PreserFlo® MicroShunt: An Overview of This Minimally Invasive Device for Open-Angle Glaucoma

 , , ,
, , ,
Abstract
:1. Introduction
2. History of PreserFlo MicroShunt
3. Surgical Technique
4. PreserFlo MicroShunt Results
PreserFlo MicroShunt in Pseudoexfoliative Glaucoma
5. PreserFlo MicroShunt vs. Trabeculectomy
6. PreserFlo MicroShunt vs. Other MIGS
7. Adverse Effects of PreserFlo MicroShunt
8. Novel Approaches
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Weinreb, R.N.; Aung, T.; Medeiros, F.A. The pathophysiology and treatment of glaucoma: A review. JAMA 2014, 311, 1901–1911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jonas, J.; Aung, T.; Bourne, R.; Bron, A.; Ritch, R.; Panda-Jonas, S. Glaucoma. Lancet 2017, 390, 31461–31469. [Google Scholar] [CrossRef]
- Gedde, S.J.; Feuer, W.J.; Shi, W.; Lim, K.S.; Barton, K.; Goyal, S.; Ahmed, I.I.K.; Brandt, J.; Primary Tube Versus Trabeculectomy Study, G. Treatment Outcomes in the Primary Tube Versus Trabeculectomy Study after 1 Year of Follow-up. Ophthalmology 2018, 125, 650–663. [Google Scholar] [CrossRef] [PubMed]
- Gedde, S.J.; Schiffman, J.C.; Feuer, W.J.; Herndon, L.W.; Brandt, J.D.; Budenz, D.L.; Tube versus Trabeculectomy Study, G. Treatment outcomes in the Tube Versus Trabeculectomy (TVT) study after five years of follow-up. Am. J. Ophthalmol. 2012, 153, 789–803.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gedde, S.J.; Herndon, L.W.; Brandt, J.D.; Budenz, D.L.; Feuer, W.J.; Schiffman, J.C.; Tube Versus Trabeculectomy Study, G. Postoperative complications in the Tube Versus Trabeculectomy (TVT) study during five years of follow-up. Am. J. Ophthalmol. 2012, 153, 804–814.e1. [Google Scholar] [CrossRef] [Green Version]
- Gazzard, G.; Konstantakopoulou, E.; Garway-Heath, D.; Garg, A.; Vickerstaff, V.; Hunter, R.; Ambler, G.; Bunce, C.; Wormald, R.; Nathwani, N.; et al. Selective laser trabeculoplasty versus eye drops for first-line treatment of ocular hypertension and glaucoma (LiGHT): A multicentre randomised controlled trial. Lancet 2019, 393, 1505–1516. [Google Scholar] [CrossRef] [Green Version]
- Saheb, H.; Ahmed, I.I.K. Micro-invasive glaucoma surgery: Current perspectives and future directions. Curr. Opin. Ophthalmol. 2012, 23, 96–104. [Google Scholar] [CrossRef]
- Richter, G.M.; Coleman, A.L. Minimally invasive glaucoma surgery: Current status and future prospects. Clin. Ophthalmol. 2016, 10, 189–206. [Google Scholar]
