1. Introduction
Functional neurological disorders (FND) have seen their nomenclature and understanding of mechanisms evolve across history. In ancient Greece, they were considered a form of hysteria (ancient Greek: hystera = uterus), with symptoms due to a wandering uterus. Sigmund Freud later postulated the theory of “conversion”, i.e., the conversion of an intrapsychic conflict into a neurological physical symptom. In line of this view of a causal psychological factor, the term ‘psychogenic’ has since then been widely used. However, in light of new knowledge stemming from neuroscience, pathophysiology of FND is now understood as a dysfunction in the central nervous system, hence the reappearance of the term “functional”, which is less stigmatizing and better accepted by patients [
1,
2]. In 2013, new diagnostic criteria of the Diagnostic and Statistical Manual of Mental Disorders DSM-5 highlighted the fact that diagnosis is not an exclusion process but relies on the presence of positive clinical characteristics.
FND represent a common disorder, diagnosed in about one-third of general neurology out-patients [
3]. They are more common in women than men and have a peak incidence between the ages of 35 and 50 [
4], even though presentation throughout the lifespan is possible. As they affect mostly young people, socio-economic impact is significant [
4,
5]. In this context and alongside recent new neuroscientific insights, FND attract a growing interest both in clinical practice and academic activities. Teaching programs are being developed and a new international society was created in 2019 (fndsociety.org). Several clinical centers developed around the world over the last years, offering a specific and multidisciplinary therapy for patients suffering from FND. Therapeutic offerings range from in- and outpatient clinics [
6,
7,
8] to stepped care programs [
9], as well as specific motor rehabilitation programs for functional movement disorder [
10]. Furthermore, international treatment recommendations have also been elaborated upon [
11,
12].
Also in Switzerland, there was a lack of specialized FND treatment program (in- and out-patient) until 2016. It was not unusual that FND patients did not have any therapies and neither neurological nor psychiatric follow-up. In 2016, a new clinical care setting was created [
13] within the neurology department of Bern University hospital, Switzerland, with a merging of the Psychosomatic Unit, which has long expertise in care of patients with chronic pain, chronic fatigue, and other Somatic Symptom disorders. This article reports the current treatment path offered in this new setting, in light of recent advances in clinical knowledge in the field. It is presented in the form of a narrative review.
2. Principals of Therapeutic Approach and Treatment Steps
The FND clinic offers a multidisciplinary outpatient program—and since this year, an in-patient program involving neurologists, physiotherapists, occupational therapists, psychotherapist, and social workers closely collaborating together has been added. The FND unit consists of five neurologists (including two residents) within the clinic for psychosomatic medicine, which is run by an interdisciplinary team of internists, anesthetists and psychiatrists (six specialists, six residents) offering in- and outpatient treatment to other pathologies such as chronic pain, eating disorders, somatic symptoms disorders, etc. A team of physiotherapists (eight therapists), psychotherapists (seven psychologists) and occupational therapists (three therapists) is shared by the different subunits of the psychosomatic clinics. Patients are referred either internally (approximately 40%) from the hospital, mainly from the emergency department or neurology ward but also other departments (neurosurgery, rheumatology, internal medicine) or externally (approximately 60%) from general practitioners or primary care clinics and practitioners. Referrals are made from the whole of Switzerland, since now no other specific FND center exists in the country. The main reason for referral is suspected FND, for confirmation of diagnosis (second opinion) and treatment recommendation. Patients with all types of functional neurological symptoms are being referred: functional movement disorders (paresis/plegia, gait disorders, hyper- and hypokinetic movement disorders), functional sensory and sensorial deficits (including persistent postural-perceptual dizziness (PPPD)) as well as functional non-epileptic seizures. Mixed functional neurological symptoms are also frequent. Combinations with other complaints such as chronic pain, fatigue, chronic/periodic hypersomnia, sleep-related movement disorders, and variable psychiatric comorbidities are common. However, referrals are usually accepted only if a neurological complaint is described in the referral letter. Triage allows transferring patients with non-neurological complaints (e.g., primary chronic pain, gastrointestinal symptoms, etc.) to the appropriate clinic/consultation (pain management group, pain clinic, psychosomatic unit, etc.) and prioritize acute cases (recent onset within weeks, acute deteriorations), as our waiting list has an average waiting time of 2–3 months. Our clinic accepts cases with a large range of symptom duration—from a few days (mostly patients from the emergency department or neurological ward) to several decades as well as severity (patients still employed vs. completely care-dependent). Amongst this heterogeneous group of FND patients, treatment options need to reflect the diversity of symptom phenotypes as well as the heterogeneity and comorbidity within the patient population [
14]. According to current recommendations, our therapeutic approach is a tailored multidisciplinary management involving the neurologist, the physiotherapist, and in most of the cases also the psychotherapist [
14,
15]. In approximately 30% of the cases, out-patient treatment is organized at our FND Unit, especially for patients living in the direct vicinity or with complex semiology; in approximately 70% of the patients, interdisciplinary treatment is organized externally (patients living in geographically distant regions or with milder symptoms).
