
Economic Evaluation of Newborn Screening for Severe Combined Immunodeficiency

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
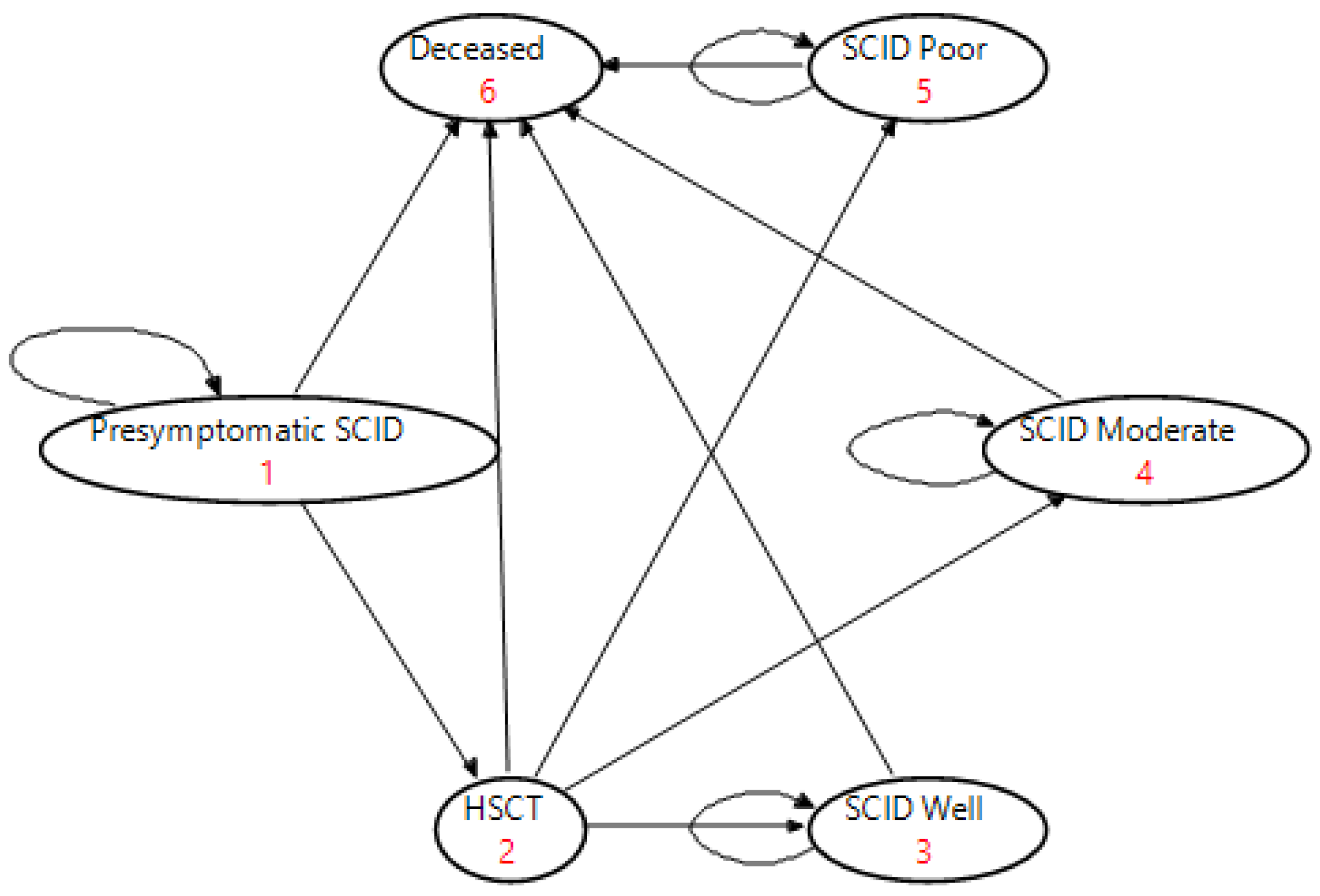
2.1. Intervention Markov Model (NBS and Early HSCT Treatment)
2.2. Comparator Markov Model (Late HSCT without NBS)
2.3. Quality of Life
2.4. Costs
2.5. Cost-Effectiveness Analysis
2.6. Sensitivity Analysis
3. Results
3.1. Cost-Effectiveness of SCID Treatment Strategies Using Markov Simulation
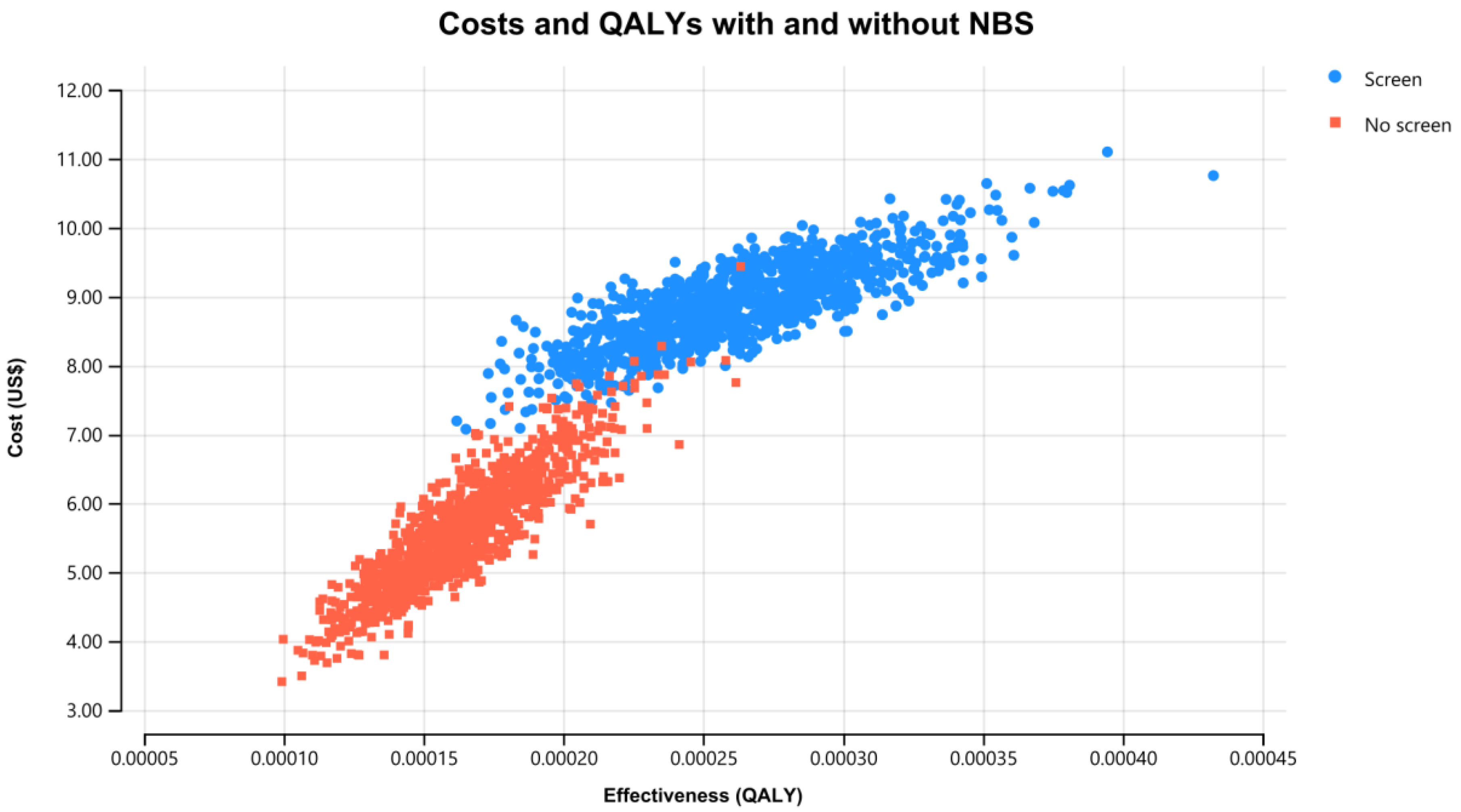
3.2. Cost-Effectiveness of NBS for SCID Including Treatment Strategies
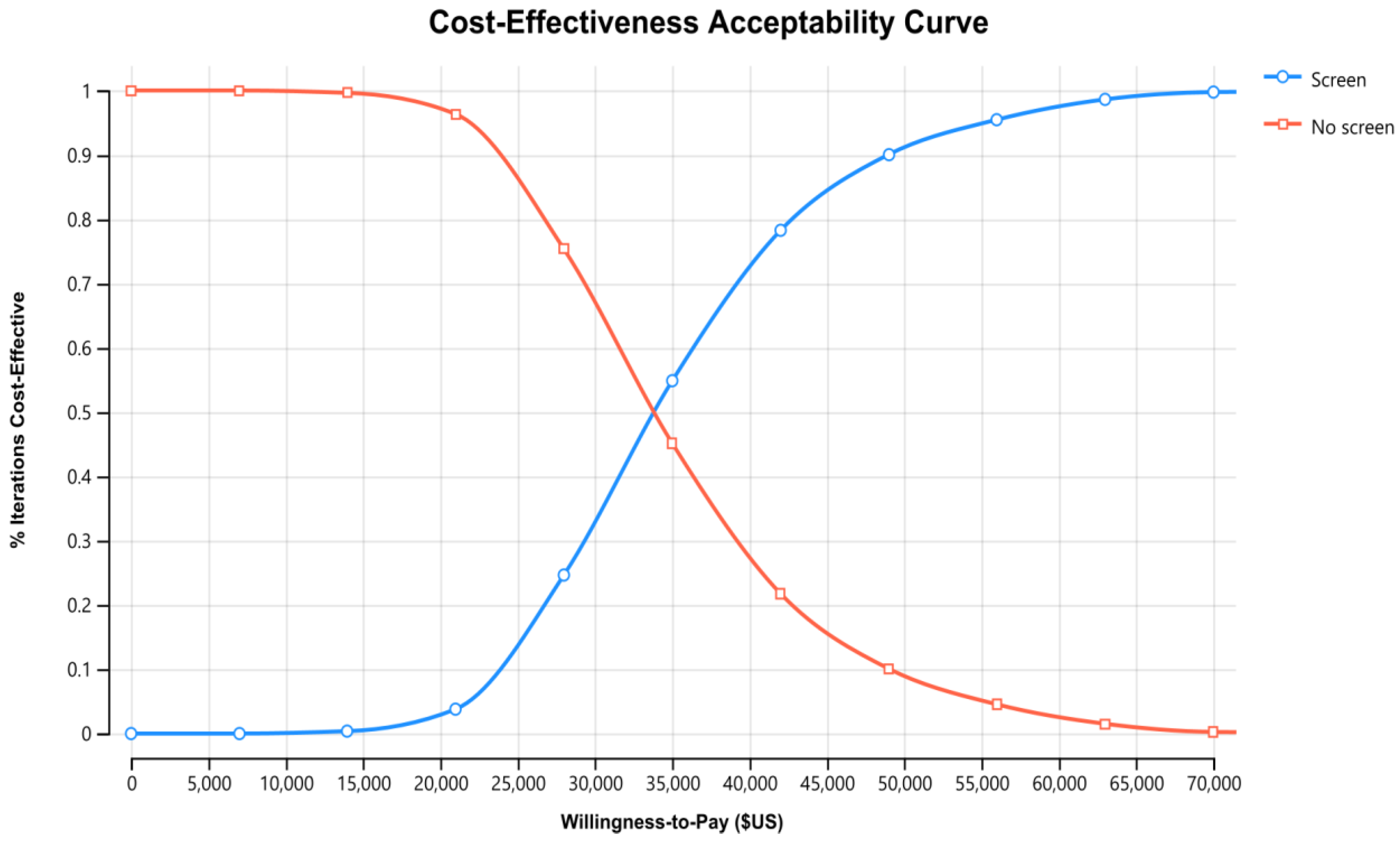
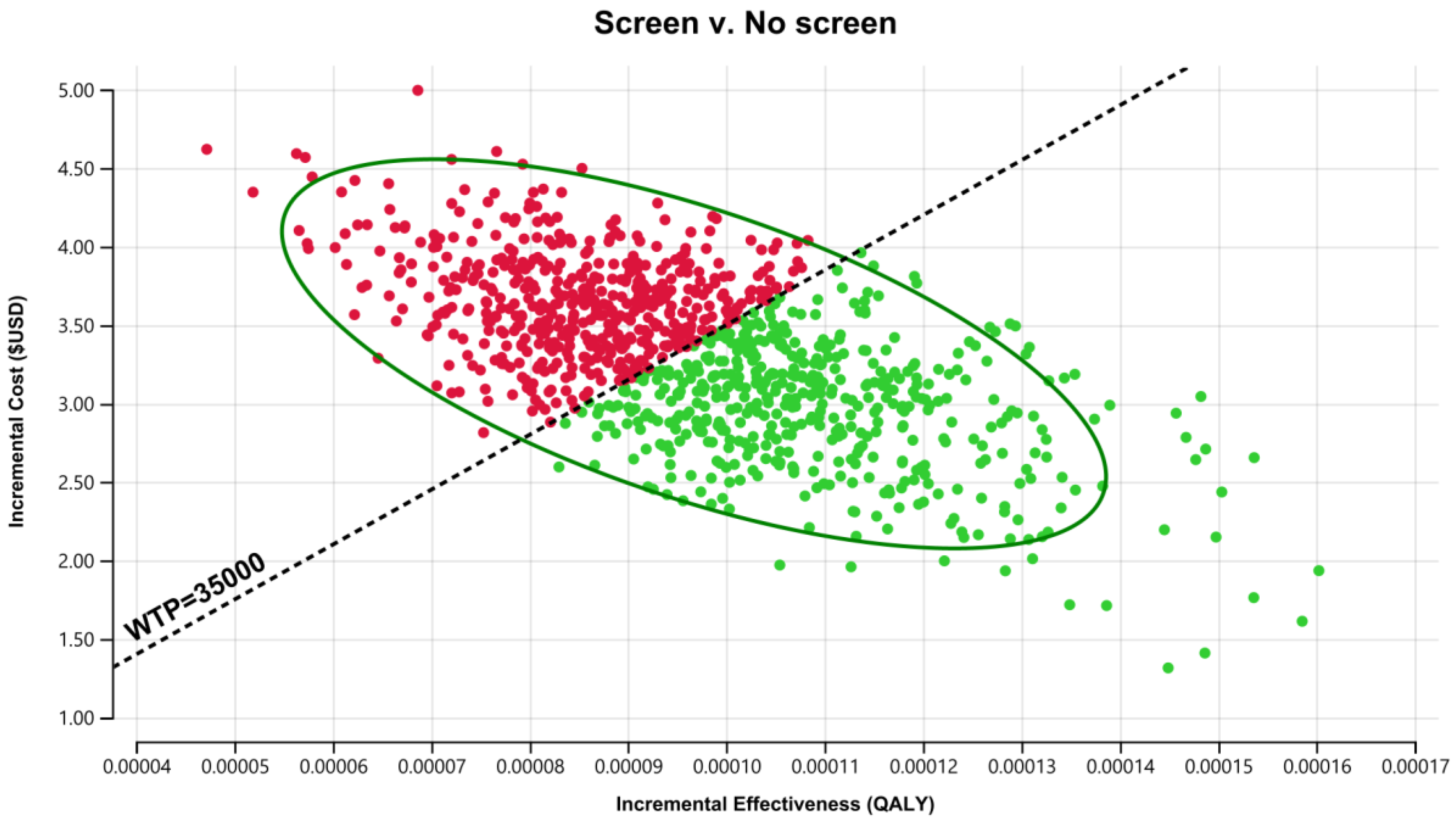
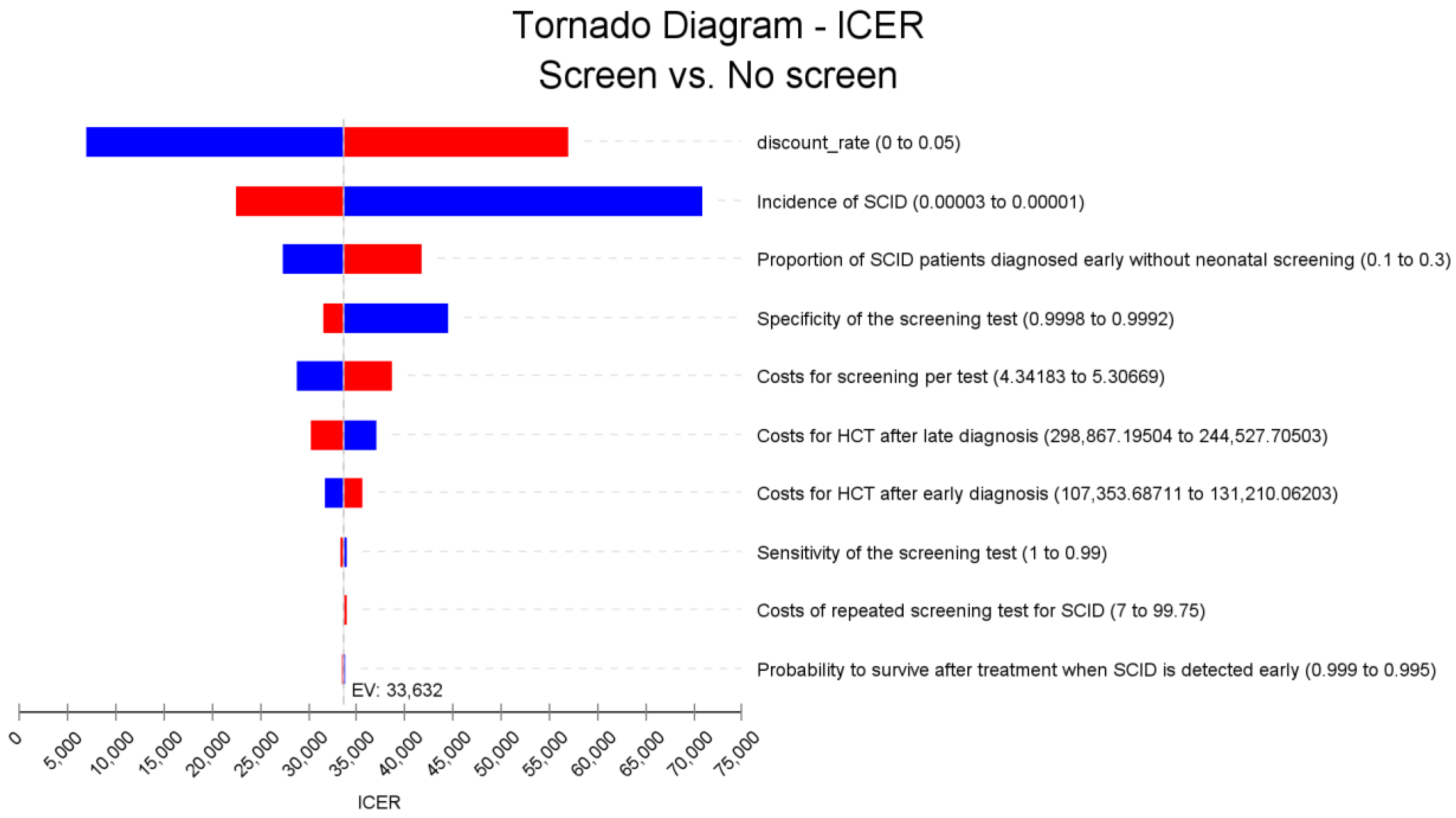
3.3. Sensitivity Analysis for the SCID NBS Cost-Effectiveness Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kwan, A.; Abraham, R.S.; Currier, R.; Brower, A.; Andruszewski, K.; Abbott, J.; Baker, M.; Ballow, M.; Bartoshesky, L.E.; Bonilla, F.A.; et al. Newborn Screening for Severe Combined Immunodeficiency in 11 Screening Programs in the United States. JAMA 2014, 312, 729–738. [Google Scholar] [CrossRef]
- Fischer, A. Severe combined immunodeficiencies (SCID). Clin. Exp. Immunol. 2000, 122, 143–149. [Google Scholar] [CrossRef]
- Lundgren, I.S.; Englund, J.A.; Burroughs, L.M.; Torgerson, T.R.; Skoda-Smith, S. Outcomes and Duration of Pneumocystis jiroveci Pneumonia Therapy in Infants with Severe Combined Immunodeficiency. Pediatr. Infect. Dis. J. 2012, 31, 95–97. [Google Scholar] [CrossRef]
