

Healthcare Provider Reports on Social Determinants of Health in Opioid Treatment

1
College of Social Work, University of Utah, 395 South 1500 East, Salt Lake City, UT 84112, USA
2
Department of Biomedical Informatics, Utah Clinical and Translational Science Institute, University of Utah, 395 South 1500 East, Salt Lake City, UT 84112, USA
*
Author to whom correspondence should be addressed.
Psych 2023, 5(1), 60-69; https://0-doi-org.brum.beds.ac.uk/10.3390/psych5010007
Submission received: 4 December 2022
/
Revised: 11 January 2023
/
Accepted: 17 January 2023
/
Published: 30 January 2023
(This article belongs to the Special Issue Prominent Papers in Psych 2021–2023!)
Abstract
:Opioid overdose and death from overdose continue to present a pressing problem in the United States. It is well-established that a range of social and economic factors, often referred to as social determinants of health (SDOH), are associated with increased opioid overdose and death. Few studies have examined healthcare provider reports on social and economic barriers to opioid treatment. Healthcare providers (N = 161) participating in opioid Project ECHO (Extension for Community Healthcare Outcomes) programs were surveyed on the portion of their patients experiencing 15 different SDOH. Results indicated that multiple determinants were experienced by the majority of their patients, with poverty as the most commonly experienced social determinant (72%). Regression analyses indicated that physicians generally reported a lower portion of patients experiencing SDOH compared with social workers, nurse practitioners, and other healthcare providers. Results suggest that SDOH are widely experienced by patients seeking opioid treatment and that professional backgrounds may be related to reports of SDOH at the point of care. Multi-disciplinary teams involving social workers, nurse practitioners, and other healthcare providers may improve the identification of social and economic barriers to opioid treatment.
1. Introduction
Since 1999, opioids have contributed to over 500,000 deaths in the United States [1]. Largely due to increasing mortality rates from fatal drug overdoses, 2014 to 2017 marked the first three-year decline in life expectancy in the United States (US) in 100 years [2]. Referred to as a “triple wave epidemic,” prescription opioids, heroin, and synthetic opioids such as fentanyl arose in succession over approximately 15 years to reverse decades of gains in life expectancy in the US [3]. Despite some success for supply and demand reduction strategies, opioids have proliferated through illegal markets for heroin and fentanyl [3], and overdose deaths have continued to rise [4]. Extensive empirical research has shown that socioeconomically disadvantaged populations are at greater risk for opioid overdose and death from overdose [5,6]. As opioid prescribing rates have dropped, it is likely that social and economic factors are playing an expanded role in maintaining demand for opioids in recent years [7,8]. Importantly, socioeconomically disadvantaged populations experience significant barriers to obtaining safe and effective medical treatments [8]. These barriers manifest as both limited access to medications for opioid use disorders (MOUD) and lack of consistent pain management treatment [8]. The set of social and economic factors that contribute to barriers to medical treatments are commonly organized under the social determinants of health (SDOH) framework and include education, poverty, employment, race/ethnicity, neighborhood environment, and geographic region [9,10]. There is a growing consensus that deeper engagement with SDOH in both medical education and clinical practice is critical to understanding the trajectory of the opioid epidemic, improving access to safe and effective opioid treatment, and formulating public health responses at federal, state, and community levels [8,11].
Social and economic factors can impact the opioid crisis through multiple pathways. Much has been written about social and economic factors related to opioid use, overdose, and mortality under the umbrella of “deaths of despair” [12] (p. 3). Growing demand for opioids has coincided with multi-decade trends in increased economic distress resulting from deindustrialization, loss of manufacturing jobs, chronic underemployment, and reduced economic and social mobility [6,12,13]. As a result, numerous studies have shown that geographic areas experiencing greater economic distress also experience higher rates of opioid use, overdose, and death from overdose [6,8,12,14]. Fewer studies, however, have examined the potential role of social and economic factors in opioid treatment. To date, research on this topic has largely emphasized reduced access to FDA-approved MOUD such as buprenorphine, methadone, and naltrexone among rural populations [15,16]. Regulatory hurdles, lack of providers with MOUD waivers, transportation infrastructure, and stigma among providers are often cited as the primary barriers to MOUD in rural areas [16]. Experts have noted that reducing regulatory barriers or increasing the number of providers is unlikely to be sufficient to increase treatment rates [17], and successful opioid treatment likely depends on also addressing a range of social and economic factors [7,8]. As such, a deeper understanding of the social and economic factors that create barriers to opioid treatment is necessary for optimizing strategies to reduce treatment barriers.
