1. Introduction
For many patients, lower limb loss limits mobility and creates a reduction in their quality of life [
1]. Statistics show an increase in lower limb amputations in Germany between 2005 and 2015 [
2]. This increase is attributable to increasing case numbers of foot-/toe amputations. In contrast to this, a decrease in major amputations and amputations above the toe is notable [
3,
4]. In 2015, 9644 transfemoral amputations were carried out in Germany [
5]. This corresponds to 17.3% of all lower limb amputations. Thus, it is the second most common amputation level.
Patients with lower limb loss are treated with an individual prosthesis to restore their independent mobility and to enable them to achieve a higher quality of life [
1]. Ensuring optimal treatment after amputation is an international challenge also with regard to quality management. Therefore, the World Health Organization (WHO) [
6,
7] and the International Society of Prosthetics and Orthotics (ISPO) [
8,
9] have defined standards and best practice guidelines to regulate the prosthesis treatment process [
10]. A consensus group including medical, physiological, psychological, prosthetic, as well as engineering experts produced these guidelines [
8,
9]. German standards in prosthetic treatment after amputation are in accordance with these international guidelines. Thus, several national [
11] and international literature [
12,
13,
14] recommend a treatment process involving a rehabilitation team. This team should include the attending physicians, nurses, occupational therapists, physiotherapists, and orthopedic technicians.
The treatment process contains three major phases (
Figure 1) after amputation: (I) clinical care involving wound healing processes; (II) the treatment of the patient with an interim prosthesis; (III) and finally the treatment of the patient with a definitive prosthesis. A short description of each phase with regard to the German context follows [
12,
15].
The clinical care phase in Germany (
Figure 1, I) lasts about two to four weeks [
11]. It follows the amputation and pursues wound healing as well as stump conditioning. Andrews et al. [
8] state that wound healing takes about six to eight weeks after amputation. An orthopedic technician oversees this process through immobilizing the residual limb and applying compression loads. Therefore, varying strategies can be recognized [
8]. Besides the support of wound healing, the physiological and psychological health of the patient can be provided as well [
13]. If the residual limb is loadable, the interim treatment (
Figure 1, II) can be started. Webster et al. [
12] advise that the fitting of the interim prosthesis should begin as soon as possible. Therefore, the particular circumstances following polytraumatic injuries should be taken into account. The interim prosthesis can be used for therapeutic training of the residual limb’s resilience [
9]. Furthermore, it enables an iterative improvement of prosthetic strategies [
12], but is dependent on the indication and eligibility of the residual limb and the care goals as well as the health of the patient. The duration of this phase is usually about three to six months in Germany [
11]. The following definitive treatment (
Figure 1, III) requires stable residual limb conditions. Isaacs-Itua et al. [
13] note the definitive treatment of a patient as being established about one year post amputation, however this is contrary to German standards. Definitive treatment can also take place after clinical care in certain cases. The manufacturing of individual prostheses is done at the beginning of treatment for long-term use by patients.
Prosthesis treatment can influence a patient’s quality of life. A patient’s perception of their quality of life often depends on the success of their rehabilitation, their achieved mobility, and their gait. In the literature, seven predictive factors are discussed: depression, prosthetic mobility, social support, a number of co-morbidities, daily social activity, a number of prosthetic problems, and age [
1]. They show a correlation between the quality of life, the condition of the patient, and the prosthetic fit, respectively [
16,
17]. Despite this, most previous studies regarding prosthesis treatment focus only on patients, considering their quality of life and investigating their requirements as well as goals for the prosthesis [
1], and assessing limitations and problems in the treatment process too. However, further investigations to fuel the development of new technologies also require basic knowledge about the technician’s view. Besides patient requirements, knowledge surrounding orthopedic technicians should be considered.
Due to the different soft tissue percentages, the treatment processes and requirements between transfemoral and transtibial amputation differ. Thus, differences in volume fluctuation impact and management are to be expected in addition to the large influence of patient variability. Despite higher case numbers of transfemoral amputations, most previous studies address transtibial amputations. In this paper, we focus on the treatment process of transfemoral amputations. Therefore, meaningful results are estimated. Despite intensive research, the authors are not aware of comprehensive, holistic studies of the requirements and limits of the treatment process from a technician’s point of view. The purpose of this study is to analyze the prosthetic treatment process in Germany, ranking the requirements of the technicians as regards prosthetic sockets, optimal socket fit, and the treatment process. Special attention is placed on the assessment of:
changes in residual limb’s conditions,
optimal socket fit,
decision-making in the socket manufacturing and possible technical limitations, as well as
indications and consequences of volume fluctuations and limitations in volume management.
Therefore, the research question relates to reported volume fluctuations of the residual limb, socket fitting in the treatment process, and the technician’s requirements regarding optimal sockets. This study points out technical limitations and further technology gaps in orthopedic technology with potential for further research. However, the investigation is related to the German context. This qualitative research is based on an expert survey involving ten orthopedic technicians.
2. Results
The results of the study were collected by an expert survey using semi-structured interviews. The statements of ten orthopedic technicians (interviewees) were analyzed via the Mayring technique. Therefore, no patient data were included. A detailed description of the methodology conducted can be found in the section Materials and Methods (
Section 4).
2.1. Residual Limb Condition for Prosthesis Treatment
The residual limb condition should be suitable for definitive treatment. Aspects mentioned by the experts include healed wounds, painlessness, and a stable volume. Therefore, a stable volume means a constant volume within moderate intraindividual ranges of about few millimeters. According to this, all orthopedic technicians report on volume fluctuations during the definitive phase (
Figure 1, III). Five orthopedic technicians outlined the constant occurrence of volume fluctuations. Seven orthopedic technicians characterized them with a very frequent occurrence. Volume fluctuations are characterized as the swelling and shrinking of the residual limb according to different influences. Six orthopedic technicians described the residual limb volume as being greater in the morning than in the evening because of swelling overnight. Due to the compression load from the prosthesis socket, the swelling goes down within some hours, as six orthopedic technicians confirmed. Furthermore, three experts stated that residual limb volume is greater in the evening without the compression loading of the prosthesis. The volume fluctuations are not equally distributed over the residual limb, as two orthopedic technicians mentioned.
