
Total Face Approach (TFA) 3D Cephalometry and Superimposition in Orthognathic Surgery: Evaluation of the Vertical Dimensions in a Consecutive Series


 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
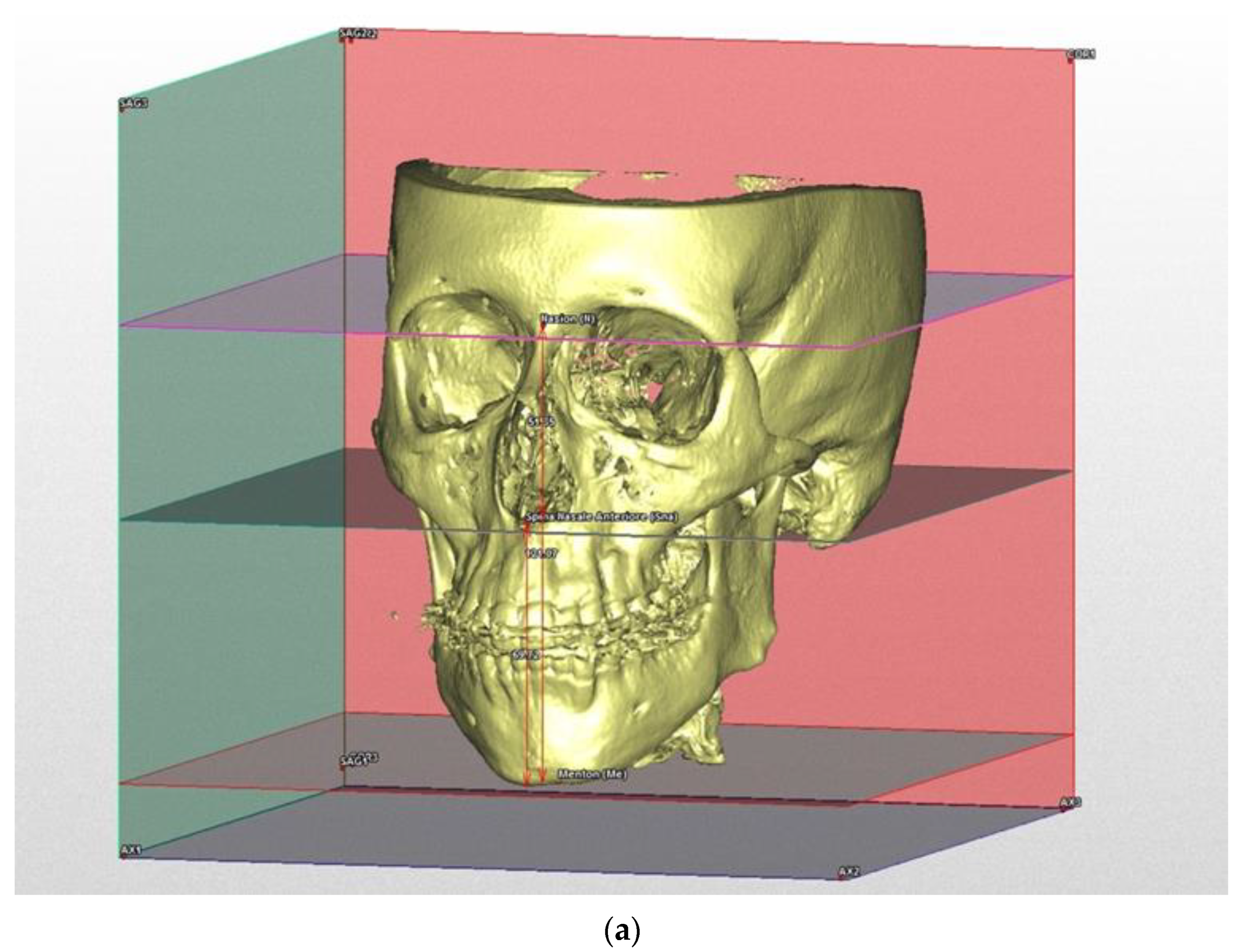
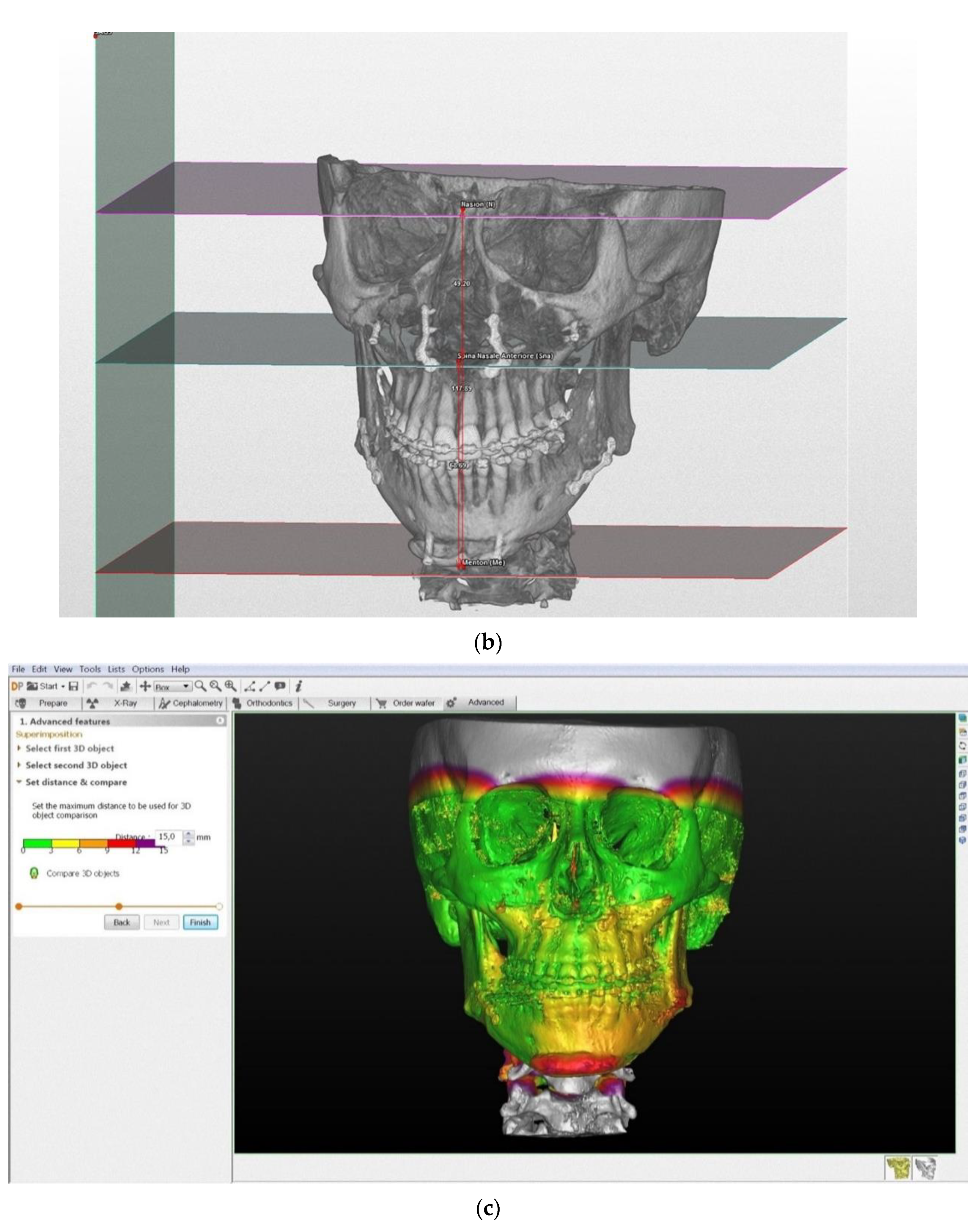
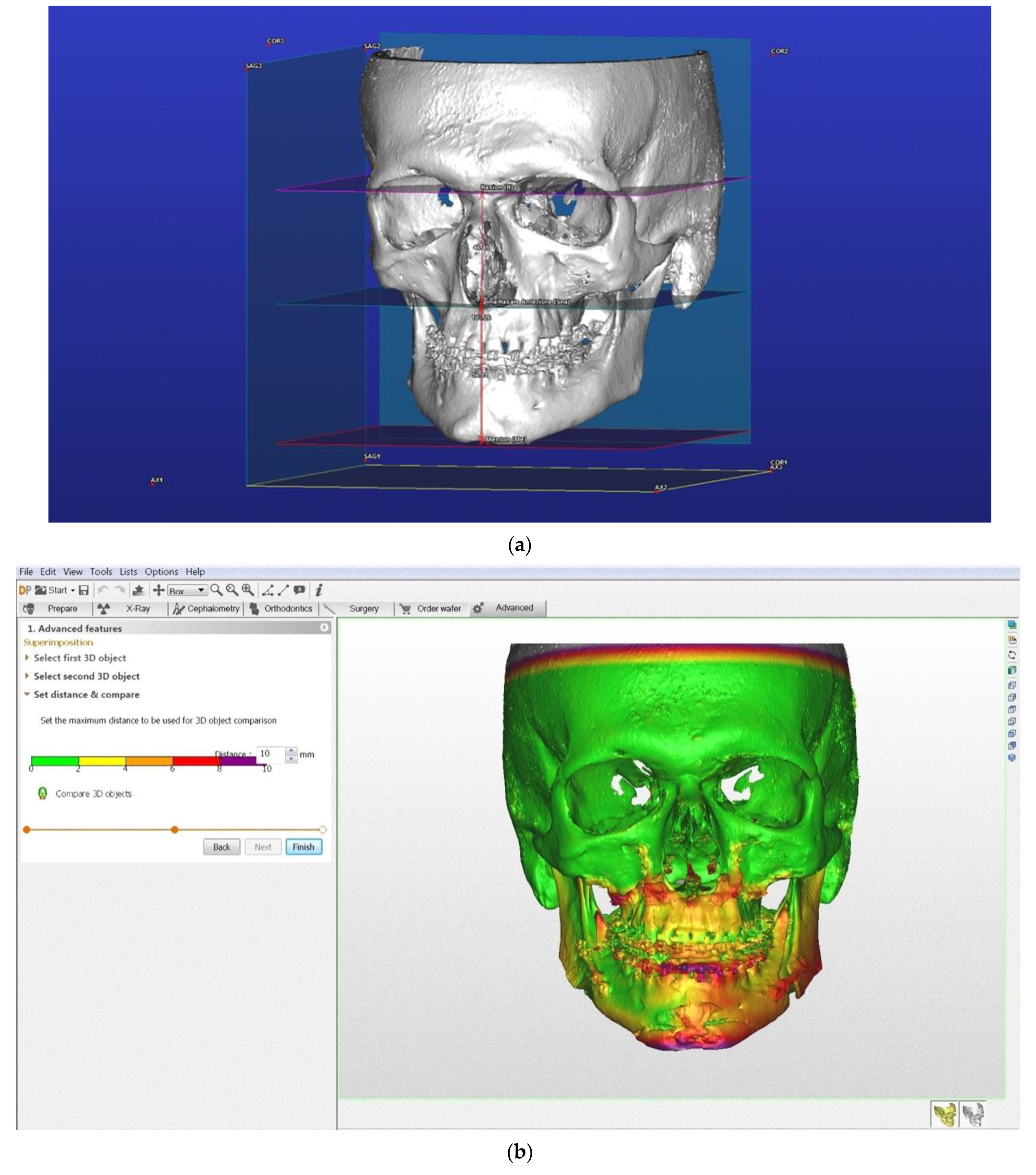
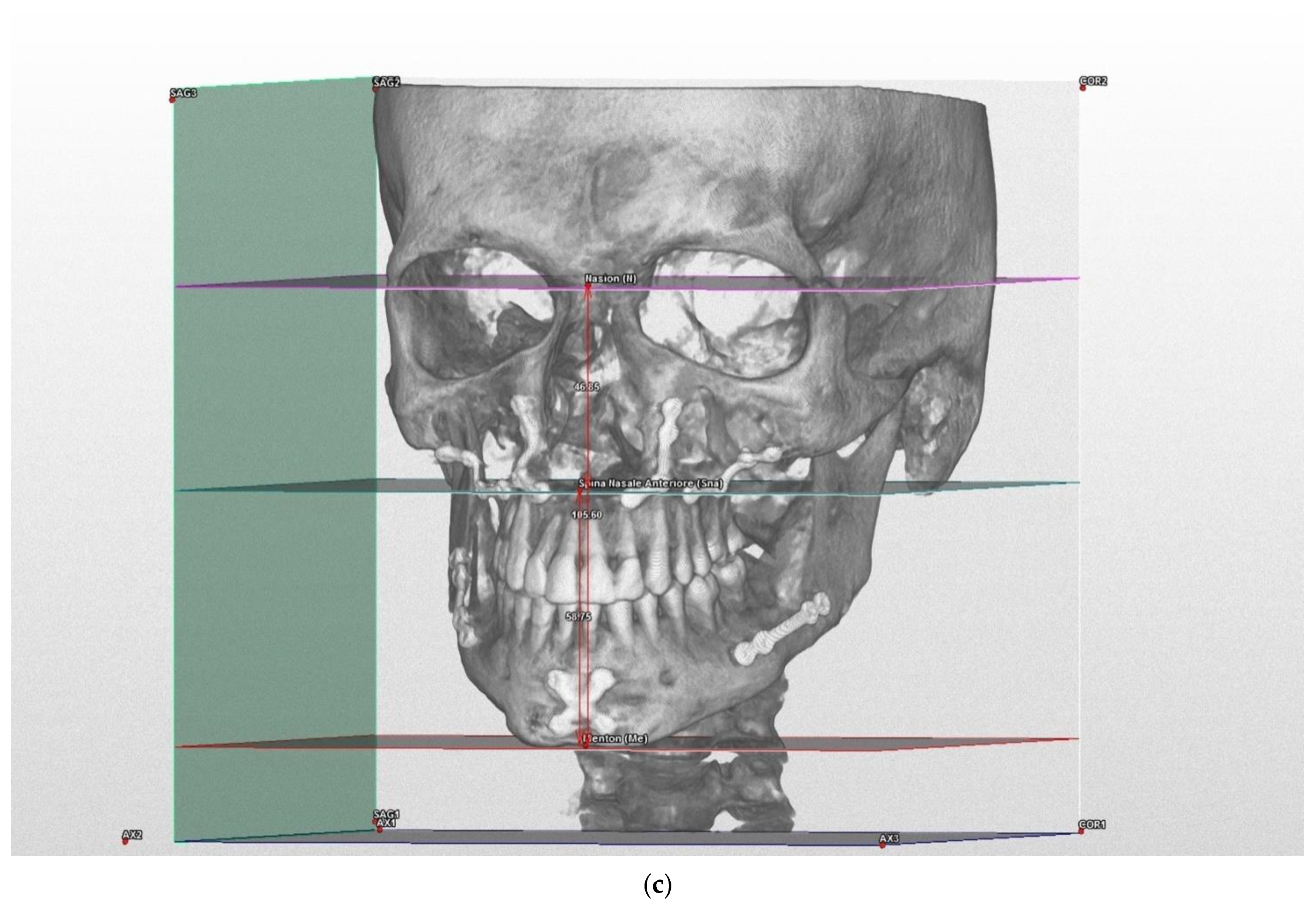
- The Anterior-Superior Vertical dimension: distance between SFP and ANS point.
- The Anterior-Superior Vertical dimension: distance between ANSP and Menton point.
- Total Anterior Vertical dimension: distance between MP and the Nasion point.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Perrotti, G.; De Vecchi, L.; Testori, T.; Weinstein, R. Analisi facciale globale: Approccio diagnostico-terapeutico multidisciplinare alla riabilitazione implantare complessa. Ital. Oral Surg. 2012, 11, 108–116. [Google Scholar] [CrossRef]
- Ackerman, J.L.; Proffit, W.R. Soft tissue limitations in orthodontics: Treatment planning guidelines. Angle Orthod. 1997, 67, 327–336. [Google Scholar] [PubMed]
- Westermark, A.; Zachow, S.; Eppley, B.L. Three-Dimensional Osteotomy Planning in Maxillofacial Surgery Including Soft Tissue Prediction. J. Craniofacial Surg. 2005, 16, 100–104. [Google Scholar] [CrossRef] [PubMed]
