A Mixed-Methods Approach to Understanding Knowledge of Mosquito-Borne Infections and Barriers for Protection in Hanoi, Vietnam

 , , ,
, , , 
Abstract
:
1. Introduction
2. Material and Methods
2.1. Study Design
2.2. Study Area and Sample
2.3. Ethical Approval
2.4. KP Questionnaire
2.5. Mapping Exercise
2.6. Statistical Analysis
2.7. System Network Analysis
3. Results
3.1. Demographics
3.2. Assessment of Knowledge
3.3. Assessment of Practices
3.4. Association Between KP Scores and Demographic Variables
3.5. Correlation Between Knowledge and Practices
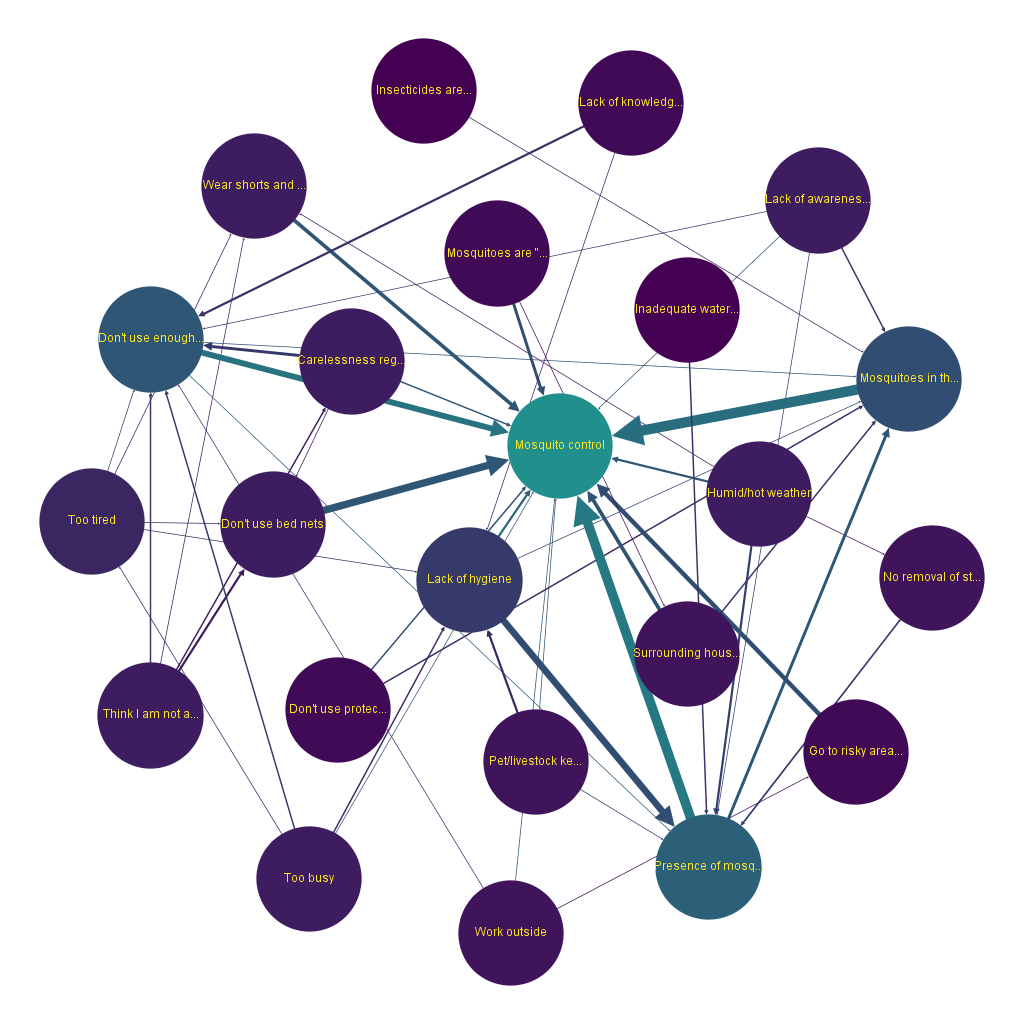
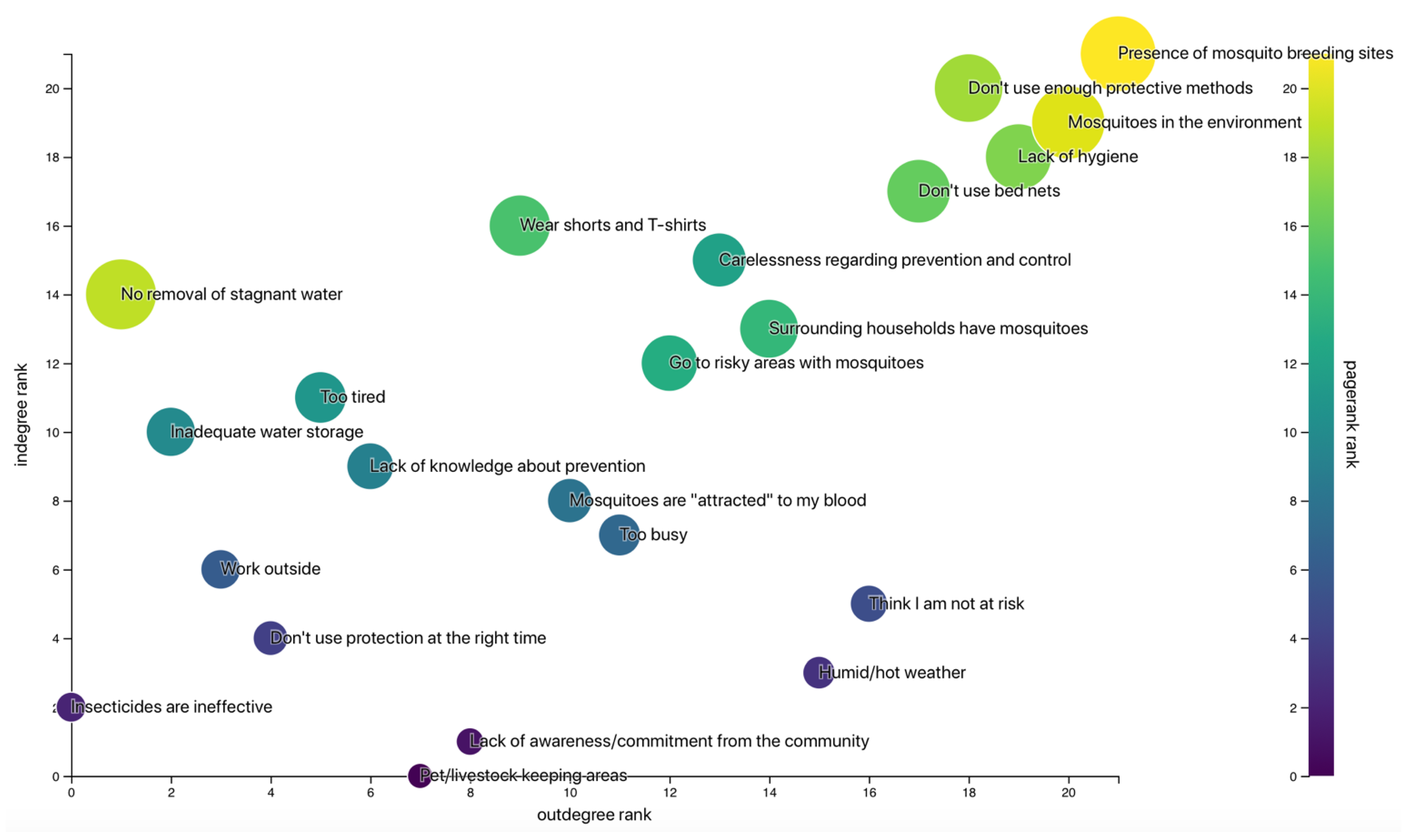
3.6. System Network Analysis
4. Discussion
5. Conclusion and Recommendations
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Brady, O.J.; Gething, P.W.; Bhatt, S.; Messina, J.P.; Brownstein, J.S.; Hoen, A.G.; Moyes, C.L.; Farlow, A.W.; Scott, T.W.; Hay, S.I. Refining the Global Spatial Limits of Dengue Virus Transmission by Evidence-Based Consensus. PLOS Neglected Trop. Dis. 2012, 6, e1760. [Google Scholar] [CrossRef]
- Bhatt, S.; Gething, P.W.; Brady, O.J.; Messina, J.P.; Farlow, A.W.; Moyes, C.L.; Drake, J.M.; Brownstein, J.S.; Hoen, A.G.; Sankoh, O.; et al. The global distribution and burden of dengue. Nature 2013, 496, 504–507. [Google Scholar] [CrossRef]
- Lee, H.S.; Nguyen-Viet, H.; Nam, V.S.; Lee, M.; Won, S.; Duc, P.P.; Grace, D. Seasonal patterns of dengue fever and associated climate factors in 4 provinces in Vietnam from 1994 to 2013. BMC Infect. Dis. 2017, 17, 218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pham Thi, K.L.; Briant, L.; Gavotte, L.; Labbe, P.; Perriat-Sanguinet, M.; Cornillot, E.; Vu, T.D.; Nguyen, T.Y.; Tran, V.P.; Nguyen, V.S.; et al. Incidence of dengue and chikungunya viruses in mosquitoes and human patients in border provinces of Vietnam. Parasites Vectors 2017, 10, 556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuong, H.Q.; Hien, N.T.; Duong, T.N.; Phong, T.V.; Cam, N.N.; Farrar, J.; Nam, V.S.; Thai, K.T.D.; Horby, P. Quantifying the Emergence of Dengue in Hanoi, Vietnam: 1998–2009. PLOS Neglected Trop. Dis. 2011, 5, e1322. [Google Scholar] [CrossRef] [PubMed]