- Kim, K.R.; Kim, J.M.; Kang, J.; Kim, Y. Pneumocystis jirovecii pneumonia in pediatric patients: An analysis of 15 confirmed consecutive cases during 14 years. Korean J. Pediatr. 2016, 59, 252–255. [Google Scholar] [CrossRef] [Green Version]
- Chan, A.; Scalchunes, C.; Boyle, M.; Puck, J.M. Early vs. delayed diagnosis of severe combined immunodeficiency: A family perspective survey. Clin. Immunol. 2011, 138, 3–8. [Google Scholar] [CrossRef] [Green Version]
- Heimall, J.; Logan, B.R.; Cowan, M.J.; Notarangelo, L.D.; Griffith, L.M.; Puck, J.M.; Kohn, D.B.; Pulsipher, M.A.; Parikh, S.; Martinez, C.; et al. Immune reconstitution and survival of 100 SCID patients post–hematopoietic cell transplant: A PIDTC natural history study. Blood 2017, 130, 2718–2727. [Google Scholar] [CrossRef] [Green Version]
- Puck, J.M. Newborn screening for severe combined immunodeficiency and T-cell lymphopenia. Immunol. Rev. 2018, 287, 241–252. [Google Scholar] [CrossRef]
- Wilson, J.M.G.; Jungner, Y.G. Principles and Practice of Screening for Disease; Public Health Papers no. 34; WHO: Geneva, Switzerland, 1968. [Google Scholar]
- Andermann, A.; Blancquaert, I.; Beauchamp, S.; Déry, V. Revisiting Wilson and Jungner in the genomic age: A review of screening criteria over the past 40 years. Bull World Health Organ 2008, 86, 317–319. [Google Scholar]