- Kerr, N.M.; Wang, J.; Barton, K. Minimally invasive glaucoma surgery as primary stand-alone surgery for glaucoma. Clin. Exp. Ophthalmol. 2017, 45, 393–400. [Google Scholar] [CrossRef]
- Pillunat, L.E.; Erb, C.; Junemann, A.G.M.; Kimmich, F. Micro-invasive glaucoma surgery (MIGS): A review of surgical procedures using stents. Clin. Ophthalmol. 2017, 11, 1583–1600. [Google Scholar] [CrossRef] [Green Version]
- Parra, M.T.M.; Lopez, J.A.S.; Grau, N.S.L.; Ceausescu, A.M.; Santonja, J.J.P. XEN implant device versus trabeculectomy, either alone or in combination with phacoemulsification, in open-angle glaucoma patients. Graefe’s Arch. Clin. Exp. Ophthalmol. 2019, 257, 1741–1750. [Google Scholar] [CrossRef]
- Grover, D.S.; Flynn, W.J.; Bashford, K.P.; Lewis, R.A.; Duh, Y.-J.; Nangia, R.S.; Niksch, B. Performance and safety of a new ab interno gelatin stent in refractory glaucoma at 12 months. Am. J. Ophthalmol. 2017, 183, 25–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
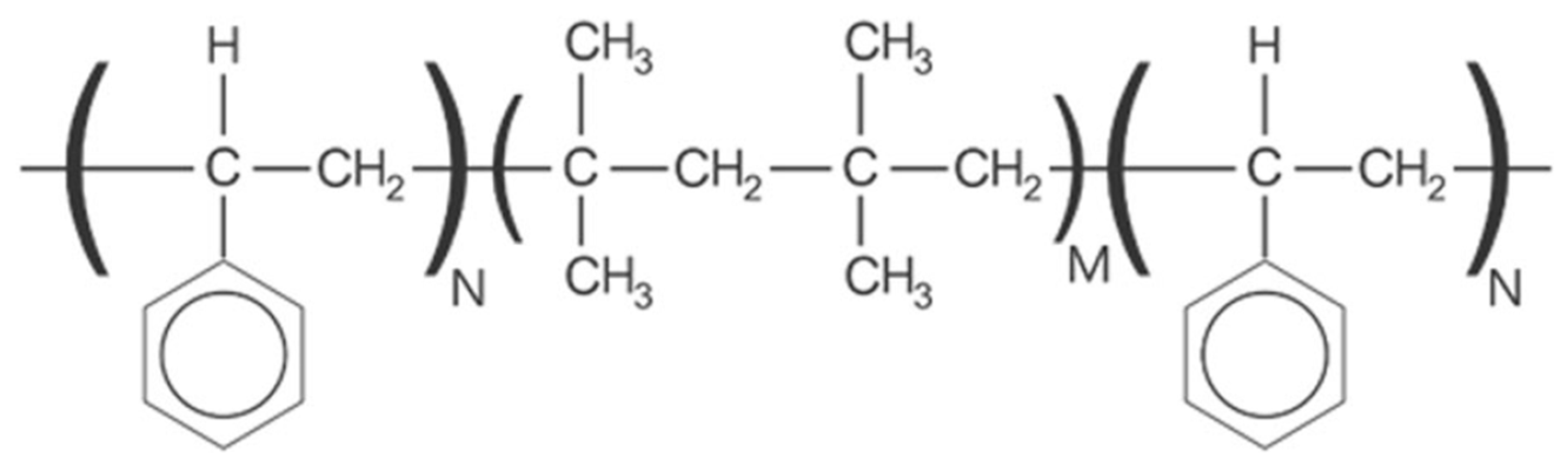
- Pinchuk, L.; Riss, I.; Batlle, J.F.; Kato, Y.P.; Martin, J.B.; Arrieta, E.; Palmberg, P.; Parrish, R.K.; Weber, B.A.; Kwon, Y.; et al. The use of poly(styrene-block-isobutylene-block-styrene) as a microshunt to treat glaucoma. Regen. Biomater. 2016, 3, 137–142. [Google Scholar] [CrossRef] [Green Version]
- Pinchuk, L.; Riss, I.; Batlle, J.F.; Kato, Y.P.; Martin, J.B.; Arrieta, E.; Palmberg, P.; Parrish, R.K.; Weber, B.A.; Kwon, Y.; et al. The development of a micro-shunt made from poly(styrene-block-isobutylene-block-styrene) to treat glaucoma. J. Biomed. Mater. Res. B 2017, 105, 211–221. [Google Scholar] [CrossRef] [PubMed]
- Batlle, J.F.; Fantes, F.; Riss, I.; Pinchuk, L.; Alburquerque, R.; Kato, Y.P.; Arrieta, E.; Peralta, A.C.; Palmberg, P.; Parrish, R.K., 2nd; et al. Three-Year Follow-up of a Novel Aqueous Humor MicroShunt. J. Glaucoma 2016, 25, e58–e65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinchuk, L.; Wilson, G.J.; Barry, J.J.; Schoephoerster, R.T.; Parel, J.M.; Kennedy, J.P. Medical applications of poly(styrene-block-isobutylene-block-styrene) (“SIBS”). Biomaterials 2008, 29, 448–460. [Google Scholar] [CrossRef]
- Parel, J.; Stoiber, J.; Fernandez, V. Optical properties and biocompatibility of a novel polymer for intraocular implants: Comparative study in the rabbit. Ophthalmic. Technol. 2004, XIV#5314-45, 24–25. [Google Scholar]