- Nguyen-Tien, T.; Lundkvist, Å.; Lindahl, J. Urban transmission of mosquito-borne flaviviruses—A review of the risk for humans in Vietnam. Infect. Ecol. Epidemiol. 2019, 9, 1660129. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Update on the Dengue Situation in the Western Pacific Region; Dengue Situation Update; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Gubler, D.J. The Global Emergence/Resurgence of Arboviral Diseases As Public Health Problems. Arch. Med. Res. 2002, 33, 330–342. [Google Scholar] [CrossRef] [Green Version]
- Minh An, D.T.; Rocklöv, J. Epidemiology of dengue fever in Hanoi from 2002 to 2010 and its meteorological determinants. Glob. Health Action 2014, 7, 23074. [Google Scholar] [CrossRef]
- Swaddiwudhipong, W.; Lerdlukanavonge, P.; Khumklam, P.; Koonchote, S.; Nguntra, P.; Chaovakiratipong, C. A survey of Knowledge, Attitude and Practice of the prevention of Dengue hemorrhagic fever in an urban community of Thailand. Southeast Asian J. Trop. Med. Public Health 1992, 5, 1–2. [Google Scholar]
- Arunachalam, N.; Tyagi, B.K.; Samuel, M.; Krishnamoorthi, R.; Manavalan, R.; Tewari, S.C.; Ashokkumar, V.; Kroeger, A.; Sommerfeld, J.; Petzold, M. Community-based control of Aedes aegypti by adoption of eco-health methods in Chennai City, India. Pathog. Glob. Health 2012, 106, 488–496. [Google Scholar] [CrossRef] [Green Version]
- Pengvanich, V. Family Leader Empowerment Program Using Participatory Learning Process for Dengue Vector Control. J. Med. Assoc. Thail. 2011, 94, 235. [Google Scholar]
- Abeyewickreme, W.; Wickremasinghe, A.R.; Karunatilake, K.; Sommerfeld, J.; Axel, K. Community mobilization and household level waste management for dengue vector control in Gampaha district of Sri Lanka; an intervention study. Pathog. Glob. Health 2012, 106, 479–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Espinoza-Gomez, F. Educational campaign versus malathion spraying for the control of Aedes aegypti in Colima, Mexico. J. Epidemiol. Community Health 2002, 56, 148–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersson, N.; Nava-Aguilera, E.; Arosteguí, J.; Morales-Perez, A.; Suazo-Laguna, H.; Legorreta-Soberanis, J.; Hernandez-Alvarez, C.; Fernandez-Salas, I.; Paredes-Solís, S.; Balmaseda, A.; et al. Evidence based community mobilization for dengue prevention in Nicaragua and Mexico (Camino Verde, the Green Way): Cluster randomized controlled trial. BMJ 2015, h3267. [Google Scholar] [CrossRef] [Green Version]
- Paixão, M.M.; Ballouz, T.; Lindahl, J.F. Effect of Education on Improving Knowledge and Behavior for Arboviral Diseases: A Systematic Review and Meta-Analysis. Am. J. Trop. Med. Hyg. 2019. [Google Scholar] [CrossRef]
