Rabies as a Public Health Concern in India—A Historical Perspective

 , ,
, ,
Abstract
:1. Introduction
2. Rabies Documentation in Pre-Independence India
3. Pasteur Institutes and Rabies Vaccination in British India
4. Rabies Control in Animals
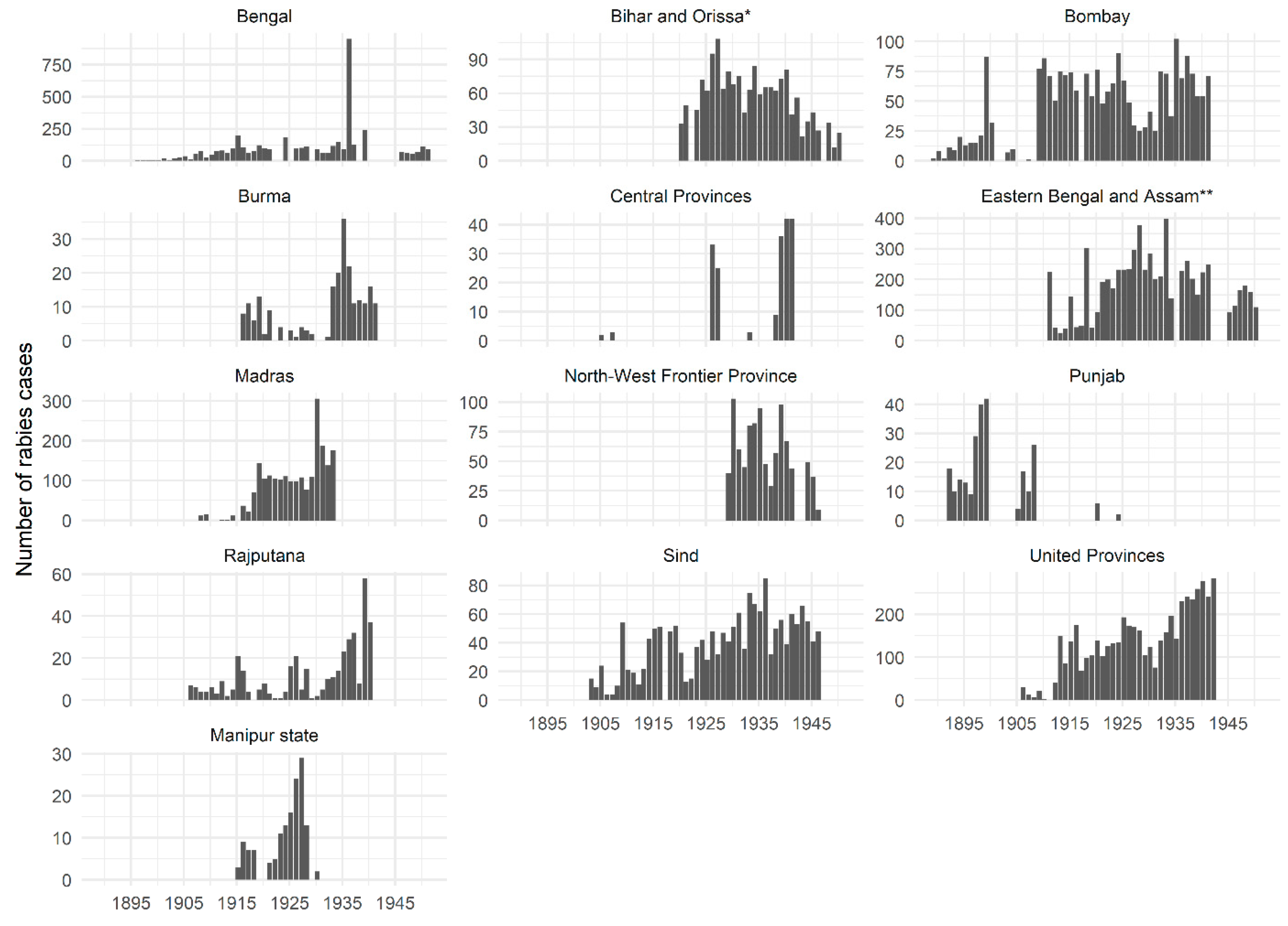
5. Historic Animal Rabies Incidence in India
6. The Origins of Its Neglect?
7. Impacts on Present-Day Debates in India
8. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- WHO|Neglected Tropical Diseases. Available online: http://www.who.int/neglected_diseases/diseases/en/ (accessed on 21 March 2020).
- Hotez, P.J.; Damania, A. India’s neglected tropical diseases. PLoS Negl. Trop. Dis. 2018, 12, e0006038. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanlon, C.A.; Childs, J.E. Chapter 3—Epidemiology. In Rabies, 3rd ed.; Jackson, A.C., Ed.; Academic Press: Boston, MA, USA, 2013; pp. 61–121. ISBN 978-0-12-396547-9. [Google Scholar]
- WHO. WHO Expert Consultation on Rabies: Third Report; Abela-Ridder, B., Ed.; World Health Organization: Geneva, Switzerland, 2018; ISBN 9789241210218. [Google Scholar]
- Sudarshan, M.K.; Madhusudana, S.N.; Mahendra, B.J.; Rao, N.S.N.; Ashwath Narayana, D.H.; Abdul Rahman, S.; Meslin, F.-X.; Lobo, D.; Ravikumar, K. Gangaboraiah Assessing the burden of human rabies in India: Results of a national multi-center epidemiological survey. Int. J. Infect. Dis. 2007, 11, 29–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gompper, M.E. Free-Ranging Dogs and Wildlife Conservation, 1st ed.; Gompper, M.E., Ed.; Oxford University Press: Oxford, UK, 2014; Volume 1, ISBN 9788578110796. [Google Scholar]
- Mani, R.S.; Willoughby, R.E. Human Rabies in South Asia. In Neglected Tropical Diseases—South Asia; Singh, S.K., Ed.; Springer International Publishing: Cham, Switzerland, 2017; pp. 349–371. ISBN 9783319684932. [Google Scholar]
- Mani, R.S.; Anand, A.M.; Madhusudana, S.N. Human rabies in India: An audit from a rabies diagnostic laboratory. Trop. Med. Int. Heal. 2016, 21, 556–563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diseases Under Surveillance: Integrated Disease Surveillance Programme (IDSP). Available online: http://www.idsp.nic.in/index1.php?lang=1&level=1&sublinkid=5985&lid=3925 (accessed on 3 August 2020).
