Virtual Reality Visual Training in an Adult Patient with Anisometropic Amblyopia: Visual and Functional Magnetic Resonance Outcomes


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Report
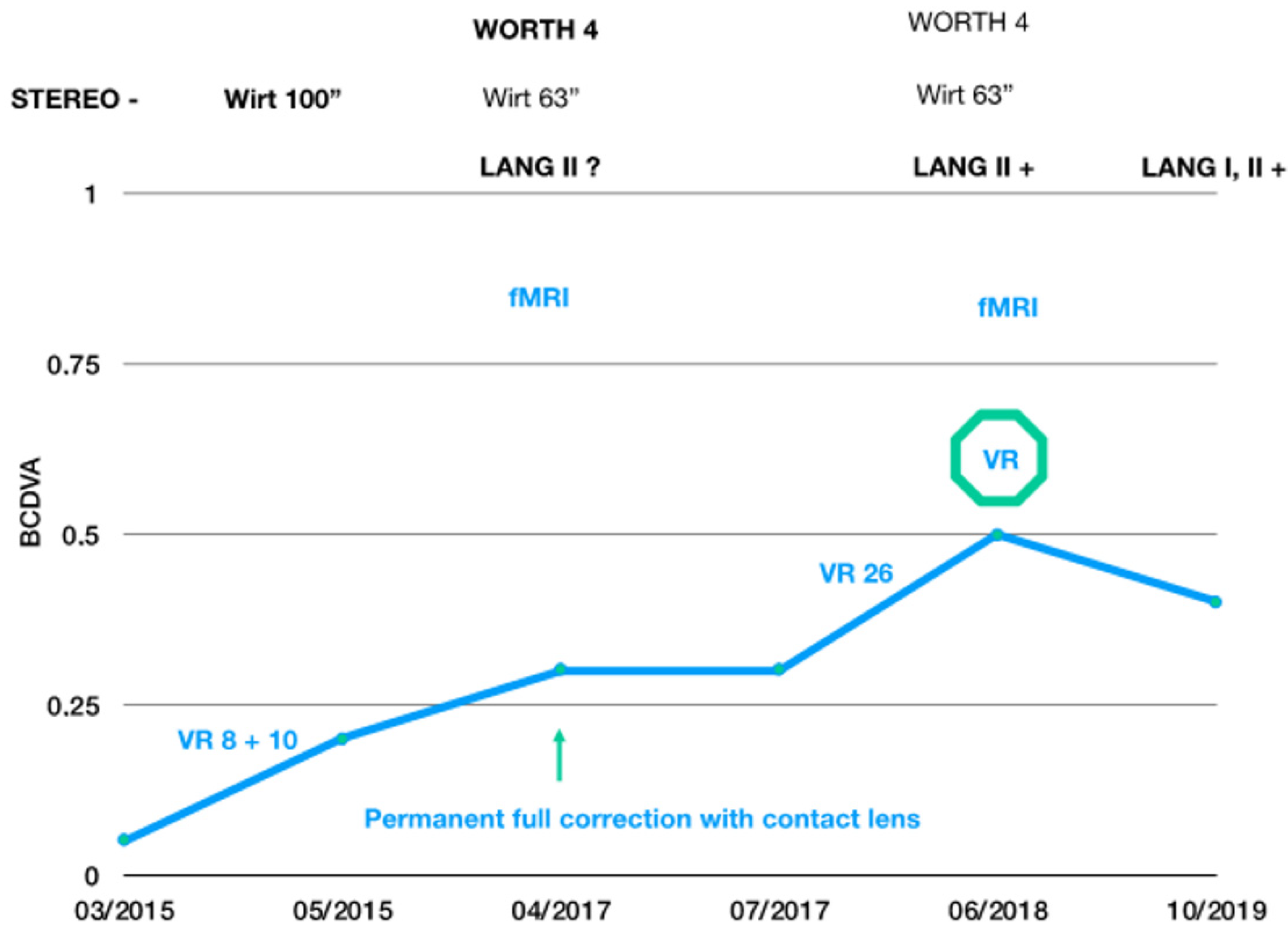
2.1. Description of the Case
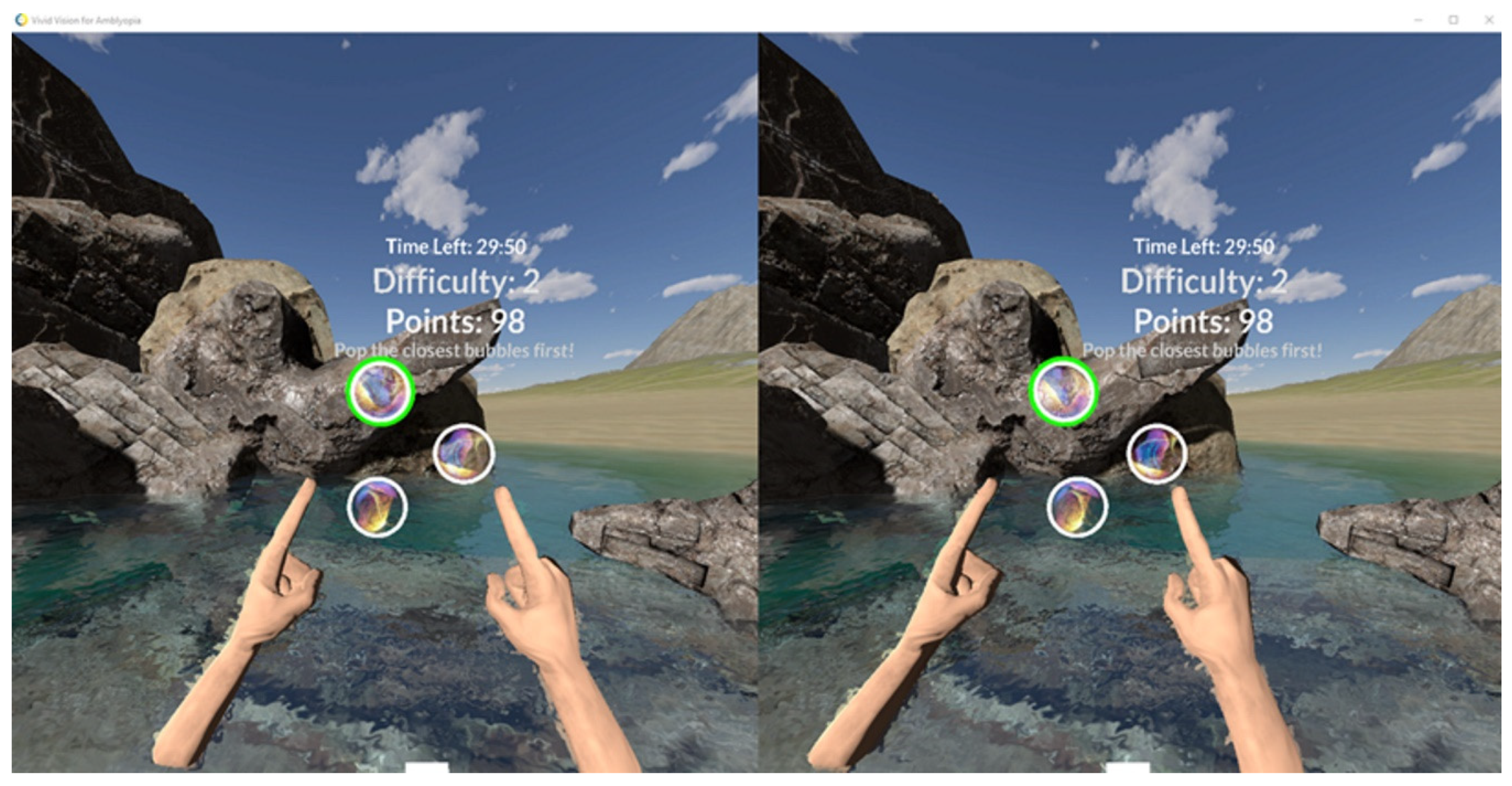
2.2. Vision Therapy
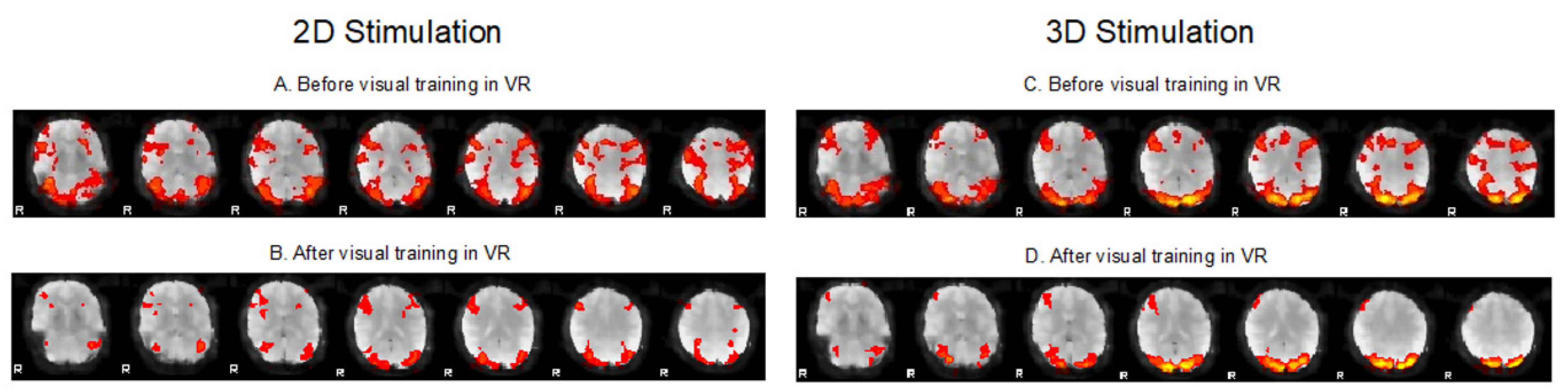
2.3. fMRI Testing
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Tommila, V.; Tarkkanen, A. Incidence of loss of vision in the healthy eye in amblyopia. Br. J. Ophthalmol. 1981, 65, 575–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coco-Martin, M.B.; Piñero, D.P.; Leal-Vega, L.; Hernández-Rodríguez, C.J.; Adiego, J.; Molina-Martín, A.; de Fez, D.; Arenillas, J.F. The potential of virtual reality for inducing neuroplasticity in children with amblyopia. J. Ophthalmol. 2020, 2020, 7067846. [Google Scholar] [CrossRef] [PubMed]
- Li, S.L.; Reynaud, A.; Hess, R.F.; Wang, Y.Z.; Jost, R.M.; Morale, S.E.; De la Cruz, A.; Dao, L.; Stager, D., Jr.; Birch, E.E. Dichoptic movie viewing treats childhood amblyopia. J. AAPOS 2015, 19, 401–405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, D.T.; Fong, A. Efficacy of neural vision therapy to enhance contrast sensitivity function and visual acuity in low myopia. J. Cataract. Refract. Surg. 2008, 34, 570–577. [Google Scholar] [CrossRef] [PubMed]