- Kusuma, Y.S.; Burman, D.; Kumari, R.; Lamkang, A.S.; Babu, B.V. Impact of health education based intervention on community’s awareness of dengue and its prevention in Delhi, India. Glob Health Promot. 2019, 26, 50–59. [Google Scholar] [CrossRef]
- Healy, K.; Hamilton, G.; Crepeau, T.; Healy, S.; Unlu, I.; Farajollahi, A.; Fonseca, D.M. Integrating the Public in Mosquito Management: Active Education by Community Peers Can Lead to Significant Reduction in Peridomestic Container Mosquito Habitats. PLoS ONE 2014, 9, e108504. [Google Scholar] [CrossRef] [Green Version]
- Sreedevi, A.; Burru, R.; Rao, G.; Yalamanchili, P.; Subhaprada, C.; Kumari, V.; Kala, S.; Ms, A. Study on awareness about vector borne diseases and education about preventive measures in rural field practice areas of Kurnool medical college, Kurnool. Int. J. Med. Sci. Public Health 2016, 5, 1803. [Google Scholar] [CrossRef] [Green Version]
- Saurabh, S.; Veerakumar, A.M.; Kalaiselvi, S.; Palanivel, C. Effectiveness of individual health education on the practice of dengue fever prevention in an urban area of Puducherry, India. Indian J. Community Health 2014, 26, 434–437. [Google Scholar]
- Hung, P.T. Factors determining Dengue in Viet Nam and vector control strategy: A literature review. Master’s Thesis, KIT (Royal Tropical Institute), Amsterdam, The Netherlands, 2016. [Google Scholar]
- Craven, L. System Effects: A Hybrid Methodology for Exploring the Determinants of Food In/Security. Ann. Am. Assoc. Geogr. 2017, 109, 1011–1027. [Google Scholar] [CrossRef]
- Mayxay, M.; Cui, W.; Thammavong, S.; Khensakhou, K.; Vongxay, V.; Inthasoum, L.; Sychareun, V.; Armstrong, G. Dengue in peri-urban Pak-Ngum district, Vientiane capital of Laos: A community survey on knowledge, attitudes and practices. BMC Public Health 2013, 13, 434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yasuoka, J.; Mangione, T.W.; Spielman, A.; Levins, R. Impact of education on knowledge, agricultural practices, and community actions for mosquito control and mosquito-borne disease prevention in rice ecosystems in Sri Lanka. Am. J. Trop. Med. Hyg. 2006, 74, 1034–1042. [Google Scholar] [CrossRef] [PubMed]
- Kumaran, E.; Doum, D.; Keo, V.; Sokha, L.; Sam, B.; Chan, V.; Alexander, N.; Bradley, J.; Liverani, M.; Prasetyo, D.B.; et al. Dengue knowledge, attitudes and practices and their impact on community-based vector control in rural Cambodia. PLoS Negl. Trop. Dis. 2018, 12, e0006268. [Google Scholar] [CrossRef] [Green Version]
