Randomised, Single Blind, Controlled, Three-Month Clinical Trial on the Evaluation and Treatment of the Ocular Surface Damage Following Phacoemulsification


Abstract
:1. Introduction
2. Methods
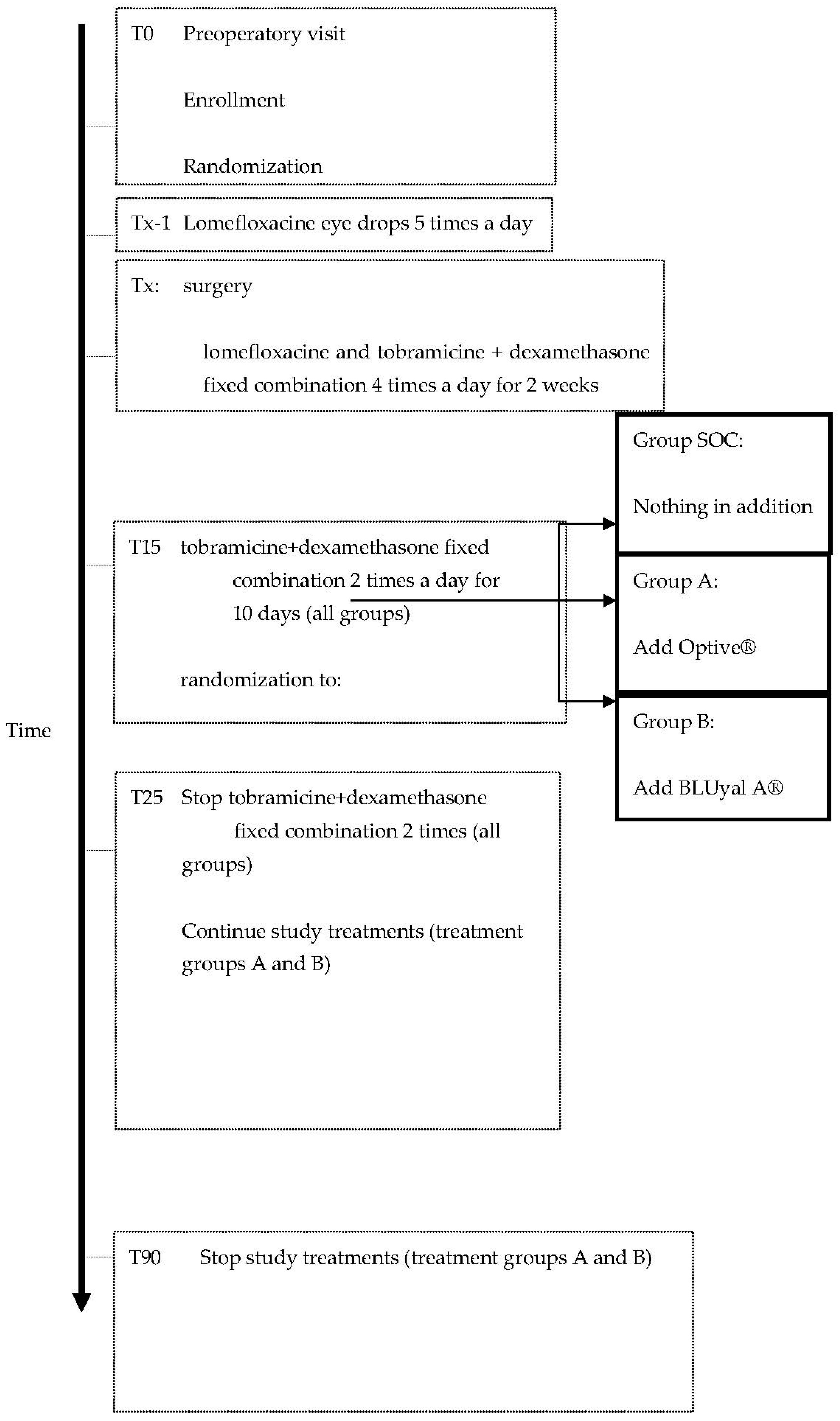
- Standard of care. The SOC treatment in use at the Clinica Oculistica was as follows: from the day of surgery, the following eye drops were used: lomefloxacine and tobramicine + dexamethasone fixed combination 4 times a day for 2 weeks; then Tobramicine + dexamethasone fixed combination 2 times a day until day 25 from surgery.