- Gateno, J.; Xia, J.J.; Teichgraeber, J.F. New 3-Dimensional Cephalometric Analysis for Orthognathic Surgery. J. Oral Maxillofac. Surg. 2011, 69, 606–622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plooij, J.M.; Maal, T.J.J.; Haers, P.; Borstlap, W.A.; Kuijpers-Jagtman, A.M.; Bergé, S.J. Digital three-dimensional image fusion processes for planning and evaluating orthodontics and orthognathic surgery. A systematic review. Int. J. Oral Maxillofac. Surg. 2011, 40, 341–352. [Google Scholar] [CrossRef]
- Perrotti, G.; Politi, M.; Testori, T. 3D Imaging and Dentistry-From Multiplanar Cephalometry to Guided Navigation in Implantology; Quintessenza Edizione: Milan, Italy, 2014; pp. 205–288. [Google Scholar]
- Perrotti, G.; Politi, M.; Testori, T. Analisi cefalometrica 3D: La ricerca di valori norma. Quintessenza Ed. 2016, 32, 29–36. [Google Scholar]
- Jiang, J.; Xu, T.; Lin, J. The Relationship Between Estimated and Registered Natural Head Position. Angle Orthod. 2007, 77, 1019–1024. [Google Scholar] [CrossRef] [PubMed]
- Perrotti, G.; Baccaglione, G.; Clauser, T.; Testarelli, L.; Del Fabbro, M.; Testori, T. Total Face Approach (TFA): A Novel 3D Approach to Describe the Main Cephalometric Craniomaxillofacial Parameters. Methods Protoc. 2021, 4, 15. [Google Scholar] [CrossRef] [PubMed]
- Swennen, G.R.J.; Schutyser, F.; Barth, E.-L.; de Groeve, P.; de Mey, A. A New Method of 3-D Cephalometry Part I: The Anatomic Cartesian 3-D Reference System. J. Craniofacial Surg. 2006, 17, 314–325. [Google Scholar] [CrossRef]