- Rigau-Pérez, J.G.; Clark, G.G.; Ruiz-Pérez, M.; Winch, P.J.; Leontsini, E.; Gubler, D.J. Community-based dengue prevention programs in Puerto Rico: Impact on knowledge, behavior, and residential mosquito infestation. Am. J. Trop. Med. Hyg. 2002, 67, 363–370. [Google Scholar]
- Huynh, T.; Tsuzuki, A.; Luu, L.; Tsunoda, T.; Takagi, M.; Kawada, H. Effect of Existing Practices on Reducing Aedes aegypti Pre-adults in Key Breeding Containers in Ho Chi Minh City, Vietnam. Am. J. Trop. Med. Hyg. 2009, 80, 752–757. [Google Scholar]
- Setbon, M.; Raude, J. Population response to the risk of vector-borne diseases: Lessons learned from socio-behavioural research during large-scale outbreaks. EHTJ 2009, 2. [Google Scholar] [CrossRef]
- Hoshi, T.; Martin Banda, P.; Foster Pemba, D.; Sunahara, T.; Minakawa, N. Beyond buzzing: Mosquito watching stimulates malaria bednets use—A household-based cluster-randomized controlled assessor blind educational trial. Emerg. Microbes Infect. 2019, 2, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Godin, G. L’éducation pour la santé : Les fondements psycho-sociaux de la définition des messages éducatifs. Sci. Soc. Santé 1991, 9, 67–94. [Google Scholar] [CrossRef]
- Nguyen-Tien, T.; Probandari, A.; Ahmad, R.A. Barriers to Engaging Communities in a Dengue Vector Control Program: An Implementation Research in an Urban Area in Hanoi City, Vietnam. Am. J. Trop. Med. Hyg. 2019, 100, 964–973. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| Characteristic | % (N = 117) |
|---|---|
| Gender | |
| Male | 42.7 (50) |
| Female | 57.3 (67) |
| Age (Mean ± SD) | 52.13 ± 13.95 |
| 18–39 | 20.5 (24) |
| 40–49 | 23.9 (28) |
| 50–59 | 24.8 (29) |
| 60+ | 30.8 (36) |
| Education | |
| Primary school | 13.7 (16) |
| Secondary school | 34.2 (40) |
| High school | 34.2 (40) |
| College/University | 17.9 (21) |
| Occupation | |
| Unemployed | 4.3 (5) |
| Farmer | 34.2 (40) |
| Worker/Seller | 17.1 (20) |
| Public or private services | 11.1 (13) |
| Self-employed | 9.4 (11) |
| Retired | 22,2 (26) |
| Student | 1.7 (2) |
| Family Member Diagnosed with Dengue | |
| Yes | 9.4 (11) |
| No | 90.6 (106) |
| Question | % (N = 117) |
|---|---|
| Which Disease(s) Transmitted by Mosquitoes Have you Heard About? | |