- Arm A: patients received an artificial tear designed with a dual action formula which contains carboxymethylcellulose 0.5% (a long lasting lubricant), glycerin (an ideal moisturiser), and purite (a safe gentle preservative) (Optive ®). This blend of ingredients can provide long-lasting, deep hydration of the tear film and corneal cells, as well as an important osmoprotection. The eye drop is safely drawn into the corneal epithelial cells below the surface to osmotically protect against hypertonic stress. That’s why it is recommended for patients with intermittent dry eye symptoms.
- Arm B: patients received a sterile isotonic ophthalmic solution made up of hyaluronic acid 0.15%, sodium hydroxymethylglycinate (N-IG) and 4 different amino acids (L-proline, L-glycine, hydrochloride L-lysine and L-leucine) (BluYalA ®). It is proposed to be able to supplement insufficient tear secretion and restore the physiological conditions of the tear film thanks to: hyaluronic acid, which stays on the ocular surface for a long time and stabilises the tear film for its mucoadhesive characteristics; the N-IG, a new generation amino acid derivative with an antimicrobial activity that should have an effective preserving action and no negative effects on the surface of the eye; and the amino acids L-proline, L-glycine, hydrochloride L-lysine and L-leucine, which are important in maintaining structural condition and metabolic processes of the cornea. Actually, the product is used to protect, humidify and lubricate the surface of the eye bringing particularly extended relief to disturbances caused by mechanical, environmental and visual stress.
2.1. Adverse Events
2.2. Blinding/Masking
2.3. Randomisation Procedures
2.4. Ocular Examination
2.4.1. Schirmer I Test (ST-I)
2.4.2. Tear Film Break-Up Time (tf-BUT)
2.4.3. Fluorescein Staining for the Evaluation of the Corneal Damage
2.4.4. Conjunctival Hyperaemia
2.4.5. Ocular Surface Disease Index (OSDI)
2.4.6. NEI-VFQ 25