- Farronato, G.; Garagiola, U.; Dominici, A.; Periti, G.; de Nardi, S.; Carletti, V.; Farronato, D. “Ten-point” 3D cephalometric analysis using low-dosage cone beam computed tomography. Prog. Orthod. 2010, 11, 2–12. [Google Scholar] [CrossRef]
- Johnston, C.; Burden, D.; Kennedy, D.; Harradine, N.; Stevenson, M. Class III surgical-orthodontic treatment: A cephalometric study. Am. J. Orthod. Dentofac. Orthop. 2006, 130, 300–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turpin, D.L. The need for video imaging. Angle Orthod. 1995, 65, 243. [Google Scholar] [PubMed]
- Cevidanes, L.H.; Oliveira, A.E.F.; Grauer, D.; Styner, M.; Proffit, W.R. Clinical Application of 3D Imaging for Assessment of Treatment Outcomes. Semin. Orthod. 2011, 17, 72–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cevidanes, L.H.; Bailey, L.J.; Tucker, S.F.; Styner, M.A.; Mol, A.; Phillips, C.L.; Proffit, W.R.; Turvey, T. Three-dimensional cone-beam computed tomography for assessment of mandibular changes after orthognathic surgery. Am. J. Orthod. Dentofac. Orthop. 2007, 131, 44–50. [Google Scholar] [CrossRef] [Green Version]
- Cevidanes, L.H.; Tucker, S.; Styner, M.; Kim, H.; Chapuis, J.; Reyes, M.; Proffit, W.; Turvey, T.; Jaskolka, M. Three-dimensional surgical simulation. Am. J. Orthod. Dentofac. Orthop. 2010, 138, 361–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- da Motta, A.T.S.; Carvalho, F.D.R.; Cevidanes, L.H.S.; Almeida, M.A.D. Assessment of mandibular advancement surgery with 3D CBCT models superimposition. Dent. Press J. Orthod. 