2.1. Neurological Assessment and Diagnostic Procedures
A definitive diagnosis is made by the team of neurologists (three neurologists, two residents) on the basis of clinical positive signs and after careful exclusion of an alternate possible neurological disease explaining the symptom. A dual diagnosis of FND and a comorbidity with other neurological diseases is also carefully considered (for example, multiple sclerosis or past stroke with current FND). The initial visit consists of a 1.5 h neurological consultation (covered by health assurance) with a junior neurologist in training (1 h), then supervised by a senior neurologist with expertise and training in FND (30 min). This procedure enables trainees to be integrated during their rotation of residency in neurology, with the aim to expose all future neurologists to this common disorder. In complex movement disorders, patients are evaluated interdisciplinary together with our colleagues of the Movement Disorder Unit and Liaison Psychiatry. Patient population ranges from classical movement disorders (e.g., Parkinson) with relevant functional comorbidities, to primary complex functional movement disorders and movement disorders with manifestation making specific psychiatric/psychotherapeutic treatment approach necessary (e.g., Chorea Huntington, tic disorders) or resulting of a psychiatric context (e.g., catatonia, drug-induced movement disorders).
At first evaluation, we do not only focus on the actual symptoms or affected body part, but a full neurological exam is always performed, and clinical positive signs documented (see below). Usually a second evaluation is required before a definite diagnosis is reached. As many patients have had previous neurological consultations and/or exams (brain imaging, lumbar puncture, blood tests, electroencephalogram, electroneuromyography), we collect all past medical records to review the evolution of symptoms and the results of previous tests. If required, we also ask patients to send us home videos of their symptoms between visit one and two (usually 2–3 months later), to help confirm the diagnosis. Diagnosis is made according to the new definition of the Diagnostic and Statistical Manual of Mental Disorders DSM-5 (
Figure 1).
Of note, the previous version of the Diagnostic and Statistical Manual of Mental Disorders DSM-4 defined conversion disorder as the association of a functional, medically unexplained, neurological symptom (criterion A) with a psychological stressor (criterion B). Even though, psychological traumas have been reported to be higher in FND patients compared to healthy volunteers [
16], psychopathology is not always evident; a substantial proportion of patients (from 14% to 77%) do not report having experienced traumatic events in their history [
17]. Yet, if psychological factors alone are not sufficient to explain the etiology of FND, they are still important risk factors and/or maintaining factors [
18,
19]. Since 2013, the new DSM-5 version (American Psychiatric Association 05/2013 (
Figure 1)) underlines the importance of making a ‘positive’ diagnosis of conversion disorder/FND based on positive clinical signs rather than associated psychological factors. The diagnosis can specify whether there is an associated stressor or not as an adjunct information, but the presence of a stressor is no longer needed to ascertain the diagnosis. The new criterion (B) requires that clinical findings provide evidence for incompatibility between the symptoms and recognized neurological/neuroanatomical or medical conditions’ (American Psychiatric Association, 2013) [
20,
21]. The way to provide the evidence for incompatibility is to use clinical positive signs [
22] (e.g., drift without pronation (
Figure 2)) or paraclinical tests [
23] (e.g., electrophysiological tremor analysis) that are specific and reliable for functional neurological disorder (FND) [
24,
25]. The DSM-5 classification takes into consideration that FND is a spectrum disorder, with its generic classification in different subtypes according to the symptom (e.g., F44.4 for motor FND (weakness or movement disorder), F44.5 for non-epileptic attacks or seizures, F44.6 for sensory symptoms and F44.7 for mixed symptoms). For reviews on how to make the diagnosis, please refer for example to J. Stone an A. Carson 2011 [
26].
During follow-up visits, focused neurological exam and clinical positive signs are documented. If a functional movement disorder is present, the Simplified Functional Movement Disorders Rating Scale (S-FMDRS) is executed as a follow-up parameter. In functional non-epileptic seizures, the frequency of seizures (seizures per week or month) is documented.
2.2. Communication and Explanation of the Diagnosis
Communication and explanation of the diagnosis by the neurologist is of great importance and represents the first step of a therapeutic approach [
27,
28] (see also
Figure 3). This is usually undertaken in a second visit (1 h). This allows time to obtain and review the full medical record, as mentioned above. Of note, we often mention the diagnosis of FND at the end of the first visit and hand out information flyers to the patient. We explain that this is the suspected diagnosis but that we need to review brain scans/letters/blood-cerebrospinal fluid tests, etc. before being able to confirm a definite diagnosis. Analogous to other disorders a positive diagnosis should be given. This is what we usually do during the second visit. We do not list the “non-diagnoses” (“you don’t have multiple sclerosis, stroke, etc.”), unless mentioned by the patient and with the aim to eliminate potential fears the patient may explicitly express of other neurological diseases [
28]. Having a name for a diagnosis is seen as a great relief by the patients and can avoid repeated, mostly unnecessary, medical investigations (“doctor shopping”) and consecutively a delay of appropriate treatment [
27,
29]. We thus use the term ‘functional disorder’, as it is descriptive (disorder due to dysfunction of nervous system) and nonjudgmental [
2,
30]. As an explanatory model, the comparison of the human brain with a computer, as a metaphor, can be helpful [
28]: The anatomical/structural setup (“hardware”) is intact, but there are alterations within the functional level (analogous to a “software problem”). This also explains the fact that investigations (e.g., MRI, etc.) are normal. We highlight the fact that due to the absence of major structural correlate, symptoms are potentially reversible with treatment [
27,
29]. For further information, we refer patients/relatives/involved physicians to the websites
www.neurosymptoms.org (translated in several languages) or
www.nonepilepticattacks.info (in English). We also designed short videos and information brochures to explain the diagnosis in the three national languages (German, French, Italian) and English. We either show these information videos (
http://www.neurologie.insel.ch/de/unser-angebot/psychosomatische-medizin/ambulatorium/sprechstunde-fuer-funktionelle-neurologische-stoerungen-fns/, 27 October 2021) directly during this second visit or we provide the link to our clinic website. We emphasize that symptoms are real, not imagined or simulated and that responsible altered brain activity patterns in FND can be visualized by fMRI (currently only used for research purposes). If needed, we explain findings from research that showed distinctive changes in brain activation when comparing functional symptoms to fake symptoms (voluntarily produced by simulators/feigners) [
31,
32,
33,
34,
35]. Compared to healthy controls and actors feigning weakness, patients with functional weakness showed decreased dorsolateral, prefrontal cortical activity, reduced activation of the contralateral parietal region, and increased perfusion in the frontal region, hereby suggesting that frontal regions were inhibiting the motor and premotor areas when patient tried to move their affected limb, as if the ‘center of volition’ was malfunctioning. By consequence, symptoms are perceived as involuntary and must be distinguished from simulating. This is of importance for our patients, who often have seen their benefit/insurance allowance rejected because they were thought to fabricate their symptoms.