In recent years, healthcare provider education and consultation programs have been designed specifically to increase access to modern treatment practices among providers serving disadvantaged patient populations. Project ECHO (Extension for Community Healthcare Outcomes) is one such program offering a telementoring platform designed to address knowledge gaps among providers [18]. ECHO programs offer continuing medical education, provide case consultation with subject matters experts, and improve access to specialized medical knowledge for patients in underserved areas [18]. Given the program goal, healthcare providers participating in Project ECHO are likely to treat patient populations encountering a range of social and economic barriers to opioid treatment. As such, these providers have in-depth, first-hand information on social and economic barriers to opioid treatment.
Relatively few attempts have been made to assess healthcare provider or patient reports on social or economic barriers to opioid treatment. One recent systematic review examining provider and patient perspectives on MOUD did not include any studies focused on the role of economic factors [19]. Provider reports on social factors were limited to the negative impact of social stigma for both providers and patients on providing MOUD [19]. Currently available studies on provider reports have largely emphasized challenges from the provider end (e.g., regulatory issues, lack of provider training on MOUD, misinformation on MOUD), as opposed to barriers created by the contexts in which patient care takes place. A recent systematic review of client reports on barriers to accessing MOUD did identify multiple social and economic factors including low health literacy, stigma from future employers, social stigma, treatment costs, long travel distance to care, and chaotic lifestyles [20]. Given recent calls for a stronger consideration of social and economic factors in combatting the opioid crisis, an examination of healthcare provider reports on social and economic barriers to treatment is warranted. As such, the aim of the current study is to describe healthcare provider reports on the portion of their patients in opioid treatment that experience specific SDOH. Additionally, this study also sought to explore differences in reports of SDOH by healthcare provider and clinic characteristics. Due to the exploratory nature of this study, no a priori hypotheses were specified on the distribution of reported social determinants or their interrelationships. Given the typical roles and responsibilities of social workers in clinic settings, we expect social workers to report higher percentages of their patients experiencing multiple SDOH.
2. Materials and Methods
2.1. Participants and Procedures
Data were collected from healthcare providers that signed up to attend at least one session of a Project ECHO program related to opioids, chronic pain, substance use, or medication assisted treatment. Regional ECHO program hubs are situated across the US and Canada and maintain email contacts list for each program specialty topic. Requests to distribute a survey were sent by email to 180 contact persons at 86 hubs sponsoring ECHO programs related to opioids, chronic pain, substance use, or medication-assisted treatment. Potential respondents were provided background information on the goals of the research project and a brief definition of SDOH in the context of opioid treatment. The survey was administered from December 2020 to February 2021 using the REDCap platform [21]. Respondents that completed at least one question regarding SDOH were included in the sample (N = 161). No incentives were provided for participation.
2.2. Measures
The survey included questions on professional experience, involvement with opioid-focused ECHO programs, and reports on their patients’ experiences with SDOH. Respondents were asked to provide information on their professional background (e.g., job title, years in practice), current employment (e.g., health clinic name and location), involvement with opioid-focused ECHO programs, comfort in identifying SDOH at the point of care, and facility resources to address SDOH (see Table 1). Respondents were asked to estimate the percentage from 0% to 100% of their patients that experienced each SDOH (see Table 2). The 15 SDOH provided to respondents were educational limitations/low health literacy, poverty/low financial resources, insufficient/no health insurance, food insecurity, homeless/unstable housing, unstable/unpredictable work schedule, transportation issues, long travel distance from provider, exposure to unsafe environments, immigrant/migrant status, insufficient social support from family/friends, family care demands/issues, perceived stigma around treatment, language barriers, and other SDOH not listed. Clinic zip codes were classified as rural or urban based on the 2010 Rural-Urban Community Area Codes [22]. Small town and rural codes were classified as “rural” and metro- and micropolitan codes were classified as “urban.”
2.3. Analytic Strategy
Survey results were analyzed with descriptive statistics, bivariate correlations, and regression analysis. Descriptive statistics were computed for all variables. Bivariate Pearson correlations were estimated among variables describing the portion of patients that experienced each social determinant. Correlations greater than 0.17 were significant at p < 0.05 and correlations greater than 0.22 were significant at p < 0.01. Given the conceptual overlap and correlations among provider reports on SDOH, principal components analysis (PCA) summarized provider reports on 14 SDOH prior to examination of differences by provider and clinic characteristics (see Appendix A Table A1). Similar approaches to summarizing and subsequently predicting correlated reports are common [23]. One principal component accounting for 43% of the variance in SDOH was extracted and provider and clinic characteristics were regressed on that principal component. Provider job titles were dummy coded prior to analysis with physician or M.D. serving as the referent category. Regression analysis was completed with Mplus v8.6 and data were clustered by zip code using the type = “complex” command [24]. Missing data were handled by full information maximum likelihood. The PCA was conducted with the “prcomp” command using the psych package of R v4.1 [25].