The orthopedic technician’s assessments differ regarding the estimated ranges of volume fluctuations during the definitive phase. Two orthopedic technicians reported on occurring ranges of up to 10 mm within one day. Furthermore, three orthopedic technicians outlined a range of about 10% of the residual limb’s scope. Six orthopedic technicians classified volume fluctuation ranges of around 3% up to 6% from the residual limb’s scope. Therefore, specialized treatment is necessary according to the occurring fluctuation range.
2.2. Factors Influencing Socket Manufacturing
A huge variety of socket techniques are available for the prosthetic treatment of transfemoral amputees. All respondents reported that choosing a suitable technique is dependent on many different influencing factors. There is no generally suitable socket technique that can fulfill the needs of all patients. During treatment, all interviewed orthopedic technicians complete an anamnesis questionnaire to consider patient-relevant influencing factors. This questionnaire depends on the regulations of German health insurance funds but can differ between orthopedic companies. Contents generally include patient data regarding themor occupational and social environment, living situation, and health. Eight out of ten orthopedic technicians highlighted the need for an anamnesis on patient’s psychological health in order to obtain a holistic view of the patient’s situation.
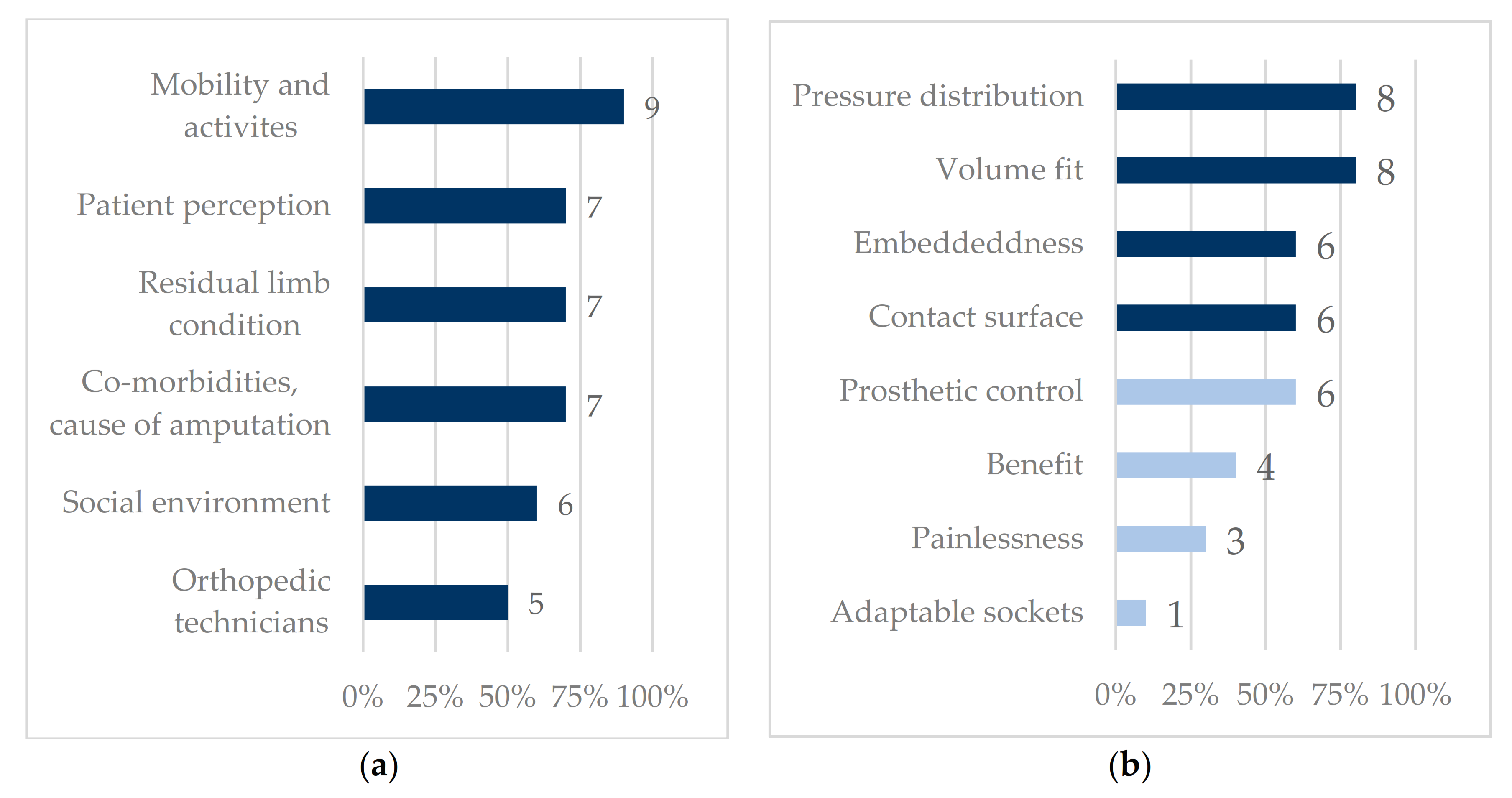
A weighting of individual aspects emerged from the interviews (
Figure 2a). The factors influencing socket manufacturing demonstrate the strong patient-centered focus of the orthopedic technician. Nine orthopedic technicians outline
mobility score and activities as an important aspect. This point considers the patient’s mobility before and after the amputation, as well as the desired mobility of the patient. More than half of the respondents name each of the following aspects as necessary information for choosing socket technique:
patient perception (7 experts state this aspect),
residual limb condition (7),
co-morbidities and cause of amputation (7), and
social environment (6). The orthopedic technicians interviewed emphasized that the
patient perception concerns the individual’s sensation of pain, comfort, and body image as well as experiences from previous socket treatment. The
residual limb condition estimates the proportion of soft tissue, fat tissue, and muscle of the residual limb as well as the osseous situation. It strongly correlates with the
co-morbidities and cause of amputation, as well as
mobility and activities. Less mobility and voluminous residual limbs place lower demands on the contour accuracy of the prosthesis socket in comparison to skeletonized or muscularly residual limbs.
Co-morbidities and the cause of amputation can influence wound healing and pain perception. Therefore, they are important aspects for choosing the proper socket technique. The
social environment addresses the care needs of the patient as well as their housing situation and takes place in the anamnesis questionnaire. According to this, different prosthetic modules are applicable. Another aspect is the
orthopedic technician (5). This aspect considers the specific certifications of an orthopedic technician and the limits on the socket techniques that the orthopedic technician is allowed to utilize.
