
Measurement of Physical Fitness and 24/7 Physical Activity, Standing, Sedentary Behavior, and Time in Bed in Working-Age Finns: Study Protocol for FINFIT 2021

 ,
,  , , , , , and
, , , , , and
Abstract
:1. Introduction
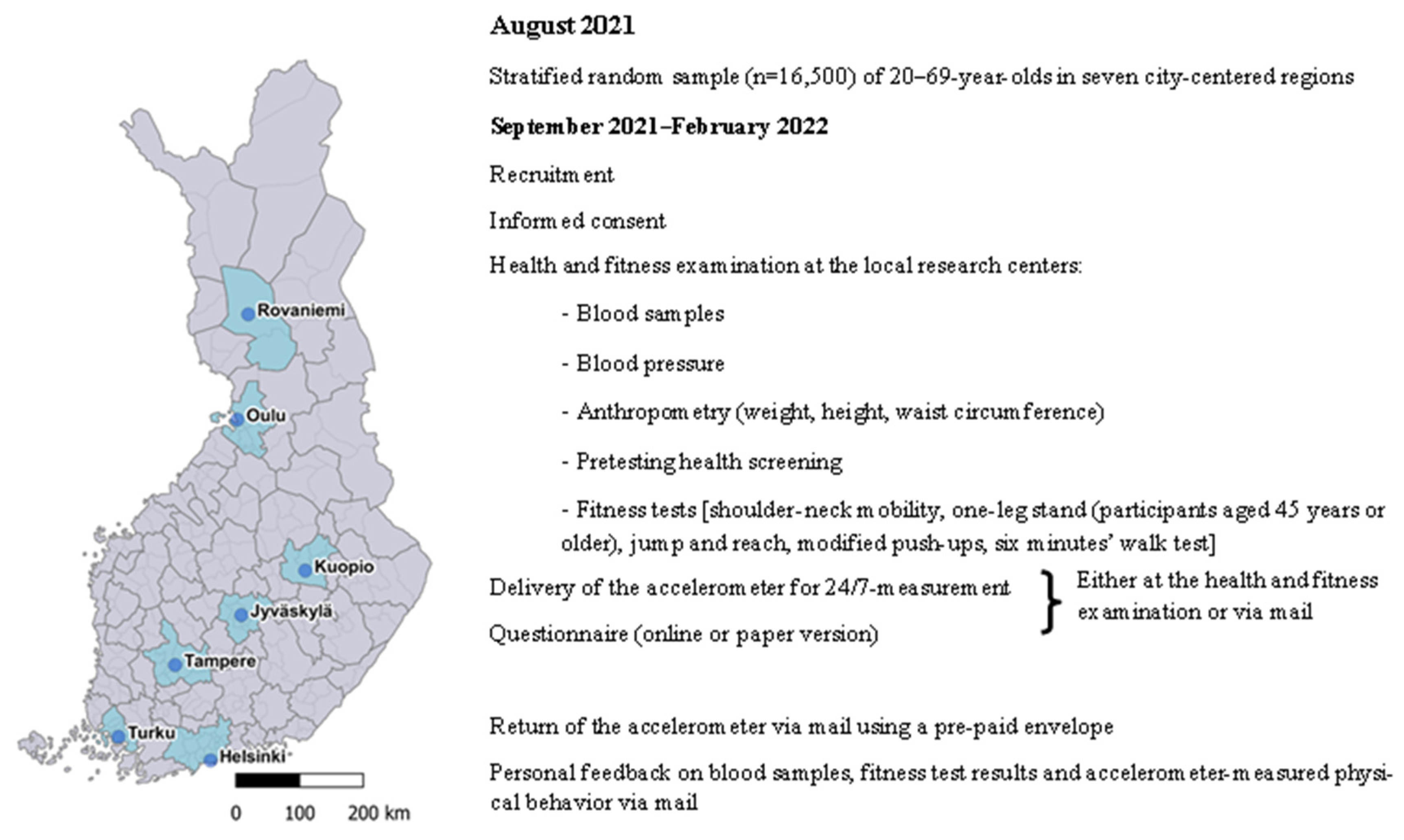
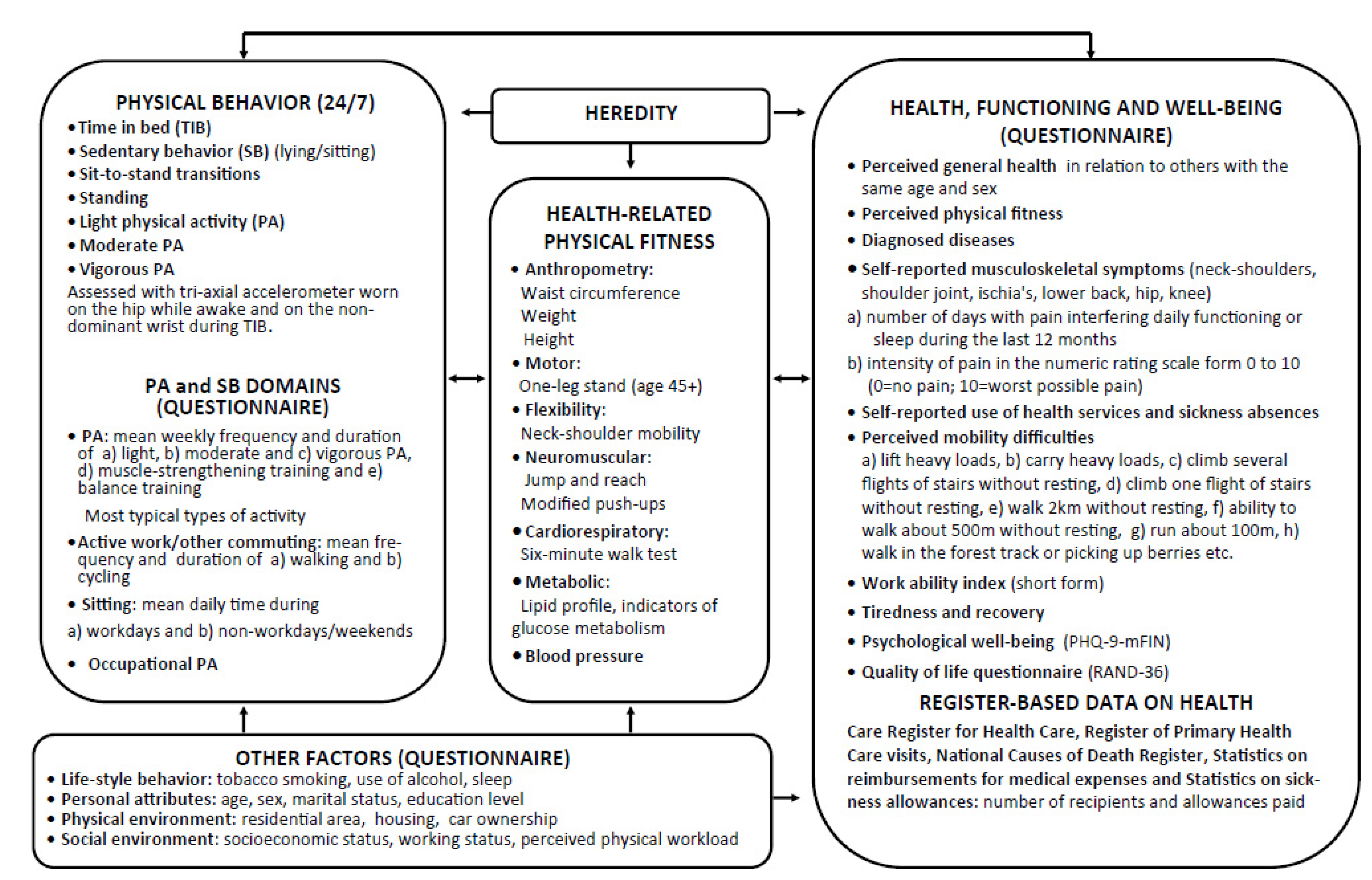
2. Materials and Methods
3. Procedures
3.1. Assessment of 24 h Physical Behavior (PA, Standing, SB, TIB)
3.2. Self-Reported Sleep
3.3. Self-Reported Physical Activity and Sedentary Behavior
3.4. Assessment of Health-Related Physical Fitness
3.5. Assessment of Health
3.6. Statistical Analysis
4. Expected Results
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- GBD. Five insights from the Global Burden of Disease Study 2019. Lancet 2020, 396, 1135–1159. [Google Scholar] [CrossRef]
- US Department of Health and Human Services. Physical activity guidelines for Americans. Available online: https://health.gov/sites/default/files/2019-09/Physical_Activity_Guidelines_2nd_edition.pdf (accessed on 18 October 2021).