- Acosta, A.C.; Espana, E.M.; Yamamoto, H.; Davis, S.; Pinchuk, L.; Weber, B.A.; Orozco, M.; Dubovy, S.; Fantes, F.; Parel, J.M. A newly designed glaucoma drainage implant made of poly(styrene-b-isobutylene-b-styrene)—Biocompatibility and function in normal rabbit eyes. Arch. Ophthalmol.-Chic. 2006, 124, 1742–1749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fantes, F.; Acosta, A.; Carraway, J.; Pinchuk, L.; Weber, B.; Davis, S.; Arrieta, E.; Parel, J.M. An independent GLP evaluation of a new glaucoma drain, the MIDI. Investig. Ophthalmol. Vis. Sci. 2006, 47, 3547. [Google Scholar]
- Arrieta, E.A.; Aly, M.; Parrish, R.; Dubovy, S.; Pinchuk, L.; Kato, Y.; Fantes, F.; Parel, J.M. Clinicopathologic correlations of poly-(styrene-b-isobutylene-b-styrene) glaucoma drainage devices of different internal diameters in rabbits. Ophthalmic Surg. Lasers Imaging 2011, 42, 338–345. [Google Scholar] [CrossRef] [PubMed]
- Pinchuk, L.; Fantes, F.; Zhou, Y.; Martin, J.; Parel, J.M. The BPEI–InnFocus Glaucoma Drainage Implant–The MiDi: Concept, Physics and Pressure Control. Investig. Ophthalmol. Vis. Sci. 2006, 47, 36. [Google Scholar]
- Silber, S.; Colombo, A.; Banning, A.P.; Hauptmann, K.; Drzewiecki, J.; Grube, E.; Dudek, D.; Baim, D.S. Final 5-year results of the TAXUS II trial: A randomized study to assess the effectiveness of slow- and moderate-release polymer-based paclitaxel-eluting stents for de novo coronary artery lesions. Circulation 2009, 120, 1498–1504. [Google Scholar] [CrossRef] [Green Version]
- Strickler, F.; Richard, R.; McFadden, S.; Lindquist, J.; Schwarz, M.C.; Faust, R.; Wilson, G.J.; Boden, M. In vivo and in vitro characterization of poly(styrene-b-isobutylene-b-styrene) copolymer stent coatings for biostability, vascular compatibility and mechanical integrity. J. Biomed. Mater. Res. A 2010, 92, 773–782. [Google Scholar] [CrossRef]
- Sadruddin, O.; Pinchuk, L.; Angeles, R.; Palmberg, P. Ab externo implantation of the MicroShunt, a poly (styrene-block-isobutylene-block-styrene) surgical device for the treatment of primary open-angle glaucoma: A review. Eye Vis. (Lond) 2019, 6, 36. [Google Scholar] [CrossRef] [PubMed]
- Morita, K.; Gao, Y.; Saito, Y.; Higashide, T.; Kobayashi, A.; Ohkubo, S.; Sugiyama, K. In vivo confocal microscopy and ultrasound biomicroscopy study of filtering blebs after trabeculectomy: Limbus-based versus fornix-based conjunctival flaps. J. Glaucoma 2012, 21, 383–391. [Google Scholar] [CrossRef] [PubMed]
- An, D.; Morgan, W.H.; Yu, D.Y. Glymphatics and lymphatics in the eye and central nervous system. Clin. Exp. Ophthalmol. 2017, 45, 440–441. [Google Scholar] [CrossRef]