- Baxter, J.M. One in a million, or one in thousand: What is the morbidity of rabies in India? J. Glob. Health 2012, 2, 1–4. [Google Scholar] [CrossRef]
- Suraweera, W.; Morris, S.K.; Kumar, R.; Warrell, D.A.; Warrell, M.J.; Jha, P. Deaths from Symptomatically Identifiable Furious Rabies in India: A Nationally Representative Mortality Survey. PLoS Negl. Trop. Dis. 2012, 6, e1847. [Google Scholar] [CrossRef] [Green Version]
- Masthi, N.R.; Pradeep, B.; Bilagumba, G. A multicentric community survey on animal exposures among humans in India. Indian J. Public Health 2019, 63, S9–S14. [Google Scholar] [CrossRef]
- National Plans: Planning Commission, Government of India. Available online: https://niti.gov.in/planningcommission.gov.in/docs/plans/planrel/index.php?state=planbody.htm (accessed on 30 July 2020).
- Bagcchi, S. India fights rabies. Lancet Infect. Dis. 2015, 15, 156–157. [Google Scholar] [CrossRef]
- Search|Open Government Data (OGD) Platform India. Available online: https://data.gov.in/search/site?query=rabies (accessed on 29 July 2020).
- Union Budget of India 2018–2019: Notes on Demands for Grants, Demand No. 42; Department of Health and Family Welfare: New Delhi, India, 2018; pp. 134–141.
- Union Budget of India 2019–2020: Notes on Demands for Grants, Demand No. 42; Department of Health and Family Welfare: New Delhi, India, 2019; pp. 136–143.
- Union Budget of India 2020–2021: Notes on Demands for Grants, Demand No. 42; Department of Health and Family Welfare: New Delhi, India, 2020; pp. 135–143.
- Chakrabarti, P. Bacteriology in British India: Laboratory Medicine and the Tropics; University of Rochester Press: Rochester, NY, USA, 2012; ISBN 9781580464086. [Google Scholar]
- Tarantola, A. Four Thousand Years of Concepts Relating to Rabies in Animals and Humans, Its Prevention and Its Cure. Trop. Med. Infect. Dis. 2017, 2, 5. [Google Scholar] [CrossRef] [Green Version]
- Wasik, B.; Murphy, M. Rabid—A Cultural History of the World’s Most Diabolical Virus; Penguin Books Ltd.: London, UK, 2012; ISBN 9780143123576. [Google Scholar]
- Parpia, S.A. Imperial Hunting Grounds: A New Reading of Mughal Cultural History. Ph.D. Thesis, The University of Adelaide, Adelaide, SA, Australia, 20 December 2018. [Google Scholar]
- Johnson, D. Sketches of Field Sports as Followed by the Natives of India with Observations on the Animals; Longman and Co.: London, UK, 1822; p. 261. [Google Scholar]
- Fayrer, J.; Balfour, J. Hydrophobia. Lancet 1877, 110, 785–786. [Google Scholar] [CrossRef]
- Destruction of Life by Snakes, Hydrophobia etc. in Western India, by an Ex-Commissioner; WH Allen and Co.: London, UK, 1880; p. 120.
- Vaughan, J. Canine Rabies in India. Ind. Med. Gaz. 1896, 31, 273–275. [Google Scholar] [CrossRef] [Green Version]
- Martin, E. Rabies in India. J. Comp. Pathol. Ther. 1895, 8, 207–212. [Google Scholar] [CrossRef]
- Benham, F.L. A collection of cases of hydrophobia reported as successfully treated. Lancet 1890, 135, 458–460. [Google Scholar] [CrossRef]
- Medicus. Rabies. Lancet 1829, 12, 459–461. [Google Scholar] [CrossRef]
- [Anonymous]. Vaidyapusthakam; Western Star Office: Cochin, India, 1876; p. 15. (In Malayalam) [Google Scholar]
- Pirkis, F. Results of the trial of the Buisson Bath treatment for rabies at Allahabad, Ferozepore and Sialkote 1898. India Office Records and Private Papers, British Library, IOR/P/5418 August 1898 nos 249-51: July 1898–August 1898. Available online: http://access.bl.uk/item/viewer/ark:/81055/vdc_100079495983.0x000001 (accessed on 20 October 2020).
- Collection 11/40—Inspection by Military Veterinary Subordinates Instead of Veterinary Officers of Dogs Suspected of Rabies; India Office Records and Private Papers; IOR/L/MIL/7/873; British Library: London, UK, 1914–1919.