- Piercy, K.L.; Troiano, R.P.; Ballard, R.M.; Carlson, S.A.; Fulton, J.E.; Galuska, D.A.; George, S.M.; Olson, R.D. The Physical Activity Guidelines for Americans. JAMA 2018, 320, 2020–2028. [Google Scholar] [CrossRef]
- Chastin, S.; McGregor, D.; Palarea-Albaladejo, J.; Diaz, K.M.; Hagströmer, M.; Hallal, P.C.; van Hees, V.T.; Hooker, S.; Howard, V.J.; Lee, I.-M.; et al. Joint association between accelerometry-measured daily combination of time spent in physical activity, sedentary behaviour and sleep and all-cause mortality: A pooled analysis of six prospective cohorts using compositional analysis. Br. J. Sports Med. 2021, 55, 1277–1285. [Google Scholar] [CrossRef] [PubMed]
- Husu, P.; Suni, J.; Vähä-Ypyä, H.; Sievänen, H.; Tokola, K.; Valkeinen, H.; Mäki-Opas, T.; Vasankari, T. Objectively measured sedentary behavior and physical activity in a sample of Finnish adults: A cross-sectional study. BMC Public Health 2016, 16, 920. [Google Scholar] [CrossRef] [Green Version]
- Hukkanen, H.; Husu, P.; Sievänen, H.; Tokola, K.; Vähä-Ypyä, H.; Valkeinen, H.; Mäki-Opas, T.; Suni, J.H.; Vasankari, T. Aerobic physical activity assessed with accelerometer, diary, questionnaire and interview in a Finnish population sample. Scand. J. Med. Sci. Sports 2018, 2810, 2196–2206. [Google Scholar] [CrossRef] [PubMed]
- Du, Y.; Liu, B.; Sun, Y.; Snetselaar, L.G.; Wallace, R.B.; Bao, W. Trends in adherence to the physical activity guidelines for Americans for aerobic activity and time spent on sedentary behavior among US adults, 2007 to 2016. JAMA Netw. Open 2019, 2, e197597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ding, D.; Lawson, K.D.; Kolbe-Alexander, T.L.; Finkelstein, E.A.; Katzmarzyk, P.T.; van Mechelen, W.; Pratt, M. Lancet Physical Activity Series 2 Executive Committee. The economic burden of physical inactivity: A global analysis of major non-communicable diseases. Lancet 2016, 388, 1311–1324. [Google Scholar] [CrossRef]
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.M.; Altenburg, T.M.; Chinapaw, M.J.M. SBRN Terminology Consensus Project Participants. Sedentary Behavior Research Network (SBRN)—Terminology Consensus Project process and outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 141, 75. [Google Scholar] [CrossRef] [Green Version]
- Owen, N.; Healy, G.N.; Dempsey, P.C.; Salmon, J.; Timperio, A.; Clark, B.K.; Goode, A.D.; Koorts, H.; Ridgers, N.D.; Hadgraft, N.T.; et al. Sedentary Behavior and Public Health: Integrating the Evidence and Identifying Potential Solutions. Annu. Rev. Public Health 2020, 41, 265–287. [Google Scholar] [CrossRef] [Green Version]
- Katzmarzyk, P.T.; Ross, R.; Blair, S.N.; Després, J.P. Should we target increased physical activity or less sedentary behavior in the battle against cardiovascular disease risk development? Atherosclerosis 2020, 311, 107–115. [Google Scholar] [CrossRef]