3. Results
Table 1 describes respondents’ professional experience, comfort with the concept of SDOH, and clinic characteristics. Survey responses (N = 161) were recorded from 30 separate ECHO hubs, 123 zip codes, and 138 health clinics across the US. No survey responses were received from healthcare providers in Canada. Respondents indicated their job title as physician or M.D. (37%), social worker (19%), nurse practitioner (15%), or other healthcare provider (30%) and averaged 15 years in practice. Approximately 92% of respondents were at least somewhat comfortable identifying SDOH at the point of care and 66% of respondents agreed that their facility had adequate resources to address SDOH.
Table 2 provides respondent reports on the portion of patients experiencing each SDOH. Respondents cited poverty/low financial resources as the most commonly experienced social determinant for their patients (72.05%) and immigrant/migrant status as the least commonly experienced (19.57%).
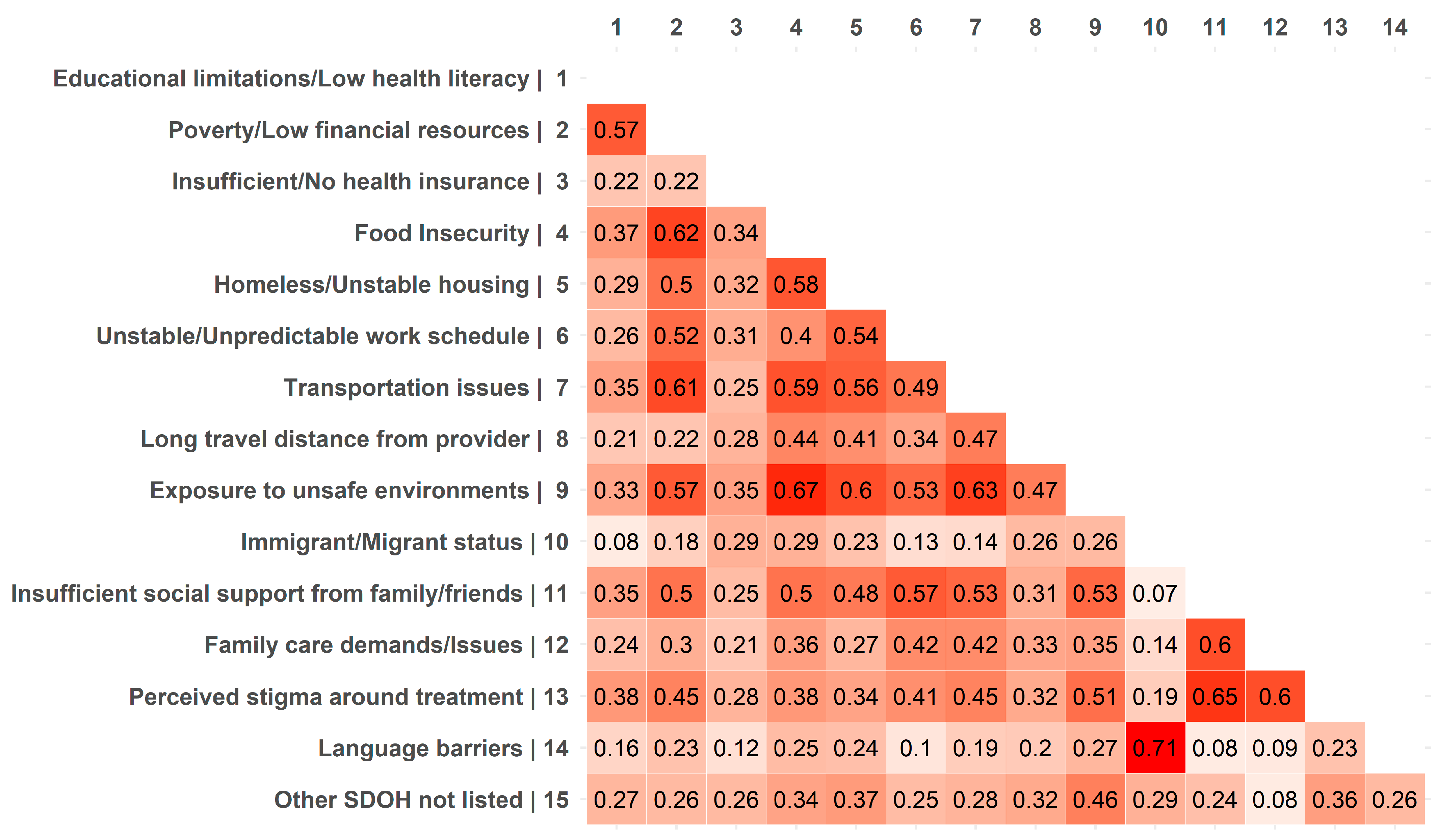
Table 3 provides the results of regression analysis. Results indicated that social workers (Est. = 1.269, p = 0.027), nurse practitioners (Est. = 2.197, p = 0.001), and other healthcare providers (Est. = 2.135, p < 0.001) reported significantly higher SDOH scores compared to physicians. Significant differences in SDOH scores were not observed by years in practice, comfort identifying SDOH, or clinic characteristics. Figure 1 provides a heatmap of bivariate correlations among healthcare provider reports of the most commonly experienced SDOH. Poverty/low financial resources and exposure to unsafe environments were most consistently related to multiple SDOH (seven bivariate correlations of 0.50 or greater). Figure 2 depicts a healthcare provider reports on the percentage of their patients experiencing each SDOH by provider professional background. Physicians tended to report a lower percentage of their patients experiencing each SDOH compared with social workers, nurse practitioners, and other healthcare providers.