- Jeon, T.Y.; Kim, H.J.; Kim, S.T.; Chung, T.Y.; Kee, C. MR imaging features of giant reservoir formation in the orbit: An unusual complication of Ahmed glaucoma valve implantation. AJNR Am. J. Neuroradiol. 2007, 28, 1565–1566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilkins, M.; Indar, A.; Wormald, R. Intraoperative mitomycin C for glaucoma surgery. Cochrane Database Syst. Rev. 2005. [Google Scholar] [CrossRef] [PubMed]
- Martinez-de-la-Casa, J.M.; Saenz-Frances, F.; Morales-Fernandez, L.; Perucho, L.; Mendez, C.; Fernandez-Vidal, A.; Garcia-Saenz, S.; Sanchez-Jean, R.; Garcia-Feijoo, J. Clinical outcomes of combined Preserflo Microshunt implantation and cataract surgery in open-angle glaucoma patients. Sci. Rep. 2021, 11, 15600. [Google Scholar] [CrossRef]
- Shaarawy, T. Glaucoma surgery: Taking the sub-conjunctival route. Middle East Afr. J. Ophthalmol. 2015, 22, 53–58. [Google Scholar] [CrossRef] [Green Version]
- Beckers, H.J.M.; Aptel, F.; Webers, C.A.B.; Bluwol, E.; Martinez-de-la-Casa, J.M.; Garcia-Feijoo, J.; Lachkar, Y.; Mendez-Hernandez, C.D.; Riss, I.; Shao, H.; et al. Safety and Effectiveness of the PRESERFLO(R) MicroShunt in Primary Open-Angle Glaucoma: Results from a 2-Year Multicenter Study. Ophthalmol. Glaucoma 2021. [Google Scholar] [CrossRef]
- Riss, I.; Batlle, J.; Pinchuk, L.; Kato, Y.P.; Weber, B.A.; Parel, J.M. One-year results on the safety and efficacy of the InnFocus MicroShunt depending on placement and concentration of mitomycin C. J. Fr. Ophtalmol. 2015, 38, 855–860. [Google Scholar] [CrossRef]
- Batlle, J.F.; Corona, A.; Albuquerque, R. Long-term Results of the PRESERFLO MicroShunt in Patients With Primary Open-angle Glaucoma From a Single-center Nonrandomized Study. J. Glaucoma 2021, 30, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Beckers, H.J.M.; Kujovic-Aleksov, S.; Webers, C.A.B.; Riss, I.; Batlle, J.; Parel, J.M. One-year results of a three-site study of the InnFocus MicroShunt (R). Acta Ophthalmol. 2017, 95, 28–29. [Google Scholar]
- Schlenker, M.B.; Durr, G.M.; Michaelov, E.; Ahmed, I.I.K. Intermediate Outcomes of a Novel Standalone Ab Externo SIBS Microshunt With Mitomycin C. Am. J. Ophthalmol. 2020, 215, 141–153. [Google Scholar] [CrossRef] [PubMed]