- Husu, P.; Tokola, K.; Vähä-Ypyä, H.; Sievänen, H.; Suni, J.; Heinonen, O.J.; Heiskanen, J.; Kaikkonen, K.M.; Savonen, K.; Kokko, S.; et al. Physical activity, sedentary behavior and time in bed among Finnish adults measured 24/7 by triaxial accelerometry. J. Meas. Phys. Behav. 2021, 42, 163–173. [Google Scholar] [CrossRef]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R., Jr.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. 2011 Compendium of Physical Activities: A second update of codes and MET values. Med. Sci. Sports Exerc. 2011, 438, 1575–1581. [Google Scholar] [CrossRef] [Green Version]
- Füzéki, E.; Engeroff, T.; Banzer, W. Health Benefits of Light-Intensity Physical Activity: A Systematic Review of Accelerometer Data of the National Health and Nutrition Examination Survey (NHANES). Sports Med. 2017, 479, 1769–1793. [Google Scholar] [CrossRef]
- Loprinzi, P.D. Light-Intensity Physical Activity and All-Cause Mortality. Am. J. Health Promot. 2017, 314, 340–342. [Google Scholar] [CrossRef] [PubMed]
- Dohrn, I.M.; Sjöström, M.; Kwak, L.; Oja, P.; Hagströmer, M. Accelerometer-measured sedentary time and physical activity-A 15 year follow-up of mortality in a Swedish population-based cohort. J. Sci. Med. Sport 2018, 217, 702–707. [Google Scholar] [CrossRef]
- Chastin, S.F.M.; De Craemer, M.; De Cocker, K.; Powell, L.; van Cauwenberg, J.; Dall, P.; Hamer, M.; Stamatakis, E. How does light-intensity physical activity associate with adult cardiometabolic health and mortality? Systematic review with meta-analysis of experimental and observational studies. Br. J. Sports Med. 2019, 53, 370–376. [Google Scholar] [CrossRef] [Green Version]
- Ekelund, U.; Dalene, K.E.; Tarp, J.; Lee, I.M. Physical activity and mortality: What is the dose response and how big is the effect? Br. J. Sports Med. 2020, 54, 1125–1135. [Google Scholar] [CrossRef] [PubMed]
- Kodama, S.; Saito, K.; Tanaka, S.; Maki, M.; Yachi, Y.; Asumi, M.; Sugawara, A.; Totsuka, K.; Shimano, H.; Ohashi, Y.; et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: A meta-analysis. JAMA 2009, 301, 2024–2035. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Li, F.; Cheng, Y. Cardiorespiratory fitness as a quantitative predictor of the risk of stroke: A dose–response meta-analysis. J. Neurol. 2020, 267, 491–501. [Google Scholar] [CrossRef] [PubMed]
- Tarp, J.; Støle, A.P.; Blond, K.; Grontved, A. Cardiorespiratory fitness, muscular strength and risk of type 2 diabetes: A systematic review and meta-analysis. Diabetologia 2019, 62, 1129–1142. [Google Scholar] [CrossRef] [Green Version]
- Lakoski, S.G.; Willis, B.L.; Barlow, C.E.; Leonard, D.; Gao, A.; Radford, N.B.; Farrell, S.W.; Douglas, P.S.; Berry, J.D.; Defina, L.F.; et al. Midlife Cardiorespiratory Fitness, Incident Cancer, and Survival After Cancer in Men: The Cooper Center Longitudinal Study. JAMA Oncol. 2015, 12, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Pozuelo-Carrascosa, D.P.; Alvarez-Bueno, C.; Cavero-Redondo, I.; Morais, S.; Lee, I.-M.; Martinez-Vizcaino, V. Cardiorespiratory fitness and site-specific risk of cancer in men: A systematic review and meta-analysis. Eur. J. Cancer 2019, 113, 58–68. [Google Scholar] [CrossRef] [PubMed]
