
Performance of an Emergency Road Ambulance Service in Bhutan: Response Time, Utilization, and Outcomes

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Settings
2.2.1. General Setting
2.2.2. Specific Setting
The Health Help Centre (112 Hotline) and Ambulance Network
Study Population and Period
2.3. Data Collection, Analysis, and Statistics
3. Results
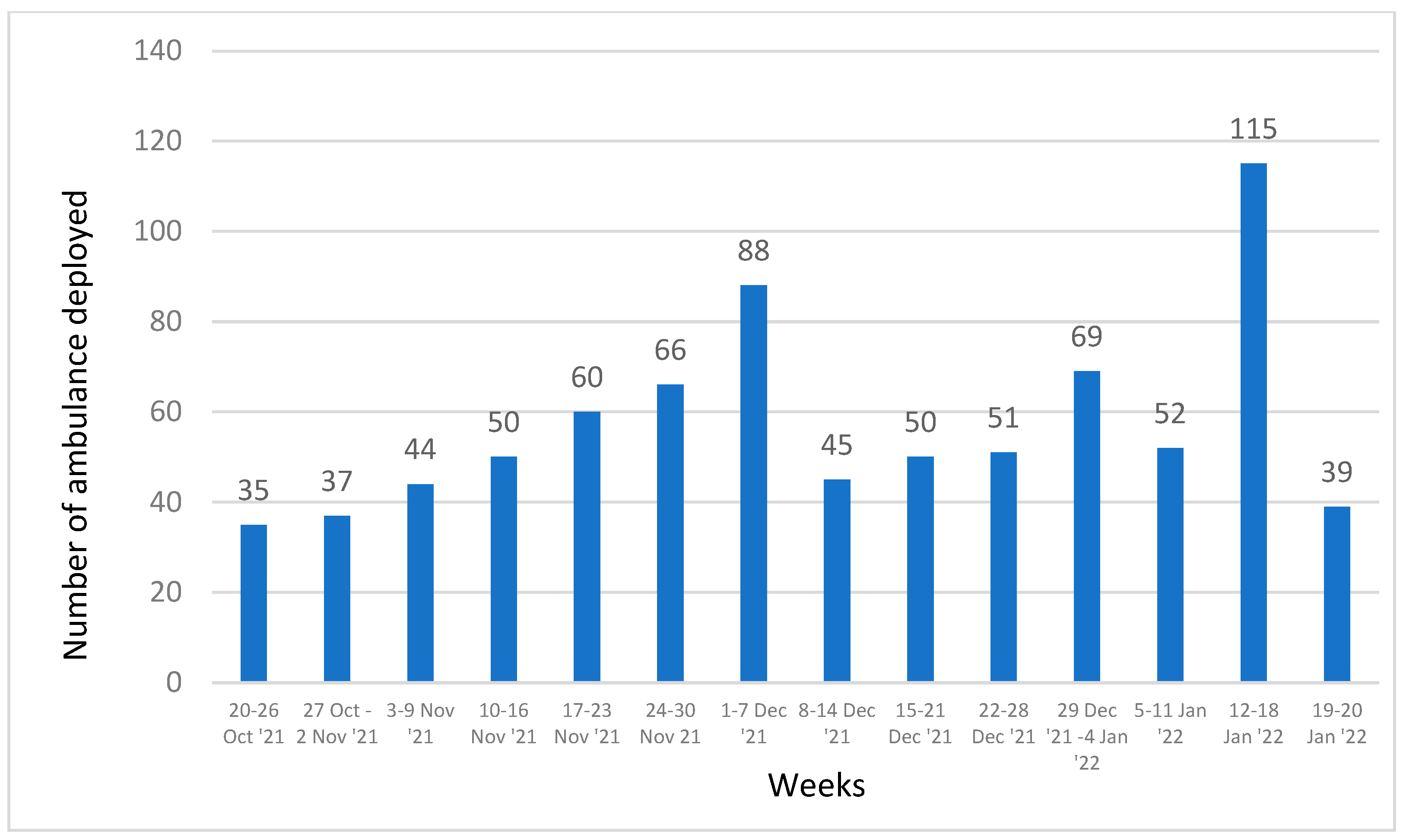
3.1. Caller Details and Trend of Ambulance Deployments
3.2. Ambulance Response Time and Patient Transport Time
3.3. Patient Characteristics and Morbidities
3.4. Ambulance Exit Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Accorsi, S.; Somigliana, E.; Solomon, H.; Ademe, T.; Woldegebriel, J.; Almaz, B.; Zemedu, M.; Manenti, F.; Tibebe, A.; Farese, P.; et al. Cost-effectiveness of an ambulance-based referral system for emergency obstetrical and neonatal care in rural Ethiopia. BMC Pregnancy Childbirth 2017, 17, 220. [Google Scholar] [CrossRef] [Green Version]
- Godefay, H.; Kinsman, J.; Admasu, K.; Byass, P. Can innovative ambulance transport avert pregnancy-related deaths? One-year operational assessment in Ethiopia. J. Glob. Health 2016, 6, 010410. [Google Scholar] [CrossRef]
- Henry, J.A.; Reingold, A.L. Prehospital trauma systems reduce mortality in developing countries: A systematic review and me-ta-analysis. J. Trauma Acute Care Surg. 2012, 73, 261–268. [Google Scholar]
- Blackwell, T.H.; Kaufman, J.S. Response time effectiveness: Comparison of response time and survival in an urban emergency medical services system. Acad. Emerg. Med. 2002, 9, 288–295. [Google Scholar]
- Ong, M.E.H.; Chiam, T.F.; Ng, F.S.P.; Sultana, P.; Lim, S.H.; Leong, B.S.-H.; Ong, V.Y.K.; Tan, E.C.C.; Tham, L.P.; Yap, S.; et al. Reducing Ambulance Response Times Using Geospatial-Time Analysis of Ambulance Deployment. Acad. Emerg. Med. 2010, 17, 951–957. [Google Scholar] [CrossRef]
- Stein, C.; Wallis, L.; Adetunji, O. Meeting national response time targets for priority 1 incidents in an urban emergency medical services system in South Africa: More ambulances won’t help. S. Afr. Med J. 2015, 105, 840–844. [Google Scholar] [CrossRef] [Green Version]