- Mad Dogs. Times India (1861-Current), 7 October 1861; p. 2.
- A rabid dog: Four officers bitten. The Times of India (1861-Current), 23 May 1907; p. 8.
- Rabies among jackals. The Times of India (1861-Current), 7 February 1930; p. 14.
- Sirius. Hydrophobia in Dogs--Symptoms of. The Bombay Times and Journal of Commerce, 30 April 1859; p. 279. [Google Scholar]
- The mad dog. The Court Magazine and Belle Assemblee, July 1832–January 1837, Volume 9, pp. 27–38.
- Mad dogs. The Times of India (1861-Current), 21 July 1865; p. 4.
- Rabies in Bombay: To the editor of “The Times of India”. The Times of India (1861-Current), 11 September 1936; p. 20.
- Stray dogs in Calcutta: Corporation’s new plan. The Times of India (1861-Current), 23 May 1925; p. 14.
- Destruction of stray dogs in Poona. The Times of India (1861-Current), 1 March 1929; p. 7.
- Rabies in Bombay: A menace to the public. The Times of India (1861-Current), 14 April 1923; p. 12.
- Rabies in Bombay: Cases in Cumballa Hill District—To the editor of the Times of India. The Times of India (1861-Current), 27 August 1935; p. 16.
- WPP. II: To the editor of the Times of India. The Times of India (1861-Current), 6 February 1911; p. 7.
- 1895–1951—Annual Report of the Civil Veterinary Department, Bengal—Medicine—Veterinary > Civil Veterinary Departments—Medical History of British India—National Library of Scotland. Available online: https://digital.nls.uk/indiapapers/browse/archive/75719892 (accessed on 24 June 2020).
- (185) Page 17. Annual Report of the Civil Veterinary Department, Bengal and of the Bengal Veterinary College for the year 1935–1936. Available online: https://digital.nls.uk/indiapapers/browse/archive/77010889 (accessed on 22 July 2020).
- Pemberton, N.; Worboys, M. Mad Dogs and Englishmen; Palgrave Macmillan: London, UK, 2007; ISBN 978-1-349-35998-1. [Google Scholar]
- Field, J.; Prevost, F.; McCausland, G. Rabies in Bombay: To the editor of The Times of India. The Times of India (1861-Current), 4 February 1911; p. 8. [Google Scholar]
- Cave Canem: Rabies and Plague—To the editor of The Times of India. The Times of India (1861-Current), 28 February 1911; p. 8.
- Arnold, D. Colonizing the Body: State Medicine and Epidemic Disease in Nineteenth-Century India; University of California Press: Berkeley, CA, USA; Los Angeles, CA, USA, 1993. [Google Scholar]
- Kidambi, P. “An infection of locality”: Plague, pythogenesis and the poor in Bombay, c. 1896–1905. Urban History 2004, 31, 249–267. [Google Scholar] [CrossRef] [Green Version]
- Chattopadhyay, S. Representing Calcutta: Modernity, Nationalism and the Colonial Uncanny; Routledge: London, UK, 2005. [Google Scholar]
- Rabies vaccines: WHO position paper—April 2018. WHO Wkly. Epidemiol. Rec. 2018, 93, 201–220.
- Mackenzie, T. Proposed establishment of a Pasteur Institute in connection with the Bacteriological Laboratory at Poona 1892; India Office Records and Private Papers; IOR/P/4345 August 1893; British Library: London, UK, 1893; nos 79–87, pp. 327–355. [Google Scholar]
- Clive Webb, E. Rabies and its Control in India. Vet. J. 1911, 67, 157–166. [Google Scholar] [CrossRef]
- Patients for the Pasteur Institute. The Times of India (1861-Current), 5 April 1899; p. 5.
- Bitten by a rabid dog. The Times of India (1861-Current), 15 February 1899; p. 5.
- Fremantle, F. Health and Empire; John Ouseley Ltd.: London, UK, 1911. [Google Scholar]
- Cheema, G. Historical Notes: Rabies, Anti-Rabic Vaccine and the Raj. Indian J. Hist. Sci. 2015, 50, 514–520. [Google Scholar] [CrossRef]
- Guenther, R. Works of the East Indian Pasteur Institute for Hydrophobia in Kasauli, India. Public Heal. Rep. 1901, 16, 2446. [Google Scholar]
- East India (sanitary measures). Report on sanitary measures in India in 1912–1913. Vol. XLVI. 20th Century House of Commons Sessional Papers. 1914, 46. Available online: https://0-parlipapers-proquest-com.brum.beds.ac.uk/parlipapers/docview/t70.d75.1914-018116 (accessed on 20 October 2020).
- East India (sanitary measures). Report on sanitary measures in India in 1907–1908. Vol. XLI. 20th Century House of Commons Sessional Papers. 1909, 41. Available online: https://0-parlipapers-proquest-com.brum.beds.ac.uk/parlipapers/docview/t70.d75.1909-011353 (accessed on 20 October 2020).
- East India (sanitary measures). Report on sanitary measures in India 1914–1915. Vol. XLVIII. 20th Century House of Commons Sessional Papers. 1916, 48. Available online: https://0-parlipapers-proquest-com.brum.beds.ac.uk/parlipapers/docview/t70.d75.1916-020132 (accessed on 20 October 2020).
- Rabies in Bombay: To the editor of The Times of India from the Director, Bombay Bacteriological Laboratory. The Times of India (1861-Current), 4 October 1924; p. 15.
