Measurement of Head Circumference: Implications for Microcephaly Surveillance in Zika-Affected Areas

 , , , , add
Show full author list
, , , , add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Teixeira, M.G.; da Conceicao, N.C.M.; de Oliveira, W.K.; Nunes, M.L.; Rodrigues, L.C. The Epidemic of Zika Virus-Related Microcephaly in Brazil: Detection, Control, Etiology, and Future Scenarios. Am. J. Public Health 2016, 106, 601–605. [Google Scholar] [CrossRef]
- DeSilva, M.; Munoz, F.M.; Sell, E.; Marshall, H.; Tse Kawai, A.; Kachikis, A.; Heath, P.; Klein, N.P.; Oleske, J.M.; Jehan, F.; et al. Congenital microcephaly: Case definition & guidelines for data collection, analysis, and presentation of safety data after maternal immunisation. Vaccine 2017, 35, 6472–6482. [Google Scholar] [CrossRef]
- Silva, A.A.; Barbieri, M.A.; Alves, M.T.; Carvalho, C.A.; Batista, R.F.; Ribeiro, M.R.; Lamy-Filho, F.; Lamy, Z.C.; Cardoso, V.C.; Cavalli, R.C.; et al. Prevalence and Risk Factors for Microcephaly at Birth in Brazil in 2010. Pediatrics 2018, 141. [Google Scholar] [CrossRef] [Green Version]
- Graham, K.A.; Fox, D.J.; Talati, A.; Pantea, C.; Brady, L.; Carter, S.L.; Friedenberg, E.; Vora, N.M.; Browne, M.L.; Lee, C.T. Prevalence and Clinical Attributes of Congenital Microcephaly-New York, 2013–2015. MMWR Morb. Mortal. Wkly. Rep. 2017, 66, 125–129. [Google Scholar] [CrossRef]
- Morris, J.K.; Rankin, J.; Garne, E.; Loane, M.; Greenlees, R.; Addor, M.C.; Arriola, L.; Barisic, I.; Bergman, J.E.; Csaky-Szunyogh, M.; et al. Prevalence of microcephaly in Europe: Population based study. BMJ 2016, 354, i4721. [Google Scholar] [CrossRef] [Green Version]
- Candelo, E.; Caicedo, G.; Feinstein, M.M.; Pachajoa, H. Microcephaly in Colombia before the Zika outbreak: A systematic literature review. Biomedica 2018, 38, 127–134. [Google Scholar] [CrossRef]
- Orioli, I.M.; Dolk, H.; Lopez-Camelo, J.S.; Mattos, D.; Poletta, F.A.; Dutra, M.G.; Carvalho, F.M.; Castilla, E.E. Prevalence and clinical profile of microcephaly in South America pre-Zika, 2005–2014: Prevalence and case-control study. BMJ 2017, 359, j5018. [Google Scholar] [CrossRef] [Green Version]
- Harville, E.W.; Buekens, P.M.; Cafferata, M.L.; Gilboa, S.; Tomasso, G.; Tong, V. Measurement error, microcephaly prevalence and implications for Zika: An analysis of Uruguay perinatal data. Arch. Dis. Child. 2020, 105, 428–432. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Measuring Head Circumference. Available online: https://www.cdc.gov/zika/pdfs/microcephaly_measuring.pdf (accessed on 12 October 2019).
