1. Introduction
Helicobacter pylori (Hp) is a spiral-shaped Gram-negative bacterium that colonizes the stomach, and it is characterized by high urease enzyme activity. Hp infection is widely diffuse, since it involves around half of the world population, and it always leads to gastric mucosal inflammation and damage, despite that in the vast majority of cases it runs completely asymptomatically [
1]. The basic lesion is the progressive mucosal inflammation that may eventually lead to peptic ulcer disease, mucosa-associated lymphatic tissue (MALT) lymphoma and gastric adenocarcinoma.
The diagnosis of Hp infection can be assessed by a variety of invasive and non-invasive tests [
2]. Upper gastrointestinal endoscopy with histological evaluation of biopsies, taken from the gastric body and antrum, is the current reference standard for the detection of Hp infection. Specific stains such as Giemsa or Warthin–Starry can enhance the visibility of Hp on histological sections, and consequently the sensitivity of the assay. A higher specificity of Hp detection in biopsy samples may be obtained by the use of more complex and expensive tests such as immunochemistry, polymerase chain reaction (PCR), or bacterial culture. PCR can also be used for the detection of clarithromycin and fluoroquinolone resistance, and the culture of gastric biopsies for Hp has the supplementary benefit of characterizing the antimicrobial susceptibility of specific Hp strains but has the disadvantage of a low sensitivity [
3]. Noninvasive methods include the urea breath test, stool antigen and serum IgG tests, which differ in diagnostic accuracy and clinical application [
4].
In addition to these laboratory-based diagnostic assays, Hp infection may be also diagnosed with the use of point-of-care or bedside test—the rapid urease test (RUT), that is currently indicated by guidelines as a first-line diagnostic test [
5]. Hp urease is essential for the metabolism of bacteria and colonization of the gastric mucosa. The presence of this enzyme in a clinical sample may be visualized by hydrolyzing urea in a test medium to ammonia and carbon dioxide. The resulting high local concentration of bicarbonate produced by urea degradation raises the pH that can be detected by a color-based pH-indicator [
6], usually phenol red, that changes the color from yellow (pH 6.8) to magenta (pH 8.4). The time needed for color change is inversely proportional to bacterial density in the biopsy. Different RUTs display different reaction times to provide accurate results, and a minimum of 105 organisms is usually required for a positive finding in agar medium [
7].
Biopsy urease tests can determine the presence of urease activity in a gastric specimen. Multiple commercial RUT kits are available in different formats. The major advantage of this type of tests is the availability of a bed-side test within minutes to a few hours, which allows the clinicians to have results shortly after endoscopy. In this regard, RUTs represent accurate and rapid tests for the diagnosis of Hp infection, with evident positive implication for the correct management of the patients. In fact, the possibility to have the results right after the endoscopic procedure allows the clinician to make a correct diagnosis and eventually to prescribe eradication therapy, thus avoiding multiple visits and resources wasting. Moreover, the possibility to have Hp results in a short time may also increase the test accuracy, since other bacterial species also display slow urease activity that can lead to false delayed positive results.
Although specificity and sensitivity between 90 and 95% for RUTs has been reported, in particular for 24 h reads, false positive and false negative test results are possible, mostly if the test response time is slow. Furthermore, treatment with proton pump inhibitors (PPIs) are reported to lead to false negative results because these drugs reduce the colonization density of Hp within the stomach. Siavoshi et al. [
8] reported a reduction in sensitivity of the
Campylobacter pylori (CP) test at 1 h from 92% without PPI to 74% during PPI assumption. Moreover, it has been demonstrated that PPIs exhibit bactericidal activity against Hp and can cause elevation of pH level in the stomach, which in turn may lead to an accumulation of the ammonia produced by Hp urease and the reduction in bacterial viability. PPIs can also induce spiral forms of Hp to turn into coccoid ones with lower urease activity [
9]. Lansoprazole exhibited bactericidal activity 4-fold higher than omeprazole and 16-fold higher than pantoprazole, respectively. The inhibitory effect of lansoprazole on RUTs was twice more than omeprazole and six times more than pantoprazole. These results indicate that the effect of PPI on Hp could depend on the kind and dosage of PPI consumed by patients [
10].