- Imboden, M.T.; Harber, M.P.; Whaley, M.H.; Finch, W.H.; Bishop, D.L.; Kaminsky, L.A. Cardiorespiratory fitness and mortality in healthy men and women. J. Am. Coll. Cardiol. 2018, 72, 2283–2292. [Google Scholar] [CrossRef] [PubMed]
- van der Velde, J.H.; Koster, A.; van der Berg, J.D.; Sep, S.J.S.; van der Kallen, C.J.H.; Dagnelie, P.C.; Schram, M.T.; Henry, R.M.A.; Eussen, S.J.P.M.; Van Dongen, M.C.J.M.; et al. Sedentary Behavior, Physical Activity, and Fitness-The Maastricht Study. Med. Sci. Sports Exerc. 2017, 49, 1583–1591. [Google Scholar] [CrossRef] [PubMed]
- Knaeps, S.; Bourgois, J.G.; Charlier, R.; Mertens, E.; Lefevre, J.; Wijndaele, K. Ten-year change in sedentary behaviour, moderate-to-vigorous physical activity, cardiorespiratory fitness and cardiometabolic risk: Independent associations and mediation analysis. Br. J. Sports Med. 2018, 52, 1063–1068. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schram, M.T.; Sep, S.J.; van der Kallen, C.J.; Dagnelie, P.C.; Koster, A.; Schaper, N.; Henry, R.M.A.; Stehouwer, C.D.A. The Maastricht Study: An extensive phenotyping study on determinants of type 2 diabetes, its complications and its comorbidities. Eur. J. Epidemiol. 2014, 29, 439–451. [Google Scholar] [CrossRef]
- Zou, D.; Wennman, H.; Ekblom, Ö.; Grote, L.; Arvidsson, D.; Blomberg, A.; Torén, K.; Bergström, G.; Börjesson, M.; Hedner, J. Insomnia and cardiorespiratory fitness in a middle-aged population: The SCAPIS pilot study. Sleep Breath. 2019, 231, 319–326. [Google Scholar] [CrossRef] [Green Version]
- Vincent, G.E.; Jay, S.M.; Sargent, C.; Vandelanotte, C.; Ridgers, N.D.; Ferguson, S.A. Improving Cardiometabolic Health with Diet, Physical Activity, and Breaking Up Sitting: What about Sleep? Front. Physiol. 2017, 8, 865. [Google Scholar] [CrossRef] [Green Version]
- Smiley, A.; King, D.; Bidulescu, A. The association between sleep duration and metabolic syndrome: The NHANES 2013/2014. Nutrients 2019, 11, 2582. [Google Scholar] [CrossRef] [Green Version]
- Gardner, M. Sleep, health and society. Sleep Med. Clin. 2017, 121, 1–22. [Google Scholar] [CrossRef]
- Kredlow, M.A.; Capozzoli, M.C.; Hearon, B.A.; Calkins, A.W.; Otto, M.W. The effects of physical activity on sleep: A meta-analytic review. J. Behav. Med. 2015, 383, 427–449. [Google Scholar] [CrossRef]
- Wang, F.; Boros, S. The effect of physical activity on sleep quality: A systematic review. Eur. J. Physiother. 2021, 23, 11–18. [Google Scholar] [CrossRef]
- Kanagasabai, T.; Riddell, M.C.; Ardern, C.I. Physical Activity Contributes to Several Sleep-Cardiometabolic Health Relationships. Metab. Syndr. Relat. Disord. 2017, 151, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Chaput, J.P.; Carson, V.; Gray, C.E.; Tremblay, M.S. Importance of all movement behaviors in a 24 hour period for overall health. Int. J. Environ. Res. Public Health 2014, 1112, 12575–12581. [Google Scholar] [CrossRef] [PubMed]