2.5. Statistics
3. Results
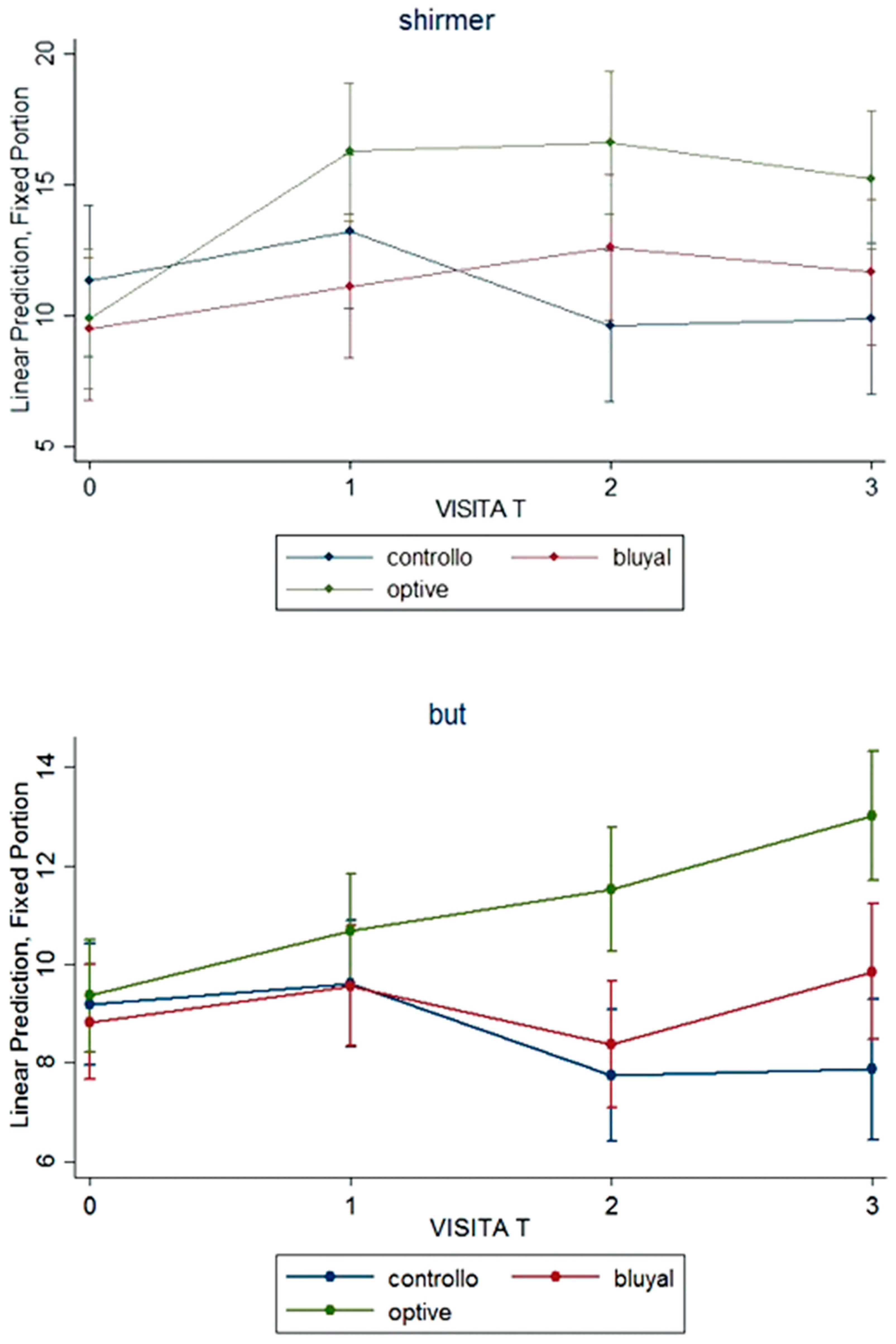
3.1. Signs
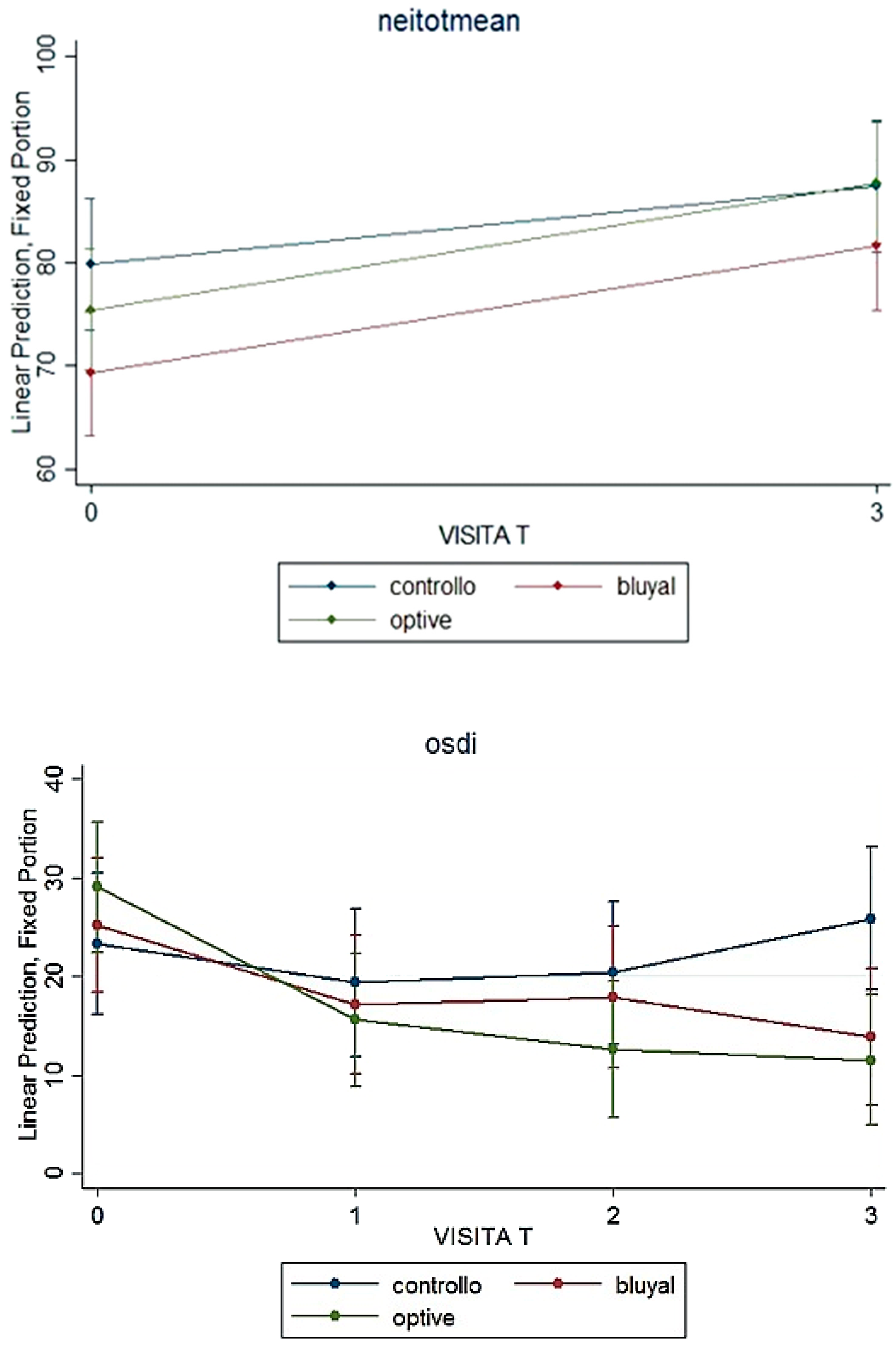
3.2. Symptoms
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kohlhaas, M. Corneal sensation after cataract and refractive surgery. J. Cataract. Refract. Surg. 1998, 24, 1399–1409. [Google Scholar] [CrossRef]
- Li, X.M.; Hu, L.; Wang, W. Investigation of dry eye disease and analysis of the pathogenic factors in patients after cataract surgery. Cornea 2007, 26, S16–S20. [Google Scholar] [CrossRef] [PubMed]
- Sitompui, R.; Sancoyo, G.S.; Hutauruk, J.A.; Gondhowiardjo, T.D. Sensitivity change in cornea and tear layer due to incision difference on cataract surgery with either manual small-incision cataract surgery or phacoemulsification. Cornea 2008, 27, S13–S18. [Google Scholar] [CrossRef] [Green Version]
- Ram, J.; Gupta, A.; Brar, G.S.; Kaushik, S.; Gupta, A. Outcomes of phacoemulsification in patients with dry eye. J. Cataract. Refract. Surg. 2002, 28, 1386–1389. [Google Scholar] [CrossRef]
- Cho, Y.K.; Kim, M.S. Dry eye after cataract surgery and associated intraoperative risk factors. Korean J. Opthalmol. 2009, 23, 65–73. [Google Scholar] [CrossRef] [Green Version]
- Walker, T.D. Benzalkonium toxicity. Clin. Experiment Ophthalmol. 2004, 32, 657. [Google Scholar] [CrossRef]
- Khanal, S.; Tomlinson, A.; Esakowitz, L.; Bhatt, P.; Jones, D.; Nabili, S.; Mukerji, S. Changes in corneal sensitivity and tear physiology after phacoemulsification. Ophthal. Physiol. Opt. 2008, 28, 127–134. [Google Scholar] [CrossRef]
- Donnenfeld, E.D.; Solomon, K.; Perry, H.D.; Doshi, S.J.; Ehrenhaus, M.; Solomon, R.; Biser, S. The effect of hinge position on corneal sensation and dry eye after LASIK. Ophthalmology 2003, 110, 1023–1029. [Google Scholar] [CrossRef]
- Wolffsohn, J.S.; Arita, R.; Chalmers, R.; Djalilian, A.; Dogru, M.; Dumbleton, K.; Gupta, P.K.; Karpecki, P.; Lazreg, S.; Pult, H.; et al. TFOS DEWS II Diagnostic Methodology report. Ocul. Surf. 2017, 15, 539–574. [Google Scholar] [CrossRef]