Since McNulty and Wise first described the biopsy urease test in 1985 [
11], several modifications have been developed and validated in an attempt to improve the feasibility, accuracy and rapidity of the tests. In particular, modification of the media and of the devices has been proposed, with semi-solid phase (agar gel), liquid phase (bottle) and solid phase (dry plate) being the most popular ones. However, the accuracy and rapidity of the test is still a matter of debate, and no specific recommendations are available about the desired characteristic of RUTs in clinical practice. In particular, the ideal time point for optimal reading for the old generation RUTs often exceeds 1–3 h, therefore limiting practical advantages and requiring extra time for endoscopists and patients. The iNatal duo test is a new generation of ultra-rapid RUT that offers high accuracy and availability of results in a few minutes, allowing rapid response and fast managing of patients, who can be diagnosed with Hp infection and eventually have treatment prescription before leaving the endoscopy room.
The aim of the present study is to prospectively evaluate the diagnostic accuracy and reaction time of the new-generation ultra-rapid urease test, the iNatal duo test, in comparison with other commercial RUTs in different formats for the diagnosis of Hp infection, considering histology as the gold standard.
2. Results
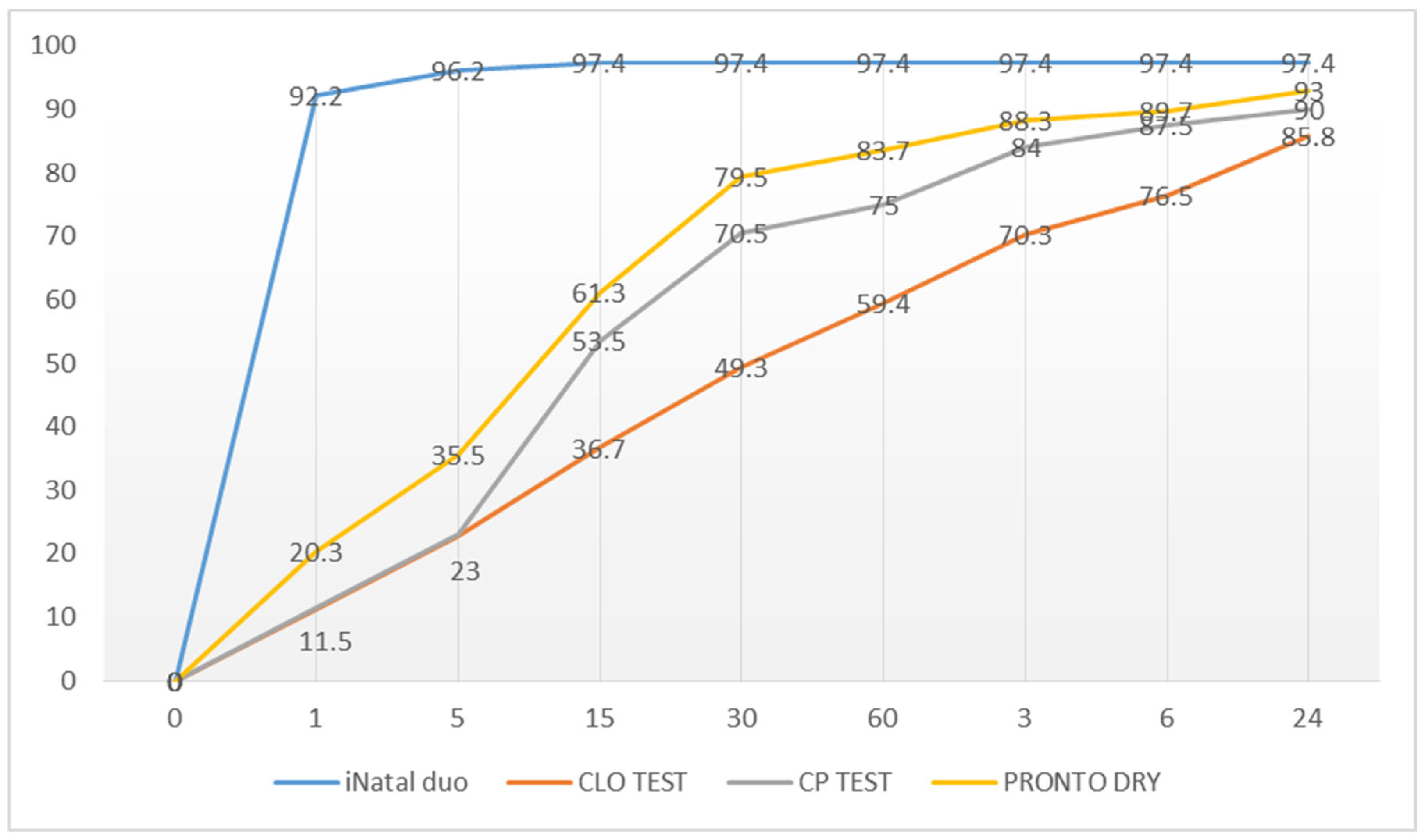
A total of 1122 consecutive dyspeptic patients were included in this study. Among those, 924 (544(59%) females, mean age 52) were not taking PPIs and were evaluated for accuracy comparison of the four RUTs. In those patients, Hp infection was diagnosed by histology in 225 (24.3%) patients, while the other 699 patients were regarded as negative. No false positive was recorded for all the tested RUTs, so that the specificity of the tests was 100%. Considering sensitivity, consistent differences emerged among the RUTs at different time points (