The orthopedic technician’s requirements for an optimal socket differ: Several different technical (
Figure 2b: dark bars) and functional (
Figure 2b: light bars) requirements are placed on the prosthesis socket in order to optimize the prosthesis fit. A weighting of the requirements was derived from the interviews based on the frequency with which they were mentioned (
Figure 2b). The technical requirements are more often highlighted than the functional ones. Most orthopedic technicians state
pressure distribution (8) and
volume fit (8) as important technical objectives in realizing an ideal socket fit. The pressure distribution should be adapted to the osseous structures and the soft tissue to gain adherence between residual limb and socket. Moreover, the pressure distribution should generate a supportive compression load. Furthermore, the socket should accommodate the residual limb volume, and hence an optimal volume fit is required. More than half of the orthopedic technicians cited
embeddedness (6),
the contact surface (6), and
prosthetic control (6) as important aspects.
Embeddedness specifies the fitting of the prosthesis socket to the distal end of the residual limb. The anatomy of the residual limb requires minimum pressure at the end of the residual limb in order to avoid soft tissue injury to the residual femur. According to a suitable
pressure distribution, a homogenous
contact surface also should be implemented. In connection with the technical requirements, further functional requirements can be derived for the socket.
Prosthetic control is a functional socket requirement. A suitable
prosthetic control depends on the
contact surface and the
volume fit. Fewer orthopedic technicians quote the
benefit (4) for the patient as well as
painlessness (3) as relevant factors. These factors aim to enable the patients to cope with their everyday life. The consensus is that the
benefit strongly depends on the requirements of
painlessness and
prosthetic control, whereas the
painlessness is still related to the
volume fit. In addition, one orthopedic technician requested
adaptable sockets for each patient. Expert CQ said: “All residual limbs react during the day, (...) the volume changes. It is desirable from my point of view for each socket to be adjustable in volume after transfemoral amputation.” (All interviews were conducted in German. The literal translation is given in the text, here is the supplementary original: „Alle Stümpfe reagieren im Laufe des Tages, (…) das Volumen verändert sich. Es ist aus meiner Sincht wünschenswert, wenn jeder Schaft nach transfemoraler Amputation in seinem Volumen verstellbar ist.“ (CQ)). Previously in Germany, only patients with comparatively large volume fluctuations would receive adjustable sockets depending on their mobility, individual requirements, and patient sensation.
2.3. Course of Action for Socket Manufacturing
A consistent course of action for socket manufacturing emerged from the orthopedic technician interviews (
Figure 3) and can be divided into two phases: a planning phase (blue background) and a phase for iterative socket adjustment (grey background). However, the methods differ in sub-steps according to the expert’s experiences and available technical equipment. Therefore, decision-making nodes are included.
All orthopedic technicians mentioned an anamnesis for collecting, capturing, and documenting patient data. Therefore, an
anamnesis questionnaire takes place at the beginning of the process. Information regarding the patient’s physical state of health and possible allergies, mobility, fitness before and after amputation, as well as social aspects are of interest. This information is collected within the framework (see
Figure S1) of the regulations of the
Bundesfachschule für Orthopädietechnik e. V. (BUFA) in Dortmund and serves for the selection of prosthesis modules and techniques. In a second step, eight orthopedic technicians quoted the
measurement of anatomical landmarks (such as circumferences and distances) and the
palpation of prominent points and structures of the residual limb. Three orthopedic technicians outlined that this method is an irreplaceable step within the process. Therefore, expert JG stated, that in his opinion “it is most beneficial to have an experienced orthopedic technician who knows how it should feel.” (“(…) bringt es am meisten einen erfahrenen Orthopädietechniker zu haben, der weiß, wie es sich anfühlen muss.” (JG)).
Socket manufacturing requires a model of the residual limb. Two methods for capturing this shape were mentioned by the orthopedic technicians: the plaster cast method and the 3-D scanning method. The plaster cast method is quoted by ten orthopedic technicians. It is considered to be the conventional method and is more exact than the 3-D scanning method. A special purpose form is shaped either by hand pressure, as practiced by nine orthopedic technicians, or by defined water pressure, as practiced by two orthopedic technicians. Thereby, two orthopedic technicians perform both methods. The hand pressure-method enables the creating of the special purpose form by the manual placement of soft tissues and is dependent on technician’s individual experiences and knowledge. The modeling by water pressure permits a special purpose form under full load and is more objective. A plaster positive can be produced based on the plaster negative. This model allows the manufacturing of a test socket by conventional thermoforming. Eight orthopedic technicians quoted the 3-D scanning method. This digital modeling method allows a volume-correlated geometry acquisition. Three orthopedic technicians reported that due to a lack of space and a reduced patient range of motion, the access of this digital modeling method to a patient’s anatomy has been limited. In addition to this, the scan does not allow the modeling of a special purpose form on the patient themselves. Alternatively, A special purpose form can be modeled by CAD-shaping. Six orthopedic technicians create customized models based on scan data and edit the individual model. Two orthopedic technicians additionally use standardized models of a library for customization and editing. Based on the digitally generated models, a material model of the residual limb can be produced, and a test socket can be manufactured conventionally. As an alternative, a digital socket can be modeled and manufactured by additive manufacturing or milled with a computerized numerical control. Two orthopedic technicians reported limits on the suitability of this 3-D scanning method for sockets with a high requirement for contour accuracy, as is the case with a residual limb with a low soft tissue percentage.
With the help of a transparent thermoplastic test socket, the prosthesis fit is evaluated according to five initial aspects (
Table 1). The most quoted parameter is
patient sensation (10) and the consideration of the
skin surface (9). These give a subjective assessment of the fit and thus evaluate comfort. The
patient sensation is essential and decisive. The patient as the end user ultimately evaluates the fulfillment of their requirements and needs. Whereas the
skin surface is used to visually validate the prosthesis fit by the orthopedic technician. Skin redness, pressure marks, skin folds, and air inclusion between the socket and the residual limb are examined. Six orthopedic technicians mention the
function (gait, adherence). The examination shows piston effects, gait instability, or compensatory movements. Five orthopedic technicians each quote the assessment of the
residual limb volume/geometry and the
properties of tissue and bone. These parameters evaluate the accommodation and embeddedness of the soft tissues and osseous structures in the socket. They examine whether the soft tissue is exiting, or if air is trapped at the distal end. This is done by palpation and a visual assessment. If the
socket fit evaluation is successful, a
socket can be manufactured. Otherwise, the test socket will be edited. By using a thermoplastic material, it can be deformed by heating and thus adapted to the patient.
