
Design Considerations for Immersive Virtual Reality Applications for Older Adults: A Scoping Review

 ,
,
Abstract
:1. Introduction
- What are the design considerations that guide the design and development of immersive VR systems for older adults?
- What characterizes the design processes followed to develop iVR systems specific for older adults?
- How to evaluate the user experience of immersive VR for older adults, and what type of studies and methods are used for evaluation?
- What are the reported usability challenges of immersive VR systems for older adults?
2. Background
2.1. Older Adults’ Acceptance of iVR Technology
2.2. Technology Design with and for Older Adults
2.3. User Experience of iVR for Older Adults
3. Method
3.1. Scoping Review Protocol
3.2. Selection Criteria
- Papers presenting systems that were specifically designed for or evaluated with older adults (65 years old or over), with recent HMDs (introduced after 2010) covering any range of physical and cognitive capabilities.
- Papers that involve mixed user groups of young and older adults with the intention to capture any specific measures tailored for the older adult user group.
- Papers in which the systems were designed for or evaluated with a general population of various age groups.
- Papers that report the use of HMD models developed prior to 2010 and mixed reality HMDs.
- Papers that use non-HMD VR setups, such as CAVE systems, were excluded because we were interested to understand characteristics of research in HMD-based setups.
- Review papers, perspective, or opinion papers.
- Literature on the effectiveness of VR health interventions that focused on primary or secondary intervention outcomes, sustainability, and intervention adherence, without examining the impact of VR.
- Papers without evaluation and reporting of results, such as demo papers or studies that focused on just the design phase.
- Papers that were published in languages other than English.
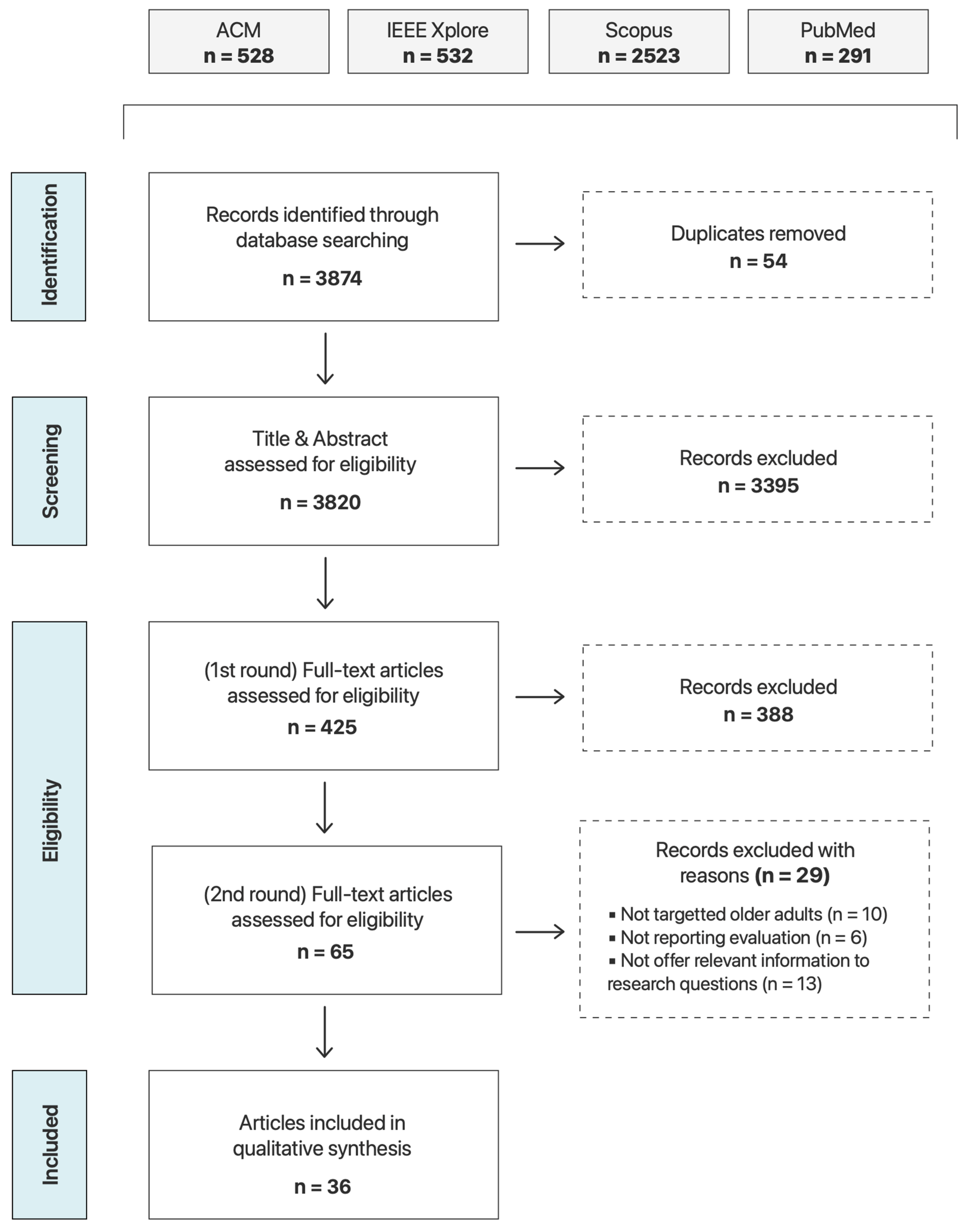
3.3. Study Selection
3.4. Evaluation
4. Results
4.1. Overview
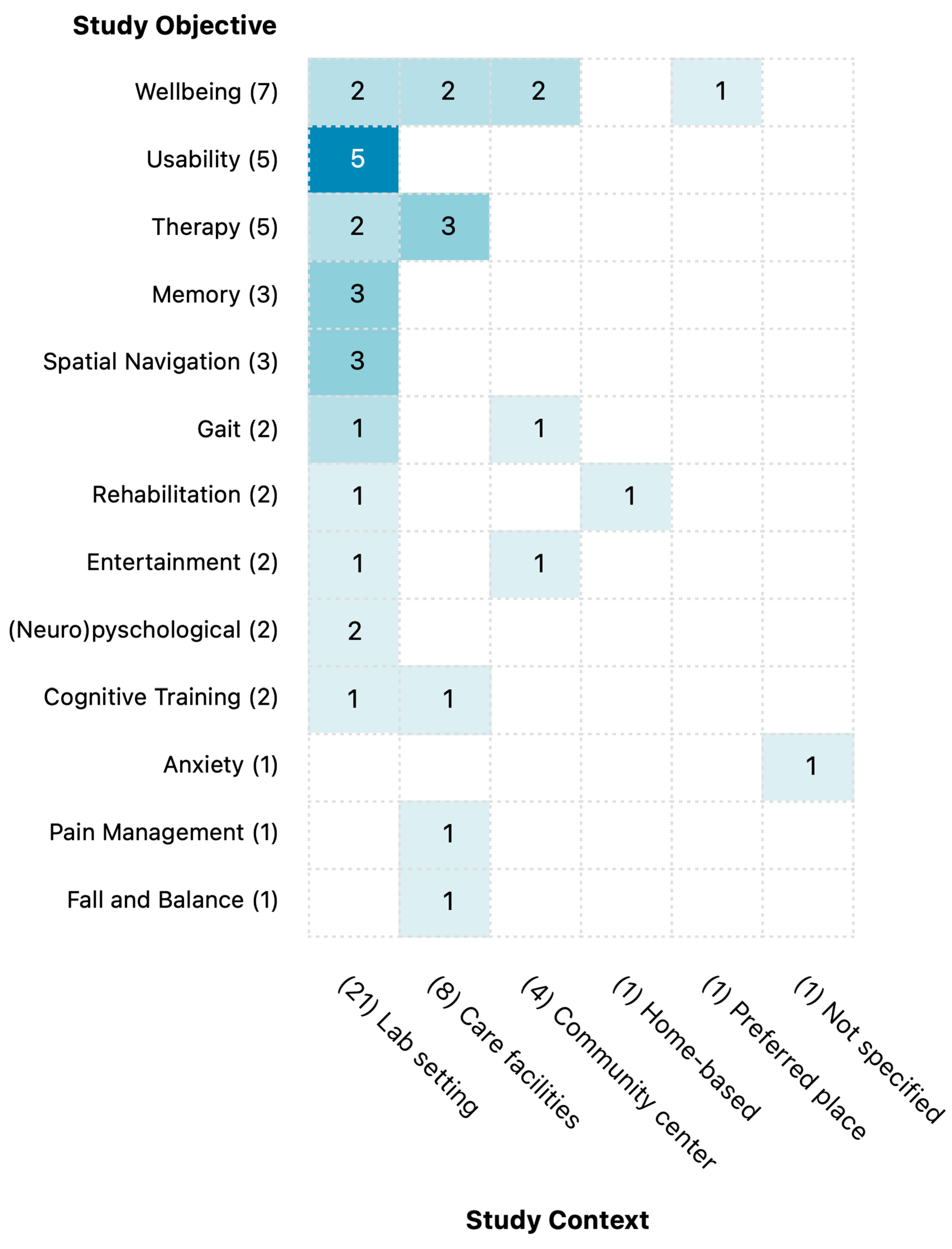
4.1.1. Study Objective and Context
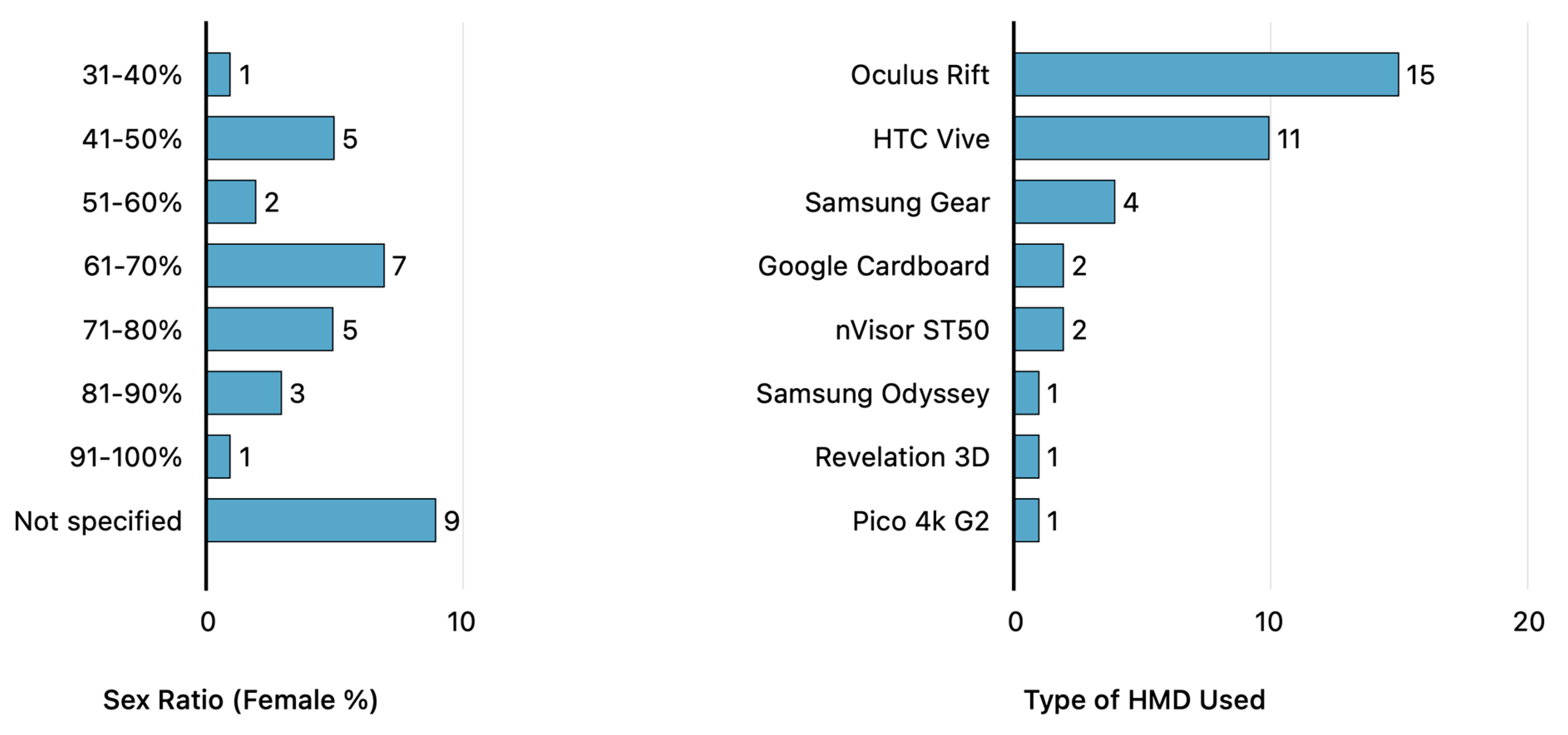
4.1.2. Study Participants
4.1.3. HMD Type
4.1.4. Application Content
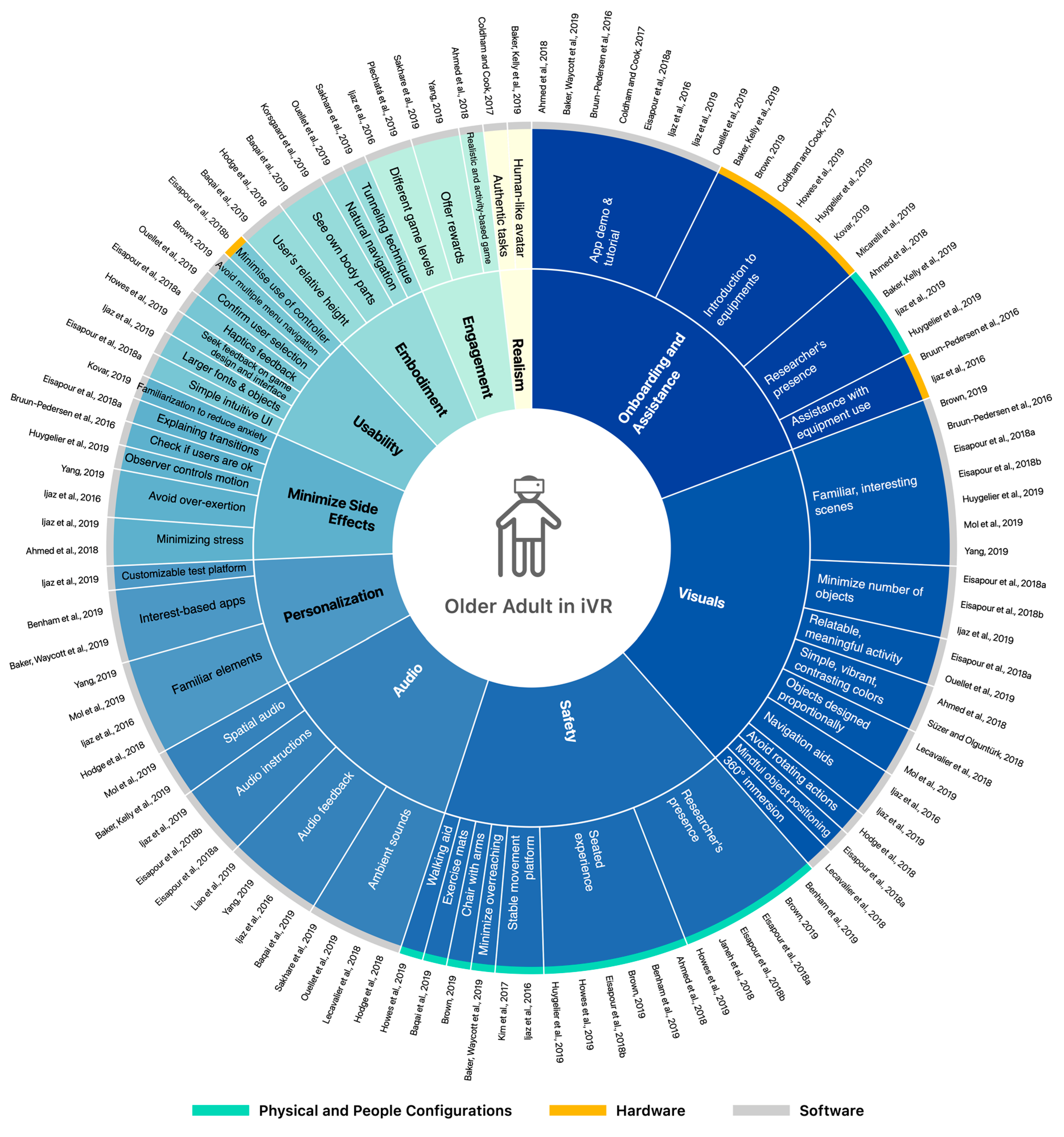
4.2. Design Considerations
4.2.1. Onboarding and Assistance
4.2.2. Safety
4.2.3. Embodiment
4.2.4. Visuals
4.2.5. Audio
4.2.6. Realism
4.2.7. Personalization
4.2.8. Usability
4.2.9. Engagement
4.2.10. Minimize Side Effects
4.3. Design Process
4.4. Evaluation
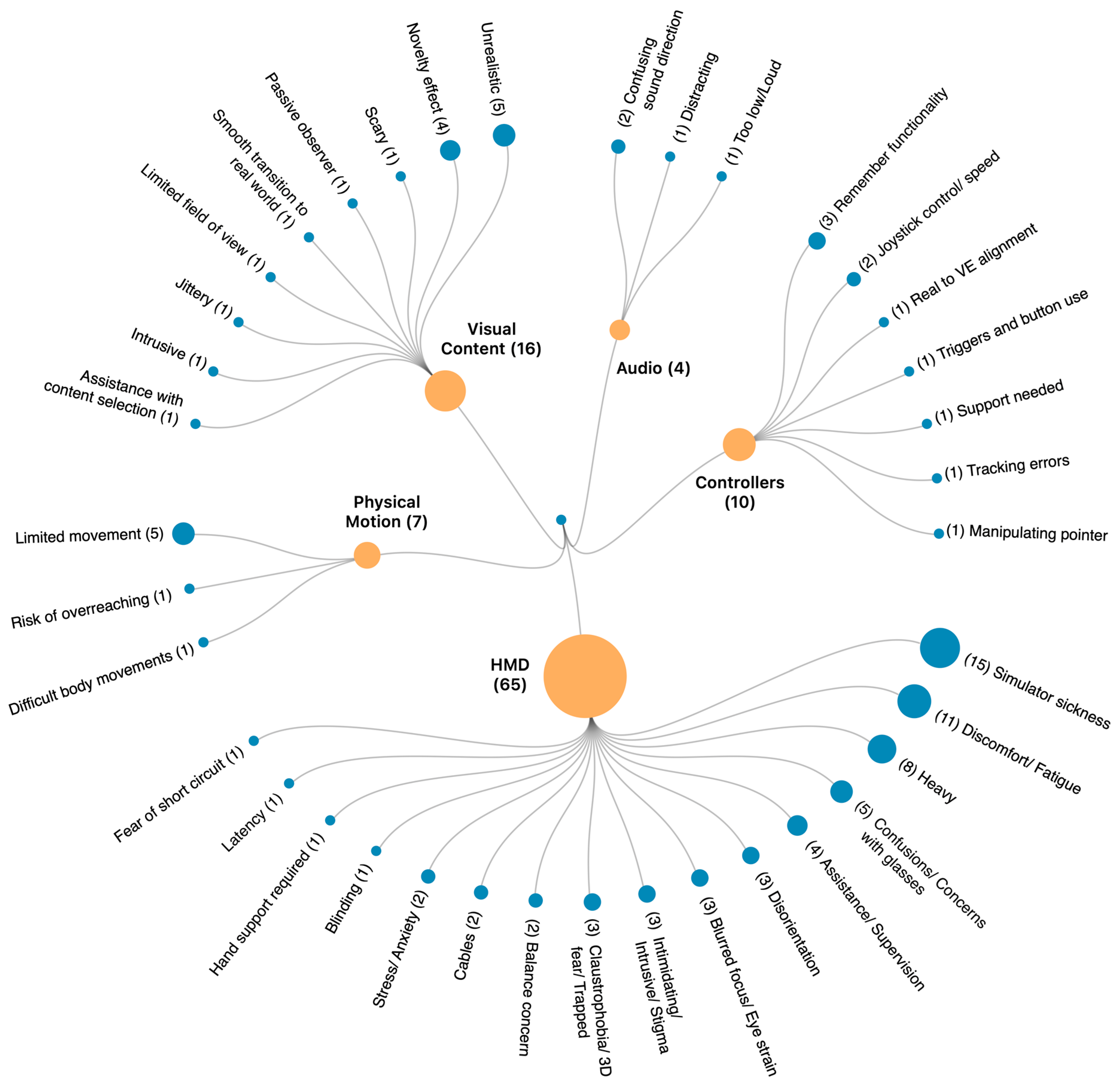
4.5. Reported Usability Challenges
4.6. Summary
5. Discussion
5.1. Design Considerations
5.1.1. Tension between “Familiar” vs. “New” experiences
5.1.2. Transition between Virtual to Real World
5.1.3. Active vs. Passive User Participation in Immersive Experiences
5.2. Design Process
5.3. Evaluation
5.4. Usability Challenges
5.5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations. World Population Ageing 2019. In Economic and Social Affairs, Population Division; United Nations: New York, NY, USA, 2019. [Google Scholar]
- A Andrews, J.; Brown, L.J.; Hawley, M.S.; Astell, A.J. Older Adults’ Perspectives on Using Digital Technology to Maintain Good Mental Health: Interactive Group Study. J. Med. Internet Res. 2019, 21, e11694. [Google Scholar] [CrossRef] [PubMed]