Figure 1). The number of positive patients at different time points for the different RUTs is represented in
Table 1. The iNatal duo test has higher sensitivity at every time point. The second more sensible test was the Pronto Dry test, but iNatal duo showed significantly better sensitivity compared with that one at every time point, too (at 5 min: 96% vs. 36%,
p < 0.0001; at 24 h: 98% vs. 93%,
p < 0.05 by chi-squared test).
In particular, the global sensitivity of the iNatal duo test was 97.4% (with 100% specificity), the positive predictive value (VPN) was 100% and the negative predictive value (VPP) was 99.3%. The global results of the iNatal duo test in patients not taking PPIs and the accuracy data at different time points are presented in
Table 2 and
Table 3. The iNatal duo test reached the highest performance as early as 15 min, and no other additional positive result was observed thereafter.
The iNatal duo test displayed a higher concordance rate (κ) with histology at every time point (at 15 min: iNatal duo 0.99, CLO 0.46, CP: 0.63, Pronto 0.71; at 30 min: iNatal duo 0.99, CLO 0.60, CP 0.78, Pronto 0.85; at 6 h: iNatal duo 0.99, CLO 0.83, CP 0.91, Pronto 0.93; at 24 h: iNatal duo 0.99, CLO 0.90, CP 0.93, Pronto 0.95).
We then intended to test the accuracy of the most accurate RUT, i.e., the iNalal duo test, in an additional sub-group of 198 patients who had a concomitant assumption of PPIs. The global results of the iNatal duo test, in patients under PPI therapy, and the accuracy data at different time points are presented in
Table 4 and
Table 5. Concomitant PPI use did not affect the diagnostic accuracy of the iNatal duo test.