- El Mallah, M.K.; Chakravarthy, U.; Hart, P.M. Amblyopia: Is visual loss permanent? Br. J. Ophthalmol. 2000, 84, 952–956. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, M.; Xiao, H.; Xie, B.; Yin, X.; Wang, J.; Yang, H. Morphologic changes in the visual cortex of patients with anisometropic amblyopia: A surface-based morphometry study. BMC Neurosci. 2019, 20, 39. [Google Scholar]
- Lu, Z.; Huang, Y.; Lu, Q.; Feng, L.; Nguchu, B.A.; Wang, Y.; Wang, H.; Li, G.; Zhou, Y.; Qiu, B.; et al. Abnormal intra-network architecture in extra-striate cortices in amblyopia: A resting state fMRI study. Eye Vis. 2019, 6, 20. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Coyle, D.; Maguire, L.; McGinnity, T.M.; Hess, R.F. Long timescale fMRI neuronal adaptation effects in human amblyopic cortex. PLoS ONE 2011, 6, e26562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, B.; Maehara, G.; Goddard, E.; Farivar, R.; Mansouri, B.; Hess, R.F. Long-Range Interocular Suppression in Adults with Strabismic Amblyopia: A Pilot fMRI Study. Vision 2019, 3, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hess, R.F.; Mansouri, B.; Thompson, B. A new binocular approach to the treatment of amblyopia in adults well beyond the critical period of visual development. Restor. Neurol. Neurosci. 2010, 28, 793–802. [Google Scholar] [CrossRef]
- Žiak, P.; Holm, A.; Halička, J.; Mojžiš, P.; Piñero, D.P. Amblyopia treatment of adults with dichoptic training using the virtual reality oculus rift head mounted display: Preliminary results. BMC Ophthalmol. 2017, 17, 105. [Google Scholar] [CrossRef] [Green Version]
- Yalcin, E.; Balci, O. Efficacy of perceptual vision therapy in enhancing visual acuity and contrast sensitivity function in adult hypermetropic anisometropic amblyopia. Clin. Ophthalmol. 2014, 8, 49–53. [Google Scholar]