Specific diagnostic features on examination can be demonstrated (e.g., Hoover sign or tremor entrainment) and be useful to explain the pathophysiological mechanisms and reveal the potential reversibility of the condition as well as the pathological influence of attention towards symptoms [
6,
27]. Consecutively distraction techniques (e.g., music, talking, or altered gait patterns) can be explained by the neurologist and used by physiotherapists [
11] during their session with the aim to reinstate automatic neurological control and redirect unhelpful movement-focused attention.
Psychological factors as potentially important risk and/or maintaining factors can be discussed [
6]. We emphasize that psychological factors potentially influencing the symptoms are not necessarily trauma or for example severe depression, but also psychological stressors of daily life (e.g., stress at work). The impact of the current symptoms can also represent in itself a burden that required psychotherapeutic help. Nevertheless, discussing referral to psychotherapy often requires a trustful doctor–patient relationship and may not always be addressed during the early consultations. Individualized therapy is composed for every patient according to their symptoms and their biopsychosocial situation. Assessment of accompanying symptoms e.g., sleep disturbance, fatigue, pain, cognitive symptoms, and comorbid psychiatric symptoms is important and supportive drug therapy can be considered [
28,
29]. During our neurological evaluation, we are therefore also attentive to possible comorbid psychiatric symptoms, and—if suspected—psychiatrist/psychotherapist is involved for further diagnostic and therapeutic assessment.
2.3. Development of an Individualized Treatment Concept
Most patients receive physiotherapy, which we organize (after the first or second visit). Only in the case of very mild symptoms can a wait-and-see approach be adopted. For patients with motor deficits, primarily activating exercises are aimed at; for comorbid muscular pain, stretching exercises and myorelaxing approaches are recommended. In the case of sensory deficits, but also with functional non-epileptic seizures, exercises for body awareness are of great importance, supplemented with relaxation techniques (see
Section 2.4). Whenever possible, physiotherapy is organized internally in our institution, especially if symptoms are complex or severe. When this is difficult due to geographical issues (e.g., patients live too far away for weekly treatment), additional information is given to the external physiotherapist (information brochure, telephone contact) or physiotherapeutic sessions in our institution alternate with residence near treatment (for example, weekly physiotherapeutic sessions, with sessions in our institution every second week). Teaching courses for physiotherapeutic approach of FND are held regularly at our institution to build up a network of FND specialized physiotherapists. Participants of this course and physiotherapist with whom we have had already made good experiences in the work with other FND patients are prioritized in the assignment of our patients.
According to clinical semiology, involvement of speech therapist and/or occupational therapist are recommended. Speech therapy (organized externally, at ENT-department of our university clinic or extern clinic) can be beneficial in restoring normal speech patterns and can also help with restoring normal breathing and swallowing patterns [
36]. Occupational therapy (within our department or externally, depending on geographical issues and symptom complexity) aims to prevent activity avoidance and dependence on others by developing strategies to handle daily life as well as possible according to individual based interests and needs of daily living, work, and leisure taking the patients symptoms into account. Through guided activity practice, practical management of pain and fatigue are addressed as well as helpful strategies, including structure and routine (ex. daily plan with regular timeouts) to prevent activity and cognitive overload [
37].
Regarding psychotherapy, indication is not given in every patient and needs to be evaluated at an individual level. In patients with rapid symptom regression and without associated psychological factors (e.g., psychiatric comorbidity, ongoing psycho-social stress situation), psychotherapy is mostly not indicated If psychological factors are present, their revelation as well as the acceptance of psychotherapy often needs a trusting doctor–patient relationship. Premature recommendation for psychotherapy can therefore threaten the therapeutic relationship. In our institution, we are offering time-limited cognitive behavior-based and symptom-orientated psychotherapy. At the beginning of treatment, patient are seen every 2–3 weeks, with subsequent expansion of the intervals to 4–8 weeks depending on individual cases. There is no defined upper limit in number of therapy sessions; nevertheless, when indication for psychotherapeutic follow-up is still given after 6–12 months of treatment, we refer patients to a private practice established psychotherapist to guarantee a long-term follow-up. In this sense, we also refer patients directly to a private practice, if a long-term psychotherapy is predictable (e.g., trauma therapy). If the patient already has a treating psychotherapist, exchange/information by telephone is actively sought. Psychotherapy is covered by Swiss insurances when done, prescribed or supervised by a physician.