- Stefan, C.; Dumitrica, D.M. Systane and cataract surgery. Oftalmologia 2007, 51, 100–104. (In Romanian) [Google Scholar]
- Rossi, G.C.M.; Milano, G.; Tinelli, C. The Italian version of the 25-item National Eye Institute Visual Function Questionnaire: Translation, Validity and Reliability. J. Glaucoma 2003, 12, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Shiffman, R.M.; Christianson, M.D.; Jacobsen, G.; Hirsch, J.D.; Reis, B.L. Reliability and validity of the ocular surface disease index. Arch. Ophthalmol. 2000, 118, 615–621. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, M.A.; Villalobos, P.A.; Torraldo-Jienez, P.; Giron, N. The effect of preservative-free Hpguar on dry eye after phacoemulsification: A flow cytometric study. Eye 2010, 24, 1331–1337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yao, K.; Bao, Y.; Ye, J. Efficacy of 1% carboxymethylcellulose sodium for treating dry eye after phacoemulsification: Results from a multicenter, open-label, controlled study. BMC Ophthalmol. 2015, 15, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donghyun, J.; Minij, P.; Hee, J.L.; Man, S.K.; Eun, C.K. Comparison of treatment with preservative-free versus preserved sodium hyaluronate 0.1% and fluorometholone 0.1% eyedrops after cataract surgery in patients with preexisting dry eye syndrome. J. Cat. Refr. Surg. 2015, 41, 756–763. [Google Scholar]
- Lee, J.H.; Song, I.S.; Kim, K.L.; Yoon, S.Y. Effectiveness and optical quality of topical 3.0% diquafosol versus 0.05% cyclosporine A in dry eye patients following cataract surgery. J. Ophthalmol. 2016, 2016, 8150757. [Google Scholar] [CrossRef] [Green Version]
- Bron, A.J.; Evans, V.E.; Smith, J.A. Grading of corneal and conjunctival staining in the context of other dry eye tests. Cornea 2003, 22, 640–650. [Google Scholar] [CrossRef]
- DEWS. The epidemiology of dry eye disease: Report of the Epidemiology Subcommittee of the International Dry Eye WorkShop. Ocul. Surf. 2007, 5, 93–107. [Google Scholar] [CrossRef]