- Fea, A.M.; Laffi, G.L.; Martini, E.; Economou, M.A.; Caselgrandi, P.; Sacchi, M.; Au, L. Effectiveness of MicroShunt in Patients with Primary Open-Angle and Pseudoexfoliative Glaucoma: A Retrospective European Multicenter Study. Ophthalmol. Glaucoma 2021. [Google Scholar] [CrossRef] [PubMed]
- Küchle, M.; Nguyen, N.; Hannappel, E.; Naumann, G. The blood-aqueous barrier in eyes with pseudoexfoliation syndrome. Ophthalmic. Lit. 1996, 2, 137. [Google Scholar]
- Schumacher, S.; Nguyen, N.X.; Kuchle, M.; Naumann, G.O. Quantification of aqueous flare after phacoemulsification with intraocular lens implantation in eyes with pseudoexfoliation syndrome. Arch. Ophthalmol.-Chic. 1999, 117, 733–735. [Google Scholar] [CrossRef] [Green Version]
- Gedde, S.J.; Schiffman, J.C.; Feuer, W.J.; Herndon, L.W.; Brandt, J.D.; Budenz, D.L.; Tube Versus Trabeculectomy Study, G. Three-year follow-up of the tube versus trabeculectomy study. Am. J. Ophthalmol. 2009, 148, 670–684. [Google Scholar] [CrossRef]
- Gedde, S.J.; Schiffman, J.C.; Feuer, W.J.; Parrish, R.K., 2nd; Heuer, D.K.; Brandt, J.D.; Tube Versus Trabeculectomy Study, G. The tube versus trabeculectomy study: Design and baseline characteristics of study patients. Am. J. Ophthalmol. 2005, 140, 275–287. [Google Scholar] [CrossRef]
- Gedde, S.J.; Schiffman, J.C.; Feuer, W.J.; Herndon, L.W.; Brandt, J.D.; Budenz, D.L. Treatment outcomes in the tube versus trabeculectomy study after one year of follow-up. Am. J. Ophthalmol. 2007, 143, 9–22. [Google Scholar] [CrossRef] [PubMed]
- Chou, J.; Turalba, A.; Hoguet, A. Surgical Innovations in Glaucoma: The Transition From Trabeculectomy to MIGS. Int. Ophthalmol. Clin 2017, 57, 39–55. [Google Scholar] [CrossRef]
- Pillunat, K.R.; Herber, R.; Haase, M.A.; Jamke, M.; Jasper, C.S.; Pillunat, L.E. PRESERFLO MicroShunt versus trabeculectomy: First results on efficacy and safety. Acta Ophthalmol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Baker, N.D.; Barnebey, H.S.; Moster, M.R.; Stiles, M.C.; Vold, S.D.; Khatana, A.K.; Flowers, B.E.; Grover, D.S.; Strouthidis, N.G.; Panarelli, J.F. Ab-externo MicroShunt versus Trabeculectomy in Primary Open-Angle Glaucoma: 1-year Results from a 2-year Randomized, Multicenter Study. Ophthalmology 2021, 128, 1710–1721. [Google Scholar] [CrossRef] [PubMed]
- Quaranta, L.; Micheletti, E.; Carassa, R.; Bruttini, C.; Fausto, R.; Katsanos, A.; Riva, I. Efficacy and Safety of PreserFlo((R)) MicroShunt After a Failed Trabeculectomy in Eyes with Primary Open-Angle Glaucoma: A Retrospective Study. Adv. Ther. 2021, 38, 4403–4412. [Google Scholar] [CrossRef] [PubMed]