- Health Partners Consulting Group. Cost-Effectiveness of Newborn Screening for Severe Combined Immune Deficiency. A Report Prepared for the National Screening Unit; Health Partners Consulting Group: Auckland, New Zealand, 2014.
- Ding, Y.; Thompson, J.D.; Kobrynski, L.; Ojodu, J.; Zarbalian, G.; Grosse, S.D. Cost-Effectiveness/Cost-Benefit Analysis of Newborn Screening for Severe Combined Immune Deficiency in Washington State. J. Pediatr. 2016, 172, 127–135. [Google Scholar] [CrossRef] [Green Version]
- Bessey, A.; Chilcott, J.; Leaviss, J.; de la Cruz, C.; Wong, R. A Cost-Effectiveness Analysis of Newborn Screening for Severe Combined Immunodeficiency in the UK. Int. J. Neonatal Screen. 2019, 5, 28. [Google Scholar] [CrossRef] [Green Version]
- Van der Burg, M.; Mahlaoui, N.; Gaspar, H.B.; Pai, S. Universal Newborn Screening for Severe Combined Immunodeficiency (SCID). Front Pediatr. 2019, 7, 373. [Google Scholar] [CrossRef]
- Marle, M.E.V.D.A.-V.; Blom, M.; Van der Burg, M.; Bredius, R.G.M.; Van der Ploeg, C.P.B. Economic Evaluation of Different Screening Strategies for Severe Combined Immunodeficiency Based on Real-Life Data. Int. J. Neonatal Screen. 2021, 7, 60. [Google Scholar] [CrossRef]
