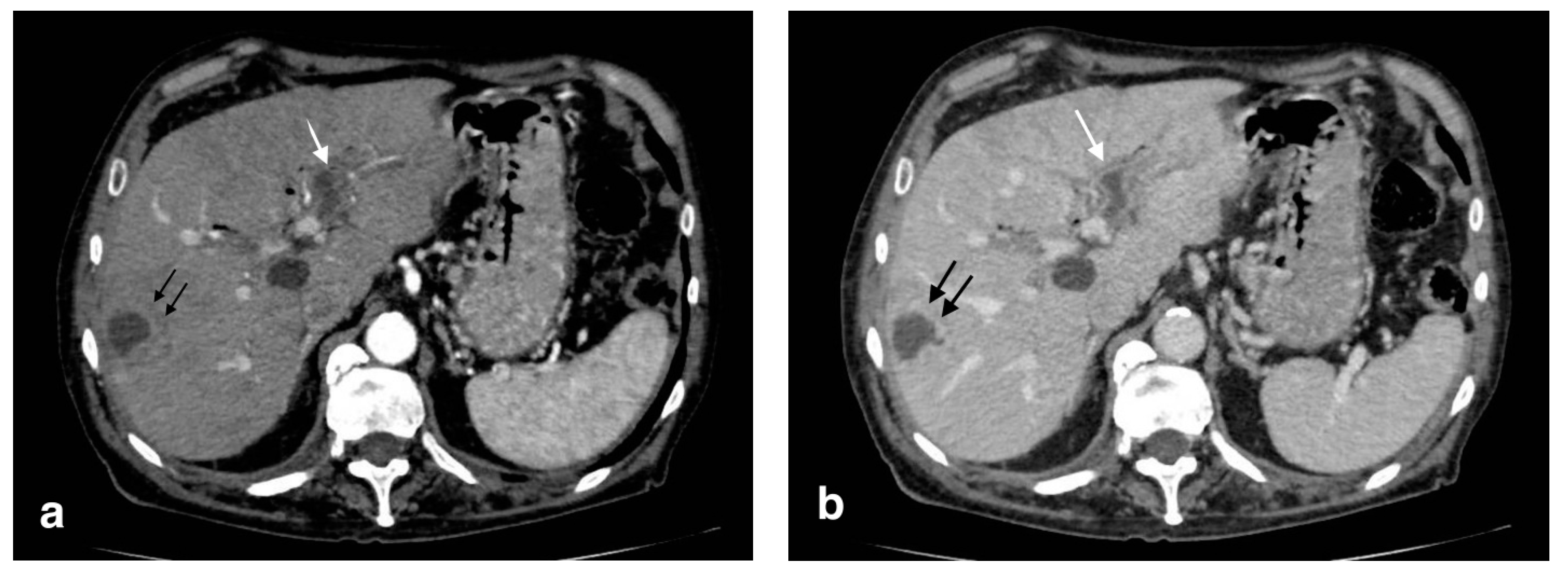
4.2. Pericholecystic and Liver Abscesses
5. Vascular Complications
5.1. Portal Vein Thrombosis (PVT) and Pylephlebitis
5.2. Visceral Arteries Pseudoaneurysm
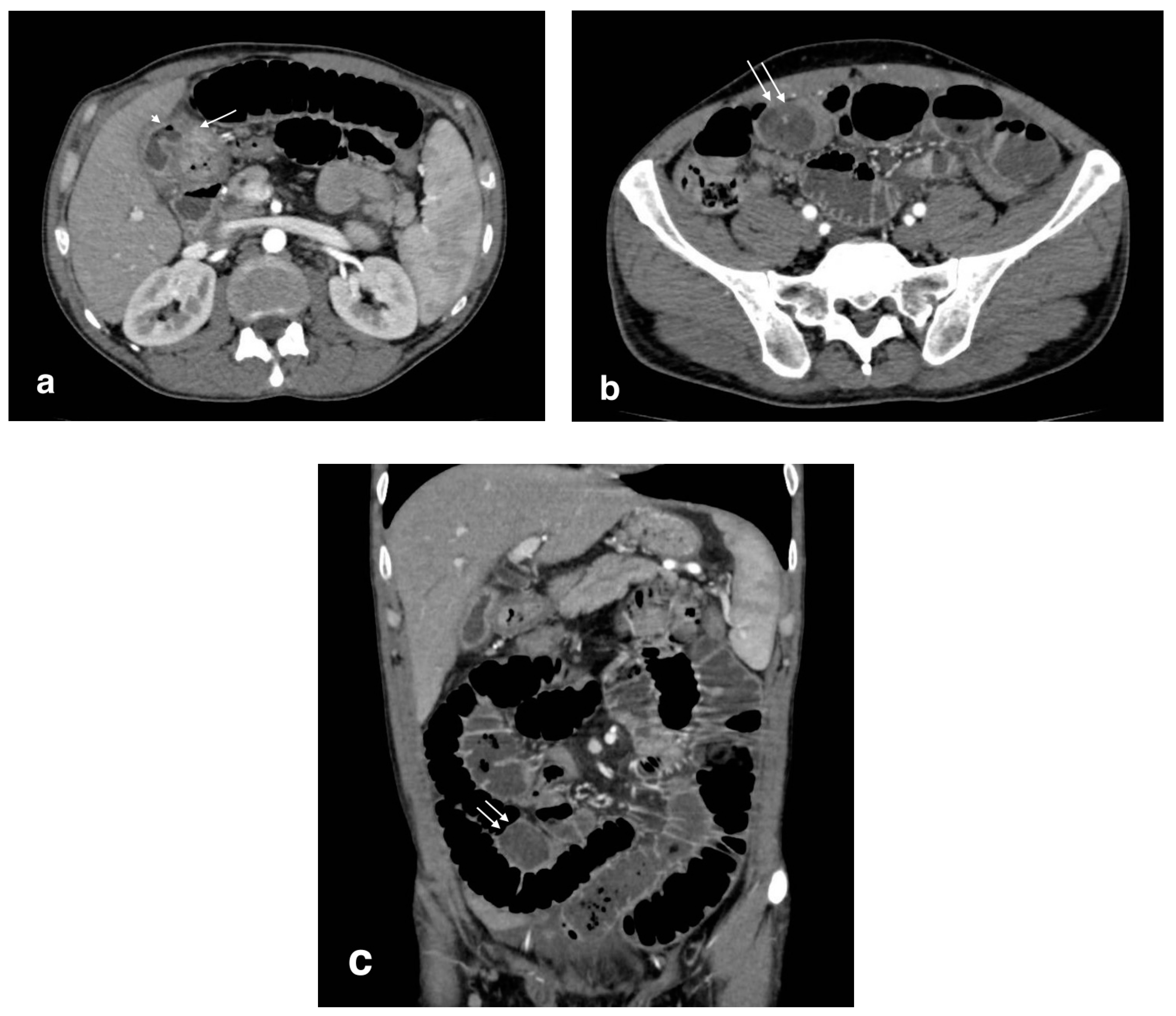
6. Extrabiliary Gastrointestinal Complications
6.1. Colitis
6.2. Biliary Pancreatitis
7. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ukegjini, K.; Schmied, B.M. Diagnosis and treatment of acute cholecystitis. Ther. Umsch. 2020, 77, 133–146. [Google Scholar] [CrossRef] [PubMed]
- Trowbridge, R.L.; Rutkowski, N.K.; Shojania, K.G. Does this patient have acute cholecystitis? JAMA 2003, 289, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Zenobii, M.F.; Accogli, E.; Domanico, A.; Arienti, V. Update on bedside ultrasound (US) diagnosis of acute cholecystitis (AC). Intern. Emerg. Med. 2016, 11, 261–264. [Google Scholar] [CrossRef] [PubMed]
- Martellotto, S.; Dohan, A.; Pocard, M. Evaluation of the CT Scan as the First Examination for the Diagnosis and Therapeutic Strategy for Acute Cholecystitis. World J. Surg. 2020, 44, 1779–1789. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, D.; Ojili, V.; Nepal, P.; Nagar, A.; Hernandez-Delima, F.J.; Bajaj, D.; Choudhary, G.; Gupta, N.; Sharma, P. A pictorial review of gall stones and its associated complications. Clin. Imaging. 2020, 60, 228–236. [Google Scholar] [CrossRef]
- Barie, P.S.; Eachempati, S.R. Acute acalculous cholecystitis. Gastroenterol. Clin. N. Am. 2010, 39, 343–357. [Google Scholar] [CrossRef]
- Chawla, A.; Bosco, J.I.; Lim, T.C.; Srinivasan, S.; Teh, H.S.; Shenoy, J.N. Imaging of acute cholecystitis and cholecystitis-associated complications in the emergency setting. Singap. Med. J. 2015, 56, 438–443. [Google Scholar] [CrossRef] [Green Version]
- Barakos, J.A.; Ralls, P.W.; Lapin, A.S.; Johnson, M.B.; Radin, D.R.; Colletti, P.M.; Boswell, W.D.; Halls, J.M. Cholelithiasis: Evaluation with CT. Radiology 1987, 162, 415–418. [Google Scholar] [CrossRef]