- Dutton, H. (66) Page 4. Annual Report of the Prince of Wales Medical College, Patna for the year 1928–1829. Available online: https://digital.nls.uk/indiapapers/browse/archive/74971598 (accessed on 15 July 2020).
- (274) Page 258. Regulations for the Medical Services of the Army in India. Available online: https://digital.nls.uk/indiapapers/browse/archive/74907253 (accessed on 15 July 2020).
- East India (sanitary measures). Report on sanitary measures in India in 1906–1907. Vol. XL. 20th Century House of Commons Sessional Papers. 1908, 40. Available online: https://0-parlipapers-proquest-com.brum.beds.ac.uk/parlipapers/docview/t70.d75.1908-010135 (accessed on 20 October 2020).
- Rabies Treatment in Southern India. Nature 1940, 145, 739. [CrossRef] [Green Version]
- Rabies in India. Nature 1961, 190, 678. [CrossRef]
- Annual Report 2015–2016—Pasteur Institute of India; Coonoor, India, 2017, p. 39. Available online: http://pasteurinstituteindia.com/annual.html (accessed on 20 October 2020).
- Pasteur Institute of India, Kasauli—The fourteenth annual report of the Central Committee of the Association Together with the Report of the Directors of the Institute for the Year Ending 31st December 1914. Available online: https://digital.nls.uk/indiapapers/browse/archive/74947969 (accessed on 28 July 2020).
- Porter, L. Proposals for the Collection of Statistics of Persons Bitten by Rabid Animals; India Office Records and Private Papers; IOR/P/8955 Jan 1912; British Library: London, UK, 1912; nos 14–15; pp. 3–11. [Google Scholar]
- (1) Front Cover. Annual administration report of the Civil Veterinary Department, Madras Presidency, 1926–1933. Available online: https://digital.nls.uk/indiapapers/browse/archive/75692280 (accessed on 24 June 2020).
- Webster, W. Rabies and Anti-Rabic Treatment in India; Govt. India Press: Simla, India, 1946; p. 17. [Google Scholar]
- Greig, E. Rabies and Anti-Rabic Treatment in India 1921; Superintendent, Government Printing: Rangoon, Burma, India, 1921; p. 16. [Google Scholar]
- Pasteur Institute in India: Most bites by dogs. The Times of India (1861-Current), 5 July 1928; p. 13.
- Pratik Chakrabarti “Living versus Dead”: The Pasteurian Paradigm and Imperial Vaccine Research. Bull. Hist. Med. 2010, 84, 387–423. [CrossRef] [PubMed] [Green Version]
- Semple, D. The Preparation of a Safe and Efficient Antirabic Vaccine; Scientific Memoirs by Officers of the Medical and Sanitary Departments of the Government of India: Calcutta, India, 1911. [Google Scholar]
- Taylor, L.H.; Costa, P.; Briggs, D.J. Chapter 15—Public Health Management of Humans at Risk. In Rabies, 3rd ed.; Jackson, A.C., Ed.; Academic Press: Boston, MA, USA, 2013; pp. 543–573. ISBN 978-0-12-396547-9. [Google Scholar]
- Rupprecht, C.E.; Nagarajan, T.; Ertl, H. Rabies Vaccines. In Plotkin’s Vaccines; Elsevier: Philadelphia, PA, USA, 2018; pp. 918–942.e12. [Google Scholar]
- Chakrabarti, P. Pasteurian Paradigm and Vaccine Research in India. In Bacteriology in British India; Chakrabarti, P., Ed.; Laboratory Medicine and the Tropics; Boydell and Brewer Limited: Suffolk, UK, 2012; Volume 22, pp. 142–178. ISBN 9781580464086. [Google Scholar]
- Bradfield, E. (251) [Page] 239. An Indian Medical Review. Available online: https://digital.nls.uk/indiapapers/browse/archive/74941238 (accessed on 14 July 2020).
- Palsetia, J.S. Mad Dogs and Parsis: The Bombay Dog Riots of 1832. J. R. Asiat. Soc. 2001, 11, 13–30. [Google Scholar] [CrossRef]
- (160) Page 94. Proceedings of the Second Meeting of Veterinary Officers in India, Calcutta. 1923. Available online: https://digital.nls.uk/indiapapers/browse/archive/75515450 (accessed on 23 June 2020).
- Bombay corporation: Destruction of stray dog. The Times of India (1861-Current), 2 January 1912; p. 4.
- The proposed dog tax: To the editor of The Times of India. The Times of India (1861-Current), 6 December 1887; p. 4.
- Simla municipality: Campaign against jackals. The Times of India (1861-Current), 12 September 1907; p. 7.
- (1) Front Cover. Annual report of the Punjab Veterinary College and of the Civil Veterinary Department, Punjab, 1909–1919. Available online: https://digital.nls.uk/indiapapers/browse/archive/75528073 (accessed on 24 June 2020).
- Indian notes and news: Simla electric supply, Campaign against jackals, Employment abroad, To purify water, The Mahomedan position, Calcutta ferry service. The Times of India (1861-Current), 27 April 1909; p. 8.
- McLean, F. An appeal to dog-lovers: To the editor of The Times of India. The Times of India (1861-Current), 7 April 1919; p. 8. [Google Scholar]
- Rabies in India. Lancet 1910, 175, 116–117. [CrossRef]
- (266) Page 9. Annual Report of the Civil Veterinary Department Bihar and Orissa for the Year 1926–1927. Available online: https://digital.nls.uk/indiapapers/browse/archive/75903625 (accessed on 22 July 2020).