- Grosse, S.D.; Thompson, J.D.; Ding, Y.; Glass, M. The Use of Economic Evaluation to Inform Newborn Screening Policy Decisions: The Washington State Experience. Milbank Q. 2016, 94, 366–391. [Google Scholar] [CrossRef] [Green Version]
- Chan, K.; Davis, J.; Pai, S.-Y.; Bonilla, F.A.; Puck, J.M.; Apkon, M. A Markov model to analyze cost-effectiveness of screening for severe combined immunodeficiency (SCID). Mol. Genet. Metab. 2011, 104, 383–389. [Google Scholar] [CrossRef] [Green Version]
- Van der Ploeg, C.P.B.; Blom, M.; Bredius, R.G.M.; van der Burg, M.; Schielen, P.C.J.I.; Verkerk, P.H.; Van den Akker-van Marle, M.E. Cost-effectiveness of newborn screening for severe combined immunodeficiency. Eur. J. Pediatrics 2019, 178, 721–729. [Google Scholar] [CrossRef]
- McGhee, S.A.; Stiehm, E.R.; McCabe, E.R. Potential Costs and Benefits of Newborn Screening for Severe Combined Immunodeficiency. J. Pediatr. 2005, 147, 603–608. [Google Scholar] [CrossRef]
- Kariyawasam, D.S.T.; Russell, J.S.; Wiley, V.; Alexander, I.E.; Farrar, M.A. The implementation of newborn screening for spinal muscular atrophy: The Australian experience. Genet. Med. 2019, 22, 557–565. [Google Scholar] [CrossRef]
- Shih, S.T.F.; Keller, E.; Wiley, V.; Farrar, M.A.; Wong, M.; Chambers, G.M. Modelling the Cost-Effectiveness and Budget Impact of a Newborn Screening Program for Spinal Muscular Atrophy and Severe Combined Immunodeficiency. Int. J. Neonatal Screen. 2022, 8, 45. [Google Scholar] [CrossRef]