After finishing the manufacturing process, the prosthesis is given to the patient for permanent use. However, this is not the end of the treatment process. YV explained, “the majority of patients are such that we are always on it. So, we have to put something in, take something out.” ((…) der Großteil der Patienten ist so, dass wir immer dran sind. Also wir müssen etwas einlegen, etwas rausnehmen. (YV)). This implies, that the care process never ends. Instead, it is a constant cycle of adaptation. If the patient recognizes struggles (such as pain, reduced instability, or adherence), the orthopedic technician will evaluate the socket fit again. Nevertheless, if the patient does not notice any complications, the orthopedic technician will evaluate the prosthesis and thus the socket fit at intervals of about six to 12 months.
Orthopedic technicians assess the consequences of an unsuitable fit differently (
Figure 4). Seven consequences can be derived from the expert survey according to an unsuitable socket fit. The most common consequences named are
chronic pain and pathological tissue damage (9), as well as
a loss of sensitivity/guidance and thus mobility (9). Pain and tissue damage (such as pressure ulcers) due to the socket being too large can be caused by friction between the socket and the residual limb, the impingement of the distal femoral end into the soft tissue, or inappropriate pressure loading. The effects of a socket that is too small in size are circulatory disturbance due to an unwanted vacuum at the distal end of the residual limb or unsuitable pressure loading. The majority of the orthopedic technicians also mentioned a
change in body statics (7), in which the gait and the stability of the patient are affected negatively. It also leads to the
loss of sensitivity/guidance and thus mobility. Furthermore, five orthopedic technicians stated that the previously named consequences can lead to the patient’s
rejection of the prosthesis. Pain and an unsuitable gait may result in a loss of confidence and build negative associations. Less mentioned consequences include
post-amputation for pathological damage (2) and an
increase of metabolic consumption (1) following pathological tissue damage and
change in body statics. One orthopedic technician stated that there are
no long-term consequences to be expected (1) because of an unsuitable socket fit.
2.4. Compensation of Volume Fluctuation
Volume fluctuations can lead to an unsuitable fit during the definitive phase (
Figure 1, III) due to water storage in the residual limb. Different factors can influence the intensity and frequency of the fluctuations (
Figure 5). The orthopedic technicians described three main groups of influencing factors:
external incidences,
patient incidences, and
co-morbidities.
Influences from various co-morbidities are described frequently. More than half of the orthopedic technicians named medication (8; such as cortisone, water tablets), metabolic diseases (8; such as according to diabetes, rheumatism, and dialysis), and diseases of the vascular system (6; such as peripheral artery disease (PAD)), as leading to the swelling and shrinking of the residual limb within one day or leading to the changes in weight of the patient. Furthermore, five orthopedic technicians mention cancer in connection with chemotherapy and radiotherapy. Such therapies can favor water storage and weight changes. Thus, they can influence volume fluctuations.
Environmental influences (7) were also considered to be a decisive factor and were quoted by about half of the orthopedic technicians. Seven orthopedic technicians named the weather, in particular great heat, as a strong influencing factor. Furthermore, sweating due to high temperature is mentioned as being a problem for patients. It leads to friction between the residual limb and socket. One orthopedic technician described perforated liners for cooling and assessed them as unsuitable. Furthermore, seven orthopedic technicians also quoted the time of day (7) as an influencing factor. This is according to the assessment of factors influencing the socket technique as well as the changes of residual limb conditions within one day. Few orthopedic technicians assessed that the socket shape/prosthesis fit (4) can influence the volume fluctuation, too. The pressure distribution leads to the compression of the soft tissue and the squeezing out of the lymphatic fluids.
Most orthopedic technicians quoted patient compliance (8) as influencing patient incidences. The influence exerted by the patient compliance relates to the patient’s acceptance of the prosthesis and thus their daily duration of wearing and their mobility. It depends on their perception of the socket fit and their level of physiological health. Therefore, high mobility according to a high acceptance could lead to less volume fluctuation. Five orthopedic technicians mention diet (5). In addition to co-morbidities, diet also can influence the volume fluctuation in a short-term manner by influencing hydrologic balance. Moreover, losing or gaining weight due to changes in diet can also influence the residual limb volume in the long term. Factors that were quoted far less frequently included the residual limb anatomy (3) containing the length of the residual limb and the soft tissue overhang, as well as the hormone balance (1).
Four orthopedic technicians stated that between 2% and 4% of transfemoral amputees require the consideration of special treatment in prosthesis manufacturing. Therefore, several compensation techniques are available. The orthopedic technicians summarized the different technical requirements for these compensation techniques (
Table 2), besides the main requirement
benefit. Thus, most orthopedic technicians mentioned that the compensation technique has to
ensure handling by the patient (8). This includes both motor and cognitive handling. Four orthopedic technicians emphasized the
implementation of the technical requirements in the socket concerning pressure distribution (4). According to this, one orthopedic technician requested the ability of circumferential shape regulation at defined points. Nevertheless, the
dimensions and assembly effort (4) should be kept the same, as four orthopedic technicians mentioned. A small number of orthopedic technicians also quoted that “
form follows function” (3).
Besides the technical requirements, the orthopedic technicians assessed the following available compensation techniques:
editing socket (post-processing),
changing stockings or liners, implementation of a
cable system with panels, and a
pneumatic system. Additionally, all orthopedic technicians were asked to assess a hypothetical
automatic, sensor-controlled compensation technique (
Figure 6).