- Gillmann, K.; Mansouri, K. Minimally invasive glaucoma surgery: Where is the evidence? Asia-Pac. J. Ophthalmol. 2020, 9, 203. [Google Scholar] [CrossRef] [PubMed]
- Bartelt-Hofer, J.; Flessa, S. Comparative efficacy and cost-utility of combined cataract and minimally invasive glaucoma surgery in primary open-angle glaucoma. Int. Ophthalmol. 2020, 40, 1469–1479. [Google Scholar] [CrossRef] [Green Version]
- Scheres, L.M.J.; Kujovic-Aleksov, S.; Ramdas, W.D.; de Crom, R.; Roelofs, L.C.G.; Berendschot, T.; Webers, C.A.B.; Beckers, H.J.M. XEN((R)) Gel Stent compared to PRESERFLO MicroShunt implantation for primary open-angle glaucoma: Two-year results. Acta Ophthalmol. 2021, 99, e433–e440. [Google Scholar] [CrossRef]
- Sheybani, A.; Lenzhofer, M.; Hohensinn, M.; Reitsamer, H.; Ahmed, I.I.K. Phacoemulsification combined with a new ab interno gel stent to treat open-angle glaucoma: Pilot study. J. Cataract Refract. Surg. 2015, 41, 1905–1909. [Google Scholar] [CrossRef]
- Sheybani, A.; Dick, H.B.; Ahmed, I.I.K. Early Clinical Results of a Novel Ab Interno Gel Stent for the Surgical Treatment of Open-angle Glaucoma. J. Glaucoma 2016, 25, e691–e696. [Google Scholar] [CrossRef]
- Green, W.; Lind, J.T.; Sheybani, A. Review of the Xen Gel Stent and InnFocus MicroShunt. Curr. Opin. Ophthalmol. 2018, 29, 162–170. [Google Scholar] [CrossRef] [PubMed]
- Wagner, F.M.; Schuster, A.K.; Munder, A.; Muehl, M.; Pfeiffer, N.; Hoffmann, E.M. Comparison of subconjunctival microinvasive glaucoma surgery and trabeculectomy. Acta Ophthalmol. 2021. [Google Scholar] [CrossRef]
- Bettin, P. Postoperative management of penetrating and nonpenetrating external filtering procedures. Dev. Ophthalmol. 2012, 50, 48–63. [Google Scholar]
- Brambati, M.; Bettin, P.; Ramoni, A.; Battista, M.; Bandello, F. A case of endophthalmitis following needling procedure after PRESERFLO((R)) Micro Shunt implantation. Eur. J. Ophthalmol. 2021, 11206721211019548. [Google Scholar] [CrossRef] [PubMed]
- Feldman, R.M.; Tabet, R.R. Needle revision of filtering blebs. J. Glaucoma 2008, 17, 594–600. [Google Scholar] [CrossRef]
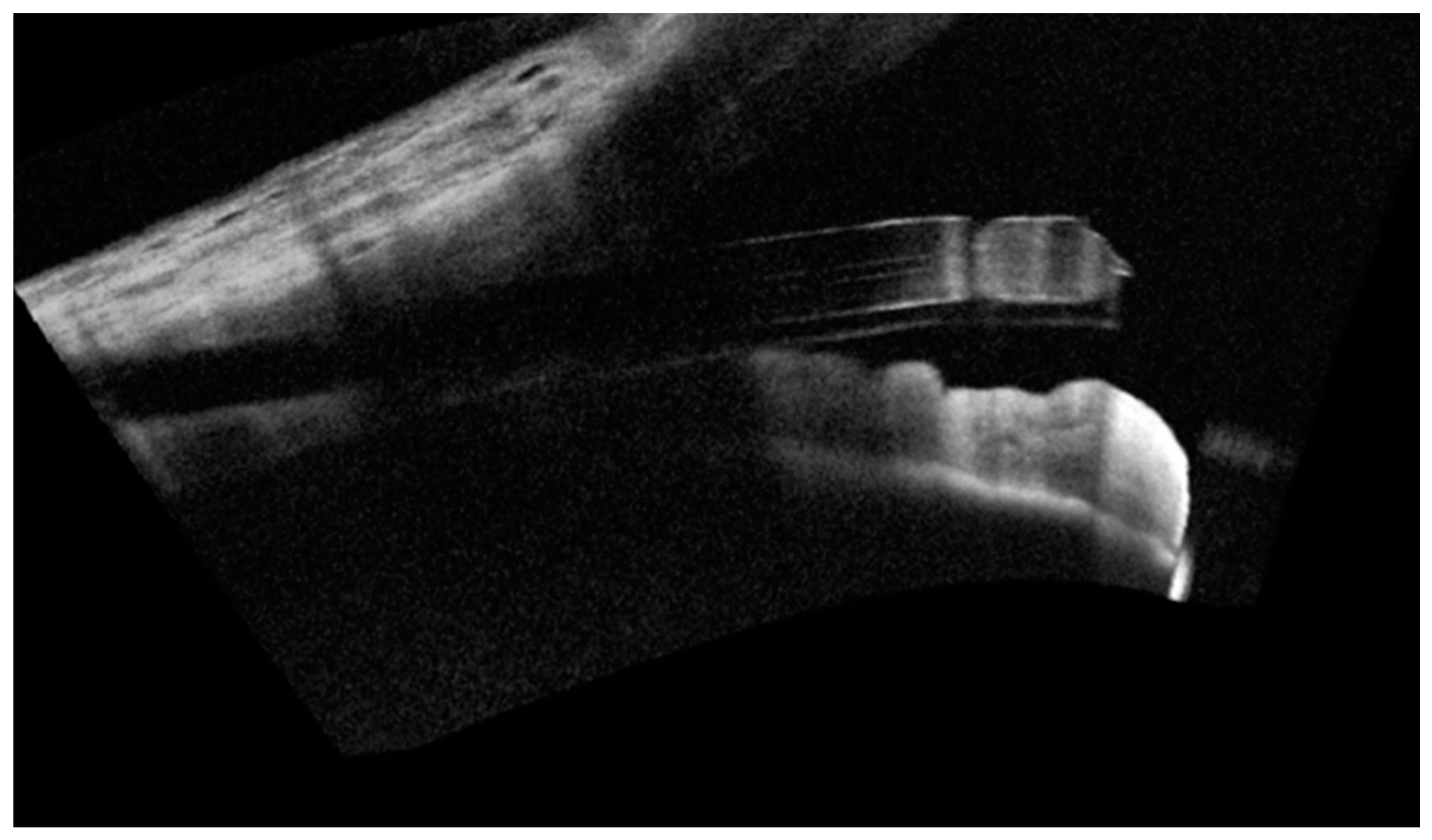
- Ibarz Barbera, M.; Morales Fernandez, L.; Tana Rivero, P.; Gomez de Liano, R.; Teus, M.A. Anterior-segment optical coherence tomography of filtering blebs in the early postoperative period of ab externo SIBS microshunt implantation with mitomycin C: Morphological analysis and correlation with intraocular pressure reduction. Acta Ophthalmol. 2021, 100, e192–e203. [Google Scholar] [CrossRef] [PubMed]