3. Discussion and Conclusions
Since Hp is the most important cause of gastritis, gastro-duodenal ulcers and gastric cancers, different tests have been developed to identify Hp infection. RUTs are used widely throughout the world in endoscopy units to determine if patients are infected with Hp. Although the basis of all these tests is the breakdown of urea by the urease activity of Hp, differences exist between the tests, and the configuration of kits is slightly different. In the evaluation of an RUT, two parameters need to be considered with priority: the test accuracy and the rapidity of the results. Factors affecting the diagnostic accuracy of the rapid urease test have been previously studied. Among others, a low density of the pathogen in the gastric mucosa can give false negative results. Furthermore, a progression of the inflammation induced by Hp, by means of an increase in gastric atrophy, can lead to a decrease in detectable bacteria [
12]. Another factor potentially influencing the diagnostic accuracy of RUTs is hypochlorhydria, typically present in PPI users. This condition can lead to false positive results since other bacteria with low urease activity might be able to colonize the stomach, and thus cause delayed positive reaction of RUTs [
13]. Two studies from India showed that the prevalence of Hp infection in adults approaches 90% in many developing countries, particularly those in the tropics [
14,
15]. In 2007, Lynn et al. [
16], in their province-based individual studies, have shown that in industrialized parts of the world (Western Europe, United States, Canada and Australia), the percentage of infected adults is lower. Chen et al. [
17] showed that the prevalence of Hp infection has been steadily declining in industrialized and emerging countries, which is probably a reflection of improved sanitary conditions, as well as the widespread use of antibiotics. Despite declining rates of Hp infection, in general, the prevalence rate of Hp in patients who undergo endoscopy remains significant. Therefore, Hp should be considered in all gastric biopsy specimens examined, regardless of the patient’s age or prevalence. The diagnosis of Hp gastritis based solely on the endoscopic gross appearance of the gastric mucosa is not recommended. The accurate diagnosis of Hp gastritis rests either on the pathologic evaluation of gastric mucosal biopsies or by the detection of urease in mucosal specimens by rapid urease biopsy tests.
Previous studies have compared single RUTs with histological staining: Said et al. [
18] compared CLO test, Pronto Dry and histology in 208 Asian patients, and Van Keeken et al. [
19] matched the CLO test with GUT RUT and with histological results in 116 Dutch patients. Very recently, Eslaminejad et al. [
20] compared the CLO test with histology in 146 Iranian patients. All RUTs showed almost similar rates of sensitivity and specificity compared with the present study in patients not treated with PPI within the last 14 days before biopsy. Nonetheless, most of the previous studies evaluated the RUTs’ results at 6 or 24 h, while accuracy by 30 min, which is when the patient is still in the endoscopy room and can be therefore informed of the results right away, has not been considered for old-generation RUTs. In fact, the availability of affordable test results in a short time is important for the timely and correct management of the patient, who can be advised and eventually treated in a single time right after the endoscopic procedure. This implies obvious advantages both from a clinical and economic point of view, since unnecessary repeated visits are avoided, with clear, direct and indirect cost saving.
In the present study, the new-generation ultra-rapid RUT iNatal Duo test showed significant higher sensitivity compared with the other RUTs, with affordable results as early as within 5 min, reaching higher accuracy at 15 min. The rapidity of the results is due to the liquid media and the absence of buffer solutions, which allow a fast reaction. The effectiveness of ultra-rapid new-generation RUTs have been recently investigated. The liquid pre-Ox HUT test showed a sensitivity of 85%, a specificity of 94%, a positive predictive value of 80% and a negative predictive value of 96% in 183 patients after 10 min time [
21].
For the first time, in the present study, several RUTs were tested together in a large set of patients in order to evaluate both the accuracy and rapidity of results. The iNatal duo test showed consistently better results than the other RUTs, and the concomitant PPI utilization did not affect the accuracy of the test. In fact, as PPIs are available, they are very commonly used in patients with dyspeptic symptoms in the general population. Acid-suppressing medication prolongs the time to positivity for the rapid urease tests and may increase the numbers of false negative tests.