4. Discussion
There is a growing consensus that social and economic factors play an important part in maintaining the opioid crisis [8]. Multiple studies have reported that geographic areas experiencing greater economic distress are more acutely affected by the opioid crisis [6]. While research on barriers to opioid treatment has largely focused on regulatory issues, lack of provider MOUD training, or urban/rural divides in access to MOUD [15,16,26], few studies have sought to understand healthcare provider reports on social and economic barriers to opioid treatment [19]. A deeper understanding of social and economic barriers to treatment can inform strategies to help prevent increasing overdose and death.
Providers participating in opioid ECHO programs identified poverty as the most widespread barrier faced by their patients. Providers also rated lack of education, treatment stigma, insufficient social support, transportation issues, family care demands, and unstable work schedules as present for the majority of patients. On average, providers reporting a higher percentage of patients experiencing poverty or exposure to unsafe environments more consistently reported a higher percentage of patients experiencing multiple other social and economic factors (see Figure 1). These descriptive results suggest that multiple social and economic factors are a prominent feature of patient populations seeking opioid treatment. Further investigations on the scope of social and economic barriers experienced by patient populations using state or nationally representative samples are needed [8].
Healthcare provider professional background was significantly associated with their reports on patient experiences with SDOH. Physicians reported significantly lower portions of patients experiencing SDOH compared with social workers, nurse practitioners, and other healthcare providers even after accounting for provider and clinic characteristics. Multiple scenarios might account for these observed differences. First, physicians may be afforded less patient contact time to collect detailed social and economic histories compared to social workers, nurse practitioners, and other healthcare providers. As a result, physicians may simply possess less social and economic information about their patient populations. Second, it is likely that lower resource patients are more often referred to social workers for additional services increasing social workers’ contact with patients experiencing social and economic barriers to treatment. Third, physicians in this study may, in fact, be treating a higher resource population experiencing lower levels of negative SDOH. Finally, results may suggest that professional training may play a uniquely important role in identifying SDOH at the point of care (see Figure 2). Further research is needed to disentangle differences in reports of SDOH by professional background during provider training as well as at the point of care.
The SDOH framework [9] offers one approach to organizing information on social and economic factors relevant for healthcare providers. Provider reports on the SDOH faced by their patients may suggest entry points for improving opioid treatment. Recent commentaries have posited similar sentiments by calling for providers to conduct more detailed social and economic histories of their patients and through proposing the development of multi-faceted instruments to assess SDOH at the point of care [27,28]. Additionally, multiple recent reviews and commentaries have called for medical educators to incorporate increased content on SDOH into standard educational curriculum [29,30]. The results of the current study suggest that increased provider education along with multi-disciplinary teams including social workers, nurse practitioners, and other healthcare providers may also play an important role in gathering social and economic histories of patients.
Provider reports, however, are only one data point that should be considered in tandem with other sources of information. Patient reports on barriers to treatment along with local area measures of social and economic factors can each provide important data on the social and economic contexts in which treatment is taking place. Additionally, pairing these multiple sources of information with treatment outcome data can allow health care systems and communities to empirically assess which social and economic factors create the most pressing barriers to opioid treatment. Future research should seek to triangulate multiple sources of data on social and economic factors to improve our understanding of barriers to successful treatment. This information has the potential to help optimize community-level interventions to combat the opioid crisis [11]. Additionally, specific to ECHO programs, our findings indicate the importance of including SDOH data in harmonized frameworks that assess the impact of ECHO trainings in addition to provider, patient, and intervention information [31].