- Villar, J.; Cheikh Ismail, L.; Victora, C.G.; Ohuma, E.O.; Bertino, E.; Altman, D.G.; Lambert, A.; Papageorghiou, A.T.; Carvalho, M.; Jaffer, Y.A.; et al. International standards for newborn weight, length, and head circumference by gestational age and sex: The Newborn Cross-Sectional Study of the INTERGROWTH-21st Project. Lancet 2014, 384, 857–868. [Google Scholar] [CrossRef]
- International Fetal and Newborn Growth Consortium. INTERGROWTH-21st International Fetal and Newborn Growth Standards for the 21st Century Anthropometry Handbook; University of Oxford: Oxford, UK, 2012. [Google Scholar]
- Wright, C.M.; Bremner, M.; Lip, S.; Symonds, J.D. Does measurement technique explain the mismatch between European head size and WHO charts? Arch. Dis. Child. 2017, 102, 639–643. [Google Scholar] [CrossRef]
- Bartram, J.L.; Rigby, A.S.; Baxter, P.S. The “Lasso-o” tape: Stretchability and observer variability in head circumference measurement. Arch. Dis. Child. 2005, 90, 820–821. [Google Scholar] [CrossRef]
- Zerfas, A.J. The insertion tape: A new circumference tape for use in nutritional assessment. Am. J. Clin. Nutr. 1975, 28, 782–787. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. National Health and Nutrition Examination Series (NHANES) Anthropometry Proced. Man; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2009; p. 39. [Google Scholar]
- Bradley, J.L.; Brown, J.E.; Himes, J.H. Reliability and validity of parental measurements of infant size. Am. J. Hum. Biol. 2001, 13, 275–279. [Google Scholar] [CrossRef]
- Magalhaes-Barbosa, M.C.; Prata-Barbosa, A.; Robaina, J.R.; Raymundo, C.E.; Lima-Setta, F.; Cunha, A. New trends of the microcephaly and Zika virus outbreak in Brazil, July 2016–December 2016. Travel Med. Infect. Dis. 2017, 16, 52–57. [Google Scholar] [CrossRef]
- Bragazzi, N.L.; Alicino, C.; Trucchi, C.; Paganino, C.; Barberis, I.; Martini, M.; Sticchi, L.; Trinka, E.; Brigo, F.; Ansaldi, F.; et al. Global reaction to the recent outbreaks of Zika virus: Insights from a Big Data analysis. PLoS ONE 2017, 12, e0185263. [Google Scholar] [CrossRef] [Green Version]
- Duarte Dos Santos, C.N.; Goldenberg, S. Zika Virus and Microcephaly: Challenges for a Long-Term Agenda. Trends Parasitol 2016, 32, 508–511. [Google Scholar] [CrossRef] [Green Version]
- Buekens, P.; Alger, J.; Althabe, F.; Bergel, E.; Berrueta, A.M.; Bustillo, C.; Cafferata, M.L.; Harville, E.; Rosales, K.; Wesson, D.M.; et al. Zika virus infection in pregnant women in Honduras: Study protocol. Reprod. Health 2016, 13, 82. [Google Scholar] [CrossRef] [Green Version]
- Research Capacity Network. INTERGROWTH-21st. Available online: https://rede.tghn.org/training/intergrowth-21-training-rede/ (accessed on 14 October 2020).
- Latin American Center of Perinatology Women and Reproductive Health. Sistema Informatico Perinatal. Available online: https://paho.org/clap/index.php?option=com_content&view=article&id=84:sistema-informatico-perinatal&Itemid=242&lang=en (accessed on 6 July 2018).
- Ministerio de Desarrollo Social (MIDES). Evaluacion del Crecimiento del Nino y la Nina Desde el Nacimiento Hasta los 5 Anos de Edad [Evaluation of Growth of the Boy and Girl, from 5 to Five Years of Age]. 2016. Available online: https://www.gub.uy/ministerio-salud-publica/sites/ministerio-salud-publica/files/documentos/publicaciones/Guia%20evaluaci%C3%B3n%20crecimiento%200%20a%205%20a%C3%B1os.pdf (accessed on 18 November 2020).