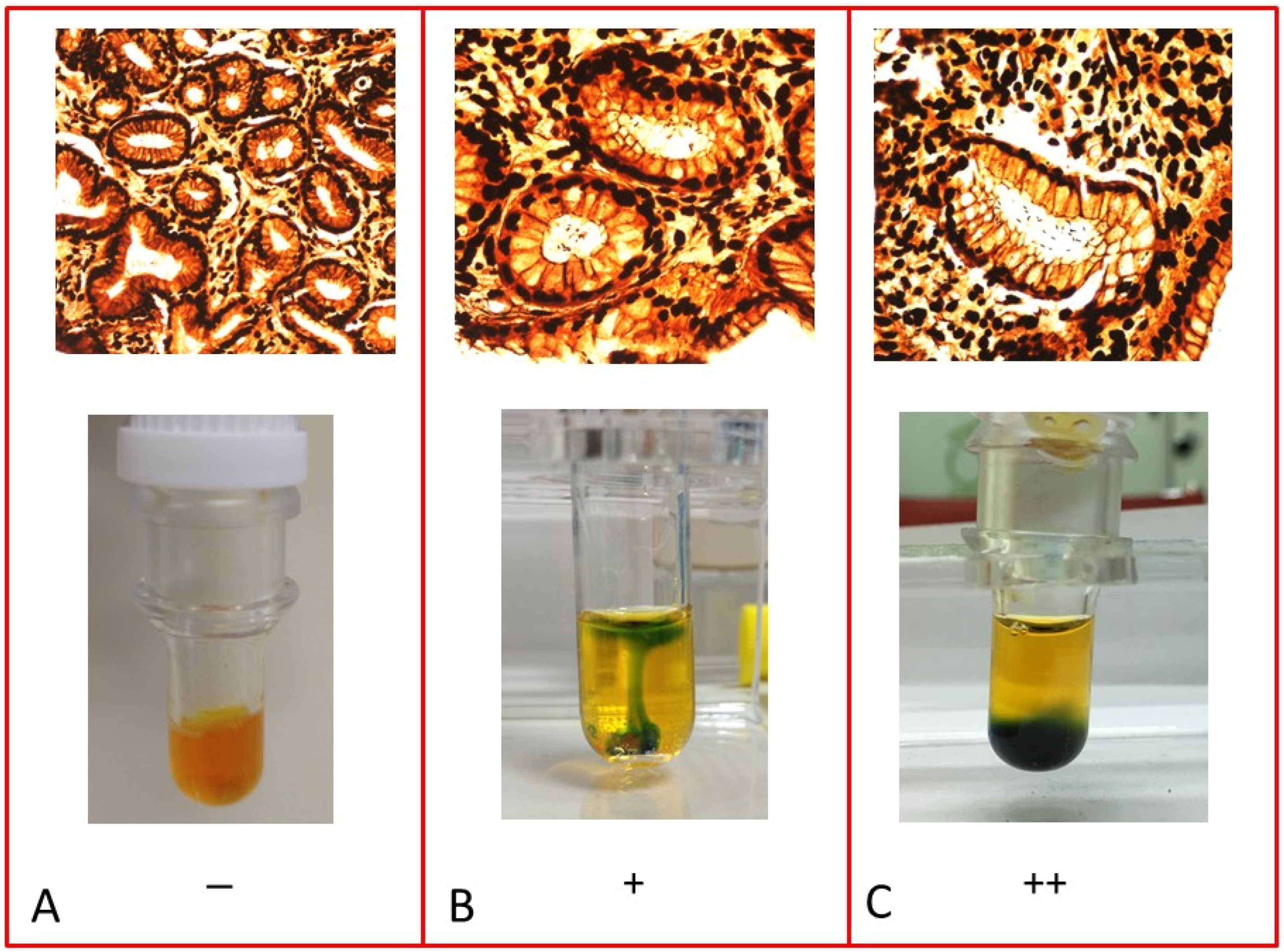
The iNatal duo test is very feasible and user-friendly, since it gives a very distinct color change, which helps even in the case of low bacterial concentration (
Figure 2). Due to the bromothymol blue indicator, the positive reaction is visible when, around the biopsy specimen, the yellow/orange color of test wells turns to a distinct dark green–blue, which is more clearly distinguishable compared with that obtained by the phenol red indicator used by the other RUTs. The advantage of the new iNatal duo test is that the results are affordable and available faster than that with other RUTs, so that Hp infection can be diagnosed and eventually managed before the patient is discharged from the endoscopic unit. It is very simple to perform and does not require special expertise, complex preparation nor extra time to the endoscopist.
