Bilateral Breast Edema: Case Report and Review of the Literature



Abstract
:1. Introduction
2. Case Presentation Section
2.1. Clinical History
2.2. Symptoms and Duration
2.3. Clinical Examination and Initial Assessment
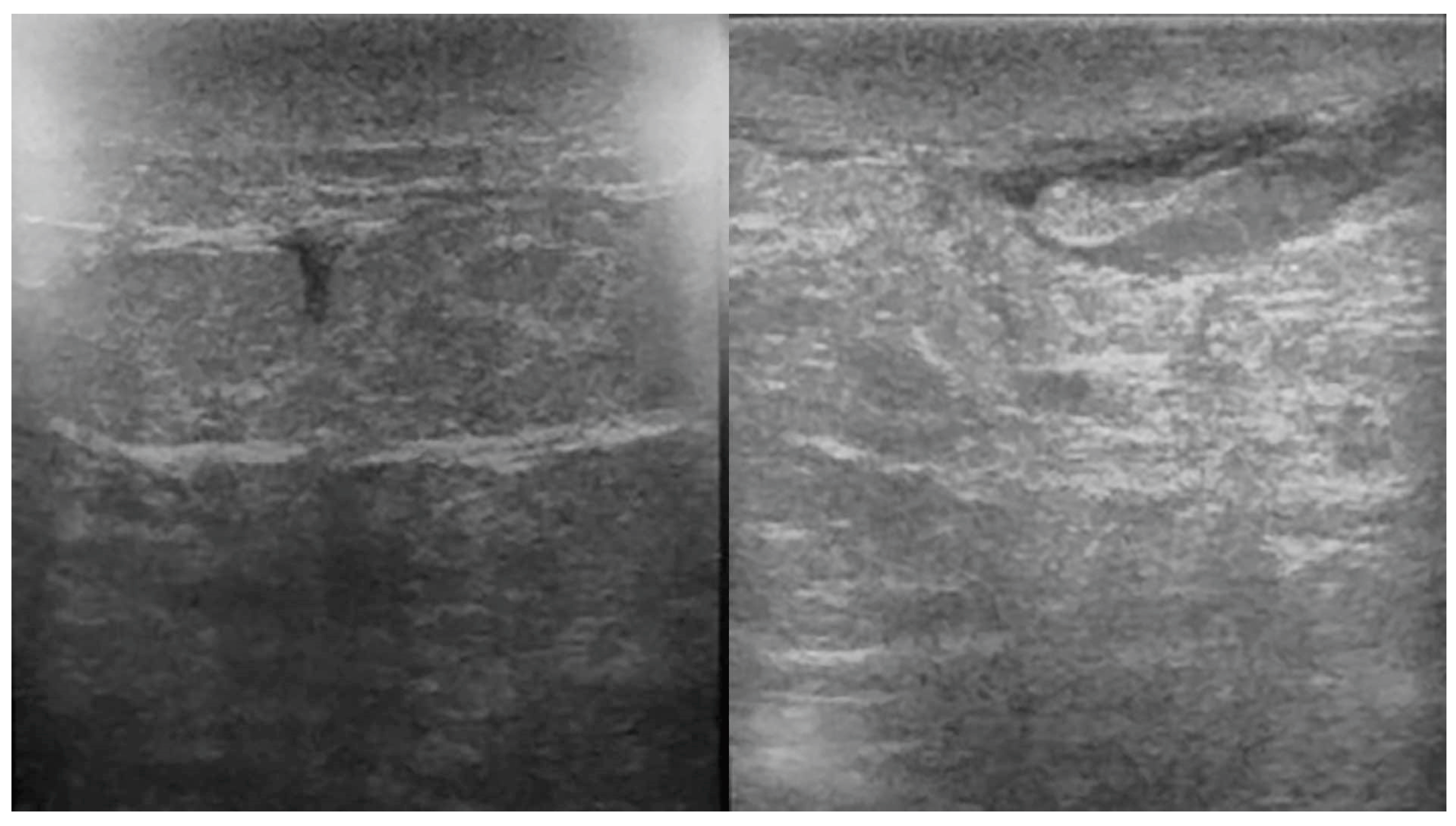
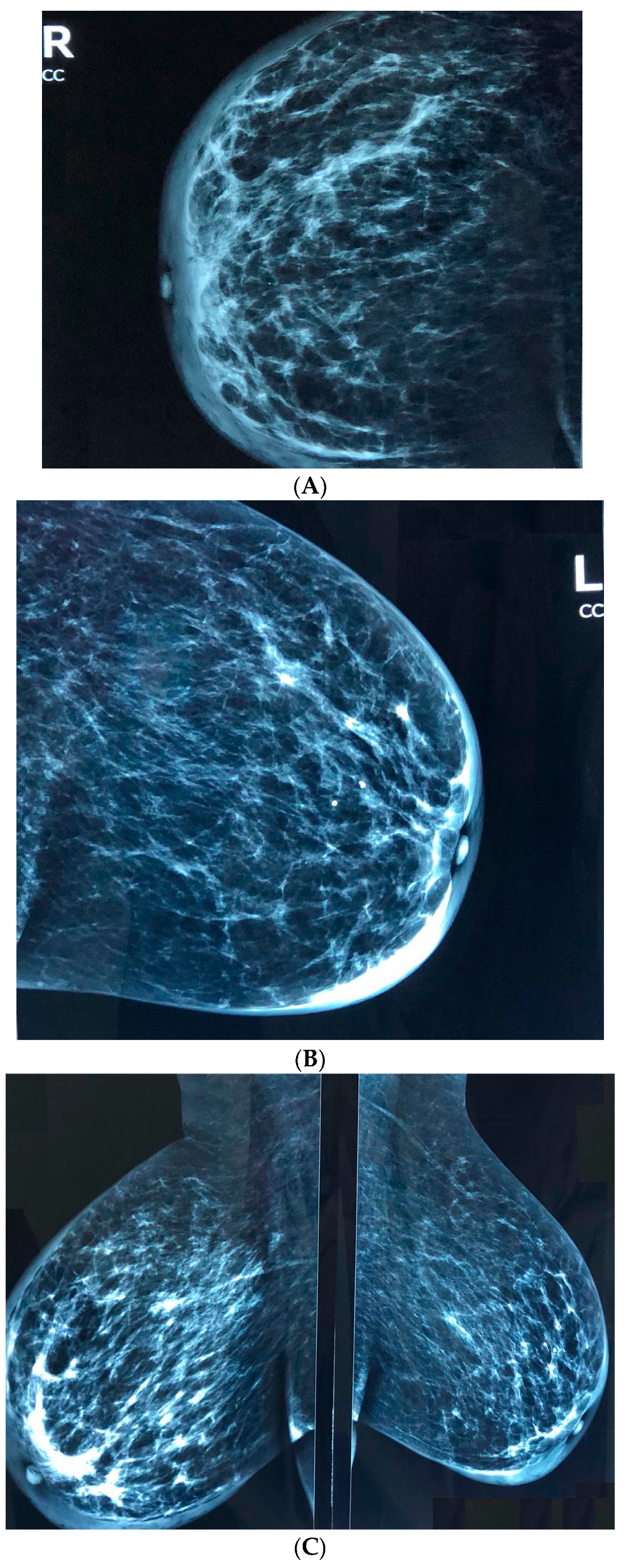
2.4. Tests
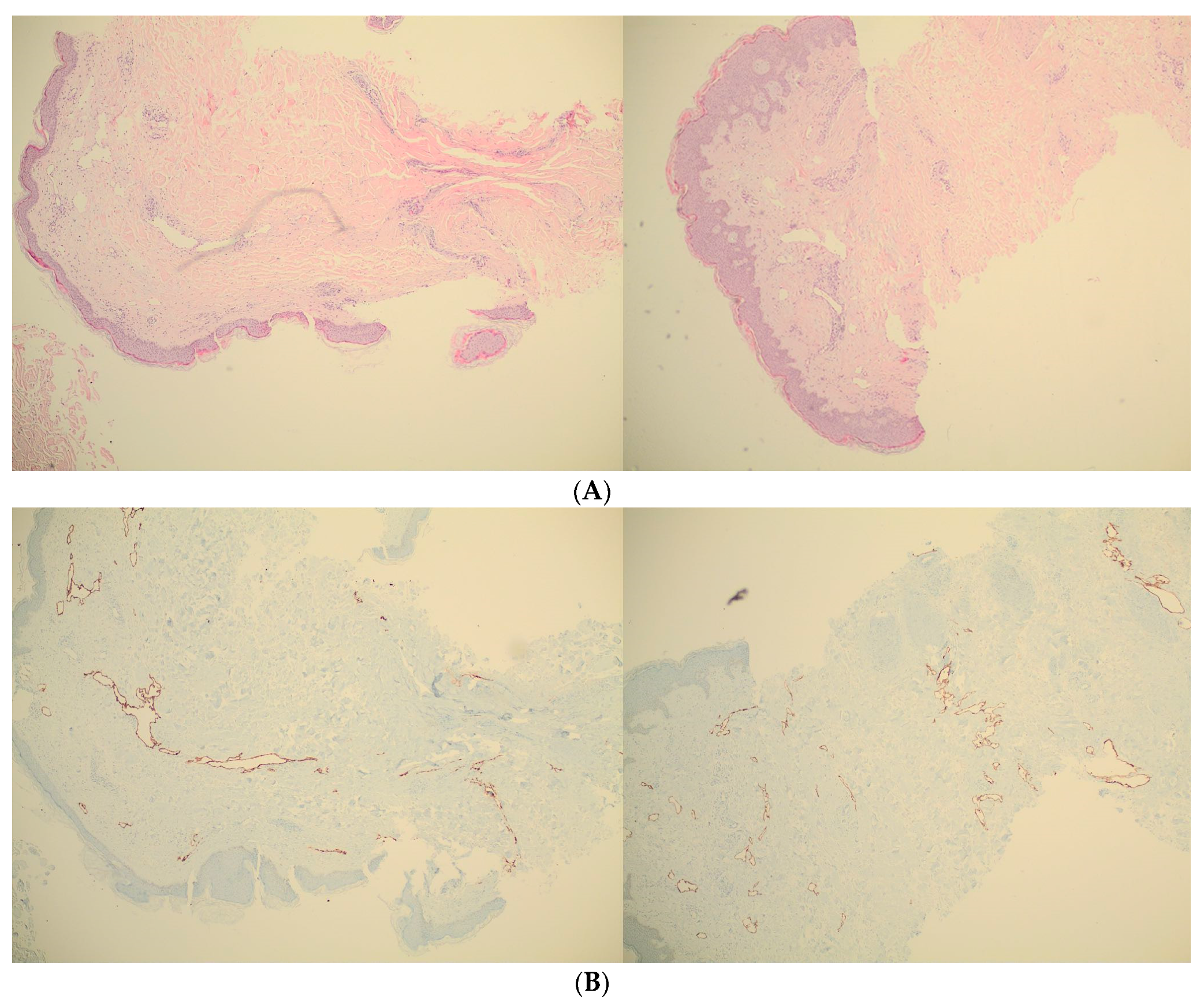
2.5. Pathology Results
3. Medical Therapy and Follow-Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Panourgias, E. Inflammatory intramammary lymph node—A benign lesion simulating malignancy ON breast MRI. Acta Endocrinol. Buchar. 2009, 5, 259–264. [Google Scholar] [CrossRef]
- Schairer, C.; Soliman, A.S.; Omar, S.; Khaled, H.; Eissa, S.; Ayed, F.B.; Khalafallah, S.; Ayoub, W.B.; Kantor, E.D.; Merajver, S.; et al. Assessment of Diagnosis of Inflammatory Breast Cancer Cases at Two Cancer Centers in Egypt and Tunisia. Cancer Med. 2013, 2, 178–184. [Google Scholar] [CrossRef] [PubMed]
- Zervoudis, S.; Iatrakis, G.; Tomara, E.; Bothou, A.; Papadopoulos, G.; Tsakiris, G. Main Controversies in Breast Cancer. World J. Clin. Oncol. 2014, 5, 359–373. [Google Scholar] [CrossRef] [PubMed]