| Don’t know any | 12.8 (15) |
| Dengue | 82.1 (96) |
| Japanese encephalitis | 0.9 (1) |
| Zika | 1.7 (2) |
| Malaria | 15.4 (18) |
| What Symptoms of MBDs do You Know? * | |
| Don’t know any | 33.3 (39) |
| High fever | 61.5 (72) |
| Muscle pain | 4.3 (5) |
| Nausea/vomiting | 2.6 (3) |
| Severe headache | 4.3 (5) |
| Rash | 14.5 (17) |
| Hemorrhage | 45.3 (53) |
| What do You Think Can Increase the Risk of Getting Infected with MBDs? * | |
| Don’t know | 46.2 (54) |
| Warm and wet season | 36.8 (43) |
| High population density | 1.7 (2) |
| Stagnant water | 28.2 (33) |
| Livestock keeping | 16.2 (19) |
| Can You List Mosquito Breeding Sites? * | |
| Don’t know any | 6.0 (7) |
| Clean water collection | 1.7 (2) |
| Drain/polluted water | 59.8 (70) |
| Stagnant water containers | 62.4 (73) |
| Tires | 5.1 (6) |
| Water tanks, jars or buckets | 25.6 (30) |
| Vase | 6.0 (7) |
| Bonsai rockery | 6.0 (7) |
| Garbage/rubbish | 2.6 (3) |
| Which Season do You Think is Most at Risk for MBDs? | |
| Spring | 18.8 (22) |
| Summer | 51.3 (60) |
| Autumn | 2.6 (3) |
| Winter | 0.9 (1) |
| No difference | 0.9 (1) |
| Rainy season | 25.6 (30) |
| Question | % (N = 117) |
|---|---|
| Which Methods do You Use to Prevent Yourself and Your Family from Getting Infected with MBDs? * | |
| Don’t use any | 0.9 (1) |
| Screening of doors/windows | 0.9 (1) |
| Mosquito repellent creams/liquid | 16.2 (19) |
| Mosquito nets | 83.8 (98) |
| Electric rackets | 35.9 (42) |
| Mosquito coils/Incense sticks | 2.6 (3) |
| Covering clothes | 3.4 (4) |
| Keeping lids on water tanks | 3.4 (4) |
| Use of chemicals in water containers | 4.3 (5) |
| Anti-mosquito products (e.g., insecticides) | 65.8 (77) |
| Elimination of breeding sites | 44.4 (52) |
| Fish in water containers | 6.8 (8) |
| Mosquito traps inside home | 12.8 (15) |
| How Often do You Remove Mosquito Breeding Sites? | |
| Never | 0.9 (1) |
| Once in several months | 11.1 (13) |
| Once per month | 1.7 (2) |
| 2–3 times per month | 6.8 (8) |
| Once a week | 6.8 (8) |
| 2–3 times per week | 19.7 (23) |
| Daily | 49.6 (58) |
| Only after raining | 3.4 (4) |
| Variable | K Score 7 ± 4 | p-Value (Univariable) | p-Value (Multivariable) | P Score 3 ± 1 | p-Value (Univariable) | p-Value (Multivariable) |
|---|---|---|---|---|---|---|
| Gender * | ||||||
| Male | 8 ± 3 | 0.138 | - | 4 ± 3 | 0.610 | - |
| Female | 7 ± 5 | 3 ± 2 | ||||