- Peek, S.T.; Luijkx, K.G.; Rijnaard, M.D.; Nieboer, M.E.; van der Voort, C.S.; Aarts, S.; van Hoof, J.; Vrijhoef, H.J.; Wouters, E.J. Older Adults’ Reasons for Using Technology while Aging in Place. Gerontology 2015, 62, 226–237. [Google Scholar] [CrossRef] [PubMed]
- Mujber, T.; Szecsi, T.; Hashmi, M. Virtual reality applications in manufacturing process simulation. J. Mater. Process. Technol. 2004, 155, 1834–1838. [Google Scholar] [CrossRef]
- Slater, M. Immersion and the illusion of presence in virtual reality. Br. J. Psychol. 2018, 109, 431–433. [Google Scholar] [CrossRef] [PubMed]
- Eisapour, M.; Cao, S.; Domenicucci, L.; Boger, J. Participatory Design of a Virtual Reality Exercise for People with Mild Cognitive Impairment. In Proceedings of the Conference on Human Factors in Computing Systems, 2018a. Montreal, QC, Canada, 25–27 April 2018; p. CS15. [Google Scholar] [CrossRef] [Green Version]
- Slater, M.; Lotto, B.; Arnold, M.M.; Sanchez-Vives, M.V. How we experience immersive virtual environments: The concept of presence and its measurement. Anu. Psicol. 2009, 40, 193–210. [Google Scholar]
- Tuena, C.; Pedroli, E.; Trimarchi, P.D.; Gallucci, A.; Chiappini, M.; Goulene, K.; Gaggioli, A.; Riva, G.; Lattanzio, F.; Giunco, F.; et al. Usability Issues of Clinical and Research Applications of Virtual Reality in Older People: A Systematic Review. Front. Hum. Neurosci. 2020, 14, 93. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.M.; Rhiu, I.; Yun, M.H. A Systematic Review of a Virtual Reality System from the Perspective of User Experience. Int. J. Hum.-Comput. Interact. 2019, 36, 893–910. [Google Scholar] [CrossRef]
- Silva, R.S.; Mol, A.M.; Ishitani, L. Virtual reality for older users: A systematic literature review. Int. J. Virtual Real. 2019, 19, 11–25. [Google Scholar] [CrossRef]
- Thach, K.S.; Lederman, R.; Waycott, J. How older adults respond to the use of Virtual Reality for enrichment: A systematic review. In Proceedings of the 32nd Australian Conference on Human-Computer Interaction, Sydney, Australia, 2–4 December 2020. [Google Scholar] [CrossRef]
- Abeele, V.V.; Schraepen, B.; Huygelier, H.; Gillebert, C.; Gerling, K.; Van Ee, R. Immersive Virtual Reality for Older Adults: Emperically Grounded Design Guidelines. ACM Trans. Access. Comput. 2021, 14, 1–30. [Google Scholar] [CrossRef]
- Murman, D.L. The Impact of Age on Cognition. Semin. Heart 2015, 36, 111–121. [Google Scholar] [CrossRef]
- McGrath, R.P.; Ottenbacher, K.J.; Vincent, B.; Kraemer, W.J.; Peterson, M. Muscle weakness and functional limitations in an ethnically diverse sample of older adults. Ethn. Health 2017, 25, 342–353. [Google Scholar] [CrossRef] [PubMed]
- Lim, K.; Ec, B.; Stat, M.; ATaylor, L. Factors associated with physical activity among older people—A population-based study. Prev. Med. 2005, 40, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Webber, M.S.C.; Porter, M.M.; Menec, V.H. Mobility in Older Adults: A Comprehensive Framework. Gerontology 2010, 50, 443–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmadpour, N.; Keirnan, A. Design for Ageing-in-place: Evidence from Australia. In DRS2016: Future-Focused Thinking; Lloyd, P., Bohemia, E., Eds.; Design Research Society: London, UK, 2016; Volume 4. [Google Scholar]
