
A Randomized Controlled Trial Protocol for Using an Accelerometer-Smartphone Application Intervention to Increase Physical Activity and Improve Health among Employees in a Military Workplace

 , , and
, , and
Abstract
:1. Introduction
2. Methods/Design
2.1. Participants
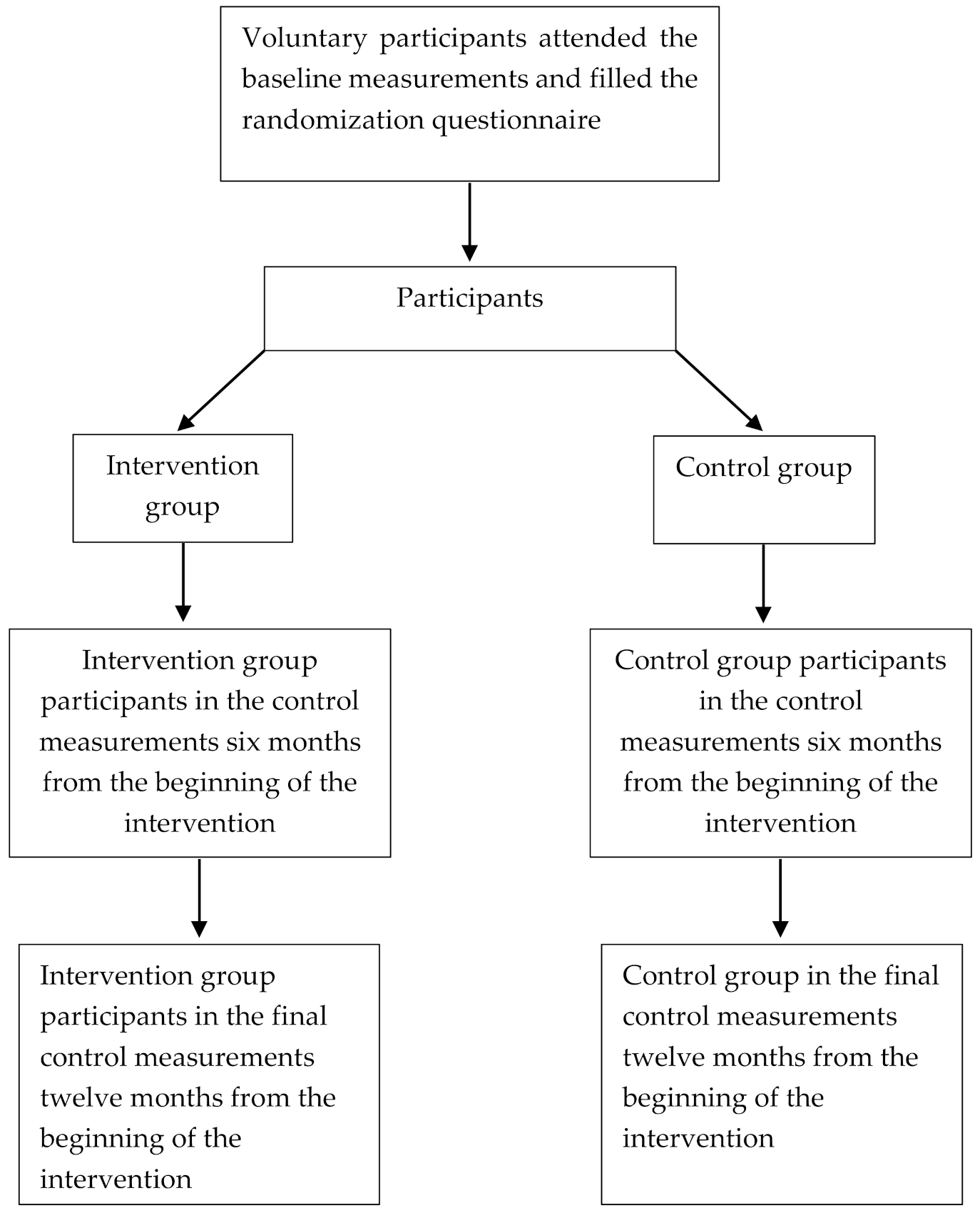
2.2. Randomization
2.3. Power Calculation and Sample Size
2.4. Intervention
2.4.1. Intervention Group
Accelerometer Measurements during the Intervention and Smartphone Application Feedback
Telephone Counselling
Training Diary
2.4.2. Control Group
2.5. Measurements
2.5.1. The Questionnaire
2.5.2. Fitness Tests
2.5.3. Body Composition
2.5.4. Blood Samples and Analyses
2.5.5. Baseline and Control Accelerometer Measurements
2.5.6. Feedback from the Measurements
3. Results
3.1. Primary Outcomes
3.2. Secondary Outcomes
3.3. Reach
3.4. Effectiveness
3.5. Maintenance
3.6. Statistical Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Warburton, D.; Nicol, C.; Bredin, S. Health benefits of physical activity: The evidence. Can. Med. Assoc. J. 2006, 174, 801–809. [Google Scholar] [CrossRef] [Green Version]
- Kline, C. The bidirectional relationship between exercise and sleep: Implications for exercise adherence and sleep improvement. Am. J. Lifestyle Med. 2014, 8, 375–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahima, R.; Lazar, M. The health risk of obesity-better metrics imperative. Science 2013, 341, 856–858. [Google Scholar] [CrossRef] [PubMed]
- Bigaard, J.; Frederiksen, K.; Tjønneland, A.; Thomsen, B.L.; Overvad, K.; Heitmann, B.L.; Sørensen, T.I.A. Waist circumference and body composition in relation to all-cause mortality in middle-aged men and women. Int. J. Obes. 2005, 29, 778–784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Achten, J.; Venables, M.; Jeukendrup, A. Fat oxidation rates are higher during running compared with cycling over a wide range of intensities. Metabolism 2003, 52, 747–752. [Google Scholar] [CrossRef]
- Donnelly, J.; Blair, S.; Jakicic, J.; Jakicic, J.; Manore, M.; Rankin, J.; Smith, B. American College of Sports Medicine Position Stand. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Med. Sci. Sports Exerc. 2009, 41, 459. [Google Scholar] [CrossRef] [PubMed]
- Amlani, N.; Munir, F. Does physical activity have an impact on sickness absence? A review. Sports Med. 2014, 44, 887–907. [Google Scholar] [CrossRef] [Green Version]
- Sjøgaard, G.; Christensen, J.; Justesen, J.; Murray, M.; Dalager, T.; Fredslund, G.; Sjøgaard, K. Exercise is more than medicine: The working age population’s well-being and productivity. J. Sport Health Sci. 2016, 5, 159–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Husu, P.; Tokola, K.; Vähä-Ypyä, H.; Sievänen, H. Physical activity, sedentary behavior and bedtime among Finnish adults measured 24/7 tri-axial accelerometery. J. Meas. Phys. Behav. 2021, 4, 163–173. [Google Scholar] [CrossRef]
- Honkamaa, S.; Hyppönen, H. PVHSM koulutusala 043-PEHENKOS palkatun henkilöstön kenttäkelpoisuus ja fyysinen työkyky; TAMPEREEN YLIOPISTO: Tampere, Finland, 2014. (In Finnish) [Google Scholar]