- Kohli, P.; Arya, S.K.; Rai, A.; Handa, U. Changes in ocular surface status after phacoemulsification in patients with senile cataract. Int. Ophthalmol. 2019, 39, 1345–1353. [Google Scholar] [CrossRef]
- Han, K.E.; Yoon, S.C.; Ahn, J.M.; Nam, S.M.; Stulting, R.D.; Kim, E.K.; Seo, K.Y. Evaluation of dry eye and meibomiam gland disfunction after cataract surgery. Am. J. Ophthalmol. 2014, 157, 1144–1150. [Google Scholar] [CrossRef]
- Cetinkaya, S.; Mestan, E.; Acir, N.O.; Cetinkaya, Y.F.; Dadaci, Z.; Yener, H.I. The course of dry eye after phacoemulsification surgery. BMC Ophthalmol. 2015, 15, 68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishrat, S.; Nema, N.; Chandravanshi, S. Incidence and pattern of dry eye after cataract surgery. Saudi J. Ophthalmol. 2019, 33, 34–40. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Activity | Visit 1 T0 (Screening) | Visit 2 Tx (Surgery) | Visit 3 T1 (1 Pod) | Visit 4 T15 (15 Pod ± 3) | Visit 5 T45 (45 Pod ± 7) | Visit 6 T90 (90 Pod ± 15) |
|---|---|---|---|---|---|---|
| Informed consent | X | |||||
| Demographic and History | X | |||||
| Physical examination | X | |||||
| Ocular examination | X | X | X | X | X | |
| Visual acuity | X | X | X | X | ||
| Eligibility criteria | X | |||||
| Surgery data | X | |||||
| Randomisation | X | |||||
| Eye drop prescription | X | X | X | |||
| Schirmer I | X | X | X | X | ||
| tBUT | X | X | X | X | X | |
| Corneal fluorescein staining | X | X | X | X | X | |
| OSDI | X | X | X | X | ||
| NEI-VFQ 25 | X | X | ||||
| Adverse events | X | X | X |
| Visit Time (Days) | SOC N = 16 | Lacrimal Substitute (LS) N = 37 | p-Value of Difference between Groups over Time | |
|---|---|---|---|---|
| Visual acuity (decimals) | 0 | 0.3 [0.2–0.4] | 0.4 [0.2–0.4] | |
| 15 | 0.8 [0.6–1.0] | 1.0 [0.8–1.0] | 0.974 | |
| 45 | 0.9 [0.8–1.0] | 1.0 [0.8–1.0] | 0.999 | |
| 90 | 0.9 [0.8–1.0] | 1.0 [1.0–1.0] | 0.515 | |