The most suitable techniques were considered to be the changing of stockings or liners or the implementation of a cable system with panels for regulating the socket volume. Five orthopedic technicians mentioned each of these techniques, however their adaptable scope range limits them. One orthopedic technician assessed a maximum scope range of about 5%. Furthermore, changing stockings or liners relates to the donning/doffing of the prosthesis. This can be uncomfortable in daily life. The implementation of a cable system results in high assembly effort and due to these high costs, however, this technique is preferred for pressure regulation. Less suitable assessed techniques include editing the socket and implementing a pneumatic system. The editing of the socket is a long-term strategy and is not suitable for short-term changes. Thus, four orthopedic technicians classified it as unsuitable for compensating daily volume fluctuations. The idea of a pneumatic system was assessed more positively. Orthopedic technicians rated this technique as unsuitable, as “they can’t build up enough pressure to really make the socket smaller and they lose air” (“die können nicht genug Druck aufbauen, um wirklich dafür zu sorgen, dass der Schaft kleiner wird und sie verlieren Luft” (RS)). Nevertheless, seven orthopedic technicians assessed the hypothetical automatic, sensor-controlled compensation technique as very suitable and necessary in order to compensate for daily volume fluctuations. Possible limits seem to be the suitable technologies for measuring pressure distribution, identifying ulcers, and varying socket scope. Two orthopedic technicians each described the technique as unsuitable or they were undecided, as patients should be able to assess their prosthesis fit and to accommodate their prosthesis by themselves, too.
3. Discussion
Prosthesis treatment is a decision-based process dependent on the professional experiences of an orthopedic technicians as well as their knowledge about the craft [
18,
19]. This expert survey illustrates the individual scope for action in the structured treatment process as well as the individual motives for decision-making due to the perceptions of the patient and the orthopedic technician. The orthopedic technician’s ranking of factors that influence socket manufacturing shows a strong patient-centered focus.
Besides medical and anatomical aspects, psychosocial aspects influence the treatment process. The findings of Godzaydinoglu et al. [
20] outline a correlation between various psychosocial aspects and patient satisfaction with their prosthesis. Thus, both aspects result in their mobility. Compared to the anamnesis questionnaire (see
Figure S1) a high discrepancy is notable due to psychological aspects. These are not yet considered in the anamnesis questionnaire but are required for a holistic treatment [
11]. The standards for prosthetic treatment as published by the WHO [
6], the British Association of Prosthetists and Orthotists (BAPO) [
21], as well as the ISPO [
8] recommend an interdisciplinary rehabilitation team containing psychological therapists. Extending the anamnesis questionnaire’s standards towards more psychological aspects can lead to a more holistic view of a patient’s situation. It may also improve interdisciplinary connections in the rehabilitation team as well as the treatment results. Baars et al. [
22] and Hanspal et al. [
19] demonstrate the dependency of satisfaction due to the prosthesis fit. Therefore, they clarify the importance of both, the anatomical and functional knowledge of the orthopedic technicians and they consider the influence of technician’s subjective experiences. These aspects highlight a high dependence on the individual technical skills and procedural knowledge of the technicians. They do not consider the required experience in empathic interactions with patients as well as the advances of different socket techniques. Results emphasize that empathic interactions are a requirement for the successful treatment of patients. This includes the empathic understanding of patient’s sensation during the fitting evaluation as well as an empathic interaction in determining the aims and goals of the patients as well as their psychological health. The significance of these interactions on patient satisfaction is considered by Day et al. [
23] and is stated in the ISPO report [
8]. In its guidelines, the WHO requires orthopedic technicians to deal empathetically with patients [
7].
The experience of a technician influences the socket technique selected and the requirements set for an optimal socket fit. Greitemann et al. [
11] give a guideline for prosthetic treatment and defined basic requirements due to international standards [
7,
8,
21]. Compared to this, the expert survey underlines the high importance of requirements due to the connection between the socket and the residual limb as regards patient satisfaction. Furthermore, comparing the quotes of the functional requirements with the technical ones it can be noted that functional requirements seem to be considered as less important. This aspect can be attributed to the dependency of the function upon the technical requirements. Mohd et al. [
17] and Safari [
18] show a direct correlation between the connection and painlessness, the prosthetic control, and thus the added benefit for the patients and their satisfaction. Furthermore, the orthopedic technicians do not state requirements due to the outer dimensions and weight of the prosthesis, cosmetics, and duration. The duration is not mentioned, whereby the outer dimensions, the weight of the prosthesis, and the cosmetics are taken into account due to the special requirements of compensation techniques. In addition to Greitemann et al. [
11], Mohd et al. [
17] emphasize duration as an important characteristic of the socket for patient satisfaction. Contrary to this, the expert survey depicts the residual limb as a dynamic structure and the prosthesis treatment as a dynamic process with the need for the continuous editing and adaptation to changes in the residual limb. The findings of Webster et al. [
12] sustain this statement with focus on traumatic amputations. Patients with a traumatic amputation in particular place high demands on the prosthesis and the socket for mobile everyday coping. Their demands vary as regards sport activities as well as the availability of technical innovations. Contrary to the patient’s requirements regarding cosmetic factors [
20], orthopedic technicians estimated cosmetics as less important for patient satisfaction. However, a weighting of requirements is not highlighted in the named international guidelines [
7,
8,
21], but may be necessary in complex situations where trade-offs are necessary. The correct implementation of all requirements can be a technical risk due to conflicting demands in the technical practice. Furthermore, international literature especially from low-income countries [
24,
25] points to the varying requirements of both patients and orthopedic technicians. Therefore, differences in priority rankings are to be expected.
However, the comparison of named international standards to reported technical practices revealed a lack in mentioned methods and techniques. In reference to new supplementary measuring and shape capturing techniques [
26,
27,
28,
29], the expert survey shows a more complex structure in the prosthetic treatment process than both the relevant national and international best practice guidelines [
7,
8,
11,
21]. The new technologies for shape capturing and manufacturing models as well as sockets are mentioned in these guidelines. Despite the possibilities offered by these new technologies, not all technologies are applicable or suitable for every patient. Thus, conventional manual methods are primarily used in the fitting process. Furthermore, recommendations for the decision-making that should determine fitting processes are not yet included in the named guidelines. Contrary to the positive assessment of Schäfer et al. [
30] of optical measurement techniques in Germany, the experts in our study assessed conventional manual methods to be more suitable. Giesberts et al. [
24] determine a socket manufacturing process for low-income countries: the use of a modular socket system (MSS) which eliminates the need for a model and allows the socket to be fitted directly to the residual limb. Therefore, manufacturing duration is limited to one day and thus is advantageous in rural areas. The findings of Suyi et al. [
26] confirm the high skill-dependency of orthopedic technicians in the manual as well as the supplemented treatment process. Nevertheless, technologies that enable the integration of decision-making nodes in the guideline for more patient-specific treatment and can supplement the work of the orthopedic technicians. The expert survey outlines the experience-based nature of the field. According to this, expert IN stated: “(...) if you give me the (system) (...) where I don’t have to palpate the patient anymore and that works, then I’ll take that, but I haven’t found a method yet that can replace that: my feeling when I press on it and the patient can tell me how it feels.” ((…) wenn Sie mir das (System) geben (…), wo ich den Patienten nicht mehr palpieren muss und das klappt, dann nehme ich das, aber ich habe bisher noch keine Methode gefunden, die mir das ersetzen kann: mein Gefühl, wenn ich da drauf drücke und der Patient mir sagen kann, wie fühlt sich das an.“ (IN)). This statement is confirmed by the international consensus [
7,
24] regarding the hands-on nature of the socket manufacturing process.