- Goktan, C.; Pekindil, G.; Orguc, S.; Coskun, T.; Serter, S. Bilateral Breast Edema in Intestinal Lymphangiectasia. Breast J. 2005, 11, 360. [Google Scholar] [CrossRef] [PubMed]
- Maeda, M.; Fugimoto, N.; Satoh, T. Bilateral Breast Edema Associated with Nephrotic Syndrome. Eur. J. Dermatol. EJD 2013, 23, 739–740. [Google Scholar] [CrossRef] [PubMed]
- Young-Afat, D.A.; Gregorowitsch, M.L.; van den Bongard, D.H.; Burgmans, I.; van der Pol, C.C.; Witkamp, A.J.; Bijlsma, R.M.; Koelemij, R.; Schoenmaeckers, E.J.; Jonasse, Y.; et al. Breast Edema Following Breast-Conserving Surgery and Radiotherapy: Patient-Reported Prevalence, Determinants, and Effect on Health-Related Quality of Life. JNCI Cancer Spectr. 2019, 3, pkz011. [Google Scholar] [CrossRef] [PubMed]
- Miller, V.; Riordan, J. Treating Postpartum Breast Edema with Areolar Compression. J. Hum. Lact. Off. J. Int. Lact. Consult. Assoc. 2004, 20, 223–226. [Google Scholar] [CrossRef] [PubMed]
- Kujawa-Myles, S.; Noel-Weiss, J.; Dunn, S.; Peterson, W.E.; Cotterman, K.J. Maternal intravenous fluids and postpartum breast changes: A pilot observational study. Int. Breastfeed. J. 2015, 10, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramos, R.M.L.; Armán, F.J.A.; García, M.T.R.; Carrero, E.B.; Fariñas, I. Breast Edema. A Pictorial Review with Pathologic Correlation. Available online: https://www.semanticscholar.org/paper/Breast-edema.