- Capurro, H.; Konichezky, S.; Fonseca, D.; Caldeyro-Barcia, R. A simplified method for diagnosis of gestational age in the newborn infant. J. Pediatr. 1978, 93, 120–122. [Google Scholar] [CrossRef]
- Conkle, J.; Ramakrishnan, U.; Flores-Ayala, R.; Suchdev, P.S.; Martorell, R. Improving the quality of child anthropometry: Manual anthropometry in the Body Imaging for Nutritional Assessment Study (BINA). PLoS ONE 2017, 12, e0189332. [Google Scholar] [CrossRef]
- Cheikh Ismail, L.; Knight, H.E.; Ohuma, E.O.; Hoch, L.; Chumlea, W.C. Anthropometric standardisation and quality control protocols for the construction of new, international, fetal and newborn growth standards: The INTERGROWTH-21st Project. BJOG 2013, 120 (Suppl. 2), 48–55. [Google Scholar] [CrossRef] [Green Version]
- Kalmin, M.M.; Gower, E.W.; Stringer, E.M.; Bowman, N.M.; Rogawski McQuade, E.T.; Westreich, D. Misclassification in defining and diagnosing microcephaly. Paediatr. Perinat. Epidemiol. 2019, 33, 286–290. [Google Scholar] [CrossRef]
- Hay, J.A.; Nouvellet, P.; Donnelly, C.A.; Riley, S. Potential inconsistencies in Zika surveillance data and our understanding of risk during pregnancy. PLoS Negl. Trop. Dis. 2018, 12, e0006991. [Google Scholar] [CrossRef] [Green Version]
- Ospina, M.L.; Tong, V.T.; Gonzalez, M.; Valencia, D.; Mercado, M.; Gilboa, S.M.; Rodriguez, A.J.; Tinker, S.C.; Rico, A.; Winfield, C.M.; et al. Zika Virus Disease and Pregnancy Outcomes in Colombia. N. Engl. J. Med. 2020, 383, 537–545. [Google Scholar] [CrossRef]
- Foote, J.M.; Hanrahan, K.; Mulder, P.J.; Nielsen, A.K.; Perkhounkova, Y.; Hein, M.; Saeidzadeh, S.; McCarthy, A.M. Growth Measurement Practices from a National Survey of Neonatal Nurses. J. Pediatr. Nurs. 2020, 52, 10–17. [Google Scholar] [CrossRef]