- Pedisic, Z.; Dumuid, D.; Olds, T.S. Integrating sleep, sedentarybehavior, and physical activity research in the emerging field of timeuse epidemiology: Definitions, concepts, statistical methods, theoreticalframework and future directions. Kinesiology 2017, 49, 252–269. [Google Scholar]
- Rosenberge, M.E.; Fulton, J.E.; Buman, M.P.; Troiano, R.P.; Grandner, M.A.; Buchner, D.M.; Haskell, W.L. The 24-hour activity cycle: A new paradigm for physical activity. Med. Sci. Sports Exerc. 2019, 51, 454–464. [Google Scholar] [CrossRef] [PubMed]
- Sievänen, H.; Kujala, U.M. Accelerometry-Simple, but challenging. Scand. J. Med. Sci. Sports 2017, 276, 574–578. [Google Scholar] [CrossRef]
- Bouchard, C.; Shephard, R.J. Physical activity, fitness and health: The model and key consepts. In Exercise, Fitness, and Health; Bouchard, C., Shephard, R.J., Stephens, T., Eds.; Human Kinetics Books: Champaign, IL, USA, 1994; pp. 106–118. [Google Scholar]
- Smith, A.M.A.; Shelley, J.M.; Dennerstein, L. Self-rated health: Biological continuum or social discontinuity? Soc. Sci. Med. 1994, 39, 77–83. [Google Scholar] [CrossRef]
- Mänty, M.; Heinonen, A.; Leinonen, R.; Törmäkangas, T.; Sakari-Rantala, R.; Hirvensalo, M.; von Bonsdorff, M.; Rantanen, T. Construct and predictive validity of a self-reported measure of preclinical mobility limitation. Arch. Phys. Med. Rehabil. 2008, 889, 1108–1113. [Google Scholar] [CrossRef]
- Hämäläinen, H.P.; Suni, J.H.; Pasanen, M.E.; Malmberg, J.J.; Miilunpalo, S.I. Predictive value of health-related fitness tests for self-reported mobility difficulties among high-functioning elderly men and women. Aging Clin. Exp. Res. 2006, 183, 218–226. [Google Scholar] [CrossRef]
- Ilmarinen, J. Work ability—A comprehensive concept for occupational health research and prevention. Scand. J. Work Environ. Health 2009, 35, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Smolander, J.; Blair, S.N.; Kohl, H.W., 3rd. Work ability, physical activity, and cardiorespiratory fitness: 2 year results from Project Active. J. Occup. Environ. Med. 2000, 42, 906–910. [Google Scholar] [CrossRef] [PubMed]
- Suni, J.; Virkkunen, T.; Husu, P.; Tokola, K.; Parkkari, J.; Kankaanpää, M. Reliability and construct validity of the modified Finnish version of the 9-item Patient Health Questionnaire and its associations within the biopsychosocial framework among female health-care workers with sub-acute or recurrent low back pain. BMC Musculoskelet. Disord. 2021, 22, 37. [Google Scholar] [CrossRef]
- Aalto, A.-M.; Aro, A.R.; Teperi, J. RAND–36 as a measure of Health-Related Quality of Life. Reliability, construct validity and reference values in the Finnish general population. Helsinki. Stakes Res. Rep. 1999, 101, 49–51, (In Finnish with a short summary in English). [Google Scholar]
- Caramaliu, R.V.; Vasile, A.; Bacis, I. Wearable vital parameters monitoring system. In Proceedings of the Advanced Topics in Optoelectronics, Microelectronics, and Nanotechnologies VII, Bucharest, Romania, 21–23 November 2002; Volume 9258, p. 92580R. [Google Scholar] [CrossRef]