- Bessey, A.; Leaviss, J.; Galvan de la Cruz, C.; Chilcott, J.; Wong, R. Cost-Effectiveness of Screening for Severe Combined Immunodeficiency (SCID) in the NHS Newborn Blood Spot Screening Programme; School of Health and Related Research (ScHARR), The University of Sheffield: Sheffield, UK, 2017. [Google Scholar]
- Brown, L.; Xu-Bayford, J.; Allwood, Z.; Slatter, M.; Cant, A.; Davies, E.G.; Veys, P.; Gennery, A.R.; Gaspar, H.B. Neonatal diagnosis of severe combined immunodeficiency leads to significantly improved survival outcome: The case for newborn screening. Blood 2011, 117, 3243–3246. [Google Scholar] [CrossRef] [Green Version]
- Pai, S.-Y.; Logan, B.R.; Griffith, L.M.; Buckley, R.H.; Parrott, R.E.; Dvorak, C.C.; Kapoor, N.; Hanson, I.C.; Filipovich, A.H.; Jyonouchi, S.; et al. Transplantation Outcomes for Severe Combined Immunodeficiency, 2000–2009. N. Engl. J. Med. 2014, 371, 434–446. [Google Scholar] [CrossRef] [Green Version]
- OECD. Purchasing Power Parities (PPP) (Indicator). 2022. Available online: https://data.oecd.org/conversion/purchasing-power-parities-ppp.htm (accessed on 25 March 2022).
- Reserve Bank of Australia. Measures of Consumer Price Inflation. 29 July 2020 20 October 2020. 2020. Available online: https://www.rba.gov.au/inflation/measures-cpi.html#year_ended (accessed on 25 March 2022).
