1. Introduction
Various robots have been actively used in therapy for children with Autism Spectrum Disorder (ASD) [
1,
2,
3,
4]. Since ASD characteristics include deficits in social communication and interaction [
5], robots have been used to improve the social communication skills or behaviors of children with ASD in several ways [
6,
7]. The primary role of robots for children with ASD was as a model of specific behaviors [
8], including gestures [
9] and facial expressions [
10]. In previous studies, humanoid robots, such as Robota and Kaspar, were controlled to move its head, arms, or facial expressions [
4]. Children with ASD who participated in the studies watched and imitated the robot’s behaviors. One study has even shown that children with ASD tend to interact more with robots than with humans [
11].
Another main purpose of using robots was to evaluate the severity of autistic traits [
12], provide feedback [
13], or elicit specific behaviors [
14]. In this case, the role of robots is to assist therapists. Previous studies have reported that using robots positively influenced therapy for children with ASD. In particular, using a robot easily drew the attention of children with ASD from the beginning of the session to the tenth therapy session in a study [
15]. Therapists have also reported that using robots is beneficial for children with ASD in therapies [
16]. That is, robots have played a central or supportive role in autism therapy.
However, the role of parents in robot-assisted therapy has not been highlighted. When considering that parents are often included directly or indirectly in therapies for children with ASD [
17], it is necessary to examine whether a parent influences a child’s interactions with a robot. Although parental interventions for children with ASD have been considered effective in traditional autism therapies [
18], studies exploring parents’ influence in robot-assisted therapy were rarely conducted. A study investigated the effects of parents’ presence on their children’s social or behavioral changes, such as engagement with a robot, smiles, and stereotyped behaviors in robot-assisted therapy [
19]. The presence of parents influenced their children’s behaviors towards the robot positively throughout ten sessions. In particular, children with severe impairments showed higher engagement with the robot when their parents are with them.
Different from the previous study, we examined the influence of a parent’s active involvement on a child’s engagement in robot-assisted activities. It is a prerequisite to maintain a child’s engagement with a robot to facilitate a specific behavior using a robot. Therefore, we focused on free play sessions which can be widely included in play-based autism therapy using a robot, and explored a parent’s influence on the moments of a child’s disengagement, which was defined as discontinuation of interactions with a robot. In particular, we explored the events of disengagement and parental influences on reinitiating the engagement. We observed what is happening before and during disengagement, and how the parent influences the child’s behaviors. We adopted a wearable device as a possible distractor which can cause disengagement. In addition, we observed whether unusual situations during disengagement happened or not and how the parent intervened the moments because a parent can be more influential in unexpected situations as a model of social reference.
We adopted a case study method to explore what kinds of factors should be considered for further research on parental influences during robot-assisted therapy. We video-recorded and observed a child and a parent’s case during robot-assisted activities. We explored what is happening between engagement and disengagement and summarized the events quantitatively referring to a reported method [
20]. Additionally, we closely observed the moments of disengagement during unusual situations and explored the parental influence qualitatively.
4. Results
We analyzed the annotations of the recorded videos regarding three aspects: (a) the child’s interactions with the robot, parent, or therapist, (b) the child’s behaviors when he was distracted, and (c) the parent’s interventions. The reliability of the two video annotators was high for the annotations of the three aspects. Intraclass correlation coefficient estimates and their 95% confident intervals were calculated using SPSS statistical package version 28 (SPSS Inc., Chicago, IL, USA) based on a mean-rating (k = 2), consistency, and two-way mixed-effects model. The average intraclass correlation coefficient was 0.834, with a interval from 0.751 to 0.858 (F(627, 627) = 6.01, p < 0.001).
4.1. Quantitative Description
This study focused on the child’s behaviors and his parent’s interventions when he disengaged from interactions with the robot. First, we quantitatively counted the durations and numbers of (1) the child’s interactions with the robot, (2) the child’s interactions with the therapist, (3) the child’s interactions with the parent, and (4) the child’s disengagement with the robot based on the video annotation.