- Ibarz Barbera, M.; Hernandez-Verdejo, J.L.; Bragard, J.; Burguete, J.; Fernandez, L.M.; Rivero, P.T.; de Liano, R.G.; Teus, M.A. Evaluation of the Ultrastructural and In Vitro Flow Properties of the PRESERFLO MicroShunt. Transl. Vis. Sci. Technol. 2021, 10, 26. [Google Scholar] [CrossRef] [PubMed]
- Teus, M.A.; Moreno-Arrones, J.P.; Castano, B.; Castejon, M.A.; Bolivar, G. Optical coherence tomography analysis of filtering blebs after long-term, functioning trabeculectomy and XEN (R) stent implant. Graef. Arch. Clin. Exp. 2019, 257, 1005–1011. [Google Scholar] [CrossRef] [Green Version]
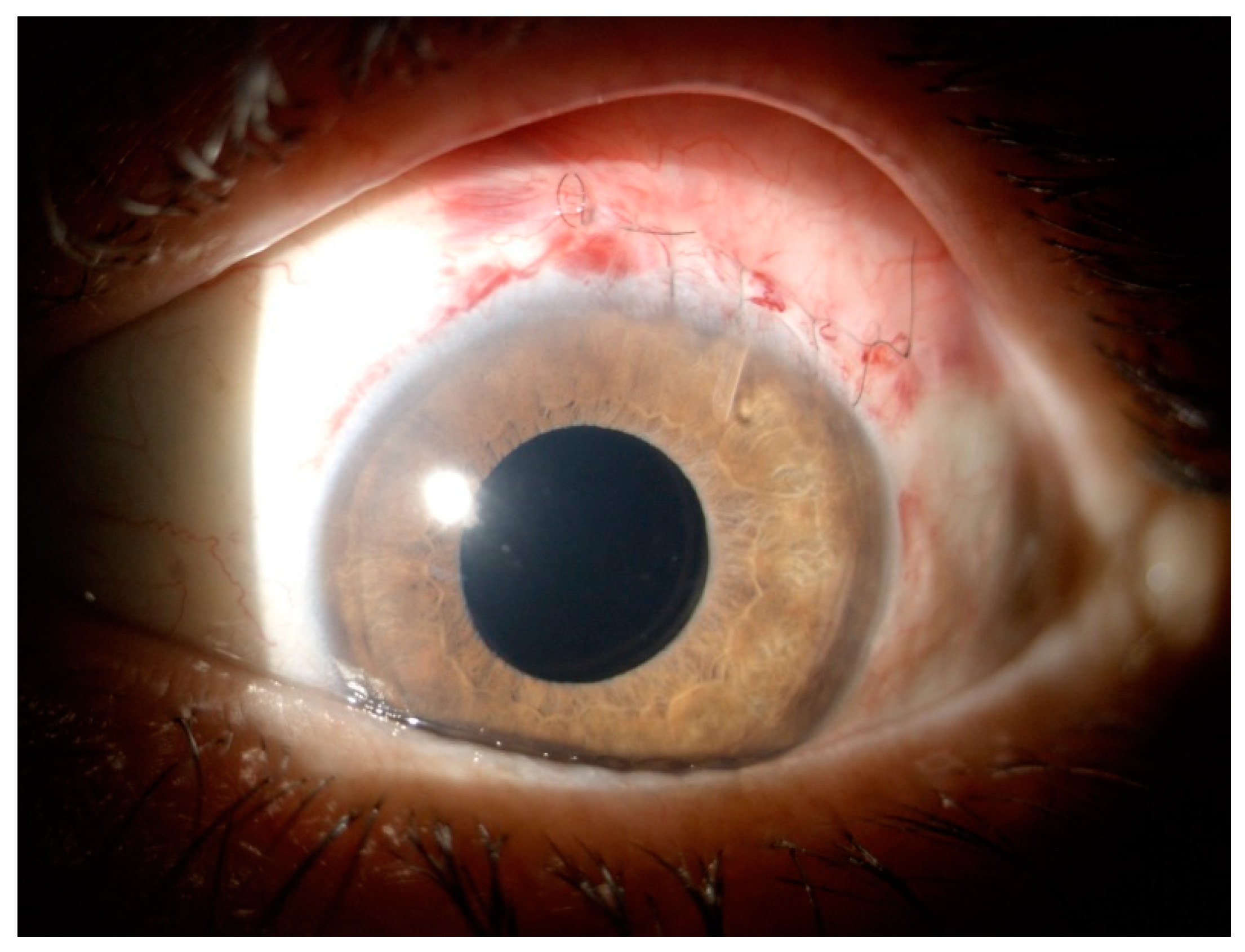
- Bunod, R.; Robin, M.; Buffault, J.; Keilani, C.; Labbe, A.; Baudouin, C. PreserFlo MicroShunt(R) exposure: A case series. BMC Ophthalmol. 2021, 21, 273. [Google Scholar] [CrossRef]
- Kerr, N.M.; Ahmed, I.I.K.; Pinchuk, L.; Sadruddin, O.; Palmberg, P.F. PRESERFLO MicroShunt. In Minimally Invasive Glaucoma Surgery; Springer: Singapore, 2021; pp. 91–103. [Google Scholar]
- Micheletti, E.; Riva, I.; Bruttini, C.; Quaranta, L. A Case of Delayed-onset Hemorrhagic Choroidal Detachment After PreserFlo Microshunt Implantation in a Glaucoma Patient Under Anticoagulant Therapy. J. Glaucoma 2020, 29, e87–e90. [Google Scholar] [CrossRef]
- Gizzi, C.; Costa, G.; Servadei, R.; Abed, E.; Ning, B.; Sharma, A.; Barton, K. A case of malignant glaucoma following insertion of Preserflo MicroShunt. Eur. J. Ophthalmol. 2021, 11206721211003492. [Google Scholar] [CrossRef]
- Vastardis, I.; Fili, S.; Perdikakis, G.; Kontopoulou, K.; Balidis, M.; Gatzioufas, Z.; Kohlhaas, M. Preliminary results of Preserflo Microshunt versus Preserflo Microshunt and Ologen implantation. Eye Vis. (Lond) 2021, 8, 33. [Google Scholar] [CrossRef] [PubMed]
- Fili, S.; Seddig, S.; Kohlhaas, M. Long-Term Results after Trabeculectomy Combined with Mitomycin C and Ologen Implant. Klin. Monbl. Augenheilkd. 2019, 236, 1107–1114. [Google Scholar] [PubMed]
- Rho, S.; Sung, Y.; Ma, K.T.; Rho, S.H.; Kim, C.Y. Bleb Analysis and Short-Term Results of Biodegradable Collagen Matrix-Augmented Ahmed Glaucoma Valve Implantation: 6-Month Follow-up. Investig. Ophthalmol. Vis. Sci. 2015, 56, 5896–5903. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papaconstantinou, D.; Georgalas, I.; Karmiris, E.; Diagourtas, A.; Koutsandrea, C.; Ladas, I.; Apostolopoulos, M.; Georgopoulos, G. Trabeculectomy with OloGen versus trabeculectomy for the treatment of glaucoma: A pilot study. Acta Ophthalmol. 2010, 88, 80–85. [Google Scholar] [CrossRef]