- Yee, A.; De Ravin, S.S.; Elliott, E.; Ziegler, J.B.; Unit, C.T.T.A.P.S. Severe combined immunodeficiency: A national surveillance study. Pediatr. Allergy Immunol. 2008, 19, 298–302. [Google Scholar] [CrossRef]
- Institute for Clinical and Economic Review (ICER). Modifications to the ICER Value Assessment Framework for Treatments for Ultra-Rare Diseases. 2020. Available online: https://icer.org/wp-content/uploads/2020/10/ICER_URD_Framework_Adapt_013120.pdf (accessed on 4 July 2022).
- Prosser, L.A. Defining the Value of Treatments of Rare Pediatric Conditions. JAMA Pediatr. 2018, 172, 1123. [Google Scholar] [CrossRef]
- Drummond, M.F.; Neumann, P.J.; Sullivan, S.D.; Fricke, F.-U.; Tunis, S.; Dabbous, O.; Toumi, M. Analytic Considerations in Applying a General Economic Evaluation Reference Case to Gene Therapy. Value Health 2019, 22, 661–668. [Google Scholar] [CrossRef] [Green Version]
- Garrison, L.P.; Jackson, T.; Paul, D.; Kenston, M. Value-Based Pricing for Emerging Gene Therapies: The Economic Case for a Higher Cost-Effectiveness Threshold. J. Manag. Care Spéc. Pharm. 2019, 25, 793–799. [Google Scholar] [CrossRef]
- Institute for Clinical and Economic Review (ICER). Modifications to the ICER Value Assessment Framework for Treatments for Ultra-Rare Diseases. 2017. Available online: https://icer.org/explore-our-research/policy-papers/orphan-drug-summit-2017/ (accessed on 4 July 2022).