- Pihlainen, K. Puolustusvoimien Palkatun Henkilöstön Liikunta-Aktiivisuuden Yhteys Terveyden Riskitekijöihin Ja Suositukset Palveluiden Kehittämiseksi; Haaga-Helia: Helsinki, Finland, 2010; (In Finnish, abstract available in English). [Google Scholar]
- Kyröläinen, H.; Häkkinen, K.; Kautiainen, H.; Santtila, M.; Pihlainen, K.; Häkkinen, A. Physical fitness, BMI and sickness absence in male military personnel. Occup. Med. 2008, 58, 251–256. [Google Scholar] [CrossRef] [Green Version]
- The Defence Command’s Personnel Division. Statement of Human Resources 2016; Juvenes Print: Naulakatu, Finland, 2017. [Google Scholar]
- Dalager, T.; Justesen, J.; Murray, M.; Boyle, E.; Sjøgaard, G. Implementing intelligent physical exercise training at the workplace: Health effects among office workers—A randomized controlled trial. Eur. J. Appl. Physiol. 2016, 116, 1433–1442. [Google Scholar] [CrossRef]
- Prieske, O.; Dalager, T.; Herz, M.; Hortobagyi, T.; Sjøgaard, G.; Søgaard, K.; Granacher, U. Effects of Physical exercise training in the workplace on physical fitness: A systematic review and meta-analysis. Sports Med. 2019, 49, 1903–1921. [Google Scholar] [CrossRef]
- Proper, K.; Koning, M.; Van der Beerk, A.; Hildebrandt, V.; Bosscher, R.; van Mechelen, W. The Effectiveness of worksite physical activity programs on physical activity, physical fitness, and health. Clin. J. Sport Med. 2003, 13, 106–117. [Google Scholar] [CrossRef]
- Gutherie, N.; Bradlyn, A.; Thompson, S.; Yen, S.; Haritatos, J.; Dillon, F.; Cole, S. Development of an accelerometer-linked online intervention system to promote physical activity in adolescents. PLoS ONE 2015, 10, e0128639. [Google Scholar] [CrossRef]
- Goode, A.; Hall, K.; Batch, B.; Huffman, K.; Hastings, S.; Allen, K.; Shaw, R.; Kanach, F.; McDuffie, J.; Kosinksi, A. The Impact of interventions that integrate accelerometers on physical activity and weight loss: A systematic review. Ann. Behav. Med. 2017, 51, 79–93. [Google Scholar] [CrossRef] [Green Version]
- Hodkinson, A.; Kontopantelis, E.; Adeniji, C.; van Marwijk, H.; McMillan, B.; Bower, P.; Panagioti, M. Accelerometer- and pedometer-based physical activity interventions among adults with cardiometabolic conditions: A systematic review and meta-analysis. JAMA Netw. Open 2019, 2, e1912895. [Google Scholar] [CrossRef] [Green Version]
- Bort-Roig, J.; Gilson, N.; Puig-Ribera, A.; Contreras, R.; Trost, S. Measuring and influencing physical activity with smartphone technology: A systematic review. Sports Med. 2014, 44, 671–686. [Google Scholar] [CrossRef]
- Vähä-Ypyä, H.; Vasankari, T.; Husu, P.; Mänttäri, A.; Vuorimaa, T.; Suni, J.; Sievänen, H. Validation of Cut-points for evaluating the intensity of physical activity with accelerometery-based mean amplitude deviation (MAD). PLoS ONE 2015, 10, e0134813. [Google Scholar] [CrossRef] [Green Version]
- Vähä-Ypyä, H.; Vasankari, T.; Husu, P.; Suni, J.; Sievänen, H. A universal, accurate intensity-based classification of different physical activities using raw data of accelerometer. Clin. Physiol. Funct. Imaging 2015, 35, 64–70. [Google Scholar] [CrossRef]