- Suppression of rabies. The Times of India (1861-Current), 20 May 1912; p. 8.
- Rabies menace in India: Need for control measures. The Times of India (1861-Current), 26 March 1935; p. 3.
- (158) Page 139. Annual Administration Report of the Civil Veterinary Department of India for the Official Year 1898–1899. Available online: https://digital.nls.uk/indiapapers/browse/archive/75506674 (accessed on 21 July 2020).
- (24) Page 17. Annual Administration Report of the Civil Veterinary Department in India for the Official Year 1908–1909. Available online: https://digital.nls.uk/indiapapers/browse/archive/75509882 (accessed on 23 July 2020).
- (1) Front Cover—Medicine—Veterinary > Civil Veterinary Departments > Proceedings of the meeting of veterinary officers in India—Medical History of British India—National Library of Scotland. Available online: https://digital.nls.uk/indiapapers/browse/archive/75514868 (accessed on 23 June 2020).
- The etiology and prevention of rabies. BMJ 1924, 1, 1059–1063. [CrossRef]
- Kurosawa, A.; Tojinbara, K.; Kadowaki, H.; Hampson, K.; Yamada, A.; Makita, K. The rise and fall of rabies in Japan: A quantitative history of rabies epidemics in Osaka Prefecture, 1914–1933. PLoS Negl. Trop. Dis. 2017, 11, e0005435. [Google Scholar] [CrossRef]
- (324) Page 6. Annual Report on the Punjab Veterinary College, Civil Veterinary Department, Punjab and the Government Cattle Farm, Hissar for the year 1915–1916. Available online: https://digital.nls.uk/indiapapers/browse/archive/75532277 (accessed on 25 June 2020).
- (300) Page 22. Annual Report of the Punjab Veterinary College, Civil Veterinary Department, Punjab, and the Government cattle Farm, Hissar for the Year 1922–1923. Available online: https://digital.nls.uk/indiapapers/browse/archive/75536082 (accessed on 15 July 2020).
- (1) Front Cover. Annual Administration report of the Civil Veterinary Department, Madras Presidency, 1910–1925. Available online: https://digital.nls.uk/indiapapers/browse/archive/75692279 (accessed on 23 June 2020).
- (1) Front cover—Medicine—Veterinary > Civil Veterinary Departments > 1911–1950—Report of the Civil Veterinary Department, Assam > Civil Veterinary Dept. Assam report 1911–1927—Medical History of British India—National Library of Scotland. Available online: https://digital.nls.uk/indiapapers/browse/archive/75722238 (accessed on 24 June 2020).
- 1937–1946—Annual Administration Report of the Civil Veterinary Department, Sind—Medicine—Veterinary > Civil Veterinary Departments—Medical History of British India—National Library of Scotland. Available online: https://digital.nls.uk/indiapapers/browse/archive/75648798 (accessed on 24 June 2020).
- (1) Front cover—Medicine—Veterinary > Civil Veterinary Departments > 1914–1940—Annual administration report of the Civil Veterinary Department, Ajmere-Merwara, British Rajputana—Medical History of British India—National Library of Scotland. Available online: https://digital.nls.uk/indiapapers/browse/archive/75645666 (accessed on 24 June 2020).
- Pinnell, L. Order under sec. 144 CrPC about muzzling of dogs issued in 1933—Memo No. 9719 G dtd. 11/12/1944. In Mss Eur D911: Papers of Leonard George Pinnell, Indian Civil Service, Bengal; India Office Records and Private Papers; British Library: London, UK, 1932–1948. [Google Scholar]
- Rabies Prevention in India. Nature 1938, 141, 72–73. [CrossRef] [Green Version]
- Pasteur Institute of Southern India. Nature 1950, 166, 257. [CrossRef]
- Animal diseases: Veterinary conference. The Times of India (1861-Current), 21 March 1923; p. 12.
- Young India, 1924–1926 by Mahatma Gandhi. Available online: https://dspace.gipe.ac.in/xmlui/handle/10973/33432 (accessed on 8 October 2020).
- (379) Page 5. Annual Administration Report of the Civil Veterinary Department, Madras Presidency for 1923–1924. Available online: https://digital.nls.uk/indiapapers/browse/archive/75699874 (accessed on 22 July 2020).
- (360) Page 12. Annual Administration Report of the Civil Veterinary Department, Madras Presidency for 1922–1923. Available online: https://digital.nls.uk/indiapapers/browse/archive/75699817 (accessed on 21 July 2020).
- (48) Page 19. Report on the Operations of the Civil Veterinary Department, Madras. Recording, with Remarks, during 1911–1912. Available online: https://digital.nls.uk/indiapapers/browse/archive/75698863 (accessed on 21 July 2020).
- (371) Page 63. Annual Administration Report of the Madras Civil Veterinary Department for the year 1928–1929. Available online: https://digital.nls.uk/indiapapers/browse/archive/75718016 (accessed on 21 July 2020).
- (53) Page 7. Annual Report of the Civil Veterinary Department Bihar and Orissa for the year 1923–1924. Available online: https://digital.nls.uk/indiapapers/browse/archive/75900869 (accessed on 23 July 2020).
- (59) Page 7. Report on the Civil Veterinary Department North-West Frontier Province, for the year 1933–1934. Available online: https://digital.nls.uk/indiapapers/browse/archive/75546705 (accessed on 22 July 2020).
- (81) Page 3. Annual Administration Report of the Civil Veterinary Department in the Bombay Presidency for the Official Year 1899–1900. Available online: https://digital.nls.uk/indiapapers/browse/archive/75678945 (accessed on 23 July 2020).