- Mugarab-Samedi, N.; Mugarab-Samedi, V.; Parker, K.; Murguia-Favela, L. 12 Cost-Benefit Analysis of Newborn Screening for Severe Combined Immune Deficiency: Literature review and results transferability. Paediatr. Child Health 2020, 25, e4–e5. [Google Scholar] [CrossRef]
- Taylor, J.L.; Lee, F.K.; Yazdanpanah, G.K.; Staropoli, J.F.; Liu, M.; Carulli, J.P.; Sun, C.; Dobrowolski, S.F.; Hannon, W.H.; Vogt, R.F. Newborn Blood Spot Screening Test Using Multiplexed Real-Time PCR to Simultaneously Screen for Spinal Muscular Atrophy and Severe Combined Immunodeficiency. Clin. Chem. 2015, 61, 412–419. [Google Scholar] [CrossRef] [Green Version]
- Gutierrez-Mateo, C.; Timonen, A.; Vaahtera, K.; Jaakkola, M.; Hougaard, D.M.; Bybjerg-Grauholm, J.; Baekvad-Hansen, M.; Adamsen, D.; Filippov, G.; Dallaire, S.; et al. Development of a Multiplex Real-Time PCR Assay for the Newborn Screening of SCID, SMA, and XLA. Int. J. Neonatal Screen. 2019, 5, 39. [Google Scholar] [CrossRef] [Green Version]
- Phan, H.C.; Taylor, J.L.; Hannon, H.; Howell, R. Newborn screening for spinal muscular atrophy: Anticipating an imminent need. Semin. Perinatol. 2015, 39, 217–229. [Google Scholar] [CrossRef]
- Dangouloff, T.; Vrščaj, E.; Servais, L.; Osredkar, D.; Adoukonou, T.; Aryani, O.; Barisic, N.; Bashiri, F.; Bastaki, L.; Benitto, A.; et al. Newborn screening programs for spinal muscular atrophy worldwide: Where we stand and where to go. Neuromuscul. Disord. 2021, 31, 574–582. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Source | Country | Results |
|---|---|---|
| Chilcott, Bessey [21] | United Kingdom | Detection of 17 affected newborns annually; total gain of 184 discounted QALYs; annual costs of SCID NBS approximately £3.0 million; ICER of £17,600 per QALY gained |
| Bessey, Chilcott [12] | United Kingdom | Screening for SCID was estimated to result in an incremental cost-effectiveness ratio (ICER) of £18,222 with a reduction in SCID mortality from 8.1 (5–12) to 1.7 (0.6–4.0) cases per year of screening. |
| Chan, Davis [16] | USA | Over a 70-year time horizon, the average cost per infant was US$8.89 without screening and US$14.33 with universal screening, ICER US$27,907/QALY. The model predicted that universal screening in the U.S. would cost approximately US$22.4 million/year with a gain of 880 life years and 802 QALYs. |
| Ding, Thompson [11] | USA (Washington State) | Additional 1.19 newborn infants with SCID detected preclinically through screening and 0.40 deaths averted in an annual birth cohort of 86,600 infants. Base-case model suggests an ICER of US$35,311 per life-year saved, and a benefit-cost ratio of either 5.31 or 2.71. |
| Mcghee, Stiehm [18] | USA | A nationwide screening program would cost an additional US$23.9 million per year for screening costs but would result in 760 years of life saved per year of screening. The cost to detect 1 case of SCID would be US$485,000. |
| Health Partners Consulting Group [10] | New Zealand | Adding newborn screening for SCID to the Newborn Metabolic Screening Program (NMSP) may result in saving of 10.0 life years at a cost of NZ30,000 per life-year. |
| Van der Ploeg, Blom [17] | Netherlands | The number of deaths due to SCID per 100,000 children was assessed to decrease from 0.57 to 0.23 and 11.7 quality adjusted life-years (QALYs) gained was expected. Total healthcare costs were €390,800 higher in a situation with screening compared to a situation without screening, resulting in a cost-utility ratio of €33,400 per QALY gained. |
| Van den Akker-Van Marle [14] | Netherlands | Cost-effectiveness ratios varied from € 41,300 per QALY for the screening strategy with T-cell receptor excision circle (TREC) ≤ 6 copies/punch to € 44,100 for the screening strategy with a cut-off value of TREC ≤ 10 copies/punch |
| Parameters | Expected Values | Distribution | Low | High | Source |
|---|---|---|---|---|---|
| Cost Parameters | US$ (A$) | ||||
| Screening test cost | $4.82 ($7) | Gamma | −10% | +10% | NBS Pilot |
| Repeat screening test cost | $6.89 ($10) | Gamma | 7 | 25 | NBS Pilot |
| Confirmatory diagnostic testing cost (after positive screening test) | $2119 ($3074) | [17] | |||
| Diagnostic testing cost (without NBS) | $3446 ($5000) | [17] | |||
| Pre-symptomatic cost | $0 ($0) | Assumption | |||
| HSCT cost (early diagnosis) | $119,282 ($173,078) | Gamma | −10% | +10% | [17] |
| HSCT cost (late diagnosis) | $271,697 ($394,233) | Gamma | −10% | +10% | [17] |
| Treatment cost for SCID patient dying prior to HSCT | $178,923 ($259,617) | [17] | |||