The parameters for evaluation relate to the requirements of the socket. Literature [
19,
22] places the focus on patient satisfaction. Contrary to this, the findings of the expert survey show—in addition to the patient’s sensation—an expert assessment of the fit by experience-based trackers, such as redness and gait. Based on this experience-based knowledge about the tissues and the gait, possible problem areas can be detected at an early stage. Dillingham et al. [
31] outline the importance of knowledge about tissue, blood circulation, and body statics to prevent tissue damage and pain. Li et al. [
32] mentioned dermatologic problems following load bearing on human skin due to prosthetic interaction. It is well known that shear forces and internal stress can lead to tissue damage as well as an increased risk of pain [
18,
33,
34]. Furthermore, pressure can decrease blood conduction [
35]. Considering biomechanical factors and avoiding internal stress on tissues lead to an increased patient satisfaction. Moreover, reduced costs due to hospitalization periods or requirement of new sockets can be expected for German health insurance funds [
36]. The education and training of orthopedic technicians in Germany follow the Education Standards of the ISPO and should include “the right mix of skills and competencies to meet the needs of people who use assistive devices” [
37]. The results of this survey clarify that the orthopedic technicians provide this knowledge in the treatment process and also express the high demand for suitable measuring techniques for evaluating socket fit. “But what I didn’t manage to do, and I’m dying to know: What is a healthy pressure in the socket?” (“Was mir aber nicht gelungen ist und das würde mich brennend interessieren: Was ist ein gesunder Druck im Schaft?” (CQ)) expert CQ outlined. Furthermore, the expert survey illustrates the desire of the technicians to access more knowledge-based methods especially for self-assessment, quality management, and documentation for German health insurance funds, according to three scientific quality criteria: that method should be objective, valid, and reliable. Contrary to the ability and suitability of the technologies described by Al-Fakih et al. [
38] and Sanders et al. [
39], our experts assessed these available technologies as not suitable for orthopedic practice with reference to handling, freedom of retroactive effects, and painlessness. Further research is needed to identify alternative measurement methods without influencing the residual limb’s tissue to enable the continuous recording of prosthesis fit and volume fluctuation. Due to suitable measurement methods, the quantification of boundary conditions is required. Furthermore, research to quantify suitable loads and to investigate the indication of tissue conditions is necessary.
An unsuitable fit can be caused by volume fluctuations [
39]. Therefore, the interviewed orthopedic technicians mentioned different reasons for volume fluctuations. Volume fluctuations can be influenced by co-morbidities as well as medications and diet. Greitemann et al. [
11] and Sanders et al. [
39] confirm these results. As international literature [
25,
40,
41,
42] points out, most amputations are related to diabetes mellitus or PAD. In conjunction with the outcome of the study as regards influencing factors for volume fluctuations, a high correlation between these co-morbidities and volume fluctuations are to be expected. Asano et al. [
1], Ebrahim et al. [
25], and Moxy et al. [
42] emphasize the importance of patient training and sensibilization for the prevention of progressive amputations and complications. Patient adherence regarding their co-morbidities is a decisive aspect in the prosthetic treatment process as well. Furthermore, there is a high interdependence between volume fluctuations and medications or diet. In addition to literature findings, orthopedic technicians outlined an effect of the prosthesis fit, the compression load, as well as the tissue condition on the volume fluctuations. The outcomes of the expert survey show variations in the assessment of the frequency and the range of volume fluctuations. This indicates a lack of conceptual clarity as well as different experiences of the orthopedic technicians depending on their patient base. The expert survey demonstrates the need for a consistent definition of volume fluctuation for communication, research process, and discourse. This inconsistency is emerging in the literature as well [
39]. Investigations due to short-term volume fluctuations are implemented under different conditions with regard to the period of analysis. Despite this, the findings are similar due the expert’s assessment. The authors report that volume fluctuations of 3% up to 6% can be measured in a short-term manner, ranging from within five minutes up to five hours [
43,
44,
45]. A change of 11% in the residual limb’s scope within one day has also been noted [
43]. The findings of scope ranges differ between investigations for long-term volume changes. A small investigation group limits these studies. Furthermore, no course detection is described. As only a short time period is considered, no evaluation within a day is possible. The specific factors influencing volume fluctuations do not allow for short-term behavior to be transferred without restrictions and a prediction of volume fluctuations is not yet possible. The lack of conceptual clarity, as well as the high inconsistency in periods of analysis, prove the need for the clear differentiation between volume fluctuations and volume changes.
The expert survey illustrated varying consequences of an unsuitable fit. In addition to pain sensation, a loss of sensitivity as well as prosthesis guidance and thus mobility are the most common risks and are reported on in the literature [
18,
46]. Roffman et al. [
47] note that these factors influence low patient satisfaction and thus are predictive for the rejection of the prosthesis. Following this, the compression of the tissues as a decongestant stimulus is missing. The interaction between volume fluctuation due to swelling and compression has already been demonstrated [
39]. However, the influence of weather on swelling has not yet been considered. Ghoseiri et al. [
48] analyzed the influence of weather and temperature on the socket interface and pointed out a direct correlation between temperature in the socket and skin defects. As regards local climate differences, the impact of temperature variations between different countries is to be expected—corresponding holistic studies are not known. However, various approaches to temperature and sweat compensation can be found in the literature [
49,
50,
51,
52,
53]. These are mainly limited to a cooling effect. Further research on the specific interactions between limb swelling and temperature or weather changes is necessary to be able to make predictive statements about limb volume.