- Aittasalo, M.; Vähä-Ypyä, H.; Vasankari, T.; Husu, P.; Jussila, A.-M.; Sievänen, H. Mean amplitude deviation calculated from raw acceleration data: A novel method for classifying the intensity of adolescents’ physical activity irrespective of accelerometer brand. BMC Sports Sci. Med. Rehabil. 2015, 7, 18. [Google Scholar] [CrossRef] [Green Version]
- Vasankari, V.; Halonen, J.; Husu, P.; Vähä-Ypyä, H.; Tokola, K.; Suni, J.; Sievänen, H.; Anttila, V.; Airaksinen, J.; Vasankari, T.; et al. Personalised eHealth intervention to increase physical activity and reduce sedentary behaviour in rehabilitation after cardiac operations: Study protocol for the PACO randomized controlled trial (NCT03470246). BMJ Open Sport Exerc. Med. 2019, 5, e000539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kujala, U.; Vaara, J.; Kainulainen, H.; Vasankari, T.; Vaara, E.; Kyröläinen, H. Associations of aerobic fitness and maximal muscular strength with metabolites in ypung men. JAMA Netw. Open 2019, 2, e198265. [Google Scholar] [CrossRef] [PubMed]
- Partinen, M.; Gislason, T. Basic Nordic Sleep Questionnaire (BNSQ): A quantitated measure of subjective sleep complaints. J. Sleep Res. 1995, 4, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Vaara, J.; Fogelholm, M.; Vasankari, T.; Santtila, M.; Häkkinen, K.; Kyröläinen, H. Associations of maximal strength and muscular endurance with cardiovascular risk factors. Int. J. Sports Med. 2014, 35, 356–360. [Google Scholar] [CrossRef] [PubMed]
- Vaara, J.; Kyröläinen, H. Reserviläisten Toimintakyky Vuonna; Juvenes Print: Tampere, Finland, 2015. (In Finnish) [Google Scholar]
- Pihlainen, K. Effects of Combined Strength an Endurance Training on Body Composition and Physical Fitness in Soldiers During a 6-Month Crisis Management operation. Master’s Thesis, University of Jyväskylä, Jyväskylä, Finland, 2021. [Google Scholar]
- Pihlainen, K.; Santtila, M.; Ohrankämmen, O.; Ilomäki, I.; Rintakoski, M.; Tiainen, S. Fitness Test Manual of the Finnish Defence Forces, 2nd ed.; Edita Prima Oy: Verkkosaarenkatu, Finland, 2011. [Google Scholar]
- Cooper, K. A means of assessing maximal oxygen intake: Correlation between field and treadmill testing. JAMA J. Am. Med. Assoc. 1968, 203, 201–204. [Google Scholar] [CrossRef]
- Storer, T.; Davis, J.; Caiozzo, V. Accurate prediction of VO2max in cycle ergometry. Med. Sci. Sports Exerc. 1990, 22, 704–712. [Google Scholar] [CrossRef]
- Suni, J.; Oja, P.; Laukkanen, R.; Millunpalo, S.; Pasanen, M.; Vartiainen, T.-M.; Vuori, I. Validity of the UKK 2 km walking test: Relations to physical activity and health. Med. Sci. Sports Exerc. 1995, 27, 77. [Google Scholar] [CrossRef]
- Santtila, M.; Häkkinen, K.; Pihlainen, K.; Kyröläinen, H. Comparison between direct and predicted maximal oxygen uptake measurement during cycling. Mil. Med. 2012, 178, 234–238. [Google Scholar] [CrossRef] [Green Version]