- Stein, C.; Wallis, L.; Adetunji, O. The Effect of the Emergency Medical Services Vehicle Location and Response Strategy on Response Times. S. Afr. J. Ind. Eng. 2015, 26, 26–40. [Google Scholar] [CrossRef] [Green Version]
- Somigliana, E.; Sabino, A.; Nkurunziza, R.; Okello, E.; Quaglio, G.; Lochoro, P.; Putoto, G.; Manenti, F. Ambulance service within a comprehensive intervention for reproductive health in remote settings: A cost-effective intervention. Trop. Med. Int. Health 2011, 16, 1151–1158. [Google Scholar] [CrossRef]
- Erkut, E.; Ingolfsson, A.; Sim, T.; Erdoğan, G. Computational Comparison of Five Maximal Covering Models for Locating Ambu-lances. Geogr. Anal. 2009, 41, 43–65. [Google Scholar]
- Sultan, M.; Abebe, Y.; Tsadik, A.W.; Jennings, C.A.; Mould-Millman, N.-K. Epidemiology of ambulance utilized patients in Addis Ababa, Ethiopia. BMC Health Serv. Res. 2018, 18, 997. [Google Scholar] [CrossRef] [Green Version]
- O’Keeffe, C.; Nicholl, J.; Turner, J.; Goodacre, S. Role of ambulance response times in the survival of patients with out-of-hospital cardiac arrest. Emerg. Med. J. 2011, 28, 703–706. [Google Scholar] [CrossRef] [Green Version]
- MOH. Ambulance Service Guideline; Emergency Medical Services Division, Department of Medical Services, Ministry of Health: Thimphu, Bhutan, 2018. [Google Scholar]
- World Health Organization. The Triple Billion Targets. Available online: https://www.who.int/news-room/questions-and-answers/item/the-triple-billion-targets (accessed on 17 March 2022).
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Bull. World Health Organ. 2007, 85, 867–872. [Google Scholar]
- World Health Organization. Monitoring Emergency Obstetric Care: A Handbook; World Health Organization: Geneva, Switzerland, 2009; Available online: https://apps.who.int/iris/bitstream/handle/10665/44121/9789241547734_eng.pdf (accessed on 22 May 2022).