- Mynatt, E.D.; Rogers, W.A. Developing technology to support the functional independence of older adults. Ageing Int. 2001, 27, 24–41. [Google Scholar] [CrossRef]
- Khosravi, P.; Rezvani, A.; Wiewiora, A. The impact of technology on older adults’ social isolation. Comput. Hum. Behav. 2016, 63, 594–603. [Google Scholar] [CrossRef]
- Charness, N.; Boot, W.R. Aging and Information Technology Use: Potential and Barriers. Curr. Dir. Psychol. Sci. 2009, 18, 253–258. [Google Scholar] [CrossRef]
- Liao, Y.-Y.; Chen, I.-H.; Lin, Y.-J.; Chen, Y.; Hsu, W.-C. Effects of Virtual Reality-Based Physical and Cognitive Training on Executive Function and Dual-Task Gait Performance in Older Adults With Mild Cognitive Impairment: A Randomized Control Trial. Front. Aging Neurosci. 2019, 11, 162. [Google Scholar] [CrossRef] [Green Version]
- Eisapour, M.; Cao, S.; Domenicucci, L.; Boger, J. Virtual Reality Exergames for People Living with Dementia Based on Exercise Therapy Best Practices. Proc. Hum. Factors Ergon. Soc. Annu. Meet. 2018b, 62, 528–532. [Google Scholar] [CrossRef]
- Goh, L.; E Allen, N.; Ahmadpour, N.; Martens, K.A.E.; Song, J.; Clemson, L.; Lewis, S.J.G.; MacDougall, H.G.; Canning, C.G. A Video Self-Modeling Intervention Using Virtual Reality Plus Physical Practice for Freezing of Gait in Parkinson Disease: Feasibility and Acceptability Study. JMIR Form. Res. 2021, 5, e28315. [Google Scholar] [CrossRef]
- Baker, S.; Kelly, R.M.; Waycott, J.; Carrasco, R.; Hoang, T.; Batchelor, F.; Ozanne, E.; Dow, B.; Warburton, J.; Vetere, F. Interrogating Social Virtual Reality as a Communication Medium for Older Adults. Proc. ACM Hum.-Comput. Interact. 2019, 3, 1–24. [Google Scholar] [CrossRef] [Green Version]
- Hodge, J.; Balaam, M.; Hastings, S.; Morrissey, K. Exploring the Design of Tailored Virtual Reality Experiences for People with Dementia. In Proceedings of the Conference on Human Factors in Computing Systems, Montreal, QC, Canada, 1–13 April 2018; p. 514. [Google Scholar] [CrossRef] [Green Version]
- Ijaz, K.; Wang, Y.; Milne, D.; Calvo, R.A. Competitive vs Affiliative Design of Immersive VR Exergames. In Lecture Notes in Computer Science (Including Subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics); Springer: Berlin/Heidelberg, Germany, 2016; Volume 9894, pp. 140–150. [Google Scholar] [CrossRef]
- Lai, X.; Lei, X.; Chen, X.; Rau, P.-L.P. Can Virtual Reality Satisfy Entertainment Needs of the Elderly? The Application of a VR Headset in Elderly Care. In Lecture Notes in Computer Science (Including Subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics); Springer: Berlin/Heidelberg, Germany, 2019; pp. 159–172. [Google Scholar] [CrossRef]
- O’Regan, J.K.; Noë, A. A sensorimotor account of vision and visual consciousness. Behav. Brain Sci. 2001, 24, 939–973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andringa, G.; Nuijten, P.L.; Macville, M.M.; Mertens, E.G.A.; Kaptein, J.J.; Bauer, A.C.M.; Doel, L.R.V.D.; Roos, A.G. Feasibility of Virtual Reality in Elderly with Dementia; Springer: Cham, Switzerland, 2019; pp. 146–149. [Google Scholar] [CrossRef]
- Brown, J.A. An Exploration of Virtual Reality Use and Application Among Older Adult Populations. Gerontol. Geriatr. Med. 2019, 5. [Google Scholar] [CrossRef] [PubMed]