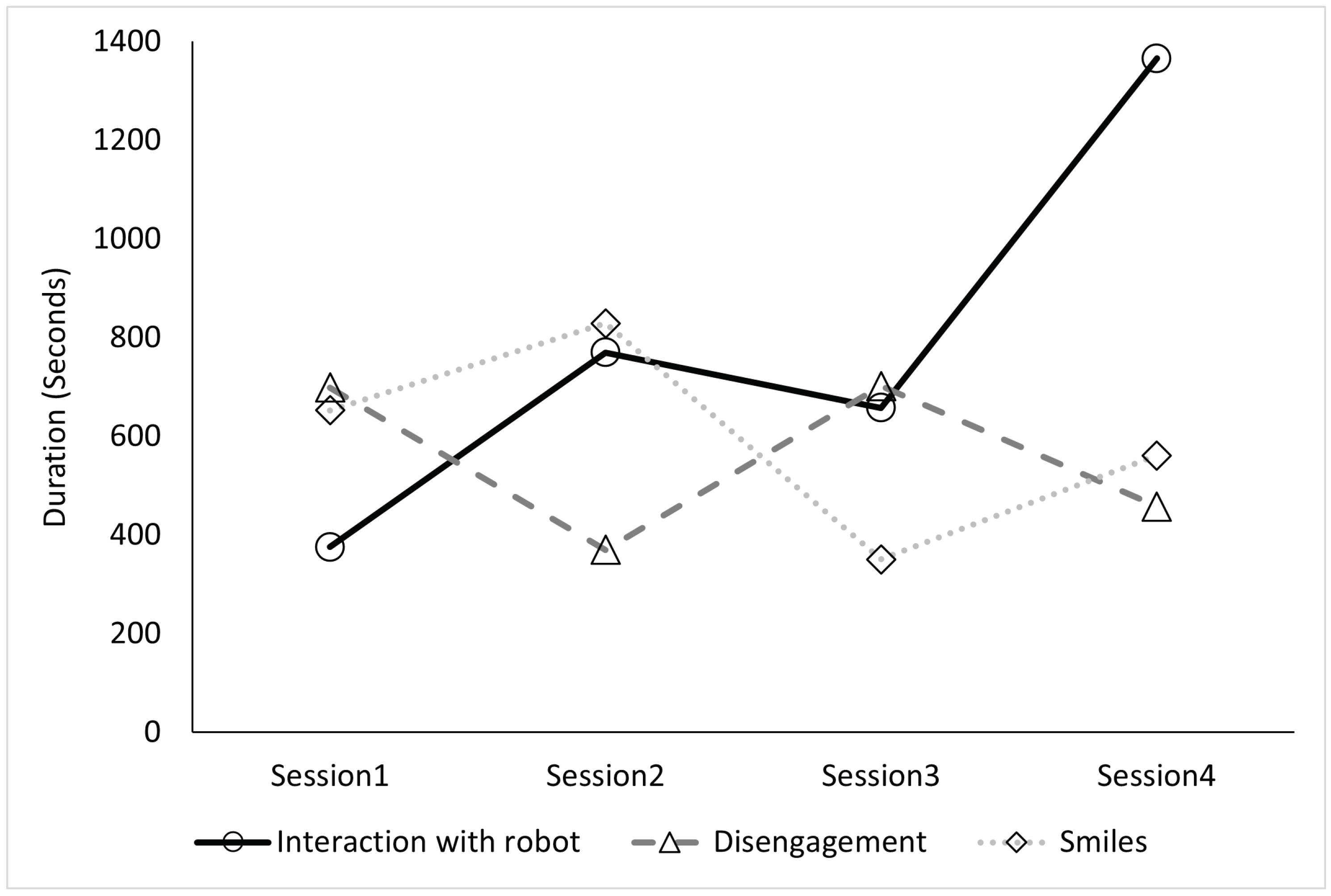
Table 1 shows the total duration and number of the child’s interactions with the robot, therapist, or parent and disengagement with the robot in each session. Moreover, it shows the total duration and the number of the child’s smiles in each session. We found that the total duration of interaction with the robot typically increased, although it decreased marginally during the third session. Notably, the total duration of interaction with the robot was the highest during the last session. The number of interactions with the robot showed the same trend as the total duration.