- Ekblom-Bak, E.; Björkman, F.; Hellenius, M.; Ekblom, B. A new submaximal cycle ergometer test for prediction of VO2max: A new submaximal cycle ergometer test. Scand. J. Med. Sci. Sports 2014, 24, 319–326. [Google Scholar] [CrossRef] [Green Version]
- Pihlainen, K.; Santtila, M.; Häkkinen, K.; Kyröläinen, H. Associations of physical fitness and body composition characteristics with simulated military task performance. J. Strength Cond. Res. 2018, 32, 1089–1098. [Google Scholar] [CrossRef] [Green Version]
- Viljanen, T.; Viitasalo, J.; Kujala, U. Strength characteristics of a healthy urban adult population. Eur. J. Appl. Physiol. 1991, 63, 43–47. [Google Scholar] [CrossRef]
- Santtila, M.; Kyröläinen, H.; Vasankari, T.; Tianen, S.; Palvalin, K.; Häkkinen, A.; Häkkinen, K. Physical fitness profiles in young Finnish men during the years 1975–2004. Med. Sci. Sports Exerc. 2006, 38, 1990–1994. [Google Scholar] [CrossRef]
- Schmidt, G. Muscle endurance and flexibility components of Singapore national physical fitness award. Aust. J. Sci. Med. Sport 1995, 27, 88–94. [Google Scholar]
- Sillanpää, E.; Cheng, S.; Häkkinen, K.; Finni, T.; Walker, S.; Pesola, A.; Ahtiainen, J.; Stenroth, L.; Selänne, H.; Sipilä, S. Body composition in 18- to 88-year-old adults—Comparison of multifrequency bioimpedance and dual-energy X-ray absorptiometry. Obesity 2014, 22, 101–109. [Google Scholar] [CrossRef]
- American Diabetes Association. Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 1997, 20, 1183–1197. [Google Scholar] [CrossRef]
- Haffner, S.; Valdez, R.; Hazuda, H.; Mitchell, B.; Morales, P.; Stern, M. Prospective analysis of the insulin-resistance syndrome (Syndrome X). Diabetes 1992, 41, 715–722. [Google Scholar] [CrossRef]
- Borén, J.; Matikainen, N.; Adiels, M.; Taskinen, M.-R. Postprandial hypertriglyceridemia as a coronary risk factor. Clin. Chim. Acta 2014, 431, 131–142. [Google Scholar] [CrossRef]
- Ference, B.; Ginsberg, H.; Graham, I.; Ray, K.; Packard, C.; Bruckert, E.; Hegele, R.; Krauss, R.; Raal, F.; Schunkert, H.; et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel. Eur. Heart J. 2017, 38, 2459–2472. [Google Scholar] [CrossRef] [Green Version]
- Prospective Studies Collaboration. Blood cholesterol and vascular mortality by age, sex, and blood pressure: A meta-analysis of individual data from 61 prospective studies with 55,000 vascular deaths. Lancet 2007, 370, 1829–1839. [Google Scholar] [CrossRef]
- Winklhofer- Roob, B.; Faustmann, G.; Roob, J. Low-density lipoprotein oxidation biomarkers in human health and disease and effects of bioactive compounds. Free Radic. Biol. Med. 2017, 111, 38–86. [Google Scholar] [CrossRef]
- Kresanov, P.; Ahotupa, M.; Vasankari, T.; Kaikkonen, J.; Kähönen, M.; Lehtimäki, T.; Viikari, J.; Raitakari, O. The associations of oxidized high-density lipoprotein lipids with risk factors for atherosclerosis: The Cardiovascular Risk in Young Finns Study. Free Radic. Biol. Med. 2013, 65, 1284–1290. [Google Scholar] [CrossRef] [PubMed]