2010, 15, 45e1–45e45. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 0–3 | 3–6 | 6–9 | 9–12 | 12–15 | mm |
| Vertical Analysis of Patient Skeletal Class II | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| TFA | Superimposition (Highest Values) | Superimposition (Most Common Values) | |||||||||||||
| Pre | Post | ∆ | ∆ | ∆ | |||||||||||
| N-Sna | Sna-me | N-Me | N-Sna | Sna-me | N-Me | ∆ N-Sna | ∆ Sna-Me | ∆ N-Me | ∆ N-Sna | ∆ Sna-Me | ∆ N-Me | ∆ N-Sna | ∆ Sna-Me | ∆ N-Me | |
| B.M. | 51.3 | 69.72 | 121.07 | 48.4 | 68.04 | 116.44 | 2.9 | 1.68 | 4.63 | ||||||
| B.L. | 46.72 | 54.75 | 101.47 | 45.3 | 60.63 | 105.93 | 1.42 | −5.88 | −4.46 | ||||||
| G.A. | 51.74 | 66.62 | 118.36 | 46.61 | 70.26 | 116.86 | 5.13 | −3.64 | 1.5 | ||||||
| H.A. | 49.91 | 67.75 | 117.66 | 45.19 | 64.4 | 109.59 | 4.72 | 3.35 | 8.07 | ||||||
| S.L. | 56.69 | 80.75 | 137.44 | 48.73 | 79.74 | 128.47 | 7.96 | 1.01 | 8.97 | ||||||
| S.D. | 45.73 | 56.45 | 102.19 | 49.4 | 59.64 | 109.04 | −3.67 | −3.19 | −6.85 | ||||||
| T.M | 47.16 | 59.04 | 106.2 | 47.16 | 66.6 | 113.76 | 0 | −7.56 | −7.56 | ||||||
| Vertical Analysis of Patient Skeletal Class III | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| TFA | Superimposition (Highest Values) | Superimposition (Most Common Values) | |||||||||||||