In contrast, the total duration and number of interactions with the therapist or parent were lower than those of the robot throughout the sessions. Moreover, the duration and number of interactions with the therapist were lower than those with the parent during the first, second, and fourth sessions. This suggests that the child played with the robot rather than interacting with people around him. When interacting with people, he interacted with his parent rather than the therapist. This indicates that the child showed a clear preference for interacting with the parent over the therapist. Therefore, the benefits of robot-assisted interventions may increase by assigning a role to a parent of children with ASD.
Regarding the interaction with the robot, we observed a trend and possible relationship with the changes in disengagement and smiles throughout the four sessions (
Figure 3,
Table 1). First, the disengagement duration showed an opposite trend to that of interactions with the robot. This result is expectable because disengagement was defined as turning away from the robot. Another noticeable point in
Table 1 is that his interaction time with the therapist or the parent was less than the disengagement time. Then, what was he doing when he was disengaged with the robot? We cover this in the next section.
Second, the duration of smiles showed the same trend as the interactions with the robot. This might be since the engagement with the robot was a fun activity that aroused smiles. However, smiles cannot explain the changes in interaction with the robot completely. The child was engaged with the robot the most during the fourth session while he smiled the most during the second session. The child may have lost interest in the robot over time but was engaged in activities with the robot. Therefore, the motivation to play with the robot can be either internal or external, such as by the parent’s directions.
4.2. Detailed Observation of Disengagement
The quantitative description indicates that the child’s interaction with the robot increased throughout the four sessions. However, the results raised questions about whether his engagement with the robot was motivated voluntarily and whether he could re-initiate the engagement by himself after disengagement. Therefore, we thoroughly observed the behaviors of the child and parent when they were not engaged in robot interaction.
Figure 4 shows a summary of the ratio of disengaged moments. We observed disengaged moments from three perspectives. The first is the child’s focus before disengagement with the robot. The second is the behavior that occurred during disengagement. The third is whether intervention by the parent occurred. The disengaged moments throughout the four sessions were observed 61 times (24 times in the first session, 8 in the second session, 14 in the third session, and 15 in the fourth session).
4.2.1. Situation before Disengagement
The most frequent situation that preceded the 61 instances of disengagement with the robot was that the child was interacting with the robot. In these cases, the child abruptly discontinued the interaction with the robot, even though the robot was controlled to show the child various movements, such as standing up, sitting down, showing gestures, or throwing a ball to retain his attention. This may imply that the activities or interactions with the robot were insufficient to maintain the child’s engagement.
The second occurrence of most disengagements was when the wearable device or other devices in the therapy room distracted the child from the robot. 52% of the instances of the child being distracted by devices were due to the wearable device, and 45% involved the child being distracted by the therapist’s camera. When the wearable device was not fixed well on his face, the child was distracted and disengaged from the robot. Although the device was adjustable and adjusted well before starting the play sessions, his movements, including running and jumping, disturbed the device adjustment from the correct position on his face. Moreover, the child often touched and tried detaching the wearable device during the play sessions, although he accepted the device during preparation time. His touch made the wearable device unstable on his face, leading his attention to the device rather than the robot, thereby, leading to disengagement with the robot. Another device that distracted the child was a laptop monitoring the EMG recordings. This case occurred just once, but it suggests that various devices used for the play sessions might distract children and cause them to have trouble focusing on the robot.
4.2.2. Behaviors during Disengagement
The annotation of the disengaged moments was based on the definition of engagement and disengagement in this study (
Table 2). In particular, we observed stereotypic behaviors in the child, unrelated talks, and looking at objects other than the robot during the moments of disengagement. The difference between unrelated talks and stereotypic verbal behaviors in this study was repetition and the length of utterance. When he mentioned repetitive and inappropriate words, we counted them as stereotypic behaviors. In contrast, we counted the behaviour as ‘unrelated talks’ when he uttered a series of sentences discussing a topic that was unrelated to the situation.