- (876) Page 23. Annual Administration Report of the Madras Civil Veterinary Department for the Year 1932–1933. Available online: https://digital.nls.uk/indiapapers/browse/archive/75719584 (accessed on 23 July 2020).
- Chakrabarti, P. Medicine and Empire: 1600–1960; Palgrave Macmillan Ltd.: Basingstoke, UK, 2013; ISBN 1137374802. [Google Scholar]
- Vaccinating Dogs. The Times of India (1861-Current), 7 December 1926; p. 8.
- Victims, O. Of the Rabid Dogs. The Times of India (1861-Current), 25 November 1940; p. 6. [Google Scholar]
- Russell, A.J.H. The Vitality of the Peoples of Southern India, its Conservation and Promotion. Sci. Mon. 1926, 23, 54–64. [Google Scholar]
- East India (sanitary measures). Report of sanitary measures in India in 1915–1916. Vol. XLIX. 20th Century House of Commons Sessional Papers. 1918, 49. Available online: https://0-parlipapers-proquest-com.brum.beds.ac.uk/parlipapers/docview/t70.d75.1917-020945 (accessed on 20 October 2020).
- Report on sanitary measures in India in 1879–80: Together with miscellaneous information up to June 1881. 19th Century House of Commons Sessional Papers. 1881, 13. 1881, 13. Available online: https://0-parlipapers-proquest-com.brum.beds.ac.uk/parlipapers/docview/t70.d75.1881-057412 (accessed on 20 October 2020).
- Report on sanitary measures in India in 1885–6: Together with miscellaneous information up to June 1887. 19th Century House of Commons Sessional Papers. 1887, 19. 1887, 19. Available online: https://0-parlipapers-proquest-com.brum.beds.ac.uk/parlipapers/docview/t70.d75.1887-063651 (accessed on 20 October 2020).
- East India (sanitary measures). Report on sanitary measures in India in 1909–1910. Vol. XLIII. 20th Century House of Commons Sessional Papers. 1911, 43. Available online: https://0-parlipapers-proquest-com.brum.beds.ac.uk/parlipapers/docview/t70.d75.1911-013831 (accessed on 20 October 2020).
- East India (sanitary measures). Report on sanitary measures in India in 1910–1911. Vol. XLIV. 20th Century House of Commons Sessional Papers. 1912, 44. Available online: https://0-parlipapers-proquest-com.brum.beds.ac.uk/parlipapers/docview/t70.d75.1912-015414 (accessed on 20 October 2020).
- East India (sanitary measures). Report on sanitary measures in India in 1908–1909. Vol. XLII. 20th Century House of Commons Sessional Papers. 1910, 42. Available online: https://0-parlipapers-proquest-com.brum.beds.ac.uk/parlipapers/docview/t70.d75.1910-012721 (accessed on 20 October 2020).
- East India (sanitary measures). Report on sanitary measures in India in 1913–1914. Vol. XLVII. 20th Century House of Commons Sessional Papers. 1915, 47. 1915, 47. Available online: https://0-parlipapers-proquest-com.brum.beds.ac.uk/parlipapers/docview/t70.d75.1914-019382 (accessed on 20 October 2020).
- East India (sanitary measures). Report on sanitary measures in India in 1911–1912. Vol. XLV. 20th Century House of Commons Sessional Papers. 1913, 45. Available online: https://0-parlipapers-proquest-com.brum.beds.ac.uk/parlipapers/docview/t70.d75.1914-017723 (accessed on 20 October 2020).
- Ministry of Health. Annual report of the Chief Medical Officer, 1919–1920. 20th Century House of Commons Sessional Papers. 1920. Available online: https://0-parlipapers-proquest-com.brum.beds.ac.uk/parlipapers/docview/t70.d75.1920-023861 (accessed on 20 October 2020).
- (113) Page 47. Proceedings of the Second Meeting of Veterinary Officers in India, Calcutta. 1923. Available online: https://digital.nls.uk/indiapapers/browse/archive/75515291 (accessed on 28 July 2020).
- HARRISON, M. A Dreadful Scourge: Cholera in early nineteenth-century India. Mod. Asian Stud. 2020, 54, 502–553. [Google Scholar] [CrossRef] [Green Version]
- Pasteur Institute of India, Kasauli. Nature 1935, 136, 677. [CrossRef] [Green Version]
- Anti-Rabic Treatment in India. Nature 1939, 144, 148. [CrossRef] [Green Version]
- Brown, K.; Gilfoyle, D. Healing the Herds; Brown, K., Gilfoyle, D., Eds.; Ohio University Press: Athens, Ohio, USA, 2010; ISBN 9780821443101. [Google Scholar]
- East India (statistical abstract). Statistical abstract for British India with statistics, where available, relating to certain Indian States from 1926-27 to 1935–36 sixty-ninth number (fourteenth number of new series). 20th Century House of Commons Sessional Papers. 1938, 69. Available online: https://0-parlipapers-proquest-com.brum.beds.ac.uk/parlipapers/docview/t70.d75.1937-035559 (accessed on 20 October 2020).
- East India (progress and condition). Statement exhibiting the moral and material progress and condition of India during the year 1929–30. Sixty-fifth number. 20th Century House of Commons Sessional Papers. 1931, 65. Available online: https://0-parlipapers-proquest-com.brum.beds.ac.uk/parlipapers/docview/t70.d75.1930-030809 (accessed on 20 October 2020).