- van Breda Vriesman, A.C.; Engelbrecht, M.R.; Smithuis, R.H.M.; Puylaert, J.B.C.M. Diffuse gallbladder wall thickening: Differential diagnosis. AJR Am. J. Roentgenol. 2007, 188, 495–501. [Google Scholar] [CrossRef]
- Kim, K.H.; Kim, S.J.; Lee, S.C.; Lee, S.K. Risk assessment scales and predictors for simple versus severe cholecystitis in performing laparoscopic cholecystectomy. Asian J. Surg. 2017, 40, 367–374. [Google Scholar] [CrossRef] [Green Version]
- Maddu, K.; Phadke, S.; Hoff, C. Complications of cholecystitis: A comprehensive contemporary imaging review. Emerg. Radiol. 2021, 28, 1011–1027. [Google Scholar] [CrossRef] [PubMed]
- Ganapathi, A.M.; Speicher, P.J.; Englum, B.R.; Perez, A.; Tyler, D.S.; Zani, S. Gangrenous cholecystitis: A contemporary review. J. Surg. Res. 2015, 197, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Chang, W.C.; Sun, Y.; Wu, E.-H.; Kim, S.Y.; Wang, Z.J.; Huang, G.-S.; Yeh, B.M. CT Findings for Detecting the Presence of Gangrenous Ischemia in Cholecystitis. AJR Am. J. Roentgenol. 2016, 207, 302–309. [Google Scholar] [CrossRef] [PubMed]
- Sunnapwar, A.; Raut, A.A.; Nagar, A.M.; Katre, R. Emphysematous cholecystitis: Imaging findings in nine patients. Indian J. Radiol. Imaging 2011, 21, 142–146. [Google Scholar] [CrossRef]
- Patel, N.B.; Oto, A.; Thomas, S. Multidetector CT of emergent biliary pathologic conditions. Radiographics 2013, 33, 1867–1888. [Google Scholar] [CrossRef]
- Boruah, D.K.; Sanyal, S.; Sharma, B.K.; Boruah, D.R. Comparative Evaluation of Ultrasonography and Cross-sectional Imaging in Determining Gall Bladder Perforation in Accordance to Niemeier’s Classification. J. Clin. Diagn. Res. 2016, 10, TC15–TC18. [Google Scholar] [CrossRef]
- Shakespear, J.S.; Shaaban, A.M.; Rezvani, M. CT findings of acute cholecystitis and its complications. AJR Am. J. Roentgenol. 2010, 194, 1523–1529. [Google Scholar] [CrossRef]
- Zaliekas, J.; Munson, J.L. Complications of gallstones: The Mirizzi syndrome, gallstone ileus, gallstone pancreatitis, complications of "lost" gallstones. Surg. Clin. N. Am. 2008, 88, 1345–1368. [Google Scholar] [CrossRef]