Of the observed behaviors during the disengagement, 88% (54 out of the 61 instances of disengagement from the robot) were due to stereotypic verbal or motor behaviors. After he was distracted by the environment or discontinued his interactions with the robot, he repeatedly showed the same behavioral patterns. Additionally, he repeatedly said the exact words or words of the same category. Various stereotypic behaviors occurred concurrently. A common pattern was standing up suddenly and walking or running around. This pattern was observed 33 times out of the 54 stereotypic behaviors. In addition to the behaviors of abrupt standing up and walking or running around, the child suddenly sang a song eight times or shouted twice. The central verbal stereotypic behavior was related to food and transportation. He suddenly mentioned food names seven times or mentioned train names twice. The most severe stereotypic behaviors were suddenly standing up, jumping, and running around while talking about specific words. It was observed twice right after he discontinued the interactions with the robot in both cases.
A total of 7% of instances of disengagement were the child looking at a person or objects other than the robot. This included the therapist, the therapist’s camera, the wearable device, and his own legs. The remaining 5% were the child performing ‘unrelated talks’—speaking about something unrelated to his current situation. He abruptly talked about a person who was not present in the room, the upcoming weather, and the room temperature.
4.2.3. Parent’s Intervention
When the child was not engaged with the robot, 84% (51 out of the 61 instances of disengagement from the robot) was intervened by his parent. Various types of interventions were observed simultaneously or consecutively by the parent. The parent’s intervention included showing him how to interact with the robot and taking the child near the robot physically. The types of parent intervention in order of frequency are as follows (The number in parentheses indicates frequency): talking about the robot to the child (15), holding or blocking the child when he tried to escape from the play area (10), calling the child (9), suggesting an activity to the child with the robot (9), pointing at the robot (7), showing gestures (5), complementing the child (4), taking the child to the robot (4), complementing the robot (2), saying “Look at the robot” to the child (2), saying “No” to the child (2), stroking the robot’s head (2), touching the robot (2), showing a mark “X” with crossed arms or fingers to the child (1), and saying “Help the robot” to the child when the robot fell (1).
After the intervention, 80% (41 out of the 51 instances of the parent’s intervention) was returning to the robot. When he did not return to the robot immediately after receiving the parent’s intervention, the parent’s next intervention was a combination of talking about the robot to the child, calling the child, complementing the child, and talking to the robot.
A noticeable pattern from the child was that he did not look at the parent’s face while the parent provided an intervention. However, we observed that he returned to the robot and imitated the parent’s behaviors or sayings in 9 out of 41 cases. The frequency of imitated behaviors was as follows (The number in parentheses indicates frequency.): touching the robot (2), stroking the robot’s head (1), and singing (1). The child also repeated what the parent had said to them to the robot. The frequency of these repeated phrases was: “You are good” (1), “Are you okay?” (1), “Help the robot” (1), “Let’s play again” (1), and “Thank you” (1).
We observed that he imitated or repeated his mother, but he did not directly look at the parent’s face. Avoiding direct gaze during social interactions is one of the autistic characteristics [
5]. Therefore, it is noticeable that the vocal, verbal, or gestural feedback was imitated by the child. It may suggest that parents can guide a child with ASD to engage with the robot by providing more effective feedback.
4.3. Qualitative Description in Unexpected Situations
We observed that more than half of the disengagement happened while the child was interacting with the robot. Therefore, we closely observed the moments of disengagement and the parent’s influence, particularly in unexpected situations with the robot. As social referencing behaviors might occur during unexpected situations, we explored if the behaviors occur from the child with ASD and how the parent influence the behaviors.
During the first session, when the child was holding a hand of the robot and the robot was walking, the robot suddenly fell down. The child looked surprised, and turned away from the robot. His mother quickly supported the falling robot, and said “Sorry” to the robot. The child was looking at the situation while keeping distant. The mother showed a gesture to urge him to come to the robot. The child approached the robot a little, but turned away from the robot with a frown on his face. His mother said “It’s okay. Come here.” Then, the child smiled and approached the robot and stroked the robot’s head. He moved back a little bit and said, “Are you ok?” to the robot.