Involving the general practitioner (GP) can also be very useful and in addition to our medical letter, we often contact the GP over the phone, when complex cases need to be discussed. As a general rule, we do not prescribe medication but only make recommendations to the GP. Furthermore, we do not get involved actively in insurance/work disability; this is also dealt with by the GP. By acting this way we avoid any potential conflict of interests as we aim for having only a therapeutic relationship with our patients rather than acting as experts regarding other potential financial or social difficulties. However, we support the GP in these aspects when diagnostic questions are raised.
Whenever possible, we try to develop an out-patient treatment setting leaving the patient in his/her usual surrounding. If out-patient treatment lacks in progress and in very complex, severe and chronic cases, in-patient programs are recommended, allowing a higher intensity of treatment, while limiting environmental and social factors that may be perpetuating symptoms. Since this year, we also offer a three-week intensive specialized in-patient treatment program. Treatment eligibility is evaluated in a preliminary consultation with the following main criteria: (1) disability primary due to FND, (2) acceptance of a multimodal treatment approach (in particular psychological interview), and (3) exclusion of severe psychiatric or other comorbidities (e.g., pain disorder, severe chronic fatigue) justifying refereeing to one of our collaborating clinics (see also
Figure 4 and
Section 2.6 and
Section 2.7 below). In severely chronic FND patients, we also preferably recommend a less-intensive and long-term rehabilitation stay in one of our collaborating rehabilitation clinics.
Pre- and posttreatment assessment (psychometric and clinical measurements with video documentation) are effectuated at hospital admission, respectively, at discharge. An in-patient program is individualized according to symptoms, with focus on intensive physiotherapy for functional movement disorders, respectively, cognitive behavioural therapy for patients suffering from functional non-epileptic seizures (PNES). Additionally, all patients benefit from psychological approach (joint-consultations, individual and group therapy) and occupational therapy (individual and group therapy). Psychoeducational knowledge is elaborated together with the patient and with the help of a therapy booklet, including also individualized notes (e.g., identified triggers, effective coping strategies, home exercises, reflections and observations from the patient and the therapeutic team, etc.). At discharge, the patient continues therapies in an ambulatory setting with a follow-up consultation at our institution in three months.
2.4. Physiotherapy
According to the consensus recommendation for physiotherapy for functional motor disorder [
11], it is important to make a complete assessment of all symptoms experienced (including associated symptoms such as pain, fatigue, etc.) and their implications in everyday life. Based on this information, physiotherapy goals are developed together with the patient (see also
Figure 5). Possible physical and/or psychological influencing factors are also discussed in the therapy sessions. Physiotherapy has a key role in improving the patients’ understanding of their disorder and its potential reversibility; for example, by demonstrating that normal movement can still occur. This can be very encouraging to the patient. A good understanding and acceptance of the diagnosis and creating an expectation of improvement are essential from the beginning of the therapy [
6,
11].
Neuroimaging using fMRI in FND patients demonstrated a reduced brain activity in the right temporo-parietal junction (TPJ), a key area involved in integrating complex sensory signals [
38,
39]. The right TPJ plays an important role in the sense of agency, which is the sense that we are the actors/agents of our own actions. The reduced TPJ activity in functional patients suggests that patients are no longer able to perceive their movement as voluntary. This probably explains—together with the earlier mentioned results [
31,
32,
33,
34,
35] showing hyperactivity of frontal regions inhibiting the motor and premotor areas—why automatic movements are better preserved than voluntary movements. Therefore, therapy should be based on goal directed rehabilitation focusing on automatic movements (e.g., walking) and functions instead of controlled movements like strengthening exercises. It is important not to concentrate on the affected body part but on meaningful activities such as walking or running, as the key in physiotherapeutic treatment of FND is to stimulate automatically generated movement by distraction or preventing the patient from cognitively controlled movement [
11]. Exercise with diverted attention can be helpful, such as walking while bouncing a ball, clapping or concentrating on a math problem. Visualization techniques can be useful during activity in order to enable normal movement. Furthermore, imaging a more fluid motor task might enable a distraction. Moving in front of a mirror may also help distract attention from monitoring body sensations. Visualization is not recommended if the patient concentrates too much on the symptoms (self-focusing) [
11].
It is advisable to provide a supportive therapy setting to allow the patient to be active rather than hands-on therapy [
11]. In functional weakness, it can be appropriate to encourage a patient to get up even if the muscle strength measurement does not correlate with the ability to stand. The subjective extent of the movement disorder often exceeds the findings that can be demonstrated objectively during therapy. Means of visual feedback (mirror, video recording) or demonstration of clinical positive signs (e.g., Hoover-sign) can provide feedback to the patient about their movements, which are often significantly different from what they imagine. The insight that normal movement is possible is often very impressive for patients and can lead to increased motivation and compliance with therapy [
11].
TENS (transcutaneous electrical nerve stimulation, producing a tingling sensation) has been tested as a potential treatment for patients with functional sensory loss to improve sensory awareness [
11,
40]. It can also be used for desensitization in hypersensitivity and allodynia, together with graded sensory stimulation, and graded movement/exercise [
11].
As a general treatment principle for physiotherapy of FND, the use of joint immobilizing devices should be avoided because they can lead to behaviors that prevent the return to normal automatic movement. For the same reason, adaptive equipment and mobility aids should be used with caution and as briefly as possible, especially in acute presentations. Sometimes, equipment may be necessary for pragmatic reasons, but should be considered as temporary and by explaining the importance of weaning their use [
11].