- Coldham, G.; Cook, D.M. VR usability from elderly cohorts: Preparatory challenges in overcoming technology rejection. In Proceedings of the 2017 National Information Technology Conference (NITC), Colombo, Sri Lanka, 13–15 September 2017; pp. 131–135. [Google Scholar] [CrossRef]
- Huygelier, H.; Schraepen, B.; Van Ee, R.; Abeele, V.V.; Gillebert, C.R. Acceptance of immersive head-mounted virtual reality in older adults. Sci. Rep. 2019, 9, 4519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, A.R.; De Schutter, B.; Franks, K.; Radina, M.E. Older Adults’ Experiences with Audiovisual Virtual Reality: Perceived Usefulness and Other Factors Influencing Technology Acceptance. Clin. Gerontol. 2018, 42, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Czaja, S.J.; Boot, W.R.; Charness, N.; Rogers, W.A. Designing for Older Adults: Principles and Creative Human Factors Approaches; CRC Press: Boca Raton, FL, USA, 2019. [Google Scholar] [CrossRef]
- Farage, M.A.; Miller, K.W.; Ajayi, F.; Hutchins, D. Design Principles to Accommodate Older Adults. Glob. J. Health Sci. 2012, 4, 2–25. [Google Scholar] [CrossRef] [Green Version]
- Johnson, J.; Finn, K. Designing User Interfaces for an Aging Population: Towards Universal Design; Morgan Kaufmann Publishers: Burlington, MA, USA, 2019. [Google Scholar]
- Kurniawan, S.; Zaphiris, P. Research-derived web design guidelines for older people. In Proceedings of the 7th International ACM SIGACCESS Conference on Computers and Accessibility, Baltimore, MD, USA, 9–12 October 2005; pp. 129–135. [Google Scholar] [CrossRef]
- Knowles, B.; Hanson, V.L.; Rogers, Y.; Piper, A.M.; Waycott, J.; Davies, N. HCI and Aging: Beyond Accessibility. In Proceedings of the Extended Abstracts of the 2019 CHI Conference on Human Factors in Computing Systems, Glasgow, Scotland, 4–9 May 2019; pp. 1–8. [Google Scholar]
- Lindsay, S.; Jackson, D.; Schofield, G.; Olivier, P. Engaging older people using participatory design. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Austin, TX, USA, 5–10 May 2012; pp. 1199–1208. [Google Scholar]
- Lazar, A.; Edasis, C.; Piper, A.M. A Critical Lens on Dementia and Design in HCI. In Proceedings of the 2017 CHI Conference on Human Factors in Computing Systems, Denver, CO, USA, 6–11 May 2017; pp. 2175–2188. [Google Scholar] [CrossRef] [Green Version]
- Coleman, G.W.; Gibson, L.; Hanson, V.L.; Bobrowicz, A.; McKay, A. Engaging the disengaged: How do we design technology for digitally excluded older adults? In Proceedings of the 8th ACM Conference on Designing Interactive Systems, Aarhus, Denmark, 16–20 August 2010; pp. 175–178. [Google Scholar]
- Newell, A.; Arnott, J.; Carmichael, A.; Morgan, M. Methodologies for involving older adults in the design process. In Proceedings of the International Conference on Universal Access in Human-Computer Interaction, Beijing, China, 22–27 July 2007; pp. 982–989. [Google Scholar]
- Forlizzi, J.; Battarbee, K. Understanding experience in interactive systems. In Proceedings of the 5th Conference on Designing Interactive Systems: Processes, Practices, Methods, and Techniques, Cambridge, MA, USA, 1–4 August 2004; pp. 261–268. [Google Scholar] [CrossRef]
- ISO DIS, 9241-210; Ergonomics of Human System Interaction—Part 210: Human-Centred Design for Interactive Systems. Ergonomics of human-system interaction: New York, NY, USA, 2010.