During the second session, when the child was touching the arm of the robot and the robot was moving arms, the robot suddenly stopped and fell down. His mother said, “Ohhhhh” while looking at the falling robot with an anxious face. The child turned away from the robot and went far away from the robot. The mother made the robot stand up, and showed a gesture to urge him to come to the robot. The child was just looking at the robot while smiling. His mother said, “Stroke the robot’s head.” Then, the child approached the robot and stroked the robot’s head, while saying “Are you ok?” to the robot.
During the third session, when the child was touching the fingers of the robot, the robot tried to stand up, but the robot fell down. The child immediately said, “Are you ok?” to the robot and shook the fallen robot. His mother said, “Save the robot.” to the child, and the child made the robot stand up while saying “I will save the robot.” The robot fell down again, and his mother said with a serious face, “Are you ok?” to the robot. The child also said, “Are you ok?” to the robot. However, the child suddenly stood up and jumped while smiling and saying “Robot, robot, small child.” His mother said “Are you ok?” to the robot again with a serious face. The child approached the robot, and said “Are you ok?” to the robot.
During the fourth session, when the child was holding a hand of the robot and the robot was walking, the robot suddenly fell down. His mother pointed out the fallen robot with an anxious face. The child approached the robot, and said “Are you ok?” to the robot. Then, the robot tried to stand up, but it stopped. The child said “Are you ok?” to the robot immediately, and pretended to cry.
His mother consistently tried to teach him how to behave in unexpected situations. Her facial expressions were either worried or serious, and she never smiled in the situations. She tried to make the child say considerate expressions and help the robot. Although the child did not refer to the mother’s facial expressions and he even smiled and jumped during the third session, his mother’s verbal expressions were effective to make him follow directions or imitated the expressions. During the final session, he immediately approached the robot and said “Are you ok?” in the expected situation without his mother’s intervention. The consistent verbal feedback by the mother may have encouraged the child to say the same verbal expressions in a similar situation.
5. Discussion
We explored parental influences and related factors to be considered, including stereotypic behaviors, distracting devices, unusual situations, and social referencing, from a case for further research on robot-assisted therapy. We examined the parental influence on a child’s engagement in robot-assisted activities. In particular, we observed what is happening before and during disengagement. In the child’s case, we attempted to identify the events which facilitated the continuation of engagement with the robot and the parent’s involvement.
First, we observed a trend of interactions between the child and robot throughout the four sessions. The total duration and number of interactions with the robot showed an overall increase. During the last session, the child showed the most extended interactions with the robot and the shortest with the therapist. Since the prerequisite of robot-assisted therapy is engagement in interactions or activities with the robot, the child showed a favorable response to robot-assisted therapy; the child interacted with the robot rather than with his parent or the therapist. However, the smiles decreased during the third and fourth sessions compared to the first and second sessions. Although smiles are expressions with various inner statuses, when considering smiles as an indicator of positive emotions or feelings, the child may have interacted with the robot involuntarily to perform a task during the third and fourth sessions.
Second, we found 61 disengaged moments and observed the child during these moments to establish what motivated him to re-initiate the interaction with the robot. When we observed what happened or the child’s action before disengagement with the robot, we observed that 54% of these disengagements were sudden; the child stopped interacting abruptly with the robot. This suggests that the robot interactions might not be sufficient for engaging the child to continue. In this study, we solely controlled the robot’s body and created movements. The robot did not talk or make sounds. Therefore, the child interacted with the robot while only receiving visual and tactile stimuli. The robot’s limited actions may have resulted in abrupt discontinuation of the interactions. However, 44% of the distractions were caused by multiple devices, including the wearable device, the therapist’s camera and the laptop monitoring the EMG recording of the wearable device. Specifically, he often touched the wearable device or tried to detach it, although he showed no resistance during the preparation of each session. This suggests that we need to consider the acceptance of a wearable device for extended periods. Moreover, the number of devices that will be used and exposed to a child with ASD during therapy should be considered. If the devices are the primary source of distraction, this might negate the positive effects of using them.