While the current study provides an important step in examining provider reports on social and economic factors in opioid treatment, some limitations should be noted. First, it is likely that some health care providers did not have full information on the social and economic situations of their patient panels. While health care provider reports are likely to be incomplete, their perceptions are likely to influence treatment approaches. As such, these reports remain an important component of patient care. Second, the study sample is limited to healthcare providers who signed up to participate in opioid ECHO programs. Given the goal of the ECHO project to connect providers in under-resourced communities with specialized treatment knowledge, it is possible that the patient populations referenced in this study are experiencing a greater depth and breadth of social and economic barriers as compared to other patient populations. As such, the results presented here should not be generalized beyond providers participating in ECHO programs. Third, no information was collected on those indicating their professional role as “other healthcare provider” and, therefore, this category may encompass a range of professional backgrounds. Fourth, it is likely that some patients both in need of opioid treatment and experiencing high levels of social and economic barriers to treatment fail to ever visit a professional healthcare provider. As such, some patients in extreme social and economic distress are not represented by in the reports of healthcare providers on SDOH. Finally, provider reports on the role of racial/ethnic discrimination were not assessed and future studies should incorporate these measures.
5. Conclusions
The results of the current study mirror recent reports that suggest multiple social and economic factors play an important role in the opioid crisis [7,8]. It is also essential to recognize that a complex and dynamic web of supply and demand factors has propelled multiple waves of the opioid epidemic [3]. At the local level, however, different factors may be more prominently related to opioid misuse [11]. Information on social and economic factors operating locally is important for community-level practitioners seeking to prevent opioid misuse in their communities. Recent reports from the state of Ohio have highlighted the importance of coordinated programmatic responses among local agencies to treat and prevent opioid misuse, reorganized funding streams to support both one-on-one treatment and community-level prevention, and detailed assessments of community-level social and economic factors related to opioid misuse [11]. While social and economic factors have become deeply intertwined with multiple facets of the opioid epidemic [8], combatting social inequalities is generally a slow process and few successes have been noted at the clinic level [32]. Coordinated federal, state, and local strategies aimed at reducing social and economic barriers specific to opioid treatment are likely necessary to help undercut demand for opioids, limit opioid overdose, and reduce death from overdose [7,8,11].
Author Contributions
C.C.: Conceptualization, Methodology, Formal analysis, Data curation, Writing—Original Draft, Visualization. R.G.: Conceptualization, Writing—Reviewing and Editing. J.C.F.: Conceptualization, Writing—Reviewing and Editing, Funding acquisition. All authors have read and agreed to the published version of the manuscript.
Funding
Research reported here was supported in full or in part by the National Center for Advancing Translational Sciences of the National Institutes of Health under Award Numbers UL1TR002538 [CCTS] and UL1TR002538-03S1 [ECHO].
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board at the University of Utah (protocol 00130779, approved 19 February 2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data are available upon request from the first author.
Acknowledgments
The authors would like to recognize the ECHO Institute at the University of New Mexico for their support of this project and for connecting the authors to ECHO hubs across the United States and Canada. The authors would also like to thank Yiliang Zhu, Jessica Reno, Laura Tomedi, Jinyang Liu, Gaelyn Archer, Mikiko Takeda, PharmD, Joanna Katzman at the University of New Mexico; Alicia S. Ventura, Samantha Blakemore, Matthew Heerema at Boston Medical Center; Sherri Green, Marisa Domino at the University of North Carolina, and Julie Donohue at the University of Pittsburgh.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A

{kind=link}
{kind=link}
Table A1.
Results of principal components analysis for the portion of patients experiencing social determinants of health.
Table A1.
Results of principal components analysis for the portion of patients experiencing social determinants of health.