- Hassenzahl, M. The Thing and I: Understanding the Relationship Between User and Product. In Funology: From Usability to Enjoyment; Kluwer Academic Publishers: Dordrecht, The Netherlands, 2003; pp. 31–42. [Google Scholar] [CrossRef]
- Tcha-Tokey, K.; Christmann, O.; Loup-Escande, E.; Loup, G.; Richir, S. Towards a model of user experience in im-mersive virtual environments. Adv. Hum.-Comput. Interact. 2018, 2018, 7827286. [Google Scholar] [CrossRef]
- Hassenzahl, M.; Tractinsky, N. User experience—A research agenda. Behav. Inf. Technol. 2006, 25, 91–97. [Google Scholar] [CrossRef]
- Stanney, K.M.; Mollaghasemi, M.; Reeves, L.; Breaux, R.; Graeber, D.A. Usability engineering of virtual environ-ments (VEs): Identifying multiple criteria that drive effective VE system design. Int. J. Hum.-Comput. Stud. 2003, 58, 447–481. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Amin, A.M.; Tong, X.; Gromala, D.; Shaw, C.D. Cardboard Mobile Virtual Reality as an Approach for Pain Distraction in Clinical Settings. In Proceedings of the 2017 CHI Conference Extended Abstracts on Human Factors in Computing Systems—CHI EA ’2017, Denver, CO, USA, 6–11 May 2017; pp. 2345–2351. [Google Scholar] [CrossRef]
- Baker, S.; Waycott, J.; Robertson, E.; Carrasco, R.; Neves, B.B.; Hampson, R.; Vetere, F. Evaluating the use of interactive virtual reality technology with older adults living in residential aged care. Inf. Process. Manag. 2019, 57, 102105. [Google Scholar] [CrossRef]
- Kim, A.; Darakjian, N.; Finley, J.M. Walking in fully immersive virtual environments: An evaluation of potential adverse effects in older adults and individuals with Parkinson’s disease. J. Neuroeng. Rehabil. 2017, 14, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ouellet, E.; Boller, B.; Corriveau-Lecavalier, N.; Cloutier, S.; Belleville, S. The Virtual Shop: A new immersive virtual reality environment and scenario for the assessment of everyday memory. J. Neurosci. Methods 2018, 303, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Bruun-Pedersen, J.R.; Serafin, S.; Kofoed, L.B. Going Outside While Staying Inside—Exercise Motivation with Immersive vs. Non–immersive Recreational Virtual Environment Augmentation for Older Adult Nursing Home Residents. In Proceedings of the 2016 IEEE International Conference on Healthcare Informatics, Chicago, IL, USA, 4–7 October 2016; pp. 216–226. [Google Scholar] [CrossRef]
- Ijaz, K.; Ahmadpour, N.; Naismith, S.L.; A Calvo, R. An Immersive Virtual Reality Platform for Assessing Spatial Navigation Memory in Predementia Screening: Feasibility and Usability Study. JMIR Ment. Health 2019, 6, e13887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korsgaard, D.; Bjørner, T.; Sørensen, P.K.; Bruun-Pedersen, J.R. Older adults eating together in a virtual living room: Opportunities and limitations of eating in augmented virtuality. In Proceedings of the ECCE 2019—31st European Conference on Cognitive Ergonomics: “‘Design for Cognition”, Belfast, UK, 10–13 September 2019; pp. 168–176. [Google Scholar] [CrossRef]
- Tomitsch, M.; Wrigley, C.; Borthwick, M.; Ahmadpour, N.; Frawley, J.; Kocaballi, A.B.; Nunez-Pacheco, C.; Straker, K. Design. Think. Make. Break. Repeat. A Handbook of Methods; BIS Publishing: Pretoria, South Africa, 2020. [Google Scholar]
- Ahmed, B.; Kim, D.H.; Hwang, Y.; Park, S.-J. Treatment of Alzheimer’s, Cognitive, Chronic Pain Rehabilitation, Depression and Anxiety disorders in One System for Elderly Using VR. In Proceedings of the 2018 15th International Conference on Ubiquitous Robots, UR, Jeju, Korea, June 28–July 1 2018; pp. 483–488. [Google Scholar] [CrossRef]
- Howes, S.; Charles, D.; Pedlow, K.; Wilson, I.M.; Holmes, D.; McDonough, S. User-centred design of an active computer gaming system for strength and balance exercises for older adults. J. Enabling Technol. 2019, 13, 101–111. [Google Scholar] [CrossRef]
- Kovar, I. Use of Virtual Reality as a Tool to Overcome the Post-Traumatic Stress Disorder of Pensioners. Int. J. Adv. Sci. Eng. Inf. Technol. 2019, 9, 841. [Google Scholar] [CrossRef]
- Micarelli, A.; Viziano, A.; Micarelli, B.; Augimeri, I.; Alessandrini, M. Vestibular rehabilitation in older adults with and without mild cognitive impairment: Effects of virtual reality using a head-mounted display. Arch. Gerontol. Geriatr. 2019, 83, 246–256. [Google Scholar] [CrossRef]
- Benham, S.; Kang, M.; Grampurohit, N. Immersive Virtual Reality for the Management of Pain in Community-Dwelling Older Adults. OTJR Occup. Particip. Health 2018, 39, 90–96. [Google Scholar] [CrossRef]
- Baqai, A.; Memon, K.; Memon, A.R.; Shah, S.M.Z.A. Interactive Physiotherapy: An Application Based on Virtual Reality and Bio-feedback. Wirel. Pers. Commun. 2018, 106, 1719–1741. [Google Scholar] [CrossRef]
- Sakhare, A.R.; Yang, V.; Stradford, J.; Tsang, I.; Ravichandran, R.; Pa, J. Cycling and Spatial Navigation in an Enriched, Immersive 3D Virtual Park Environment: A Feasibility Study in Younger and Older Adults. Front. Aging Neurosci. 2019, 11, 218. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.-C. Role-play in Virtual Reality Game for the Senior. In ACM International Conference Proceeding Series Part F1483(982); ACM: New York, NY, USA, 2019; pp. 31–35. [Google Scholar] [CrossRef]
- Mol, A.M.; Silva, R.S.; Ishitani, L. Design recommendations for the development of virtual reality focusing on the elderly. In Proceedings of the Iberian Conference on Information Systems and Technologies, CISTI, Coimbra, Portugal, 19–22 June 2019. [Google Scholar] [CrossRef]
- Süzer, K.; Olguntürk, N. The aid of colour on visuospatial navigation of elderly people in a virtual polyclinic environment. Color Res. Appl. 2018, 43, 872–884. [Google Scholar] [CrossRef]
- Lecavalier, N.C.; Ouellet, É; Boller, B.; Belleville, S. Use of immersive virtual reality to assess episodic memory: A validation study in older adults. Neuropsychol. Rehabil. 2018, 30, 462–480. [Google Scholar] [CrossRef] [PubMed]
- Plechatá, A.; Sahula, V.; Fayette, D.; Fajnerová, I. Age-Related Differences With Immersive and Non-immersive Virtual Reality in Memory Assessment. Front. Psychol. 2019, 10, 1330. [Google Scholar] [CrossRef] [PubMed]
- Bargas-Avila, J.A.; Hornbæk, K. Old wine in new bottles or novel challenges: A critical analysis of empirical studies of user experience. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Vancober, BC, Canada, 11–15 June 2011; pp. 2689–2698. [Google Scholar]