Third, we observed the child’s behavior during disengagement and intervention by the parent. Of the observed behaviors, 88% were stereotypic verbal or motor behaviors considered inappropriate and repetitive. The most common behavioral patterns were suddenly standing up, walking around, or running around. He also spoke repeatedly of specific food or car names when not engaged with the robot. This suggests that these symptoms of ASD may have been soothed while interacting with the robot. In contrast, the symptoms of ASD were prominent when the child was not engaging with the robot. Another explanation could be that focusing on a target, whether a robot or otherwise, can make the child’s symptoms less prominent. In 84% of cases, the parent provided intervention during these moments. The parent provided various types of interventions simultaneously or one by one. The most frequent intervention was talking about the robot, to the robot or calling the child. However, the types of intervention did not always make the child return to the robot. When the child did not interact with the robot after the verbal intervention, the parent attempted physical interventions, such as holding or blocking the child when he tried to escape from the play area. This shows that engaging the child with the robot is not straightforward. It was necessary to stop violent, repetitive stereotyped behavior and call the child’s attention to the robot.
Fourth, the child’s chances of interaction with the robot increased by 80% after receiving the parent’s intervention. Notably, he also imitated the parent’s behaviors or words in 9 of 41 cases. All imitated behaviors were related to hand movements and vocal behaviors. He imitated the parent’s behavior or words appropriate in the situation. As with previous research results [
36,
37], he had limited eye contact with people around him and did not look at the parent’s face directly while receiving the parent’s feedback during his disengagement. This shows that he could refer to the parent’s responses when the feedback involved voice or hand movements, but not facial expressions. The qualitative description particularly shows that the child re-initiated the interactions with the robot by referring to his mother’s verbal reactions in an unusual situation where the robot suddenly stopped or fell. Although social referencing in children with ASD has been reported limited, this study indicated that the parent facilitated a specific behavior of the child in unexpected situations and played a role as a social referencing. In addition, it should be noted that the dynamics among the child, the robot and the parent can be intentionally adopted for future robot-assisted therapy to facilitate an appropriate behavior in a social context.