| Pre | Post | ∆ | ∆ | ∆ | |||||||||||
| N-Sna | Sna-me | N-Me | N-Sna | Sna-me | N-Me | ∆ N-Sna | ∆ Sna-Me | ∆ N-Me | ∆ N-Sna | ∆ Sna-Me | ∆ N-Me | ∆ N-Sna | ∆ Sna-Me | ∆ N-Me | |
| B.F. | 50.17 | 74.87 | 125.04 | 50.67 | 67.56 | 118.22 | −0.5 | 7.31 | 6.82 | ||||||
| D.B.N. | 52.78 | 73.7 | 126.48 | 53.24 | 73.85 | 127.09 | −0.46 | −0.15 | −0.61 | ||||||
| M.S. | 50.53 | 74.07 | 124.59 | 46.4 | 68.33 | 114.74 | 4.13 | 5.74 | 9.85 | ||||||
| P.E. | 51.86 | 66.62 | 118.48 | 54.84 | 62.24 | 117.09 | −2.98 | 4.38 | 1.39 | ||||||
| T.D. | 53.02 | 73.06 | 126.07 | 55.28 | 72.88 | 128.16 | −2.26 | 0.18 | −2.09 | ||||||
| V.S. | 51.09 | 73.46 | 124.55 | 48.86 | 65.14 | 114 | 2.23 | 8.32 | 10.55 | ||||||
| TFA Multiplane 3D Cephalometry | |
|---|---|
| Pros | Cons |
| Reference points available for patient classification | Does not indicate the skeletal base where the greatest variation has occurred |
| Allows extremely accurate evaluation | Limited software types available for this kind of analysis |
| An objective method | |
| User-friendly interface | |
| Fast execution | |
| Easy to learn | |
| Superimposition | |
|---|---|
| Pros | Cons |
| Highly intuitive, useful for the orthodontist, patient and maxillo-facial surgeon | Reference points not available for patient classification |
| Identifies the area with the greatest variation | Uses variable ranges that are operator dependent |