- Verma, A.; Singh, D. Active vision therapy for pseudophakic amblyopia. J. Cataract. Refract. Surg. 1997, 23, 1089–1094. [Google Scholar] [CrossRef]
- Singh, B.; Sharma, S.; Bharti, N.; Singh, A.; Dadia, S.; Bharti, S. Visual outcomes after refractive laser corneal surgery and phakic IOL in amblyopic eyes. Int. Ophthalmol. 2020, 40, 2827–2834. [Google Scholar] [CrossRef]
- Oruçoğlu-Orucov, F.; Frucht-Pery, J.; Landau, D.; Strasman, E.; Solomon, A. LASIK correction of vision in adults with unilateral amblyopia. J. Refract. Surg. 2011, 27, 18–22. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Halicka, J.; Bittsansky, M.; Sivak, S.; Piñero, D.P.; Ziak, P. Virtual Reality Visual Training in an Adult Patient with Anisometropic Amblyopia: Visual and Functional Magnetic Resonance Outcomes. Vision 2021, 5, 22. https://0-doi-org.brum.beds.ac.uk/10.3390/vision5020022
Halicka J, Bittsansky M, Sivak S, Piñero DP, Ziak P. Virtual Reality Visual Training in an Adult Patient with Anisometropic Amblyopia: Visual and Functional Magnetic Resonance Outcomes. Vision. 2021; 5(2):22. https://0-doi-org.brum.beds.ac.uk/10.3390/vision5020022
Chicago/Turabian StyleHalicka, Juraj, Michal Bittsansky, Stefan Sivak, David P. Piñero, and Peter Ziak. 2021. "Virtual Reality Visual Training in an Adult Patient with Anisometropic Amblyopia: Visual and Functional Magnetic Resonance Outcomes" Vision 5, no. 2: 22. https://0-doi-org.brum.beds.ac.uk/10.3390/vision5020022