- Veeraraghavan, N.; Subrahmanyan, T. The value of duck-embryo vaccine and high-egg-passage Flury vaccine in experimental rabies infection in guinea pigs. Bull. World Health Organ. 1963, 29, 323–330. [Google Scholar]
- (563) Page 3. Report of the Civil Veterinary Department, North-West Frontier Province for the year 1921–1922. Available online: https://digital.nls.uk/indiapapers/browse/archive/75545198 (accessed on 23 July 2020).
- Del Rio Vilas, V.J.; Freire de Carvalho, M.J.; Vigilato, M.A.N.; Rocha, F.; Vokaty, A.; Pompei, J.A.; Molina Flores, B.; Fenelon, N.; Cosivi, O. Tribulations of the Last Mile: Sides from a Regional Program. Front. Vet. Sci. 2017, 4, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polu, S.L. Malaria—India’s True Plague. In Infectious Disease in India, 1892–1940; Palgrave Macmillan: London, UK, 2012; pp. 82–118. [Google Scholar]
- Rahman, S.A.; Isloor, S. Rabies on the Indian subcontinent. Rev. Sci. Tech. L’OIE 2018, 37, 529–542. [Google Scholar] [CrossRef]
- Venkataraman, L. India Is Far behind Sri Lanka and Bangladesh in Rabies Prevention. Available online: https://www.telegraphindia.com/opinion/india-is-far-behind-sri-lanka-and-bangladesh-in-rabies-prevention/cid/1690048 (accessed on 30 July 2020).
- Census of India: Variation in Population Since 1901. Available online: https://www.censusindia.gov.in/Census_Data_2001/India_at_glance/variation.aspx (accessed on 30 July 2020).
- Tiwari, H.K.; Robertson, I.D.; O’Dea, M.; Vanak, A.T. Knowledge, attitudes and practices (KAP) towards rabies and free roaming dogs (FRD) in Panchkula district of north India: A cross-sectional study of urban residents. PLoS Negl. Trop. Dis. 2019, 13, e0007384. [Google Scholar] [CrossRef]
- Kakkar, M.; Ramani, S.; Menon, G.; Sankhe, L.; Gaidhane, A.; Krishnan, S. ‘Zoonoses? Not sure what that is…’ An assessment of knowledge of zoonoses among medical students in India. Trans. R. Soc. Trop. Med. Hyg. 2011, 105, 254–261. [Google Scholar] [CrossRef]
- Animal Birth Control (Dogs) Rules, 2001; Animal Welfare Board of India: Chennai, India, 2001; p. 7.
- Kudumbashree|ABC Programme. Available online: http://www.kudumbashree.org/pages/216 (accessed on 20 May 2018).
- George, A.; Kumar, K.J.K. ABC- ARV Program, Corporation of Koch; Corporation of Kochi: Kerala, India, 2014. [Google Scholar]
- Reece, J.F.; Chawla, S.K. Control of rabies in Jaipur, India, by the sterilisation and vaccination of neighbourhood dogs. Vet. Rec. 2006, 159, 379–383. [Google Scholar] [CrossRef] [Green Version]
- Lenin, J.; Uniyal, M.; Vanak, A.T. Do Dogs Threaten People’s Right to Safety in Public Spaces? Available online: https://thewire.in/health/dogs-rabies-neutering-safety (accessed on 4 September 2020).
- Revised Module for Street Dog Population Management, Rabies Eradication, Reducing Man-Dog Conflict; Animal Welfare Board of India: Chennai, India, 2016; p. 308.
- At Least 120 Stray Dogs Killed in Kerala’s Ernakulam and Palakkad Districts in the Last Week. Available online: https://scroll.in/latest/819045/at-least-120-stray-dogs-killed-in-keralas-ernakulam-and-palakkad-districts-in-the-last-week (accessed on 7 October 2020).
- In a Horrifying Incident, Kerala Congress Activists Kill Dogs, Hang Them on Poles—The Financial Express. Available online: https://www.financialexpress.com/india-news/in-a-horrifying-incident-kerala-congress-activists-kill-dogs-hang-them-on-poles/393946/ (accessed on 7 October 2020).
- Srinivasan, K.; Kurz, T.; Kuttuva, P.; Pearson, C. Reorienting rabies research and practice: Lessons from India. Palgrave Commun. 2019, 5, 152. [Google Scholar] [CrossRef]
- Collinson, A.; Bennett, M.; Brennan, M.L.; Dean, R.S.; Stavisky, J. Evaluating the role of surgical sterilisation in canine rabies control: A systematic review of impact and outcomes. PLoS Negl. Trop. Dis. 2020, 14, e0008497. [Google Scholar] [CrossRef]
- Wang, J. Mad Dogs and Other New Yorkers: Rabies, Medicine, and Society in an American Metropolis, 1840–1920; Johns Hopkins University Press: Baltimore, MD, USA, 2019; ISBN 9781421409726. [Google Scholar]
- Vanak, A.T.; Home, C. Unpacking the ‘canine conundrum’. Anim. Conserv. 2018, 21, 289–290. [Google Scholar] [CrossRef] [Green Version]
- Bhalla, S.; Vanak, A.T. Killing with Compassion: Why Feeding Dogs in Public Places Must Stop! Available online: https://www.downtoearth.org.in/blog/wildlife-biodiversity/killing-with-compassion-why-feeding-dogs-in-public-places-must-stop--72092 (accessed on 4 September 2020).