- Picht, G.; Grehn, F. Classification of filtering blebs in trabeculectomy: Biomicroscopy and functionality. Curr. Opin. Ophthalmol. 1998, 9, 2–8. [Google Scholar] [CrossRef]
- Durr, G.M.; Schlenker, M.B.; Samet, S.; Ahmed, I.I.K. One-year outcomes of stand-alone ab externo SIBS microshunt implantation in refractory glaucoma. Br. J. Ophthalmol. 2022, 106, 71–79. [Google Scholar] [CrossRef]
- Jones, J.P.; Fong, D.S.; Fang, E.N.; Mesirov, C.A.; Patel, V. Characterization of Glaucoma Medication Adherence in Kaiser Permanente Southern California. J. Glaucoma 2016, 25, 22–26. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study | No. of Eyes | Pre-op IOP (mmHg) | Pre-op Drugs | Follow-Up | Final IOP (mmHg) | Post-op Drugs |
|---|---|---|---|---|---|---|
| Riss et al. (2015) [33] | 23 * | 23.8 | 2.6 | 1 year | 10.7 | 0.3 |
| Batlle et al. (2016) [15] | 23 * | 23.8 | 2.4 | 3 years | 10.7 | 0.7 |
| Batlle et al. (2021) [34] | 23 * | 23.8 | 2.4 | 5 years | 12.4 | 0.4 |
| Beckers et al. (2017) [35] | 91 | 24.3 | 2.4 | 1 year | 13.3 | 0.4 |
| Schlenker et al. (2015) [36] | 164 | 21.4 | 3.4 | 1 year | 13.3 | 0.5 |
| Martinez-de-la-Casa (2021) [30] | 58 | 21.5 | 2.3 | 1 year | 14.6 | 0.2 |
| Beckers et al. (2021) [32] | 81 | 21.7 | 2.5 | 2 year | 14.1 | 0.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gambini, G.; Carlà, M.M.; Giannuzzi, F.; Caporossi, T.; De Vico, U.; Savastano, A.; Baldascino, A.; Rizzo, C.; Kilian, R.; Caporossi, A.; et al. PreserFlo® MicroShunt: An Overview of This Minimally Invasive Device for Open-Angle Glaucoma. Vision 2022, 6, 12. https://0-doi-org.brum.beds.ac.uk/10.3390/vision6010012
Gambini G, Carlà MM, Giannuzzi F, Caporossi T, De Vico U, Savastano A, Baldascino A, Rizzo C, Kilian R, Caporossi A, et al. PreserFlo® MicroShunt: An Overview of This Minimally Invasive Device for Open-Angle Glaucoma. Vision. 2022; 6(1):12. https://0-doi-org.brum.beds.ac.uk/10.3390/vision6010012
Chicago/Turabian StyleGambini, Gloria, Matteo Mario Carlà, Federico Giannuzzi, Tomaso Caporossi, Umberto De Vico, Alfonso Savastano, Antonio Baldascino, Clara Rizzo, Raphael Kilian, Aldo Caporossi, and et al. 2022. "PreserFlo® MicroShunt: An Overview of This Minimally Invasive Device for Open-Angle Glaucoma" Vision 6, no. 1: 12. https://0-doi-org.brum.beds.ac.uk/10.3390/vision6010012