Although this study made some notable observations during robot-assisted activities, this case study has limitations. This research is based on a case of a child with ASD and his mother. The child was diagnosed with a moderate level of symptoms, but the details of his conditions, such as details of comorbid conditions, were not disclosed when we recruited the participant through the Institute for Developmental Research. In addition, the influence of a parent might be different depending on the parent’s personality or relationship with the child. However, we did not include their interactions outside of the research settings. Moreover, we focused on the quantitative analysis of their behaviors. Another limitation is that the therapy included only play sessions and that did not target specific behavioral changes. Therefore, the depth of analyzing this case has limitations.
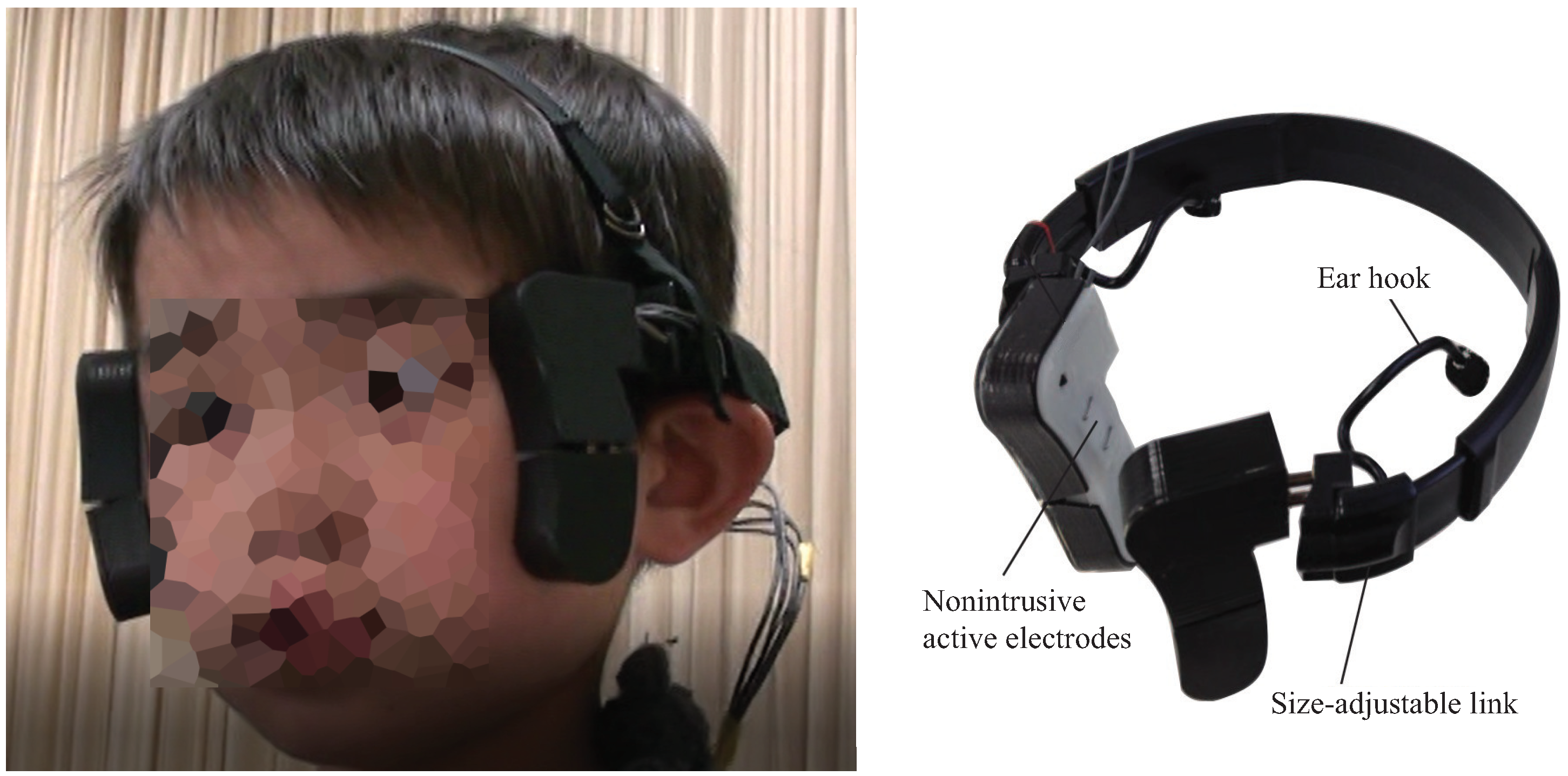
There are also limitations with the wearable device which was used in this study. There is a possibility that the device was not enough comfortable for using it throughout a session, which was around 20 min. The participant might have been bothered by the wearable device made of plastics on his face and head. If the device had a softer material and it was a smaller size covering the face and head minimally, different results might have been obtained. Otherwise, it is also possible that the child had high sensory sensitivities related to symptoms of ASD. It was challenging to apply a wearable device that satisfies an individual’s comfortableness. Therefore, it should be noted that this case might be extreme to show the negative influences of the wearable device.
However, this study provides critical insights for future research. First, the effects of parents’ intervention should be considered for maintaining engagement with a robot for autism therapy; parental intervention may increase the benefits of robot-assisted therapy. In addition, future research should consider what kinds of feedback from a parent will be more effective. Second, the child was distracted by not only the wearable device but also a video camera and a laptop. This suggests that the use of multiple technologies should be carefully considered to take full advantage of using either robots or wearable devices. Third, social referencing of a child with ASD can be considered during robot-assisted therapy involving parental participation. It is important for children to learn how to behave in an unfamiliar situation. Therefore, the new role of a robot and a parent, such as a robot assisting a parent, needs to be considered to create a therapeutic setting for social referencing.
The limitations of this study should be addressed by future research. Future studies must collect more extensive data from broader populations with ASD. Moreover, the personalities of parents or relationships between a child and a parent need to be considered. The timing, way, or purpose of parental involvement also should be further investigated. Additionally, future research will cover the effects of parent involvement in robot-assisted therapy for improving a specific social or interpersonal behavior of children with ASD.









{kind=link}
{kind=link}
{kind=link}
{kind=link}