- Kennedy, R.S.; Lane, N.E.; Berbaum, K.S.; Lilienthal, M.G. Simulator sickness questionnaire: An enhanced meth-od for quantifying simulator sickness. Int. J. Aviat. Psychol. 1993, 3, 203–220. [Google Scholar] [CrossRef]
- Slater, M.; Usoh, M.; Steed, A. Depth of presence in virtual environments. Presence Teleoperators Virtual Environ. 1994, 3, 130–144. [Google Scholar] [CrossRef]
- McAuley, E.; Duncan, T.; Tammen, V.V. Psychometric properties of the Intrinsic Motivation Inventory in a com-petitive sport setting: A confirmatory factor analysis. Res. Q. Exerc. Sport 1989, 60, 48–58. [Google Scholar] [CrossRef]
- Lessiter, J.; Freeman, J.; Keogh, E.; Davidoff, J.B. A Cross-Media Presence Questionnaire: The ITC-Sense of Presence Inventory. Presence: Teleoperators Virtual Environ. 2001, 10, 282–297. [Google Scholar] [CrossRef] [Green Version]
- Lin, C.X.; Lee, C.; Lally, D.; Coughlin, J.F. Impact of Virtual Reality (VR) Experience on Older Adults’ Well-Being. In Lecture Notes in Computer Science (Including Subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics), 10927 LNCS; Springer: Berlin/Heidelberg, Germany, 2018; pp. 89–100. [Google Scholar] [CrossRef]
- Turner, P.; Turner, S.; Van De Walle, G. How older people account for their experiences with interactive technology. Behav. Inf. Technol. 2007, 26, 287–296. [Google Scholar] [CrossRef]
- Cleary, A.M.; Brown, A.S.; Sawyer, B.D.; Nomi, J.S.; Ajoku, A.C.; Ryals, A.J. Familiarity from the configuration of objects in 3-dimensional space and its relation to déjà vu: A virtual reality investigation. Conscious. Cogn. 2012, 21, 969–975. [Google Scholar] [CrossRef]
- Petri, K.; Feuerstein, K.; Folster, S.; Bariszlovich, F.; Witte, K. Effects of Age, Gender, Familiarity with the Content, and Exposure Time on Cybersickness in Immersive Head-mounted Display Based Virtual Reality. Am. J. Biomed. Sci. 2020, 107–121. [Google Scholar] [CrossRef]
- Steed, A.; Slater, M. A virtual presence counter. Presence Teleoperators Virtual Environ. 2000, 9, 413–434. [Google Scholar]
- Men, L.; Bryan-Kinns, N.; Hassard, A.S.; Ma, Z. The impact of transitions on user experience in virtual reality. IEEE Virtual Reality 2017, 285–286. [Google Scholar] [CrossRef]
- Slater, M.; Steed, A.; Mccarthy, J.; Marinelli, F. The Virtual Ante-Room: Assessing Presence through Expectation and Surprise. 1996. Available online: https://www.researchgate.net/publication/2499466_The_Virtual_Ante-Room_Assessing_Presence_through_Expectation_and_Surprise (accessed on 9 June 2022).
- Knibbe, J.; Schjerlund, J.; Petraeus, M.; Hornbæk, K. The Dream is Collapsing: The Experience of Exiting VR. In Proceedings of the Conference on Human Factors in Computing Systems, Montreal, QC, Canada, 25–27 April 2018; pp. 1–13. [Google Scholar] [CrossRef] [Green Version]
- Huber, T.; Paschold, M.; Hansen, C.; Lang, H.; Kneist, W. Artificial Versus Video-Based Immersive Virtual Surroundings: Analysis of Performance and User’s Preference. Surg. Innov. 2018, 25, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Piccione, J.; Collett, J.; De Foe, A. Virtual skills training: The role of presence and agency. Heliyon 2019, 5, e02583. [Google Scholar] [CrossRef] [PubMed]
- James, K.H.; Humphrey, G.K.; Vilis, T.; Al, J.E.T. “Active” and “passive” learning of three- dimensional object structure within an immersive virtual reality environment. Behav. Res. Methods Instrum. Comput. 2002, 34, 383–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phelan, I.; Furness, P.J.; Fehily, O.; Thompson, A.R.; Babiker, N.T.; A Lamb, M.; A Lindley, S. A Mixed-Methods Investigation Into the Acceptability, Usability, and Perceived Effectiveness of Active and Passive Virtual Reality Scenarios in Managing Pain Under Experimental Conditions. J. Burn Care Res. 2018, 40, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Ahmadpour, N.; Keep, M.; Janssen, A.; Rouf, A.S.; Marthick, M. Design Strategies for Virtual Reality Interventions for Managing Pain and Anxiety in Children and Adolescents: Scoping Review. JMIR Serious Games 2020, 8, e14565. [Google Scholar] [CrossRef]
- Ahmadpour, N.; Randall, H.; Choksi, H.; Gao, A.; Vaughan, C.; Poronnik, P. Virtual Reality interventions for acute and chronic pain management. Int. J. Biochem. Cell Biol. 2019, 114, 105568. [Google Scholar] [CrossRef]
- Massimi, M.; Baecker, R. Participatory design process with older users. In Proceedings of the UbiCoomp2006 Workshop on Future Media, Irvine, CA, USA, 12–16 June 2006. [Google Scholar]
- Karapanos, E.; Zimmerman, J.; Forlizzi, J.; Martens, J.-B. User experience over time: An initial framework. In Proceedings of the Conference on Human Factors in Computing Systems, Boston, MA, USA, 4–9 April 2009; pp. 729–738. [Google Scholar] [CrossRef]
- Madary, M.; Metzinger, T.K. Real virtuality: A code of ethical conduct. Recommendations for Good Scientific Practice and the Consumers of VR-Technology. Front. Robot. AI 2016, 3. [Google Scholar] [CrossRef]
- Munafo, J.; Diedrick, M.; Stoffregen, T.A. The virtual reality head-mounted display Oculus Rift induces motion sickness and is sexist in its effects. Exp. Brain Res. 2016, 235, 889–901. [Google Scholar] [CrossRef]
- Saredakis, D.; Szpak, A.; Birckhead, B.; Keage, H.A.D.; Rizzo, A.; Loetscher, T. Factors Associated with Virtual Reality Sickness in Head-Mounted Displays: A Systematic Review and Meta-Analysis. Front. Hum. Neurosci. 2020, 14, 96. [Google Scholar] [CrossRef] [Green Version]
- Sharples, S.; Cobb, S.; Moody, A.; Wilson, J.R. Virtual reality induced symptoms and effects (VRISE): Comparison of head mounted display (HMD), desktop and projection display systems. Displays 2008, 29, 58–69. [Google Scholar] [CrossRef]
- Appel, L.; Appel, E.; Bogler, O.; Wiseman, M.; Cohen, L.; Ein, N.; Abrams, H.B.; Campos, J.L. Older Adults With Cognitive and/or Physical Impairments Can Benefit FROM Immersive Virtual Reality Experiences: A Feasibility Study. Front. Med. 2020, 6, 329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kugler, L. The state of virtual reality hardware. Commun. ACM 2021, 64, 15–16. [Google Scholar] [CrossRef]
- Oculus. Oculus Rift S. Available online: https://www.oculus.com/rift-s/ (accessed on 10 June 2022).