Improvement of body perception at rest or in motion is another important component of physiotherapy [
41]. The goal is to gain a better identification of physiological body sensations, but in particular stress-induced physical warning signals (pain, myalgia, etc.). Body perception and identification of early physical warning signs are particularly important in the physiotherapeutic treatment of functional non-epileptic seizures (PNES), in addition to psychotherapy, where physical and psychological factors are analyzed deeper. Since FND are typically negatively influenced by physical strain and stress in the broadest sense, improved body perception ideally allows patients to take corrective measures (e.g., taking a break or using relaxation techniques) before symptoms appear or increase. It is important to recognize and reconsider ineffective thoughts and behaviors (overstrain vs. avoidance behavior, etc.). Interests and preferences of the patients should be taken into consideration in order to find tailored therapy measures and motivate the patients.
In addition to all other symptoms, chronic pain and fatigue are often seen in patients with FND [
42]. It may be helpful for patients to understand that chronic pain does not correlate with harm but rather as a result from central hypersensitivity to pain [
11]. One key element to treat chronic pain and fatigue is breaking cycles of under-activity and over-activity with non-specific graded exercise. Thereby physical activity starts very slowly and gradually increases over time [
11]. In this way a gradual improvement in physical performance can be achieved, which can improve the patients’ quality of life [
11].
Physiotherapeutic interventions specialized for FND are efficient and lead to a significant reduction in symptoms for in- and out-patients, which are still verifiable months later [
43,
44,
45]. Physiotherapy showed improvement of symptoms in 55% of patients at 3 months of follow-up [
43]. Another randomized controlled study of physical rehabilitation in functional movement disorders reported symptom improvement in 72% of the intervention group (only 18% of the control group) [
46].
2.5. Psychotherapy
Psychotherapy is an important part of the interdisciplinary treatment. Neuroscientific evidence suggests abnormal emotional regulation processes in patients with FND: increased amygdala and periaqueductal gray (PAG) activity [
47] was measured in patients during negative emotion stimuli. Lack of habituation in amygdala activity over time suggests a general hyperarousal state in FND. Compared to healthy controls, patients may be more prone to automatic motor defense behavior, such as freeze response, mediated by PAG abnormal activity, a region known to be implicated in the freeze response in both animal [
48] and human [
49,
50] studies. There is also evidence of alteration in autonomic nerve system function in FND: decreased vagal mediated heart rate variability was observed in FND patients, both adults [
51] and children [
52], resulting in potentially inadequate protection from sympathetic stressors in these patients [
51]. Abnormal limbic–motor interaction is suspected to play a role in the generation of motor symptoms; an fMRI study looking at implicit emotion processing [
47] found a greater connectivity in functional motor disorder patients between the amygdala and the supplementary motor area (SMA), whereas another study found this same hyperconnectivity during the recall of autobiographical traumatic events. Additional finding from this study was increased dorsolateral prefrontal cortex activity and concomitant reduced hippocampal activity in patients during recall of the trauma, which is a pattern involved in active forgetting of unwanted memories [
53,
54] congruent with Freud’s repression theory.
Scientific studies prove the beneficial effect of psychotherapeutic interventions in functional movement disorders and functional non-epileptic seizures (PNES) [
55,
56]. The investigated interventions were based on cognitive behavioral therapy (CBT), integrative psychodynamic interpersonal therapeutic approaches or hypnotherapy [
14,
15,
57,
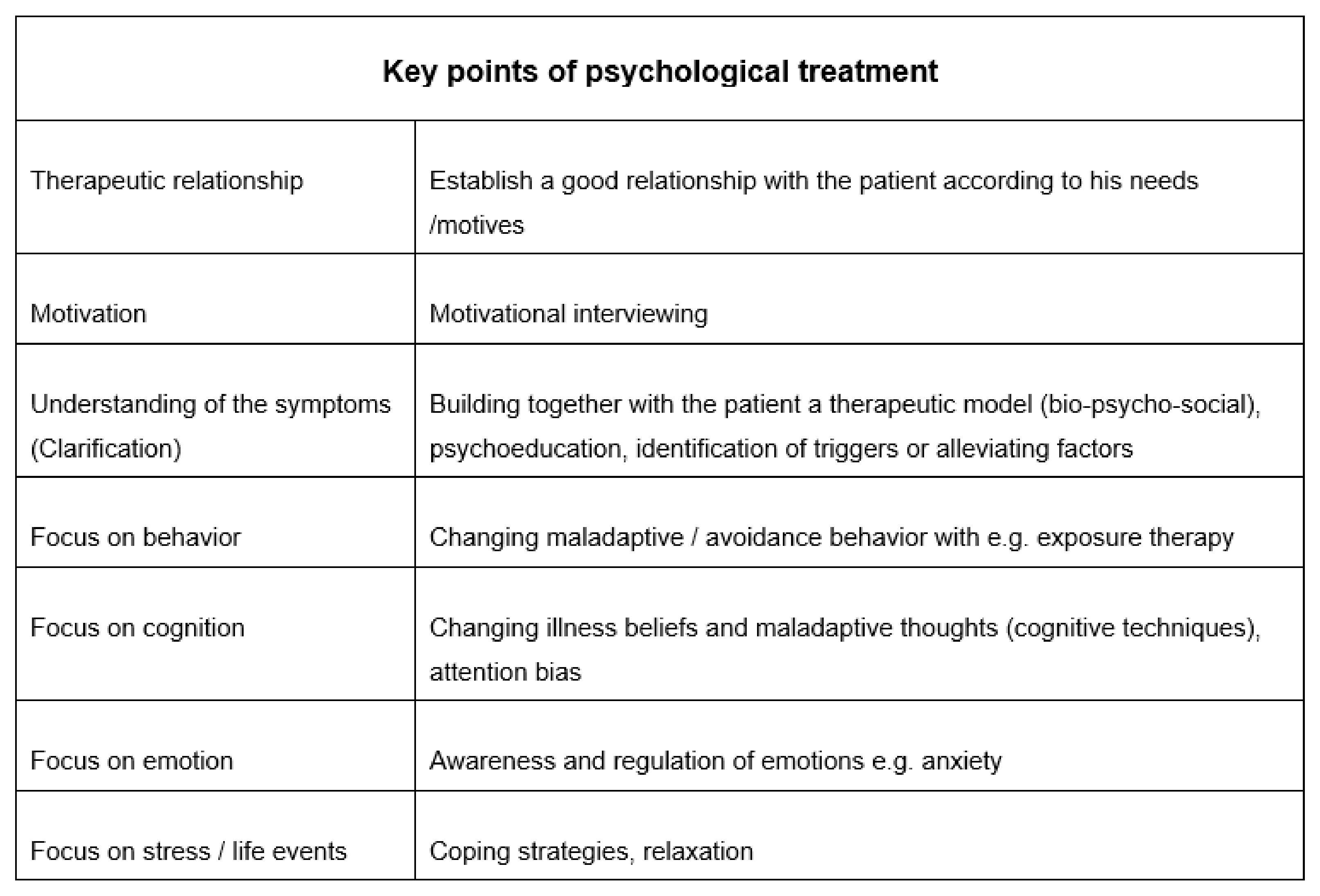