| SCID Well treatment cost (per year) | $34 ($50) | [17] | |||
| SCID Moderate treatment cost (per year) | $24,052 ($34,900) | [17] | |||
| SCID Poor treatment cost (per year) | $12,873 ($18,679) | [17] | |||
| End-of-life costs (SCID Moderate & SCID Poor) | $41,841 ($60,712) | [17] | |||
| SCID Well productivity cost | $0 | Assumption | |||
| SCID Moderate productivity cost | $1394 ($2023) | [17] | |||
| SCID Poor productivity cost | $0 ($0) | Assumption | |||
| Netherlands, 2016 PPP Euros/US$ | 0.796 | [24] | |||
| Australia, 2016 PPP A$/US$ | 1.45 | [24] | |||
| CPI inflation rate 2016 to 2019 A$ | 0.0557 | [25] | |||
| Discount rate | 0.03 | - | 0.05 | ||
| Outcome Parameters | |||||
| SCID incidence | 0.00002 | Beta | 0.000012 | 0.000025 | [1,26] |
| False Negative % in Screen (1-sensitivity) | 0.005 | Beta | 0 | 0.01 | [11] |
| False Positive % in Screen (1-specificity) | 0.0003 | Beta | 0.0002 | 0.0008 | [11] |
| % of patients early diagnosed without NBS | 0.2 | Beta | 0.1 | 0.3 | [16] |
| Probability to survive until treatment (early diagnosis) | 0.9423 | [1] | |||
| Probability to survive until treatment (late diagnosis) | 0.78 | [11] | |||
| 5-year survival (early diagnosis) | 0.94 | Beta | 0.91 | 0.98 | [23] |
| 5-year survival (late diagnosis) | 0.82 | Beta | 0.7 | 0.9 | [23] |
| SCID Well after HSCT (early diagnosis; surviving subjects) | 0.8 | [17] | |||
| SCID Moderate after HSCT (early diagnosis; surviving subjects) | 0.15 | [17] | |||
| SCID Poor after HSCT (early diagnosis; surviving subjects) | 0.05 | [17] | |||
| SCID Well after HSCT (late diagnosis; surviving subjects) | 0.5 | [17] | |||
| SCID Moderate after HSCT (late diagnosis; surviving subjects) | 0.3 | [17] | |||
| SCID Poor after HSCT (late diagnosis; surviving subjects) | 0.2 | [17] | |||
| Quality of Life Utility Value | |||||
| Utility value for pre-symptomatic SCID | 0.95 | Assumption | |||
| Utility value for SCID Well | 0.95 | [17] | |||
| Utility value for SCID Moderate | 0.75 | [17] | |||
| Utility value for SCID Poor | 0.5 | [17] | |||
| Utility value for HSCT | 0.5 | Assumption | |||
| Utility value for Deceased | 0 | Assumption |
| SCID Treatment Strategies | |||||
|---|---|---|---|---|---|
| Strategy | Cost | Incremental Cost | QALY | Incremental QALY | ICER |
| 5 years | (95% CI) | (95% CI) | (95% CI) | (95% CI) | (95% CI) |
| Late HSCT for SCID | $258,133 (247,010, 270,047) | - | 1.97078 (1.75538, 2.16004) | - | |
| Early HSCT for SCID | $135,624 (128,784, 142,120) | −$122,509 (−135,775, −108,190) | 3.50035 (3.49305, 3.50572) | 1.52957 (1.33976, 1.74600) | Dominant (dominant, dominant) |
| 60 years | |||||
| Late HSCT for SCID | $306,090 (292,494, 319,609) | - | 6.90880 (6.06863, 7.64696) | - | |
| Early HSCT for SCID | $169,177 (162,819, 175,859) | −$136,914 (−151,178, −121,509) | 13.05174 (13.01996, 13.07145) | 6.14293 (5.40464, 6.97026) | Dominant (dominant, dominant) |
| NBS for SCID | |||||
| Strategy | Cost | Incremental Cost | QALY | Incremental QALY | ICER |
| 5 years | (95% CI) | (95% CI) | (95% CI) | (95% CI) | (95% CI) |
| No screen with late HSCT | $4.67 (3.37, 6.30) | - | 0.00005 (0.00003, 0.00006) | - | - |
| Screen with early HSCT | $8.19 (7.18, 9.28) | $3.51 (2.48, 4.40) | 0.00007 (0.00005, 0.00009) | 0.00002 (0.000017, 0.000034) | $144,487 (79,155, 242,744) |
| 60 years | |||||
| No screen with late HSCT | $5.57 (4.02, 7.29) | - | 0.00016 (0.00012, 0.00021) | - | - |
| Screen with early HSCT | $8.86 (7.71, 10.08) | $3.28 (2.26, 4.24) | 0.00026 (0.00019, 0.00034) | 0.00010 (0.00007, 0.00013) | $33,632 (17,897, 59,441) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shih, S.T.F.; Keller, E.; Wiley, V.; Wong, M.; Farrar, M.A.; Chambers, G.M. Economic Evaluation of Newborn Screening for Severe Combined Immunodeficiency. Int. J. Neonatal Screen. 2022, 8, 44. https://0-doi-org.brum.beds.ac.uk/10.3390/ijns8030044
Shih STF, Keller E, Wiley V, Wong M, Farrar MA, Chambers GM. Economic Evaluation of Newborn Screening for Severe Combined Immunodeficiency. International Journal of Neonatal Screening. 2022; 8(3):44. https://0-doi-org.brum.beds.ac.uk/10.3390/ijns8030044
Chicago/Turabian StyleShih, Sophy T. F., Elena Keller, Veronica Wiley, Melanie Wong, Michelle A. Farrar, and Georgina M. Chambers. 2022. "Economic Evaluation of Newborn Screening for Severe Combined Immunodeficiency" International Journal of Neonatal Screening 8, no. 3: 44. https://0-doi-org.brum.beds.ac.uk/10.3390/ijns8030044