- Kotronen, A.; Yki-Järvinen, H.; Männistö, S.; Saarikoski, L.; Korpi-Hyövälti, E.; Oksa, H.; Saltevo, J.; Saaristo, T.; Sundvall, J.; Tuomilehto, J.; et al. Non-alcoholic and alcoholic fatty liver disease—Two diseases of affluence associated with the metabolic syndrome and type 2 diabetes: The FIN-D2D survey. BMC Public Health 2010, 10, 237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Helander, A.; Carlsson, A.; Borg, S. Longitudinal comparison of carbohydrate-deficient transferrin and gamma-glutamyl transferase: Complementary markers of excessive alcohol consumption. Alcohol 1996, 31, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Trull, A. Biomarkers of Disease an Evidence Based Approach; Cambridge University Press: Cambridge, UK, 2002. [Google Scholar]
- Vineetha, R.; Pai, K.; Vengal, M.; Gopalakrishna, K.; Narayanakurup, D. Usefulness of salivary alpha amylase as a biomarker of chronic stress and stress related oral mucosal changes—A pilot study. J. Clin. Exp. Dent. 2014, 6, 132. [Google Scholar] [CrossRef] [Green Version]
- The Defence Command’s Personnel Division. Statement of Human Resources 2018; Juvenes Print: Naulakatu, Finland, 2019. [Google Scholar]


{kind=link}
| Intervention Group | Control Group | |
|---|---|---|
| Baseline measurements before the intervention | ||
| Questionnaire | X | X |
| Body composition measurements | X | X |
| RM42-Accelerometer measurements | X | X |
| Fitness tests | X | X |
| Laboratory tests | X | X |
| Intervention lasting six months | ||
| Movesense accelerometer measurements and smartphone application feedback | X | |
| Telephone counselling | X | |
| Measurements after the intervention | ||
| Questionnaire | X | |
| Body composition measurements | X | |
| RM42 accelerometer measurements | X | X |
| Fitness tests | X | |
| Laboratory tests | X | |
| Measurements after six months from the end of the intervention | ||
| Questionnaire | X | X |
| Body composition measurements | X | X |
| RM42 accelerometer measurements | X | X |
| Fitness tests | X | X |
| Laboratory tests | X | X |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pietiläinen, E.; Kyröläinen, H.; Vasankari, T.; Santtila, M.; Luukkaala, T.; Parkkola, K. A Randomized Controlled Trial Protocol for Using an Accelerometer-Smartphone Application Intervention to Increase Physical Activity and Improve Health among Employees in a Military Workplace. Methods Protoc. 2022, 5, 1. https://0-doi-org.brum.beds.ac.uk/10.3390/mps5010001
Pietiläinen E, Kyröläinen H, Vasankari T, Santtila M, Luukkaala T, Parkkola K. A Randomized Controlled Trial Protocol for Using an Accelerometer-Smartphone Application Intervention to Increase Physical Activity and Improve Health among Employees in a Military Workplace. Methods and Protocols. 2022; 5(1):1. https://0-doi-org.brum.beds.ac.uk/10.3390/mps5010001
Chicago/Turabian StylePietiläinen, Emilia, Heikki Kyröläinen, Tommi Vasankari, Matti Santtila, Tiina Luukkaala, and Kai Parkkola. 2022. "A Randomized Controlled Trial Protocol for Using an Accelerometer-Smartphone Application Intervention to Increase Physical Activity and Improve Health among Employees in a Military Workplace" Methods and Protocols 5, no. 1: 1. https://0-doi-org.brum.beds.ac.uk/10.3390/mps5010001