58]. As a general principle, a good understanding of the diagnosis, as well as therapeutic relationship and patient’s motivation and commitment are the basic prerequisite of the psychotherapeutic intervention. The therapy is then individualized (see also
Figure 6). On the basis of a good therapeutical model, it is important to encourage patients to engage in previously avoided activities and so reduce avoidance behavior. At the same time, endurance behavior is also a relevant factor in chronification, which means that pacing aspects (rest phases, break management, assessment of one’s own limits) represent an important therapy component. Stress and external life-events as well as internal conflicts or stressors could be relevant triggers and should be explored in the therapy. Strategies for regulation of emotions and acquisition of relaxation techniques are provided. Negative thoughts as well as convictions about illness of the patients are dealt with in the classical way using cognitive methods [
59]. Higher-level problem areas like low self-esteem, mood, or anxiety are addressed on an individual basis. Sometimes, it is also important to involve relatives or family members in the therapeutic process. Finally, personal well-being is optimized by focusing on good sleep quality, sufficient recovery phases, nutrition, and social support.
In functional non-epileptic seizures, for example, we work together with the patients towards identifying prodromal symptoms and triggers of their seizures at a behavioral, physiological, and cognitive level, based on the therapeutic manual of LaFrance and Wincze published in 2015 [
60]. Seizure protocols with self-observation are part of this therapy, where patients have to observe semiology of the seizures, documenting thoughts, behavior, and other internal and external factors. The aim is to enable the patient to identify prodromes at the beginning of the seizure and to develop appropriate coping-strategies (sit/lie down to prevent injury, breathing techniques, etc.) and regain a certain degree of control. Identified triggers and possibly also alleviating factors are analyzed and if possible modified in such a manner that seizure frequency and severity get reduced. Consequences associated with the seizures (e.g., workplace problems or conflicts) and handling of the seizures in these situations should be worked out. Also for functional movement disorders as well as other functional neurological symptoms, such symptoms diaries can be useful. The aim is again to explore thoughts, behavior, and other internal and external factors associated to the symptom and elaborate together appropriate coping strategies. Thereby body perception and selective attention focusing, respectively, distraction are of great importance.
Psychotherapy is an important treatment of FND: Goldstein and colleagues (2010) showed a significant reduction in seizure frequency and a higher probability of seizure-free time in the following three months in patients who received CBT compared with those receiving standard medical care [
58]. Their behavioral therapy (12 sessions) primarily involved managing the seizures, reducing the frequency of the seizures and improving the psychosocial functioning level on the above-mentioned principles. Nevertheless, in a recently published study by Goldstein and colleagues [
61] on the effectiveness of CBT on dissociative seizures at long-term follow-up at 12 months (randomized controlled trial and multicenter study, CBT compared with standard care alone), no statistically significant advantage of the CBT group was reported for the reduction of monthly seizures. However, they reported significant changes in secondary outcome measures. For example, the group with CBT reported to be less affected by the seizures, had a longer seizure-free period in the last six months, had less impairment in psychosocial functioning, had less overall psychological distress, fewer somatic symptoms, and reported a better quality of life than patients in the group with standardized medical care. The authors conclude that the patients do benefit from additional specialized psychotherapy.