| Variables | Loadings |
|---|---|
| Exposure to unsafe environments | 0.977 |
| Transportation issues | 0.959 |
| Poverty/Low financial resources | 0.943 |
| Food Insecurity | 0.943 |
| Insufficient social support from family/friends | 0.933 |
| Homeless/Unstable housing | 0.899 |
| Perceived stigma around treatment | 0.874 |
| Unstable/Unpredictable work schedule | 0.841 |
| Family care demands/Issues | 0.763 |
| Long travel distance from provider | 0.703 |
| Educational limitations/Low health literacy | 0.696 |
| Insufficient/No health insurance | 0.541 |
| Language barriers | 0.421 |
| Immigrant/Migrant status | 0.417 |
| Eigenvalue | 9.008 |
| Variance Explained | 43% |
References
- Hedegaard, H.; Miniño, A.M.; Warner, M. Drug Overdose Deaths in the United States, 1999–2019. NCHS Data Brief 2020, 394, 1–8. [Google Scholar]
- Woolf, S.H.; Schoomaker, H. Life expectancy and mortality rates in the United States, 1959-2017. Jama 2019, 322, 1996–2016. [Google Scholar] [CrossRef] [PubMed]
- Ciccarone, D. The triple wave epidemic: Supply and demand drivers of the US opioid overdose crisis. Int. J. Drug Policy 2019, 71, 183. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Provisional Drug Overdose Death Counts. National Center for Health Statistics. 2020. Available online: http://www.cdc.gov/nchs/nvss/vsrr/drug-overdose-data.htm (accessed on 1 December 2022).
- Pear, V.A.; Ponicki, W.R.; Gaidus, A.; Keyes, K.M.; Martins, S.S.; Fink, D.S.; Rivera-Aguirre, A.; Gruenewald, P.J.; Cerdá, M. Urban-rural variation in the socioeconomic determinants of opioid overdose. Drug Alcohol Depend. 2019, 195, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Cerdá, M.; Krawczyk, N.; Hamilton, L.; Rudolph, K.E.; Friedman, S.R.; Keyes, K.M. A critical review of the social and behavioral contributions to the overdose epidemic. Annu. Rev. Public Health 2021, 42, 95–114. [Google Scholar] [CrossRef] [PubMed]
- Saloner, B.; McGinty, E.E.; Beletsky, L.; Bluthenthal, R.; Beyrer, C.; Botticelli, M.; Sherman, S.G. A public health strategy for the opioid crisis. Public Health Rep. 2018, 133, 24S–34S. [Google Scholar] [CrossRef]
- Dasgupta, N.; Beletsky, L.; Ciccarone, D. Opioid crisis: No easy fix to its social and economic determinants. Am. J. Public Health 2018, 108, 182–186. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Social Determinants of Health; WHO Regional Office for South-East Asia: New Delhi, India, 2008. [Google Scholar]
- Braveman, P.; Gottlieb, L. The social determinants of health: It’s time to consider the causes of the causes. Public Health Rep. 2014, 129, 19–31. [Google Scholar] [CrossRef] [PubMed]
- Cantu, R.; Fields-Johnson, D.; Savannah, S. Applying a social determinants of health approach to the opioid epidemic. Health Promot. Pract. 2020, 24, 1524839920943207. [Google Scholar] [CrossRef]
- Case, A.; Deaton, A. Mortality and morbidity in the 21st century. Brook. Pap. Econ. Act. 2017, 2017, 397. [Google Scholar] [CrossRef]
- Chetty, R.; Hendren, N.; Kline, P.; Saez, E. Where is the land of opportunity? The geography of intergenerational mobility in the United States. Q. J. Econ. 2014, 129, 1553–1623. [Google Scholar] [CrossRef]
- Schifanella, R.; Vedove, D.D.; Salomone, A.; Bajardi, P.; Paolotti, D. Spatial heterogeneity and socioeconomic determinants of opioid prescribing in England between 2015 and 2018. BMC Med. 2020, 18, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Showers, B.; Dicken, D.; Smith, J.S.; Hemlepp, A. Medication for opioid use disorder in rural America: A review of the literature. J. Rural. Ment. Health 2021, 45, 184. [Google Scholar] [CrossRef]
- Lister, J.J.; Weaver, A.; Ellis, J.D.; Himle, J.A.; Ledgerwood, D.M. A systematic review of rural-specific barriers to medication treatment for opioid use disorder in the United States. Am. J. Drug Alcohol Abus. 2020, 46, 273–288. [Google Scholar] [CrossRef]
- Weimer, M.B.; Wakeman, S.E.; Saitz, R. Removing one barrier to opioid use disorder treatment: Is it enough? JAMA 2021, 325, 1147–1148. [Google Scholar] [CrossRef]
- Arora, S.; Kalishman, S.G.; Thornton, K.A.; Komaromy, M.S.; Katzman, J.G.; Struminger, B.B.; Rayburn, W.F. Project ECHO: A telementoring network model for continuing professional development. J. Contin. Educ. Health Prof. 2017, 37, 239–244. [Google Scholar] [CrossRef]
- Cioe, K.; Biondi, B.E.; Easly, R.; Simard, A.; Zheng, X.; Springer, S.A. A systematic review of patients’ and providers’ perspectives of medications for treatment of opioid use disorder. J. Subst. Abus. Treat. 2020, 119, 108146. [Google Scholar] [CrossRef]
- Hall, N.Y.; Le, L.; Majmudar, I.; Mihalopoulos, C. Barriers to accessing opioid substitution treatment for Opioid Use Disorder: A systematic review from the client perspective. Drug Alcohol Depend. 2021, 221, 108651. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef]
- Economic Research Service. Rural-Urban Commuting Area Codes. Available online: https://www.ers.usda.gov/data-products/rural-urban-commuting-area-codes.aspx (accessed on 1 February 2022).