- Lassandro, F.; Gagliardi, N.; Scuderi, M.; Pinto, A.; Gatta, G.; Mazzeo, R. Gallstone ileus analysis of radiological findings in 27 patients. Eur. J. Radiol. 2004, 50, 23–29. [Google Scholar] [CrossRef]
- Lardière-Deguelte, S.; Ragot, E.; Amroun, K.; Piardi, T.; Dokmak, S.; Bruno, O.; Appere, F.; Sibert, A.; Hoeffel, C.; Sommacale, D.; et al. Hepatic abscess: Diagnosis and management. J. Visc. Surg. 2015, 152, 231–243. [Google Scholar] [CrossRef]
- Balthazar, E.J.; Birnbaum, B.A.; Naidich, M. Acute cholangitis: CT evaluation. J. Comput. Assist. Tomogr. 1993, 17, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Hong, M.J.; Kim, S.W.; Kim, H.C.; Yang, D.M. Comparison of the clinical characteristics and imaging findings of acute cholangitis with and without biliary dilatation. Br. J. Radiol. 2012, 85, e1219–e1225. [Google Scholar] [CrossRef] [Green Version]
- Zhornitskiy, A.; Berry, R.; Han, J.Y.; Tabibian, J.H. Hemobilia: Historical overview, clinical update, and current practices. Liver Int. 2019, 39, 1378–1388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karaosmanoglu, A.D.; Uysal, A.; Akata, D.; Ozmen, M.N.; Karcaaltincaba, M. Role of imaging in visceral vascular emergencies. Insights Imaging 2020, 11, 112. [Google Scholar] [CrossRef] [PubMed]
- Muneer, M.; Abdelrahman, H.; El-Menyar, A.; Zarour, A.; Awad, A.; Al-Thani, H. Acute Cholecystitis Complicated with Portal Vein Thrombosis: A Case Report and Literature Review. Am. J. Case Rep. 2015, 16, 627–630. [Google Scholar] [CrossRef] [PubMed]
- Wong, K.; Weisman, D.S.; Patrice, K.A. Pylephlebitis: A rare complication of an intra-abdominal infection. J. Community Hosp. Intern. Med. Perspect. 2013, 3, 20732. [Google Scholar] [CrossRef] [PubMed]
- Ozawa, K.; Shikino, K. Pylephlebitis due to acute cholecystitis and cholangitis. BMJ Case Rep. 2021, 14, e244912. [Google Scholar] [CrossRef]
- Teoh, Z.H.; Surya, A.; Mathialahan, T.; Khan, H. An insidious case of hepatic artery pseudoaneurysm secondary to acalculus cholecystitis. BMJ Case Rep. 2015, 2015, bcr2015212424. [Google Scholar] [CrossRef] [Green Version]