In the field of functional movement disorders, the research data available for intervention studies are rather scarce, consequently there are no evidence-based psychotherapy recommendations [
55,
56]. Sharpe and colleagues [
62] presented and evaluated a guided self-help manual based on behavioral therapy in 2011. Outpatients with functional movement disorders and seizures (randomized groups) received a self-help manual for standard treatment and additionally offered 4 × 30 min sessions for handling the manual. Parts of the content of the manual based on already existing manuals for the treatment of anxiety and depression. It includes psychoeducation on functional symptoms and diagnosis (description of common symptoms, physiology, anatomy, and psychology) as well as self-management techniques in dealing with helplessness and the symptoms. After three months, the group with the self-help manual reported an improvement in health status, although the treatment effect was no longer presented at the six-month follow up. Nevertheless, patients with the self-help manual had an improvement in the symptom profile (i.e., less symptoms). Furthermore, they reported more satisfaction regarding the treatment than the standard group. The contents of this manual are equivalent to the contents of our therapy in our in- and outpatient clinic.
In addition to the disorder-specific interventions described for example in LaFrance and Wincze [
60], superordinate (symptom-unspecific but case specific) interventions at the level of therapeutic relationships, motives/needs of the patient, and communication are also important. Based on the concept of general psychotherapy according to Klaus Grawe [
63,
64] and according to the publications of Jon Stone [
65], the communication of the diagnosis and motivational therapeutic relationship is a central component of treatment. It is essential for a therapist to behave correspondently to the important motives/needs of the patient and to try to satisfy them proactively in the therapy. These motives/needs may be loss of control/helplessness, skepticism, or self-esteem. For example, patients experience loss of control not only through reduction of bodily functions, but also through the course of the disease, which is often fluctuating. It often takes a long time before the patient knows the diagnosis. This period of uncertainty, during which different diagnoses are often uncertain, can be very unsettling for the patient and have a strong impact on his wellbeing. In addition, secondary stressors (e.g., financial, professional) or dysfunctional disease management (e.g., social withdrawal) can get worse and have a negative impact on the course of the disease. The overall context of the patient should also be taken into account in therapeutic work. It is also known from the literature that this group of patients sometimes exhibit a high level of comorbidity with anxiety disorders (including post-traumatic stress disorder and panic disorder), depression, and personality disorders [
65], which should be treated in individual psychotherapy [
10,
13,
66]. Should this be the case with certain patients, we organize special psychotherapeutic therapy (e.g., trauma therapy) following our interdisciplinary intervention.
2.6. Interdisciplinarity
In addition to communicating the diagnosis, appropriate therapeutic relationship management is of the greatest relevance for the success of treatment [
63]. Here, above all, the patient should on the one hand be given a lot of control experience and at the same time be given a consistent team, clear structure, and security. Close and good interdisciplinary cooperation [
15,
67] seems to be most promising. Interdisciplinary interventions appear to be superior to standard care [
15,
67]. Comparison of an interdisciplinary treatment (interdisciplinary neurological/psychiatric–psychotherapeutic follow-up) [
15,
67] versus treatment as usual (single interdisciplinary consultation with advise to seek psychiatric–psychotherapeutic treatment in private practice) showed a significant improvement of functional symptoms, less frequent hospital readmissions, and better scores on the mental health component of the SF-36 and on the Beck Depression Inventory and a positive effect on work incapacity. The so-called “joint consultations” are regarded as the central method of the intervention [
67]. Here, a neurologist and psychiatrist see the patient together in a longer consultation. The neurological examination takes place first, followed by a psychiatric interview. Later, in the joint consultation, the findings/diagnosis and treatment options are discussed, including the patient. Patients who had psychiatric treatment outside the joint consultation program often are not able to ameliorate their physical symptoms, suggesting that unspecific psychiatric intervention is not sufficient for FND patients [
67]. Specific psychotherapeutic approach with elaboration of coping strategies and identification of psychological triggering factors seems more promising. Furthermore, repeated medical examination and discussion with the neurologist provides reassurance that there is no other responsible organic cause, which probably explains the reduction in the use of the healthcare system [
67]. Generally, acceptance regarding psychiatric/psychotherapeutic intervention (73–83%) is relatively high [
67]. Nevertheless, if skepticism is present, according to our experience, acceptance can be improved by interdisciplinary treatment approach.
We also follow this concept in our in- and outpatient program for functional neurological disorders at the University Hospital Inselspital in Bern (see
Figure 3). The neurologist makes and explains the diagnosis and undertakes part of the motivational work for the corresponding physiotherapeutic and psychotherapeutic treatment. Longer joint consultations (90 min; covered by health assurance) take place at the beginning and repeatedly during the course of the interdisciplinary treatment. In this joint consultation, the treatment team (neurology and psychology or neurology and physiotherapy) discusses with the patient the diagnosis, the course of treatment, patient’s explanatory model, or further procedures.
Weekly interdisciplinary meetings for in- and outpatients help us to discuss different treatment aspects of a patient and to make sure that everyone is on the same level of information. All team participants identify patients where there are difficulties/relevant news or feedbacks for the whole team (patients are registered in the form of an agenda; approx. 10 min discussion per patient). This leads to uniform communication with the patient and clear treatment structure. It also allows other disciplines to be consulted in the case of new complaints and comorbidities such as pain, etc. (see section on comorbidities).
As a university clinic with constantly ongoing reassignment, treatment duration of physiotherapy and psychotherapy is time-limited. Patients who need a continuation in either physiotherapy and/or psychotherapy are assisted to find an adequate therapist close to their residence. Condition for this therapeutical transfer is a psychologically stabilized current situation, respectively a clear physiotherapeutic treatment concept to pursue. To make this therapeutical transfer as smooth as possible, direct exchange/communication occurs within each specialty (physiotherapist from our team with physiotherapist in private practice or other local facility etc.).