- Zhao, W.; Baker, S.; Waycott, J. Challenges of Deploying VR in Aged Care: A Two-Phase Exploration Study. In Proceedings of the 32nd Australian Conference on Human-Computer Interaction, Sydney, Australia, 2–4 December 2020. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Section A | |||||||||||
| References | Objectives | Context | Hardware | Type of Application | Narrative | Visual | Audio | Cohort | OA Sample Size (Female) | OA Age Range | OA Clinical Condition |
| Ahmed et al. (2018) | Psychological disorders | Lab setting | Oculus Rift | Bespoke | (1) Wrist and arm exercise for physical fitness and (2) navigation practice for memorization | VR game | – | OA | 20 (15F) | 55–84 | Both |
| Andringa et al. (2019) | Cognitive training | Day care centre | HTC Vive | Bespoke | Play VR balloon pricking game | VR game | – | OA | 10 (7F) | – | Both |
| Baker, Kelly et al. (2019) | Wellbeing | Lab setting | HTC Vive and Oculus Rift | Bespoke | Sit around a reflective pond and talk to each other | 3D VE | – | OA | 22 (11F) | 70–81 | Healthy |
| Baker, Waycott et al. (2019) | Wellbeing | Resident facilities | Oculus Rift | Commercial | Play games such as Quil (drawing), Ocean Rift (discovery), ToyBox, and Power Solitaire | VR game | – | OA, Staff | 5 (2F) | 74–88 | Patient |
| Banville et al. (2018) | Neuropsychological | Lab setting | Oculus Rift | Bespoke | Perform several tasks alone based on daily life | 3D VE | – | OA, YA | 11 (8F) | 63–72 | Healthy |
| Baqai et al. (2019) | Physiotherapy | Lab setting | Oculus Rift | Bespoke | Collect fruits hanging from a tree | VR game | Audio feedback | OA, YA | 2 (1F) | 58–68 | Patient |
| Benham et al. (2019) | Pain management | Senior day centre | HTC Vive | Commercial | Play popular games (engagement with pets, interactive music, travel) | VR game | – | OA | 12 (8F) | Mean 70.2 | Patient |
| Brown (2019) | Usability, Preferences, Application | Lab setting | Samsung Gear VR | Bespoke | Watch a series of 6 videos consisted of walks and drives around the town of the participants | 360° video | – | OA | 10 (8F) | 63–89 | Healthy |
| Bruun-Pedersen et al. (2016) | Physiothrepapy | Nursing home | Oculus Rift | Bespoke | Bike through nature-based trails | 3D VE | Bird tweets | OA | 9 (9F) | 69–101 | Healthy |
| Coldham and Cook (2017) | Usability | Lab setting | HTC Vive | Commercial | Navigate to any point in Google Earth and find their way home | 3D VE | Background noise | OA | 19 | > 65 | Healthy |
| Eisapour et al. (2018a) | Physiotherapy | Long-term care, retirement home | Oculus Rift | Bespoke | Do activities focusing on upper body motions | VR game | Audio instruction | OA, Therapists | 3 | – | Patient |
| Eisapour et al. (2018b) | Physiotherapy | Long-term care, retirement home | Oculus Rift | Bespoke | Do five motions related to neck, shoulders, and arms | VR game | Audio instruction | OA, Therapists | 6 (5F) | Mean 86.8 | Patient |
| Section B | |||||||||||
| References | Objectives | Context | Hardware | Type of Application | Narrative | Visual | Audio | Cohort | OA Sample Size, Female | OA Age Range | OA Clinical Condition |
| Hodge et al., (2018) | Entertainment | Community centre | Google Cardboard; Unspecified HMD | Bespoke | Explore and navigate through VR environments | 3D VE | Ambient sound | OA, Carers | 4 | 53–83 | Patient |
| Howes et al. (2019) | Fall & Balance | Day centre | Oculus Rift | Bespoke | Do four mini-exergames (a) knee bends; (b) leg abduction; (c) sideways walking; (d) one leg stand. | VR game | – | OA | 4 | > 65 | Healthy |
| Huang (2019) | Cognitive training | Lab setting | Oculus Rift | Commercial | Play Fruit Ninja game | VR game | – | OA | 16 | – | Healthy |
| Huygelier et al. (2019) | Usability (Acceptance) | Lab setting | Oculus Rift | Commercial | Experience the VR application Perfect of nDreams | 3D VE | – | OA | 38 (19F) | 60–92 | Healthy |
| Ijaz et al. (2016) | Wellbeing | Community centre | Oculus Rift | Bespoke | Experience a virtual tour or beat the previous players by finding more landmarks in competetive game | VR game | Audio feedback | OA, YA | 20 | 60–92 | Healthy |
| Ijaz et al. (2019) | Spatial navigation | Lab setting | Oculus Rift | Bespoke | Take a landmark recall test | Immersive photorealistic imagery | Audio instruction | OA | 22 | 50–89 | Healthy |
| Janeh et al. (2018) | Gait | Lab setting | HTC Vive | Bespoke | Walk at a normal pace along the virtual walkway | 3D VE | – | OA, YA | 21 (12F) | 45–83 | Healthy |
| Kim et al. (2017) | Neuro-rehabilitation | Lab setting | Oculus Rift | Bespoke | Walk forward in a virtual city on a pedestrian path for 800m, on a treadmill | 3D VE | – | OA, YA | 22 (16F) | Mean: 65 | Both |
| Korsgaard et al. (2019) | Wellbeing | Lab setting | Oculus Rift CV1 | Bespoke | Talk to older friends while eating a solitary meal in augmented virtuality. | 3D augmented VE | – | OA | 27 (20F) | > 65 | Healthy |
| Kovar (2019) | Anxiety | – | Samsung Gear VR | Bespoke | Watch 360° video that gradually simulated similar but easier traumatic event as he overcame in the past | 360° video | Environment sound | OA | 4 (2F) | 61–77 | Patient |
| Lai et al. (2019) | Entertainment | Lab setting | HTC Vive Pro | Commercial | Play one of the three different VR applications, i.e., The Blu, Fruit Ninja, and Tilt Brush | VR game | – | OA | 14 (9F) | 54–82 | Healthy |
| Lecavalier et al. (2018) | Memory assessment | Lab setting | Nvisor ST50 | Bespoke | Memorise a shopping list and then fetch the items in the store | 3D VE | Ambient sound | OA, YA | 57 (47F) | Mean: 67.77 | Healthy |
| Section C | |||||||||||
| References | Objectives | Context | Hardware | Type of Application | Narrative | Visual | Audio | Cohort | OA Sample Size, Female | OA Age Range | OA Clinical Condition |
| Liao et al. (2019) | Gait | Community centre | HTC Vive | Bespoke | Imitate the virtual character and adjust their movements based on the simultaneous visual and auditory feedback | 3D VE | Audio feedback | OA | 18 (11F) | >65 | Patient |
| Lin et al. (2018) | Wellbeing | Assisted living communities | Samsung Gear VR | Commercial | Watch videos, Google Street View, and guided tours | 360° video | – | OA | Pre: 35 (23F), Post: 31 (21F) | 68–99 | Healthy |
| Liu et al. (2018) | Wellbeing | Community centre | Pico 4K G2 | Commercial | Watch video contained China’s sceneries | 360° video | – | OA, YA | 58 (36F) | 60–91 | Healthy |
| Micarelli et al. (2019) | Rehabilitation | Home-based setting | Revelation 3D | Bespoke | Play the Track Speed Racing 3D game by tilting the head | VR game | – | OA | 47 (26F) | Mean 76.3 | Patient |