A limitation of the present study is that only histology was considered as gold standard, and more accurate diagnostic tools, such as PCR or culture methods, have not been included in this study. Considering the sole histology may explain, at least in part, the high specificity of all the tested RUTs (100%). Moreover, relying on histology as gold standard may be a possible flaw, in particular for the Hp diagnosis in PPI users, since it is in those patients that histology may lose accuracy. Another shortcoming of the present study could be that, in PPI users, only the iNatal duo test was assessed, and no comparison was made with the other RUTs. Finally, the cost saving of the iNatal duo test was only indirectly speculated, and no specific cost analysis was performed in this study. In this regard, it would be interesting to compare the accuracy, rapidity and cost of the iNatal duo test compared with modern genetic tests that may provide rapid results on Hp quantification, virulence and antibiotic resistance [
22].
In conclusion, the present prospective investigation on a large set of patients demonstrates that the new-generation iNatal duo test is accurate and rapid for the diagnosis of Hp infection and can contribute to the effective management of patients in endoscopic centers.
4. Materials and Methods
In the present study, consecutive patients referred to Ospedale Civile di Palestrina-ASL Roma 5 and S. Giovanni Addolorata Hospital in Rome, for an upper GI endoscopy, from January 2018 to December 2020, were included. After an overnight fasting (6 h), all the selected subjects underwent upper gastrointestinal endoscopy with flexible video-endoscope, and the endoscopic findings were recorded. Patients gave written informed consent prior to the procedure, and demographic data (age and sex), indication for upper gastrointestinal endoscopy and concomitant PPI treatment were recorded. Patients were routinely anesthetized for the procedure with midazolam and propofol and monitored by pulse oxymeter and noninvasive blood pressure measurement. For each RUT test, we obtained one biopsy specimen from the lesser curvature of the antrum and one from the corpus. For histological examination, two additional biopsy specimens were collected in the antrum and two in the corpus and fixed in neutral-buffered 4% formaldehyde. Hp identification was performed on Warthin–Starry-stained sections of paraffin-embedded tissue.
In the present study, we analyzed the performance of different generations of RUTs:
Campylobacter pylori (CP) test (Pharmangelini, Rome, Italy),
Campylobacter-Like Organism (CLO) test (Avanos Medical Devices, Alpharetta, GA, USA), Pronto Dry (Sofar, Trezzano Rosa, Italy), and iNatal Duo test (PharmExtracta, Pontenure, Italy). The media contained in the CLO test, the CP test and Pronto Dry was semi-solid phase (agar gel), liquid phase (bottle) and solid phase (dry plate), respectively. All the procedures for the RUTs were performed according to manufacturers’ instructions. The time of biopsy placement was recorded, and the wells were inspected for color change from yellow to dark green–blue (iNatal duo test,
Figure 2) or from yellow to magenta (other RUTs) at room temperature after 1, 5, 15, 30, 60 min, 3 and 24 h. The test was considered positive if a change in color was observed and recorded. The results were registered and compared with the histological evaluation, set as reference parameter, to evaluate the diagnostic accuracy of the RUTs.
Defining the histological result as the reference standard, sensitivity, specificity, positive and negative predictive value were calculated for all the RUTs in patients not taking PPI at the time of endoscopy or during the two weeks before (n = 942). The iNatal duo test’s accuracy was also evaluated in a subgroup of patients taking PPI (n = 198). Comparison in the different groups was evaluated by chi-squared and one-way ANOVA test, when indicated, and correlation with histology was calculated by the constant of correlation (κ). A value of p < 0.05 was considered significant. MedCalc software (MedCalc Software Ltd, Ostend, Belgium) version 12.5 was used for statistical calculations.


 ,
, 


{kind=link}
{kind=link}