Orthopedic technicians explain that the dynamic character of the treatment process and residual limb’s volume fluctuation requires the continuous adjustment of the socket to changes in the residual limb. For this purpose, orthopedic technicians report on varying techniques to adjust the socket fit. This research focuses on solutions that are available in Germany and is therefore limited to manual techniques. The suitability of further international discussed techniques can only be estimated based on these operating principles: compensation with socks/liners was rated positively. However, the requirement of easy handling is in opposition to this, as it is necessary to don/doff the prosthesis. In the literature [
18,
29,
54,
55,
56,
57,
58], a trend towards automatic compensation is emerging. Automatic adjustment is also seen as being beneficial by the orthopedic technicians. This finding is also supported by the investigation of Sanders et al. [
39]. Passive techniques such as pneumatic or cable systems are the basis for further developments and automation. Sanders et al. [
54], as well as Weathersby et al. [
55], describe different systems and rate effectiveness in terms of feasible pressures and geometry changes. This is contradicted by the experts’ requirements for the technologies. The disadvantages of pneumatic systems are also elaborated upon by Sanders et al. [
39] and substantiate the experts’ assessment. Contrary to this, Sanders et al. [
56] describe a hydraulic system that increases the maximum achievable pressures as a new development stage. This method was not mentioned by the orthopedic technicians and cannot yet be evaluated. However, the main disadvantages of the pneumatic system with regards to the high installation effort and the tightness of the chambers can be transferred, which is why a similarly negative assessment is to be expected. Alternatively, an automated cable system is described [
54,
55]. Due to the positive expert assessment of manual technology, a similarly good assessment of the automated one is estimated, and a high application potential is conceivable. Possible negative aspects related to installation effort and additional weight. To reduce the adjustment effort, new adaptable socket techniques are mandatory. Limitations of the existing automated, adaptable sockets include the lack of suitable measuring technologies and knowledge about the quantified, objective boundary conditions (such as pressure and compression loads), the outer dimensions, the weight of the prosthesis, and the cosmetics.
4. Materials and Methods
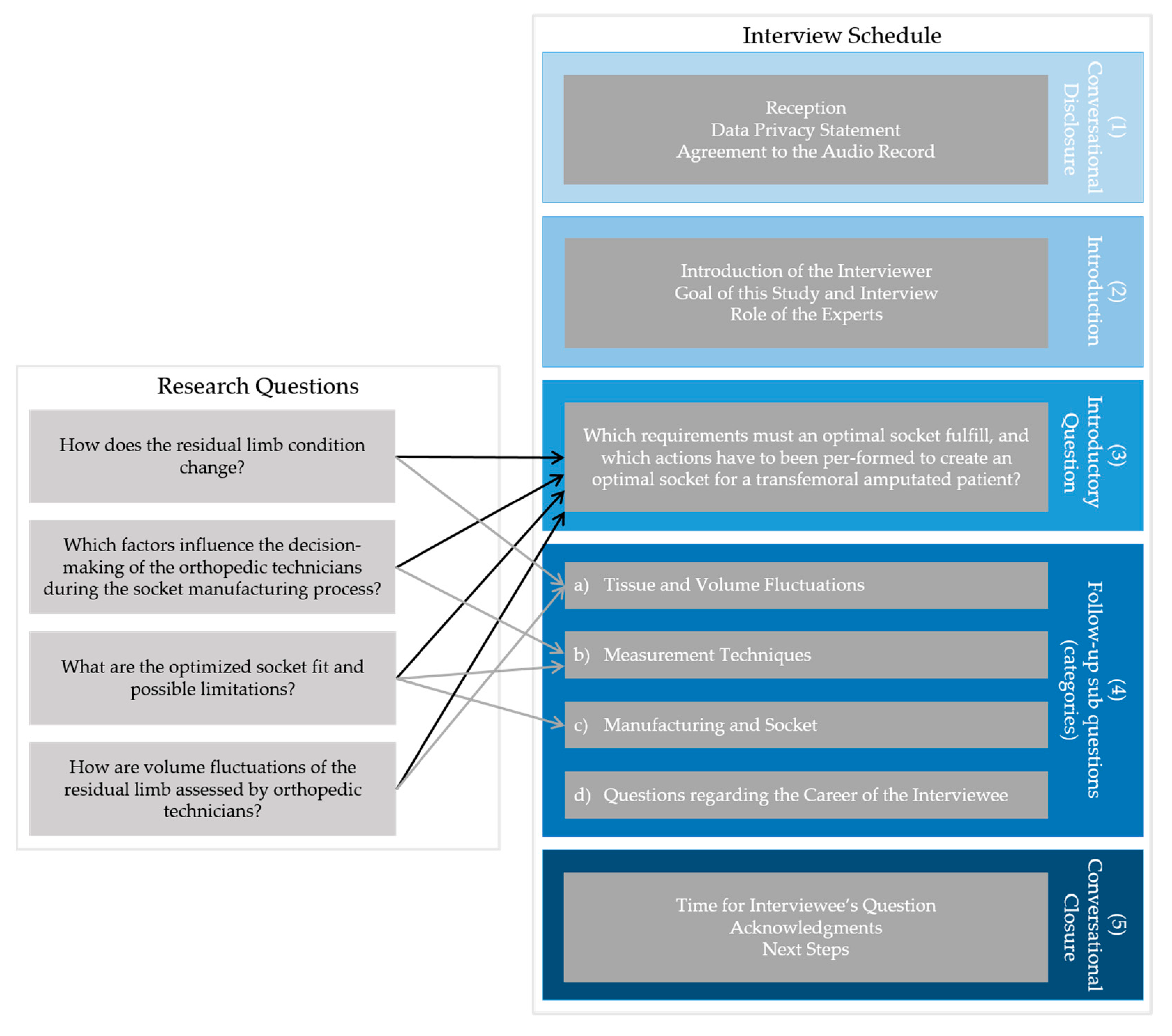
The aim of the research was to clarify the processes of prosthetic socket treatment after transfemoral amputation. Therefore, special focus was placed on the orthopedic technician’s point of view regarding their requirements as well as limitations of the process. The study contains four main research questions (see
Figure 7):
How does the residual limb condition change?
Which factors influence the decision-making of the orthopedic technicians during the socket manufacturing process?
What are the optimized socket fit and possible limitations?
How are volume fluctuations of the residual limb assessed by orthopedic technicians?