- Jaeschke, L.; Luzak, A.; Steinbrecher, A.; Jeran, S.; Ferland, M.; Linkohr, B. Schulz, H.; Pischon, T. 24 h-accelerometry in epidemiological studies: Automated detection of non-wear time in comparison to diary information. Sci. Rep. 2017, 7, 2227. [Google Scholar] [CrossRef] [Green Version]
- Vähä-Ypyä, H.; Vasankari, T.; Husu, P.; Suni, J.; Sievänen, H. A universal, accurate intensity-based classification of different physical activities using raw data of accelerometer. Clin. Physiol. Funct. Imaging 2015, 351, 64–70. [Google Scholar] [CrossRef] [PubMed]
- Vähä-Ypyä, H.; Vasankari, T.; Husu, P.; Mänttäri, A.; Vuorimaa, T.; Suni, J.; Sievänen, H. Validation of Cut-Points for Evaluating the Intensity of Physical Activity with Accelerometry-Based Mean Amplitude Deviation (MAD). PLoS ONE 2015, 108, e0134813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vähä-Ypyä, H.; Sievänen, H.; Husu, P.; Tokola, K.; Vasankari, T. Intensity paradox—Low-fit people are physically most active in terms of their fitness. Sensors 2021, 21, 2063. [Google Scholar] [CrossRef]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, P.A.; Lamonte, M.J.; Lee, I.M.; Nieman, D.C.; Swain, D.P. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 437, 1334–1359. [Google Scholar] [CrossRef] [PubMed]
- Vähä-Ypyä, H.; Husu, P.; Suni, J.; Vasankari, T.; Sievänen, H. Reliable recognition of lying, sitting, and standing with a hip-worn accelerometer. Scand. J. Med. Sci. Sports 2018, 28, 1092–1102. [Google Scholar] [CrossRef] [Green Version]
- Husu, P.; Suni, J.; Tokola, K.; Vähä-Ypyä, H.; Valkeinen, H.; Mäki-Opas, T.; Sievänen, H.; Vasankari, T. Frequent sit-to-stand transitions and several short standing periods measured by hip-worn accelerometer are associated with smaller waist circumference among adults. J. Sport Sci. 2019, 2, 1–9. [Google Scholar] [CrossRef] [PubMed]
- van Hees, V.T.; Sabia, S.; Anderson, K.N.; Denton, S.J.; Oliver, J.; Catt, M.; Abell, J.G.; Kivimaki, M.; Trenell, M.I.; Singh-Manoux, A. A Novel, open access method to assess sleep duration using a wrist-worn accelerometer. PLoS ONE 2015, 1011, e0142533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Åkerstedt, T.; Gillberg, M. Subjective and objective sleepiness in the active individual. Int. J. Neurosci. 1990, 52, 29–32. [Google Scholar] [CrossRef]
- Kaida, K.; Takahashi, M.; Akerstedt, T.; Nakata, A.; Otsuka, Y.; Haratani, T.; Fukasawa, K. Validation of the Karolinska sleepiness scale against performance and EEG variables. Clin. Neurophysiol. 2006, 1177, 1574–1581. [Google Scholar] [CrossRef]
- Suni, J.H.; Oja, P.; Laukkanen, R.T.; Miilunpalo, S.I.; Pasanen, M.E.; Vuori, I.M.; Vartiainen, T.M.; Bös, K. Health-related fitness test battery for adults: Aspects of reliability. Arch Phys Med. Rehabil. 1996, 774, 399–405. [Google Scholar] [CrossRef]
- Suni, J.H.; Miilunpalo, S.I.; Asikainen, T.M.; Laukkanen, R.T.; Oja, P.; Pasanen, M.E.; Bös, K.; Vuori, I.M. Safety and feasibility of a health-related fitness test battery for adults. Phys. Ther. 1998, 782, 134–148. [Google Scholar] [CrossRef]