2.7. Comorbidities
Patients suffering from FND often present comorbidities with both prominent chronic pain (56–79%) and chronic fatigue (48%) and also Somatic Symptom Disorder (39%) [
13]; less often, psychiatric comorbidities other than mild depression and anxiety [
13]. According to the main symptom, therapeutical lead is assigned to specific wards (FND Clinic, Psychosomatic Unit, Pain Clinic, or Liaison Psychiatry) with the other colleagues remaining as consultants. Patients with functional symptoms and signs but suffering primarily from their comorbidities are therefore referred (waiting time is approximately 2–3 months) to specialized consultations and clinics according to their leading symptom (see also
Figure 4).
We closely collaborate with our colleagues of the Psychosomatic Unit, offering an multi modal in- and out-patient program specialized for chronic pain and somatic symptom disorders. Internal interdisciplinary pain clinic composed of anesthetists, rheumatologists, and orthopedists are also regularly involved in therapeutic management of these patients. By evaluating the presence of eventual rheumatological or orthopedic comorbidities, the possibility of local infiltrations and treatment options with analgesics is given.
Collaboration with the University Sleep-Wake-Epilepsy Center is also important, as FND patients often present complaints of fatigue and circadian rhythm and sleep disorders. We also observe that sleep-related movement disorders (restless legs syndrome (RLS), periodic limb movement disorder (PLMD), benign sleep myoclonus) may favor development of additional functional movements disorders presenting when falling asleep. If chronic fatigue is the leading symptom, a therapeutic program has to be adapted according to their increased exhaustibility. Often these patients have a better benefit in external rehabilitation clinics offering less intensive and long-term therapies over 1–3 months.
Patients with severe psychiatric comorbidities as a main problem, needing a psychiatric therapeutical setting and infrastructure, are referred to our colleagues of the liaison psychiatry. They work on the same campus and are therefore easily to reach for eventual further neurological consultations during the patient’s hospitalization, if needed.
2.8. Outcome
Data concerning outcomes are variable. According to the largest prospective follow-up study in mixed FNDs (cohort study of 716 patients followed up over one year in Scotland), 68 outcomes were poor with 67% of the patients having unchanged symptoms or worse. Considering, that FND-patients seeking for help in specialized centers often present chronic and severe symptoms, may explain the rather poor outcome partly. However, several other studies with in- and outpatient treatment (mostly not exclusively multidisciplinary) have shown that the majority of patients experience a significant improvement in physical function and quality of life [
43,
44,
45,
68,
69,
70]. This also highlights the complexity of measuring outcome in this heterogeneous disorder. Capturing an overall picture of the full spectrum of possible FND symptoms, including additional physical symptoms (fatigue, pain, gastrointestinal problems, etc.) and possible psychologic/psychiatric comorbidities (anxiety, depression, dissociation, etc.) is a challenge. Long-term variability of symptoms and discrepancy between objective measures and patients’ subjective experiences of symptom make measurement even more difficult [
71]. Early diagnosis is important to prevent chronification. In fact, longer duration of symptoms before diagnosis seems to correlate with a negative outcome [
72]. Receiving health-related benefits has also a negative effect on outcome [
69]. Psychiatric comorbidity was found to be an inconsistent predictor of poor outcome [
73]. According to available studies [
73,
74] and our own experience, early diagnosis and acceptance, as well as a good understanding of the disorder by the patient, are associated with a better outcome. Investment in broader knowledge of FND in health workers and the development of easily accessible treatment plans could therefore improve future outcome measurements significantly. With this goal in mind, we have been offering since this year an intensive in-patient program for three weeks according to current evidence of other worldwide specialized centers. Specifically, a one-week intensive rehabilitation program specialized for functional motor disorders in Louisville (Frazier Rehab Institute in Louisville, KY, USA) [
10] showed an improvement in 86% of patients at discharge, with a long-term effect of significant improvement in 69% of patients six months later. Similar results are obtained by a two-week in-patient program in Boston [
8]. A mutual feature of these in-patient programs is an intensive and specialized physio- and psychotherapeutical approach, as we are now also offering in Bern. Especially patients who are recently diagnosed with FND, including ambulatory unmanageable FND patients referred from the neurological ward and emergency department, benefit from this program by preventing chronification.
2.9. Training and Research on FND
In most pre-graduate curriculum of medical studies and healthcare studies (such as physiotherapy or nursing schools), FND is only addressed marginally and often with outdated understanding of a purely psychogenic model. As a consequence, there is still a lack of specialized knowledge in the daily clinical practice of health workers as well as in the general population. Considering the high prevalence of FND, better knowledge on diagnosis and treatment of this pathology is needed.
Our new FND care setting is integrating bedside clinical teaching at different stages of the medical studies and residency as well as in other health workers. Since a few years, we have been holding lectures at medical universities of Bern, Lausanne, and Geneva to make students aware of the topic at an early stage. Medical students also have the possibility to visit our FND unit during their internship at the neurological department. At an advanced stage, neurological residents are actively involved in our consultations and, for those with special interest, fellowships in our in- and out-patient program can be organized. Together with our physiotherapists and psychologists, we also organize training courses for physiotherapists and psychologists as well as nursing staff on therapeutic principals in FND.
Furthermore, close collaboration of the clinical and research team of our university specialized center will provide data from in- and out-patient treatment to design large scale clinical trials. This will contribute to further research towards a better pathophysiological understanding of this disorder but mostly this new clinical setting can ideally host clinical trials on new treatment options.


 and
and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}