- Yin, H.; Dai, Y.; Li, H.; Xie, X.; Ren, H. The test-re-test reliability of routine infant anthropometry at primary care hospitals in Chongqing, PR China. Ann. Hum. Biol. 2013, 40, 309–317. [Google Scholar] [CrossRef]
- Lipman, T.H.; Hench, K.D.; Benyi, T.; Delaune, J.; Gilluly, K.A.; Johnson, L.; Johnson, M.G.; McKnight-Menci, H.; Shorkey, D.; Shults, J.; et al. A multicentre randomised controlled trial of an intervention to improve the accuracy of linear growth measurement. Arch. Dis. Child. 2004, 89, 342–346. [Google Scholar] [CrossRef] [Green Version]
- Gerver, W.J.; Gidding, C.; van Amstel, M.; Vles, J.S. A new device to measure short-term growth of head circumference in newborn infants. Eur. J. Pediatr. 1990, 149, 768–770. [Google Scholar] [CrossRef]
- Tirosh, E.; Weinger, M.A.; Berger, A.; Cohen, A. Biparietal diameter: An alternative measure of head growth in the low-birthweight infant. J. Med. Eng. Technol. 1992, 16, 79–81. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Women | ||
|---|---|---|
| n | % | |
| Maternal Variables | ||
| Maternal age in years (n = 667) | ||
| 12–19 | 198 | 29.7% |
| 20–34 | 404 | 60.6% |
| 35 or higher | 65 | 9.8% |
| Years of education and range (n = 667) | 9 (6–12) | |
| Infant Variables | ||
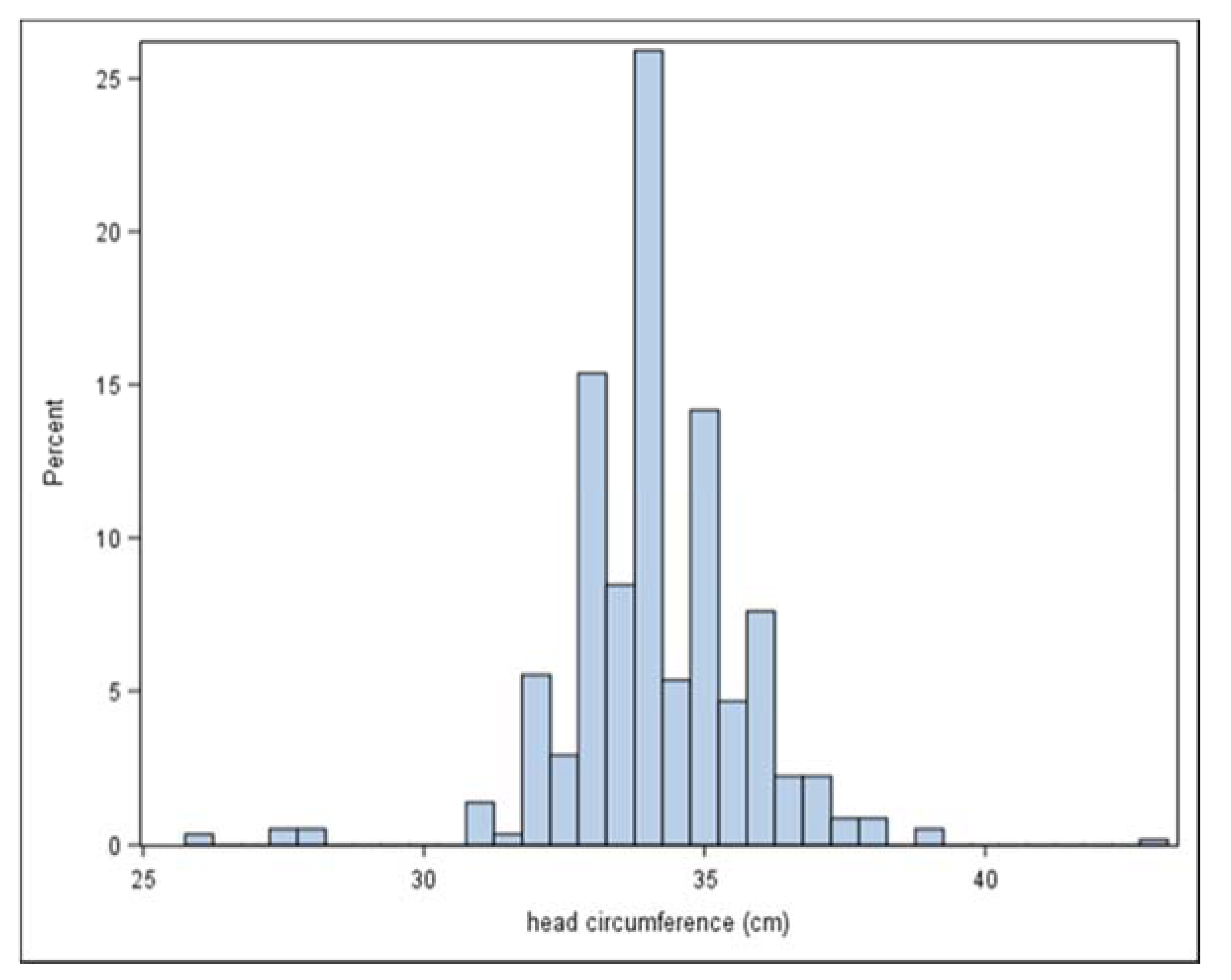
| Head circumference at birth (n = 578) | ||
| mean in cm (SD) | 34.1 (1.62) | |
| median in cm (IQR) | 34.0 (33.0–35.0) | |
| mode in cm, range | 34.0 (26–43) | |
| HC more than 2SD below the mean * | 9 | 1.56, 95% CI 0.71–2.93 ** |
| HC more than 3SD below the mean * | 2 | 0.35, 95% CI 0.04–1.24 |