- Högberg, T.; Magnusson, A.; Lützén, K.; Ewalds-Kvist, B. Swedish attitudes towards persons with mental illness. Nord. J. Psychiatry 2012, 66, 86–96. [Google Scholar] [CrossRef]
- Muthén, B.; Muthén, L. Mplus; Chapman and Hall/CRC: Boca Raton, FL, USA, 2017. [Google Scholar]
- Revelle, W. How to: Use the Psych Package for Factor Analysis and Data Reduction; Department of Psychology, Northwestern University: Evanston, IL, USA, 2016. [Google Scholar]
- Olsen, Y.; Fitzgerald, R.M.; Wakeman, S.E. Overcoming barriers to treatment of opioid use disorder. JAMA 2021, 325, 1149–1150. [Google Scholar] [CrossRef] [PubMed]
- Chaudry, E. Physician assessment of social determinants of health: A necessary component in improving care of patients. Univ. Ott. J. Med. 2021, 11. [Google Scholar] [CrossRef]
- Figueroa, J.F.; Frakt, A.B.; Jha, A.K. Addressing social determinants of health: Time for a polysocial risk score. Jama 2020, 323, 1553–1554. [Google Scholar] [CrossRef] [PubMed]
- Doobay-Persaud, A.; Adler, M.D.; Bartell, T.R.; Sheneman, N.E.; Martinez, M.D.; Mangold, K.A.; Smith, P.; Sheehan, K.M. Teaching the social determinants of health in undergraduate medical education: A scoping review. J. Gen. Intern. Med. 2019, 34, 720–730. [Google Scholar] [CrossRef] [PubMed]
- Siegel, J.; Coleman, D.L.; James, T. Integrating social determinants of health into graduate medical education: A call for action. Acad. Med. 2018, 93, 159–162. [Google Scholar] [CrossRef] [PubMed]
- Tran, L.-T.; Gouripeddi, R.; Facelli, J. A harmonized framework to evaluate impacts of ECHO pain and opioid training on patients and clinicians. In Proceedings of the American Medical Informatics Association Annual Symposium, Chicago, IL, USA, 14–17 November 2020. [Google Scholar]
- Currie, J.; Schwandt, H. The opioid epidemic was not caused by economic distress but by factors that could be more rapidly addressed. ANNALS Am. Acad. Political Soc. Sci. 2021, 695, 276–291. [Google Scholar] [CrossRef]
Figure 1.
Heatmap of bivariate correlations for healthcare provider reports on portion of their patients experiencing each SDOH. Darker colors indicate stronger correlations.
Figure 1.
Heatmap of bivariate correlations for healthcare provider reports on portion of their patients experiencing each SDOH. Darker colors indicate stronger correlations.

Figure 2.
Reports on portion of their patients experiencing each SDOH by provider background.

Table 1.
Healthcare provider and clinic characteristics.
| Variables | N | M/% | SD | Min | Max |
|---|---|---|---|---|---|
| Provider characteristics | |||||
| Professional background | |||||
| Physician or M.D. | 59 | 36.65% | - | - | - |
| Social Worker | 31 | 19.25% | - | - | - |
| Nurse Practitioner | 23 | 14.29% | - | - | - |
| Other Healthcare Provider | 48 | 29.81% | - | - | - |
| Years in practice | 159 | 14.99 | 12.30 | 0 | 51 |
| Comfort identifying SDOH at point of care | |||||
| Not comfortable | 13 | 8.13% | - | - | - |
| Somewhat comfortable | 59 | 36.88% | - | - | - |
| Very comfortable | 58 | 36.25% | - | - | - |
| Extremely comfortable | 30 | 18.75% | - | - | - |
| Attended an opioid ECHO program | 161 | 88.00% | - | 0 | 1 |
| Presented at an opioid ECHO program | 161 | 48.00% | - | 0 | 1 |
| Number of cases presented | 133 | 2.86 | 13.28 | 0 | 150 |
| Clinic characteristics | |||||
| Facility has adequate resources to address SDOH | |||||
| Strongly disagree | 4 | 2.50% | - | - | - |
| Disagree | 33 | 20.63% | - | - | - |
| Agree | 72 | 45.00% | - | - | - |
| Strongly agree | 35 | 21.88% | - | - | - |
| Unknown | 16 | 10.00% | - | - | - |
| Zip codes classified as rural | 143 | 9.10% | - | 0 | 1 |
Notes. N = 161; M = Mean; SD = standard deviation; Min = minimum; Max = maximum; Responses were recorded from 30 separate ECHO hubs, 123 zip codes, and 138 health clinics across the US.