-A-pictorial-review-with-pathologic-Ramos-Arm%C3%A1n/2447fda13d9ab77d23f43e9741c34197e6ba9c6c (accessed on 17 May 2020).
- Dhali, T.K.; Chahar, M. Thyroid Dermopathy-a Diagnostic Clue of Hidden Hyperthyroidism. Dermato-Endocrinology 2014, 6, e981078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masannat, Y.A.; Peter, M.; Turton, P.; Shaaban, A.M. Case Report of Bilateral Inflammatory Breast Cancer. Eur. J. Cancer Care 2010, 19, 558–560. [Google Scholar] [CrossRef] [PubMed]
- Verbelen, H.; Gebruers, N.; Beyers, T.; De Monie, A.-C.; Tjalma, W. Breast edema in breast cancer patients following breast- conserving surgery and radiotherapy: A systematic review. Breast Cancer Res. Treat. 2014, 147, 463–471. [Google Scholar] [CrossRef] [PubMed]
- Cao, M.M.; Hoyt, A.C.; Bassett, L.W. Mammographic Signs of Systemic Disease. Radiographics 2011, 31, 1085–1100. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1. Chief complaint: bilateral breast edema |
| 2. Clinical examination |
| 3. Breast ultrasound |
| 4. Mammography |
| 5. Magnetic resonance imaging of the breast |
| 6. Core biopsy |
| 7. Pathologic results without “formal” diagnosis |
| 8. Symptomatic treatment |
| 9. Remission of breast edema |
| 10. An idiopathic case of bilateral breast edema was concluded |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vouxinou, A.D.; Iatrakis, G.M.; Zervoudis, S.; Bothou, A.; Tsitsiou, S.; Markja, A.; Margelis, Z.; Tooulias, C.A.; Antoniou, E. Bilateral Breast Edema: Case Report and Review of the Literature. Reports 2020, 3, 18. https://0-doi-org.brum.beds.ac.uk/10.3390/reports3030018
Vouxinou AD, Iatrakis GM, Zervoudis S, Bothou A, Tsitsiou S, Markja A, Margelis Z, Tooulias CA, Antoniou E. Bilateral Breast Edema: Case Report and Review of the Literature. Reports. 2020; 3(3):18. https://0-doi-org.brum.beds.ac.uk/10.3390/reports3030018
Chicago/Turabian StyleVouxinou, Andriani D., Georgios M. Iatrakis, Stefanos Zervoudis, Anastasia Bothou, Sofia Tsitsiou, Anisa Markja, Zois Margelis, Christos A. Tooulias, and Evangelia Antoniou. 2020. "Bilateral Breast Edema: Case Report and Review of the Literature" Reports 3, no. 3: 18. https://0-doi-org.brum.beds.ac.uk/10.3390/reports3030018