| HC < 3rd percentile * | 11 | 1.90, 95% CI 0.79–3.02 |
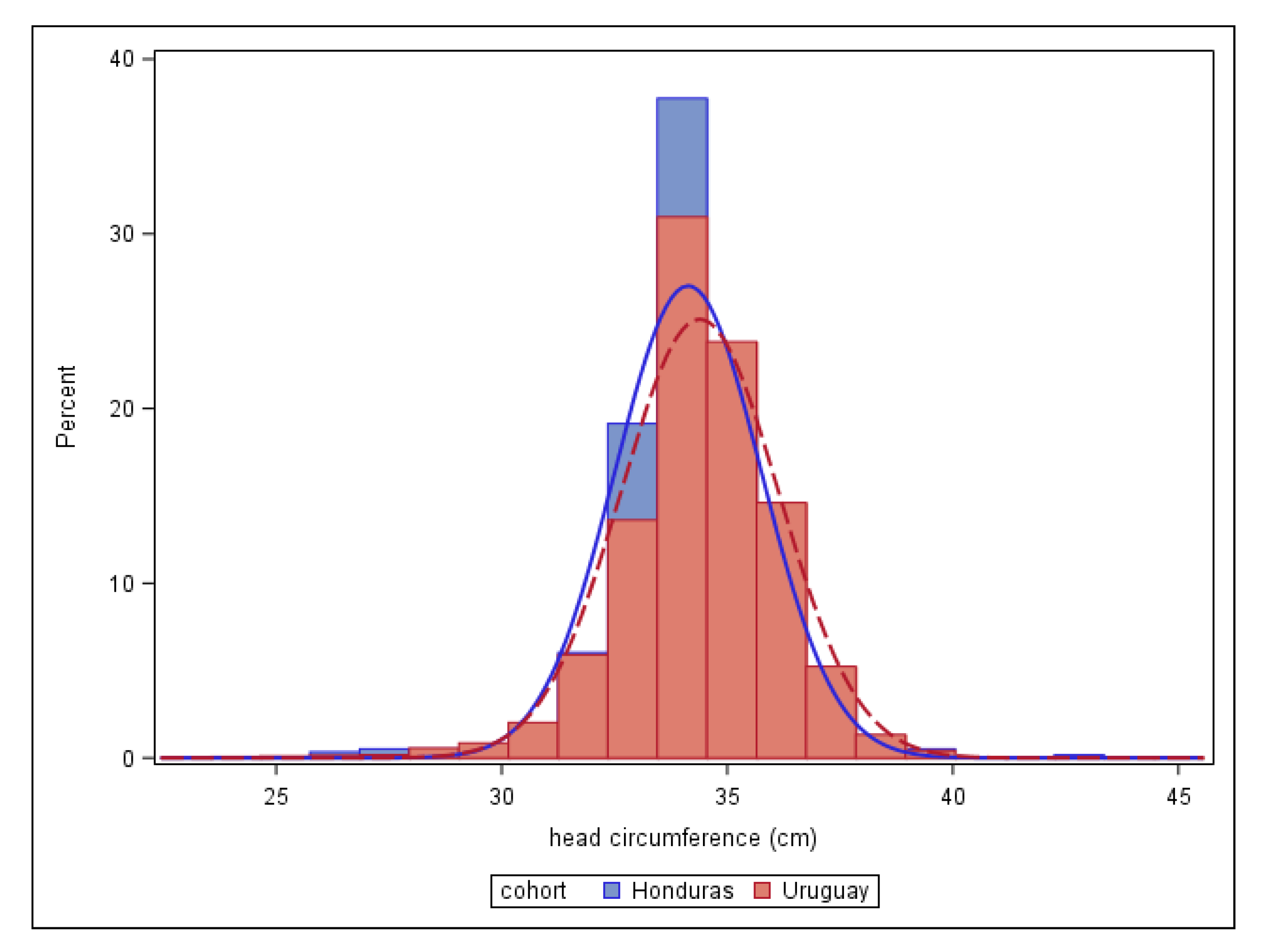
| ZIPH Cohort | Uruguay SIP | |||
|---|---|---|---|---|
| Last Digit (Tenths Place) | N | % | N | % |
| 0 | 419 | 72.4 | 188,108 | 73.5 |
| 0.1 | 0 | 0.0 | 102 | 0.0 |
| 0.2 | 10 | 1.7 | 444 | 0.2 |
| 0.3 | 8 | 1.4 | 462 | 0.2 |
| 0.4 | 5 | 0.9 | 435 | 0.2 |
| 0.5 | 112 | 19.3 | 65,196 | 25.5 |
| 0.6 | 15 | 2.6 | 304 | 0.1 |
| 0.7 | 7 | 1.2 | 291 | 0.1 |
| 0.8 | 2 | 0.3 | 432 | 0.2 |
| 0.9 | 1 | 0.2 | 145 | 0.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Harville, E.W.; Tong, V.T.; Gilboa, S.M.; Moore, C.A.; Cafferata, M.L.; Alger, J.; Gibbons, L.; Bustillo, C.; Callejas, A.; Castillo, M.; et al. Measurement of Head Circumference: Implications for Microcephaly Surveillance in Zika-Affected Areas. Trop. Med. Infect. Dis. 2021, 6, 5. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed6010005
Harville EW, Tong VT, Gilboa SM, Moore CA, Cafferata ML, Alger J, Gibbons L, Bustillo C, Callejas A, Castillo M, et al. Measurement of Head Circumference: Implications for Microcephaly Surveillance in Zika-Affected Areas. Tropical Medicine and Infectious Disease. 2021; 6(1):5. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed6010005
Chicago/Turabian StyleHarville, Emily W., Van T. Tong, Suzanne M. Gilboa, Cynthia A. Moore, Maria Luisa Cafferata, Jackeline Alger, Luz Gibbons, Carolina Bustillo, Allison Callejas, Mario Castillo, and et al. 2021. "Measurement of Head Circumference: Implications for Microcephaly Surveillance in Zika-Affected Areas" Tropical Medicine and Infectious Disease 6, no. 1: 5. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed6010005