| Age ** | ||||||
| 18–39 | 7 ± 5.5 | 0.429 | - | 3 ± 2 | 0.697 | - |
| 40–49 | 7 ± 3.5 | 3 ± 2 | ||||
| 50–59 | 8 ± 6 | 3 ± 2 | ||||
| 60+ | 7.5 ± 5 | 3.5 ± 2 | ||||
| District ** | ||||||
| Chuong My | 7 ± 4 | 0.065 | 0.092 | 3 ± 2 | 0.019 | 0.142 |
| Ha Dong | 8 ± 5 | 4 ± 2 | ||||
| Ba Dinh | 8 ± 3 | 4 ± 2 | ||||
| Education ** | ||||||
| Primary school | 6 ± 5 | 0.003 | 0.001 | 3 ± 2 | 0.041 | 0.233 |
| Secondary school | 7 ± 3.5 | 3 ± 2.5 | ||||
| High school | 8.5 ± 4 | 4 ± 2 | ||||
| College/University | 8 ± 4 | 3 ± 2 | ||||
| Occupation** | ||||||
| Unemployed | 6 ± 1 | 0.022 | 0.396 | 3 ± 2 | 0.003 | 0.319 |
| Farmer | 7 ± 4.5 | 3 ± 2 | ||||
| Worker/Seller | 7 ± 2.5 | 3 ± 0.5 | ||||
| Public or private services | 9 ± 5 | 5 ± 2 | ||||
| Self-employed | 8 ± 6 | 5 ± 3 | ||||
| Retired | 9 ± 5 | 4 ± 2 | ||||
| Student | 3.5 ± 1 | 2 ± 4 | ||||
| Family member diagnosed with dengue * | ||||||
| Yes | 12 ± 6 | 0.047 | 0.050 | 4 ± 1 | 0.032 | 0.188 |
| No | 7 ± 0.4 | 3 ± 1 |
| Factor | Weighted Indegree | Weighted Outdegree | Eigencentrality | PageRank |
|---|---|---|---|---|
| Presence of mosquito breeding sites | 20 | 17 | 0.525666 | 0.098047 |
| Do not use enough protective methods | 14 | 10 | 0.065081 | 0.064626 |
| Lack of hygiene | 7 | 13 | 0.035786 | 0.043412 |
| Do not use bed nets | 5 | 10 | 0.039116 | 0.032595 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chapot, L.; Nguyen-Tien, T.; Pham-Thanh, L.; Nguyen-Viet, H.; Craven, L.; Lindahl, J.F. A Mixed-Methods Approach to Understanding Knowledge of Mosquito-Borne Infections and Barriers for Protection in Hanoi, Vietnam. Trop. Med. Infect. Dis. 2020, 5, 66. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed5020066
Chapot L, Nguyen-Tien T, Pham-Thanh L, Nguyen-Viet H, Craven L, Lindahl JF. A Mixed-Methods Approach to Understanding Knowledge of Mosquito-Borne Infections and Barriers for Protection in Hanoi, Vietnam. Tropical Medicine and Infectious Disease. 2020; 5(2):66. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed5020066
Chicago/Turabian StyleChapot, Lorraine, Thang Nguyen-Tien, Long Pham-Thanh, Hung Nguyen-Viet, Luke Craven, and Johanna F Lindahl. 2020. "A Mixed-Methods Approach to Understanding Knowledge of Mosquito-Borne Infections and Barriers for Protection in Hanoi, Vietnam" Tropical Medicine and Infectious Disease 5, no. 2: 66. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed5020066