| Schirmer I (mm) | 0 | 10 [10–12] | 10 [7–10] | --- |
| 15 | 12 [8–16] | 10.5 [6.5–21] | 0.173 | |
| 45 | 10.5 [5–12.5] | 12 [9–20] | <0.001 | |
| 90 | 10 [7–11.5] | 12.5 [10–17] | 0.001 | |
| BUT (s) | 0 | 9 [7.5–10] | 9 [8–10] | --- |
| 15 | 10 [7–12] | 10 [9–11.5] | 0.455 | |
| 45 | 8 [6–10] | 10 [8–12] | 0.009 | |
| 90 | 7.5 [6–9.5] | 9 [10.5–13] | <0.001 | |
| Corneal fluorescein staining (Grade > 0) Number (%) | 0 | 0 (0) | 5 (13.5) | |
| 15 | 2 (13.3) | 1 (2.8) | 0.981 | |
| 45 | 3 (18.7) | 4 (11.8) | 0.982 | |
| 90 | 3 (18.7) | 2 (5.6) | 0.981 | |
| Conjunctival hyperaemia (Grade > 0) Number (%) | 0 | 0 (0) | 4 (11.1) | |
| 15 | 1 (6.7) | 6 (16.7) | 0.990 | |
| 45 | 1 (6.7) | 5 (15.1) | 0.990 | |
| 90 | 2 (12.5) | 5 (15.1) | 0.990 | |
| DES Number (%) | 0 | 5 (31.3) | 15 (40.5) | |
| 15 | 6 (40) | 16 (44.4) | 0.979 | |
| 45 | 8 (50) | 13 (38.2) | 0.114 | |
| 90 | 8 (50) | 9 (25) | 0.019 | |
| OSDI score | 0 | 21.3 [14.6–31.6] | 18.3 [12.5–42.5] | |
| 15 | 17.4 [12.5–22.5] | 12.2 [6.3–25] | 0.096 | |
| 45 | 19.2 [14.7–23.4] | 8.3 [5–22.2] | 0.026 | |
| 90 | 24.1 [14–37.4] | 7.5 [4.9–16.8] | <0.001 |
| NEI-VFQ Subscale Median [IQR] | Visit Time (Days) | SOC N = 16 | Lacrimal Substitute (LS) N = 37 | p-Value of Difference between Groups over Time |
|---|---|---|---|---|
| General health-GH | 0 | 50 [25–50] | 50 [50–50] | |
| 90 | 50 [25–62.5] | 50 [50–50] | 0.186 | |
| General vision-GV | 0 | 40 [40–60] | 40 [40–60] | |
| 90 | 60 [60–80] | 80 [60–80] | <0.001 | |
| Ocular pain-OP | 0 | 81.2 [62.5–100] | 75 [62.5–87.5] | |
| 90 | 87.5 [81.2–100] | 87.5 [75–100] | 0.708 | |
| Near activity-NA | 0 | 83.3 [54.2–87.5] | 66.6 [50–83.3] | |
| 90 | 91.6 [79.2–100] | 83.3 [75–91.6] | 0.004 | |
| Distance activity-DA | 0 | 91.6 [70.8–100] | 83.3 [58.3–91.6] | |
| 90 | 95.8 [79.2–100] | 91.6 [83.3–100] | 0.443 | |
| Vision-specific social functioning-VSSF | 0 | 93.7 [87.5–100] | 100 [75–100] | |
| 90 | 100 [87.5–100] | 100 [87.5–100] | 0.347 | |