Table 2.
Healthcare provider reports on the portion of their patients experiencing social determinants of health (SDOH).
Table 2.
Healthcare provider reports on the portion of their patients experiencing social determinants of health (SDOH).
| Variables | N | M | SD | Min | Max |
|---|---|---|---|---|---|
| Educational limitations/Low health literacy | 145 | 61.05 | 22.70 | 5 | 98 |
| Poverty/Low financial resources | 147 | 72.05 | 22.30 | 0 | 100 |
| Insufficient/No health insurance | 145 | 34.74 | 25.97 | 0 | 100 |
| Food Insecurity | 142 | 46.54 | 25.37 | 0 | 100 |
| Homeless/Unstable housing | 143 | 39.25 | 27.45 | 0 | 100 |
| Unstable/Unpredictable work schedule | 145 | 52.20 | 24.50 | 0 | 97 |
| Transportation issues | 142 | 55.14 | 22.59 | 0 | 97 |
| Long travel distance from provider | 142 | 37.94 | 24.23 | 0 | 90 |
| Exposure to unsafe environments | 140 | 48.86 | 27.50 | 1 | 100 |
| Immigrant/Migrant status | 145 | 19.57 | 19.02 | 0 | 79 |
| Insufficient social support from family/friends | 143 | 57.00 | 21.03 | 0 | 100 |
| Family care demands/Issues | 142 | 55.01 | 21.91 | 0 | 100 |
| Perceived stigma around treatment | 143 | 58.86 | 27.86 | 0 | 100 |
| Language barriers | 144 | 22.23 | 22.56 | 0 | 95 |
| Other SDOH not listed | 116 | 37.37 | 26.72 | 0 | 92 |
Notes. N = 161; M = Mean; SD = standard deviation; Min = minimum; Max = maximum.
Table 3.
Results of linear regression examining differences in healthcare provider reports on the portion of patients experiencing social determinants of health (SDOH).
Table 3.
Results of linear regression examining differences in healthcare provider reports on the portion of patients experiencing social determinants of health (SDOH).
| Variables | SDOH Principal Component Scores | |||
|---|---|---|---|---|
| Est | SE | Std. | p | |
| Provider characteristics | ||||
| Professional background | ||||
| Social worker a | 1.269 | 0.574 | 0.204 | 0.027 |
| Nurse practitioner a | 2.197 | 0.681 | 0.314 | 0.001 |
| Other healthcare provider a | 2.135 | 0.461 | 0.399 | <0.001 |
| Years in practice | −0.179 | 0.237 | −0.073 | 0.450 |
| Comfort identifying SDOH | 0.306 | 0.241 | 0.109 | 0.205 |
| Clinic Characteristics | ||||
| Resources for SDOH | −0.423 | 0.303 | −0.132 | 0.162 |
| Located in a rural zip code | −0.079 | 0.747 | −0.009 | 0.916 |
| Intercept | −0.741 | 1.023 | - | 0.469 |
| R2 | 0.181 | 0.063 | - | 0.004 |
Notes. N = 161; Est = unstandardized estimate; SE = standard error; Std. = standardized estimate; p = p-value; SEs clustered by zip code; a = referent is Physician or M.D.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Cambron, C.; Gouripeddi, R.; Facelli, J.C. Healthcare Provider Reports on Social Determinants of Health in Opioid Treatment. Psych 2023, 5, 60-69. https://0-doi-org.brum.beds.ac.uk/10.3390/psych5010007
AMA Style
Cambron C, Gouripeddi R, Facelli JC. Healthcare Provider Reports on Social Determinants of Health in Opioid Treatment. Psych. 2023; 5(1):60-69. https://0-doi-org.brum.beds.ac.uk/10.3390/psych5010007
Chicago/Turabian StyleCambron, Christopher, Ramkiran Gouripeddi, and Julio C. Facelli. 2023. "Healthcare Provider Reports on Social Determinants of Health in Opioid Treatment" Psych 5, no. 1: 60-69. https://0-doi-org.brum.beds.ac.uk/10.3390/psych5010007