- Suni, J.H.; Oja, P.; Miilunpalo, S.I.; Pasanen, M.E.; Vuori, I.M.; Bös, K. Health-related fitness test battery for adults: Associations with perceived health, mobility, and back function and symptoms. Arch. Phys. Med. Rehabil. 1998, 795, 559–569. [Google Scholar] [CrossRef]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 11, 111–117. [Google Scholar]
- Mänttäri, A.; Suni, J.; Sievänen, H.; Husu, P.; Vähä-Ypyä, H.; Valkeinen, H.; Tokola, K.; Vasankari, T. Six-minute walk test: A tool for predicting maximal aerobic power (VO2max) in healthy adults. Clin. Physiol. Funct. Imaging 2018, 38, 1038–1045. [Google Scholar] [CrossRef] [PubMed]
- van der Velde, J.H.P.M.; Schaper, N.C.; Stehouwer, C.D.A.; van der Kallen, C.J.H.; Sep, S.J.S.; Schram, M.T.; Henry, R.M.A.; Dagnelie, P.C.; Eussen, S.J.P.M.; Van Dongen, M.C.J.M.; et al. Which is more important for cardiometabolic health: Sedentary time, higher intensity physical activity or cardiorespiratory fitness? The Maastricht Study. Diabetologia 2018, 6112, 2561–2569. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Time in Bed = Wrist-Worn Time | Hip-Worn Time | ||||
|---|---|---|---|---|---|
| Number (N) of over 5° Changes in the Wrist Angle during 20 min Window | Physical Behavior | Absolute Threshold | Relative Threshold | APE (°) | |
| High movement | N ≥ 14 | Lying | MET ≤ 1.5 | MET ≤ 1.5 | 73≥ |
| Medium movement | 2 ≤ N ≤ 13 | Reclining | MET ≤ 1.5 | MET ≤ 1.5 | 30–73 |
| Low movement | N ≤ 1 | Sitting | MET ≤ 1.5 | MET ≤ 1.5 | 11.6–30 |
| Standing | MET ≤ 1.5 | MET ≤ 1.5 | 0–11.6 | ||
| Light PA | 1.5 < MET ≤ 3 | 1.5 < MET & VO2R ≤ 40% | |||
| Moderate PA | 3 < MET ≤ 6 | 40% < VO2R ≤ 60% | |||
| Vigorous PA | MET > 6 | VO2R > 60% | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Husu, P.; Vähä-Ypyä, H.; Tokola, K.; Sievänen, H.; Mänttäri, A.; Kokko, S.; Kaikkonen, K.M.; Savonen, K.; Vasankari, T. Measurement of Physical Fitness and 24/7 Physical Activity, Standing, Sedentary Behavior, and Time in Bed in Working-Age Finns: Study Protocol for FINFIT 2021. Methods Protoc. 2022, 5, 7. https://0-doi-org.brum.beds.ac.uk/10.3390/mps5010007
Husu P, Vähä-Ypyä H, Tokola K, Sievänen H, Mänttäri A, Kokko S, Kaikkonen KM, Savonen K, Vasankari T. Measurement of Physical Fitness and 24/7 Physical Activity, Standing, Sedentary Behavior, and Time in Bed in Working-Age Finns: Study Protocol for FINFIT 2021. Methods and Protocols. 2022; 5(1):7. https://0-doi-org.brum.beds.ac.uk/10.3390/mps5010007
Chicago/Turabian StyleHusu, Pauliina, Henri Vähä-Ypyä, Kari Tokola, Harri Sievänen, Ari Mänttäri, Sami Kokko, Kaisu M. Kaikkonen, Kai Savonen, and Tommi Vasankari. 2022. "Measurement of Physical Fitness and 24/7 Physical Activity, Standing, Sedentary Behavior, and Time in Bed in Working-Age Finns: Study Protocol for FINFIT 2021" Methods and Protocols 5, no. 1: 7. https://0-doi-org.brum.beds.ac.uk/10.3390/mps5010007