- Patil, N.S.; Kumar, A.H.; Pamecha, V.; Gattu, T.; Falari, S.; Sinha, P.K.; Mohapatra, N. Cystic artery pseudoaneurysm-a rare complication of acute cholecystitis: Review of literature. Surg Endosc. 2022, 36, 871–880. [Google Scholar] [CrossRef]
- Bennett, J.; Fay, D.; Krysztopik, R. Right hepatic artery false aneurysm secondary to acalculous cholecystitis. BMJ Case Rep. 2010, 2010, bcr0820103258. [Google Scholar] [CrossRef] [Green Version]
- Tulsyan, N.; Kashyap, V.S.; Greenberg, R.K.; Sarac, T.P.; Clair, D.G.; Pierce, G.; Ouriel, K. The endovascular management of visceral artery aneurysms and pseudoaneurysms. J. Vasc. Surg. 2007, 45, 276–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soudack, M.; Epelman, M.; Gaitini, D. Spontaneous Thrombosis of hepatic Posttraumatic Pseudoaneurysms. JUM Case Rep. 2003, 22, 99–103. [Google Scholar] [CrossRef] [PubMed]














Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sandomenico, F.; Sanduzzi, L.; La Verde, E.; Vicenzo, E.; Pirolo, L.; Maione, S.; Setola, F.R.; Macchia, V.; Dello Iacono, U.; Barbato, D.; et al. Multidetector Computed Tomography (MDCT) Findings of Complications of Acute Cholecystitis. A Pictorial Essay. Tomography 2022, 8, 1159-1171. https://0-doi-org.brum.beds.ac.uk/10.3390/tomography8020095
Sandomenico F, Sanduzzi L, La Verde E, Vicenzo E, Pirolo L, Maione S, Setola FR, Macchia V, Dello Iacono U, Barbato D, et al. Multidetector Computed Tomography (MDCT) Findings of Complications of Acute Cholecystitis. A Pictorial Essay. Tomography. 2022; 8(2):1159-1171. https://0-doi-org.brum.beds.ac.uk/10.3390/tomography8020095
Chicago/Turabian StyleSandomenico, Fabio, Luca Sanduzzi, Emilia La Verde, Emilio Vicenzo, Luigi Pirolo, Salvatore Maione, Francesca Rosa Setola, Valeria Macchia, Umberto Dello Iacono, Domenico Barbato, and et al. 2022. "Multidetector Computed Tomography (MDCT) Findings of Complications of Acute Cholecystitis. A Pictorial Essay" Tomography 8, no. 2: 1159-1171. https://0-doi-org.brum.beds.ac.uk/10.3390/tomography8020095