| Vision-specific mental health-VSMH | 0 | 90.6 [68.7–93.7] | 75 [56.2–93.7] | |
| 90 | 90.6 [84.4–93.7] | 87.5 [75–93.7] | 0.075 | |
| Vision-specific role dependency-VSRD | 0 | 87.5 [87.5–100] | 75 [62.5–100] | |
| 90 | 100 [87.5–100] | 100 [75–100] | 0.404 | |
| Vision-specific dependency-VSD | 0 | 100 [83.3–100] | 100 [75–100] | |
| 90 | 100 [100–100] | 100 [91.6–100] | 0.048 | |
| Driving-D | 0 | 81.2 [62.5–100] | 81.2 [56.2–100] | |
| 90 | 81.2 [75–93.7] | 87.5 [75–100] | 0.645 | |
| Colour vision-CV | 0 | 100 [100–100] | 100 [75–100] | |
| 90 | 100 [100–100] | 100 [100–100] | 0.238 | |
| Peripheral vision-PV | 0 | 100 [75–100] | 75 [50–100] | |
| 90 | 100 [75–100] | 100 [75–100] | 0.776 | |
| Total mean | 0 | 86.5 [72.5–96.6] | 75.6 [63.6–85.2] | |
| 90 | 89.4 [82.5–93] | 85.5 [79.8–92.6] | 0.030 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rossi, G.C.M.; Tinelli, C.; Milano, G.; Lanteri, S.; Ricciarelli, G.; Giannì, L.; Pasinetti, G.M.; Scudeller, L. Randomised, Single Blind, Controlled, Three-Month Clinical Trial on the Evaluation and Treatment of the Ocular Surface Damage Following Phacoemulsification. Vision 2022, 6, 42. https://0-doi-org.brum.beds.ac.uk/10.3390/vision6030042
Rossi GCM, Tinelli C, Milano G, Lanteri S, Ricciarelli G, Giannì L, Pasinetti GM, Scudeller L. Randomised, Single Blind, Controlled, Three-Month Clinical Trial on the Evaluation and Treatment of the Ocular Surface Damage Following Phacoemulsification. Vision. 2022; 6(3):42. https://0-doi-org.brum.beds.ac.uk/10.3390/vision6030042
Chicago/Turabian StyleRossi, Gemma Caterina Maria, Carmine Tinelli, Giovanni Milano, Sara Lanteri, Gabriella Ricciarelli, Laura Giannì, Gian Maria Pasinetti, and Luigia Scudeller. 2022. "Randomised, Single Blind, Controlled, Three-Month Clinical Trial on the Evaluation and Treatment of the Ocular Surface Damage Following Phacoemulsification" Vision 6, no. 3: 42. https://0-doi-org.brum.beds.ac.uk/10.3390/vision6030042