- Nadal, D. Rabies in the Streets; Penn State University Press: University Park, PA, USA, 2020; Volume 16, ISBN 9780271085951. [Google Scholar]
- Rabies kills tens of thousands yearly. Vaccinating dogs could stop it. The New York Times. Available online: https://www.nytimes.com/2019/07/22/science/rabies-dogs-india.html (accessed on 18 October 2020).
- Thiagarajan, K. Man bites dog: India’s progress in tackling rabies. BMJ 2020, 368, l6979. [Google Scholar] [CrossRef] [PubMed]
- Byrnes, H.; Britton, A.; Bhutia, T. Eliminating Dog-Mediated Rabies in Sikkim, India: A 10-Year Pathway to Success for the SARAH Program. Front. Vet. Sci. 2017, 4, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cherian, V.; Dugg, P.; Khan, A.M. Prevalence of pet dog ownership in an urban colony of East Delhi and awareness regarding canine zoonotic diseases and responsible pet ownership among dog owners. Indian J. Community Med. 2020, 45, 89–91. [Google Scholar] [CrossRef] [PubMed]
- Radhakrishnan, S.; Vanak, A.T.; Nouvellet, P.; Donnelly, C.A. Population characteristics of owned and unowned dogs at two urban locations in Kerala, India. 2020; unpublished; manuscript in preparation. [Google Scholar]
- Wentworth, D.; Hampson, K.; Thumbi, S.M.; Mwatondo, A.; Wambura, G.; Chng, N.R. A social justice perspective on access to human rabies vaccines. Vaccine 2019, 37, A3–A5. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, M.C.; Shah, H.A.; Pandey, A.; Bilinski, A.M.; Kakkar, M.; Clark, A.D.; Townsend, J.P.; Abbas, S.S.; Galvani, A.P. One Health approach to cost-effective rabies control in India. Proc. Natl. Acad. Sci. USA 2016, 113, 14574–14581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mindekem, R.; Lechenne, M.S.; Naissengar, K.S.; Oussiguere, A.; Kebkiba, B.; Moto, D.D.; Alfaroukh, I.O.; Ouedraogo, L.T.; Salifou, S.; Zinsstag, J. Cost Description and Comparative Cost Efficiency of Post-Exposure Prophylaxis and Canine Mass Vaccination against Rabies in N’Djamena, Chad. Front. Vet. Sci. 2017, 4, 38. [Google Scholar] [CrossRef] [PubMed]
- Yasobant, S.; Saxena, D.; Bruchhausen, W.; Memon, F.Z.; Falkenberg, T. Multi-sectoral prioritization of zoonotic diseases: One health perspective from Ahmedabad, India. PLoS ONE 2019, 14, e0220152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sekar, N.; Shah, N.K.; Abbas, S.S.; Kakkar, M. Research Options for Controlling Zoonotic Disease in India, 2010–2015. PLoS ONE 2011, 6, e17120. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Year | Numbers Treated (Number of Deaths) | Reference | ||
|---|---|---|---|---|
| European | Native/Indian | Total | ||
| 1900–1901 1 | 146 (1) | 175 (9) | 321 (10) | [130] |
| 1901–1902 1 | 215 (2) | 328 (11) | 543 (13) | [130] |
| 1902–1903 1 | 269 (1) | 315 (12) | 584 (12) | [130] |
| 1903–1904 1 | 248 (0) | 364 (10) | 612 (10) | [130] |
| 1904–1905 1 | 307 (0) | 570 (12) | 877 (12) | [130] |
| 1905–1906 1 | 342 (2) | 803 (19) | 1145 (21) | [130] |
| 1906–1907 1 | 452 (2) | 846 (17) | 1308 (19) | [130] |
| Interim, 09/08–31/12, 1907 1 | 146 (1) | 373 (4) | 519 (5) | [130] |
| 1908 2 | 342 (2) | 1047 (24) | 1729 (26) | [128,130] |
| 1909 2 | 675 (3) | 1920 (25) | 2595 (28) | [126,130] |
| 1910 2 | 575 (0) | 2325 (43) | 2900 (43) | [127,130] |
| 1911 2 | 297(1) | 2911 (50) | 3208 (51) | [130] |
| 1912 2 | 400 (0) | 4388 (59) | 4788 (59) | [61] |
| 1913 2 | 2 (2) | 5271 (66) | 5273 (68) | [129] |
| 1914 2 | NA (1) | NA (60) | 5795 (61) | [63] |
| 1915 2 | 468 (1) | 6409 (41) | 6877 (42) | [123] |
| 1933 1 | 1356 (0) | 14,582 (83) | 15,938 (83) | [134] |
| 1936 1 | 1357 (0) | NA (97) | NA (97) | [135] |
| 1938 3 | NA (NA) | NA (NA) | 12,396 (21) | [68] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Radhakrishnan, S.; Vanak, A.T.; Nouvellet, P.; Donnelly, C.A. Rabies as a Public Health Concern in India—A Historical Perspective. Trop. Med. Infect. Dis. 2020, 5, 162. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed5040162
Radhakrishnan S, Vanak AT, Nouvellet P, Donnelly CA. Rabies as a Public Health Concern in India—A Historical Perspective. Tropical Medicine and Infectious Disease. 2020; 5(4):162. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed5040162
Chicago/Turabian StyleRadhakrishnan, Sreejith, Abi Tamim Vanak, Pierre Nouvellet, and Christl A. Donnelly. 2020. "Rabies as a Public Health Concern in India—A Historical Perspective" Tropical Medicine and Infectious Disease 5, no. 4: 162. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed5040162