As mentioned above, semi-structured interviews in an explorative expert survey [
59,
60,
61] was chosen as a suitable research design. The study focuses on the “expert knowledge” of orthopedic technicians. This knowledge is gained through their work experience, skills as procedural knowledge, and so-called textbook knowledge. To guarantee a high level of expert knowledge, the definition of experts in this study included the certificate “Meister” (master craftsman)—in Germany the highest state-approved professional qualification in crafts—as well as several years working experience (minimum five years). The education and training of all orthopedic technicians in Germany are also in accordance with international standards, and accreditations are awarded [
37]. The principle of the
BUFA, Stefan Bieringer, acted as gatekeeper and recruited potential participants who were interested in taking part in this study.
The required data was collected using the qualitative interview method [
59,
60,
61,
62]. The interviews were designed as individual and semi-structured. “Individual” refers to the fact that the same interviewer always carried out the interviews on a one-on-one basis. “Semi-structured” denotes the research question is translated into an interview guide consisted of the introductory question and a set of prepared follow-up sub questions, sorted in different categories of research themes: with the aim of pushing the interview in the direction of the research question. All interviews ran off the same schedule (see
Figure 7):
Conversational disclosure: reception, data privacy statement, agreement to the audio record;
Introduction: introduction of the interviewer, the goal of this study and interview, and the role of the experts;
Introductory question: the introductory question was asked word-for-word followed by the unrestricted, uninterrupted, open-ended response of the interviewee;
Follow-up sub questions: inquiries by follow-up sub questions were undertaken with regards to the content and direct questions were asked regarding career, as well as,
Conversational closure: time for interviewee questions, acknowledgments, and next steps.
After designing the introductory question as well as the potential follow-up sub questions, the interview schedule itself and the interview guide is pretested once. In addition to the interviewer and the interviewee, a third person participated as a supervisor in this pretest. The interviewee and supervisor gave feedback regarding the interview guide and execution. Only minor adaptations to the interview guide were required. They also reflected upon the behavior of the interviewer, and it was recommended that the interviewer slows down and takes more time during the interview in general.
The final introductory question was decided upon: “Welche Anforderungen werden an einen optimalen Prothesenschaft gestellt und welche Handlungsschritte durchlaufen Sie bis zur Erreichung eines optimalen Prothesenschafts mit einem transfemoral-amputierten Patienten?” (All interviews were in German, translation of the introductory question: Which requirements must an optimal socket fulfill, and which actions do you have to perform to create an optimal socket for a transfemoral amputated patient?). Categories of follow-up sub questions broached the following issues: (a) tissue and volume fluctuations, (b) measurement techniques, (c) manufacturing and socket, as well as direct questions regarding the career of the interviewee. All relevant topics not mentioned in the interviewee response to the introductory question were followed up on.
It was planned that interviews would be undertaken face-to-face. However, due to travel restrictions caused by the pandemic all interviews were organized as a videoconference. The sample contained ten experts. All interviewed experts are “Meister”. The variation within the sample regarding working experience ranged from 7 to 40 years. In light of this, all interviewees fulfilled the requirements of being a considered expert within this study. The interviews took place in August and September 2020.
The shortest interview lasted 34 min and the longest interview 50 min. All interviews were audio recorded by a separate Dictaphone, anonymized, and transcribed by the same transcription rules. A verbatim transcript was decided upon. Spoken language was transcribed word-for-word and any dialect or unclear articulation were translated into standard language. Not transcribed were any filler words, repetition of words back-to-back, or information related to the pitch and tone of the voice as well as nonverbal characteristics. Pause length is not mentioned in the interview transcription, but interruptions, such as those based on a technical issue, are registered. Linguistic obscurities are marked in the transcript.
The interviews were evaluated using the Mayring technique [
63,
64]. During the first step of the evaluation, the interview transcripts were read, all content-bearing text passages were indicated and summarized as well as paraphrased with own words. In the second step, the interview transcripts were read again, and all summarizing paraphrases were generalized. In the third step, all semantically identical paraphrases were cut out, content-bearing paraphrases were adopted, paraphrases with similar statements were assorted, and paraphrases with several statements on the same referent were combined. These generalized and reduced findings were compared with all interview transcripts again with the aim to compile descriptive statistics.
5. Conclusions
Ten orthopedic technicians took part in this expert survey. This sample size is common for a qualitative interview project with an exploratory characteristic and follows the golden rule to “interview as many subjects as necessary to find out what you need to know” [
61]. Normally, the number of interviews depends on the purpose. The purpose of this study was to investigate the perspectives of orthopedic technician on the prosthesis treatment process surrounding any possible limitations in the available technologies. The interviews showed at a certain point a saturation, and further interviews may yield little new information.
The outcome of this research reveals a strong patient-centered focus as well as the use of experience-based decisions in prosthesis treatment. For a holistic comparison of the perspectives of both orthopedic technicians and patients, more explorative expert surveys should be conducted. Therefore, patients should be interviewed as experts. This will allow the establishment of connections between the two groups and also highlight any differences in requirements.
Furthermore, suitable methods may lead to improvements in the self-monitoring, self-adjustment, and quality management of prostheses. Despite this, the orthopedic technician’s desire for supplementary techniques and a trend towards a knowledge base can be outlined, however, there is a discrepancy between available techniques and their possibilities of use in the treatment process. For this purpose, suitable technologies to enable continuous measurements in the everyday lives of patients, as well as for socket adjustment, are necessary. Further investigations that provide objective, valid, and reliable measurement tools with the freedom to implement retroactive effects are required, as well as miniaturized and integratable actuators for socket adjustment with low assembly effort, low weight, and low cognitive effort for patients. Suitable technologies for geometry and temperature compensation are required for holistic adaptation.
In addition to pressures, other physiological parameters are decisive and need to be taken into account in socket adjustment. Further research should therefore look at the fundamental issues regarding the quantification of the tissue properties and determine any corresponding parameters in order to create adaptable material models. It is mandatory to determine the dynamic interaction between the residual limb and the prosthesis socket in order to understand the variability of the interface. Furthermore, new measuring methods should also be investigated as regards adaptive lightweight technologies or adjustable materials.
Prosthesis treatment can be supplemented by further research and development. The research and development possibilities are limited in the orthopedic technician’s trade. Existing technology limitations and gaps illustrate the need for further basic research for knowledge-based orthopedic technology, considering orthopedic technician’s experience.


 ,
, 







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}