| Requires few reference landmarks in the areas not involved in the surgical variations | |
| Applicable to all available software | |
| Highly intuitive, useful for the orthodontist, patient and maxillo-facial surgeon | |
| Identifies the area with the greatest variation | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perrotti, G.; Baccaglione, G.; Clauser, T.; Scaini, R.; Grassi, R.; Testarelli, L.; Reda, R.; Testori, T.; Del Fabbro, M. Total Face Approach (TFA) 3D Cephalometry and Superimposition in Orthognathic Surgery: Evaluation of the Vertical Dimensions in a Consecutive Series. Methods Protoc. 2021, 4, 36. https://0-doi-org.brum.beds.ac.uk/10.3390/mps4020036
Perrotti G, Baccaglione G, Clauser T, Scaini R, Grassi R, Testarelli L, Reda R, Testori T, Del Fabbro M. Total Face Approach (TFA) 3D Cephalometry and Superimposition in Orthognathic Surgery: Evaluation of the Vertical Dimensions in a Consecutive Series. Methods and Protocols. 2021; 4(2):36. https://0-doi-org.brum.beds.ac.uk/10.3390/mps4020036
Chicago/Turabian StylePerrotti, Giovanna, Giulia Baccaglione, Tommaso Clauser, Riccardo Scaini, Roberta Grassi, Luca Testarelli, Rodolfo Reda, Tiziano Testori, and Massimo Del Fabbro. 2021. "Total Face Approach (TFA) 3D Cephalometry and Superimposition in Orthognathic Surgery: Evaluation of the Vertical Dimensions in a Consecutive Series" Methods and Protocols 4, no. 2: 36. https://0-doi-org.brum.beds.ac.uk/10.3390/mps4020036