| Mol et al. (2019) | Wellbeing | Participants’ preferred places | Google Cardboard | Bespoke | Dance an old song (Y.M.C.A.) inside the living room | VR game | Ambient sound | OA | 10 (8F) | 60–77 | Healthy |
| Ouellet et al. (2019) | Memory assessment | Lab setting | Nvisor ST50 | Bespoke | Participants memorize shopping list and later have to "buy" these same items | 3D VE | Ambient sound | OA, YA | 54 (44F) | Mean 68 Mean 67.20 | Both |
| Plechatá et al. (2019) | Memory assessment | Lab setting | HTC Vive | Bespoke | Memorize a shopping list and later find and collect recalled items in the virtual grocery store | 3D VE | – | OA, YA | 36 (23F) | 60–91 | Healthy |
| Roberts et al. (2019) | Usability (Acceptance) | Lab setting | Samsung Gear VR | Commercial | View two audio-visual VR simulations ("Jurassic World" and "Cirque du Soleil") | 3D VE | – | OA | 41 (31F) | 50–99 | Both |
| Sakhare et al. (2019) | Spatial navigation | Lab setting | HTC Vive Pro | Bespoke | Bike 0.5 miles to a fountain landmark | 3D VE | Music | OA, YA | 20 (10F) | 52–70 | Healthy |
| Seo et al. (2019) | Usability (Experience) | Lab setting | Samsung Odyssey | Bespoke | Evacuate the subway station | 3D VE | – | OA, YA | 5 (4F) | 65–77 | Healthy |
| Süzer and Olguntürk (2018) | Spatial navigation | Lab setting | HTC Vive | Bespoke | Take route replication task and picture classification test | 3D VR | – | OA | 90 (45F) | 65–80 | Healthy |
| Yang (2019) | Therapy | Lab setting | HTC Vive | Bespoke | Help Little Red Riding Hood to navigate through the game | VR game | Audio feedback, Music | OA | 6 | 65–70 | Healthy |
| UX Research Methods | Number of Articles (%) | References | Type of Methods |
|---|---|---|---|
| None | 1 (2.8%) | Liao et al. (2019) | |
| Qualitative | 9 (25%) | Baker, Kelly et al. (2019), Benham et al. (2019), Brown (2019), Coldham and Cook (2017), Eisapour et al. (2018a), Hodge et al. (2018), Korsgaard et al. (2019), Seo et al. (2019), Yang (2019) | Focus groups, interviews, observations, audio, and video recordings. |
| Quantitative | 15 (41.7%) | Ahmed et al. (2018), Banville et al. (2018), Eisapour et al. (2018b), Huang (2019), Huygelier et al. (2019), Janeh et al. (2018), Kim et al. (2017), Kovar (2019), Lai et al. (2019), Lecavalier et al. (2018), Micarelli et al. (2019), Ouellet et al. (2019), Plechatá et al. (2019), Sakhare et al. (2019), Süzer and Olguntürk (2018) | Physiological data, task performance data, standardised and custom questionnaires. |
| Mixed methods | 11 (30.5%) | Andringa et al. (2019), Baker, Waycott et al. (2019), Baqai et al. (2019), Bruun-Pedersen et al. (2016), Howes et al. (2019), Ijaz et al. (2016), Ijaz et al. (2019), Lin et al. (2018), Liu et al. (2019), Mol et al. (2019), Roberts et al. (2019) |
| UX Aspects | Number of Articles (%) | References |
|---|---|---|
| Generic | 13 (36.1%) | Andringa et al. (2019), Baker, Kelly et al. (2019), Baker, Waycott et al. (2019), Brown (2019), Bruun-Pedersen et al. (2016), Eisapour et al. (2018a), Hodge et al. (2018), Howes et al. (2019), Ijaz et al. (2016), Ijaz et al. (2019), Korsgaard et al. (2019), Mol et al. (2019), Yang (2019) |
| Presence/Immersion | 12 (33.3%) | Banville et al. (2018), Bruun-Pedersen et al. (2016), Eisapour et al. (2018a), Huang (2019), Huygelier et al. (2019), Janeh et al. (2018), Kim et al. (2017), Lecavalier et al. (2018), Liu et al. (2019), Roberts et al. (2019), Sakhare et al. (2019), Süzer and Olguntürk (2018) |
| Performance | 10 (27.8%) | Ahmed et al. (2018), Andringa et al. (2019), Banville et al. (2018), Baqai et al. (2019), Ijaz et al. (2019), Lecavalier et al. (2018), Ouellet et al. (2019), Plechatá et al. (2019), Sakhare et al. (2019), Süzer and Olguntürk (2018) |
| Others * | 9 (25.0%) | Andringa et al. (2019), Baqai et al. (2019), Brown (2019), Eisapour et al. (2018b), Ijaz et al. (2016), Howes et al. (2019), Roberts et al. (2019), Sakhare et al. (2019), Seo et al. (2019) |
| Cybersickness/Discomfort/Challenges | 8 (22.2%) | Banville et al. (2018), Huygelier et al. (2019), Janeh et al. (2018), Kim et al. (2017), Lecavalier et al. (2018), Micarelli et al. (2019), Sakhare et al. (2019), Seo et al. (2019) |
| Experience | 7 (19.4%) | Baker, Kelly et al. (2019), Baker, Waycott et al. (2019), Baqai et al. (2019), Benham et al. (2019), Bruun-Pedersen et al. (2016), Coldham and Cook (2017), Mol et al. (2019) |
| Motivation | 7 (19.4%) | Andringa et al. (2019), Baker, Kelly et al. (2019), Bruun-Pedersen et al. (2016), Huygelier et al. (2019), Ijaz et al. (2016), Ijaz et al. (2019), Lecavalier et al. (2018) |
| Usability/Applicability/Acceptability/Perceived Usefulness/Desirability | 7 (19.4%) | Baker, Waycott et al. (2019), Bruun-Pedersen et al. (2016), Howes et al. (2019), Huygelier et al. (2019), Lin et al. (2018), Plechatá et al. (2019), Roberts et al. (2019) |
| Affect/Emotion/Feeling | 6 (16.7%) | Lai et al. (2019), Lin et al. (2018), Liu et al. (2019), Mol et al. (2019), Roberts et al. (2019), Seo et al. (2019) |
| Attitude/Perception | 6 (16.7%) | Brown (2019), Huygelier et al. (2019), Lai et al. (2019), Lin et al. (2018), Liu et al. (2019), Mol et al. (2019) |
| Anxiety/Stress | 5 (13.9%) | Andringa et al. (2019), Ijaz et al. (2019), Kim et al. (2017), Kovar (2019), Sakhare et al. (2019) |
| Enjoyment | 4 (11.1%) | Andringa et al. (2019), Eisapour et al. (2018b), Huygelier et al. (2019), Ijaz et al. (2016) |
| Satisfaction/Likely to recommend | 3 (8.3%) | Eisapour et al. (2018b), Ijaz et al. (2019), Lin et al. (2018) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ijaz, K.; Tran, T.T.M.; Kocaballi, A.B.; Calvo, R.A.; Berkovsky, S.; Ahmadpour, N. Design Considerations for Immersive Virtual Reality Applications for Older Adults: A Scoping Review. Multimodal Technol. Interact. 2022, 6, 60. https://0-doi-org.brum.beds.ac.uk/10.3390/mti6070060
Ijaz K, Tran TTM, Kocaballi AB, Calvo RA, Berkovsky S, Ahmadpour N. Design Considerations for Immersive Virtual Reality Applications for Older Adults: A Scoping Review. Multimodal Technologies and Interaction. 2022; 6(7):60. https://0-doi-org.brum.beds.ac.uk/10.3390/mti6070060
Chicago/Turabian StyleIjaz, Kiran, Tram Thi Minh Tran, Ahmet Baki Kocaballi, Rafael A. Calvo, Shlomo Berkovsky, and Naseem Ahmadpour. 2022. "Design Considerations for Immersive Virtual Reality Applications for Older Adults: A Scoping Review" Multimodal Technologies and Interaction 6, no. 7: 60. https://0-doi-org.brum.beds.ac.uk/10.3390/mti6070060