{kind=link}
{kind=link}
{kind=link}
| Level of Health Facility | Number of Hospital Beds | Number of Allocated Ambulances |
|---|---|---|
| National referral hospital | 350 | 6 |
| Regional referral hospital | 150 | 5 |
| General/larger district hospital | 40–60 | 3 |
| Smaller district hospital | 20–39 | 2 |
| Sub-district hospital | 10 | 1 |
| Reasons for Call | Ambulance Exit Outcomes |
|---|---|
| Non-pregnancy-related outcomes:
|
Pregnancy-related outcomes:
|
| District | District Population | Total Ambulance Deployment | Standardized Deployment 1 |
|---|---|---|---|
| Punakha | 28,842 | 69 | 23.9 |
| Sarpang | 46,571 | 88 | 18.9 |
| Dagana | 24,648 | 43 | 17.4 |
| Trashigang | 44,984 | 72 | 16.0 |
| Bumthang | 17,471 | 26 | 14.9 |
| TrashiYangtse | 16,929 | 25 | 14.8 |
| Zhemgang | 17,648 | 25 | 14.2 |
| Monggar | 36,526 | 47 | 12.9 |
| Haa | 14,374 | 18 | 12.5 |
| Chhukha | 71,473 | 74 | 10.4 |
| Lhuentse | 13,852 | 12 | 8.7 |
| Paro | 46,717 | 39 | 8.3 |
| SamdrupJongkhar | 34,949 | 29 | 8.3 |
| Thimphu | 139,726 | 116 | 8.3 |
| Trongsa | 22,763 | 16 | 7.0 |
| WangduePhodrang | 46,157 | 31 | 6.7 |
| Samtse | 61,353 | 39 | 6.4 |
| Pema Gatshel | 23,247 | 14 | 6.0 |
| Gasa | 3910 | 2 | 5.1 |
| Tsirang 2 | 22,186 | 0 | 0.0 |
| Median | IQR | Range | |
|---|---|---|---|
| Time from call to ambulance being assigned | 4 | 3 | 1–178 |
| Time from being assigned to ambulance deployment | 6 | 8 | 1–186 |
| Time from deployment to reaching the scene | 30 | 44 | 1–271 |
| Ambulance response time 1 | 42 | 50.5 | 3–271 |
| Patient transport time 2 | 41 | 49 | 2–272 |
| Characteristics | Category | Number | (%) |
|---|---|---|---|
| 801 | |||
| Age category (years) | |||
| Under 5 (≤5) | 39 | (4.9) | |
| 6–18 | 57 | (7.1) | |
| 19–30 | 194 | (24.2) | |
| 31–60 | 317 | (39.6) | |
| ≥61 | 186 | (23.2) | |
| Not recorded | 8 | (1.0) | |
| Sex | Male | 365 | (45.6) |
| Female | 424 | (52.9) | |
| Not recorded | 12 | (1.5) | |
| Occupation | Unemployed | 94 | (11.7) |
| Employed | 91 | (11.4) | |
| Housewife | 98 | (12.2) | |
| Student | 48 | (6.0) | |
| Farmer | 305 | (38.1) | |
| Military | 3 | (0.4) | |
| Not recorded | 162 | (20.2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tshokey, T.; Tshering, U.; Lhazeen, K.; Abrahamyan, A.; Timire, C.; Gurung, B.; Subedi, D.C.; Wangdi, K.; Vilas, V.D.R.; Zachariah, R. Performance of an Emergency Road Ambulance Service in Bhutan: Response Time, Utilization, and Outcomes. Trop. Med. Infect. Dis. 2022, 7, 87. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed7060087
Tshokey T, Tshering U, Lhazeen K, Abrahamyan A, Timire C, Gurung B, Subedi DC, Wangdi K, Vilas VDR, Zachariah R. Performance of an Emergency Road Ambulance Service in Bhutan: Response Time, Utilization, and Outcomes. Tropical Medicine and Infectious Disease. 2022; 7(6):87. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed7060087
Chicago/Turabian StyleTshokey, Tshokey, Ugyen Tshering, Karma Lhazeen, Arpine Abrahamyan, Collins Timire, Bikash Gurung, Devi Charan Subedi, Kencho Wangdi, Victor Del Rio Vilas, and Rony Zachariah. 2022. "Performance of an Emergency Road Ambulance Service in Bhutan: Response Time, Utilization, and Outcomes" Tropical Medicine and Infectious Disease 7, no. 6: 87. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed7060087