
State of the Art: An Update on Adult Burn Resuscitation
by
Jacqueline M. Causbie
1, 
Lauren A. Sattler
1,2,
Anthony P. Basel
1,3,
Garrett W. Britton
1,3,* and
Leopoldo C. Cancio
3 1
School of Medicine, Uniformed Services University of the Health Sciences, Bethesda, MD 20814, USA
2
Brooke Army Medical Center, Fort Sam Houston, TX 78234, USA
3
US Army Institute of Surgical Research, Fort Sam Houston, TX 78234, USA
*
Author to whom correspondence should be addressed.
Eur. Burn J. 2021, 2(3), 152-167; https://0-doi-org.brum.beds.ac.uk/10.3390/ebj2030012
Submission received: 6 July 2021
/
Revised: 3 August 2021
/
Accepted: 5 August 2021
/
Published: 9 September 2021
(This article belongs to the Special Issue Critical Care in Burns)
Abstract
:Treatment of patients with severe burn injuries is complex, relying on attentive fluid resuscitation, successful management of concomitant injuries, prompt wound assessment and closure, early rehabilitation, and compassionate psychosocial care. The goal of fluid resuscitation is to maintain organ perfusion at the lowest possible physiologic cost. This requires careful, hourly titration of the infusion rate to meet individual patient needs, and no more; the risks of over-resuscitation, such as compartment syndromes, are numerous and life-threatening. Recognizing runaway resuscitations and understanding how to employ adjuncts to crystalloid resuscitation are paramount to preventing morbidity and mortality. This article provides an update on fluid resuscitation techniques in burn patients, to include choosing the initial fluid infusion rate, using alternate endpoints of resuscitation, and responding to the difficult resuscitation.
1. Introduction
According to Dr. Basil A. Pruitt, Jr., the goal of fluid resuscitation is to maintain organ perfusion at the lowest possible cost, which relies on careful, hourly titration of the infusion rate to meet individual patient needs, and no more [1]. The risks of over-resuscitation are significant, including compartment syndrome, pulmonary edema, gastrointestinal dysfunction, impaired wound healing, and many more. Recognizing a runaway resuscitation and understanding how to employ adjuncts to crystalloid-based resuscitation are paramount to reducing the morbidity and mortality associated with burn shock. This article provides an overview of current practice in burn shock resuscitation.
2. Overlapping Phases of Care
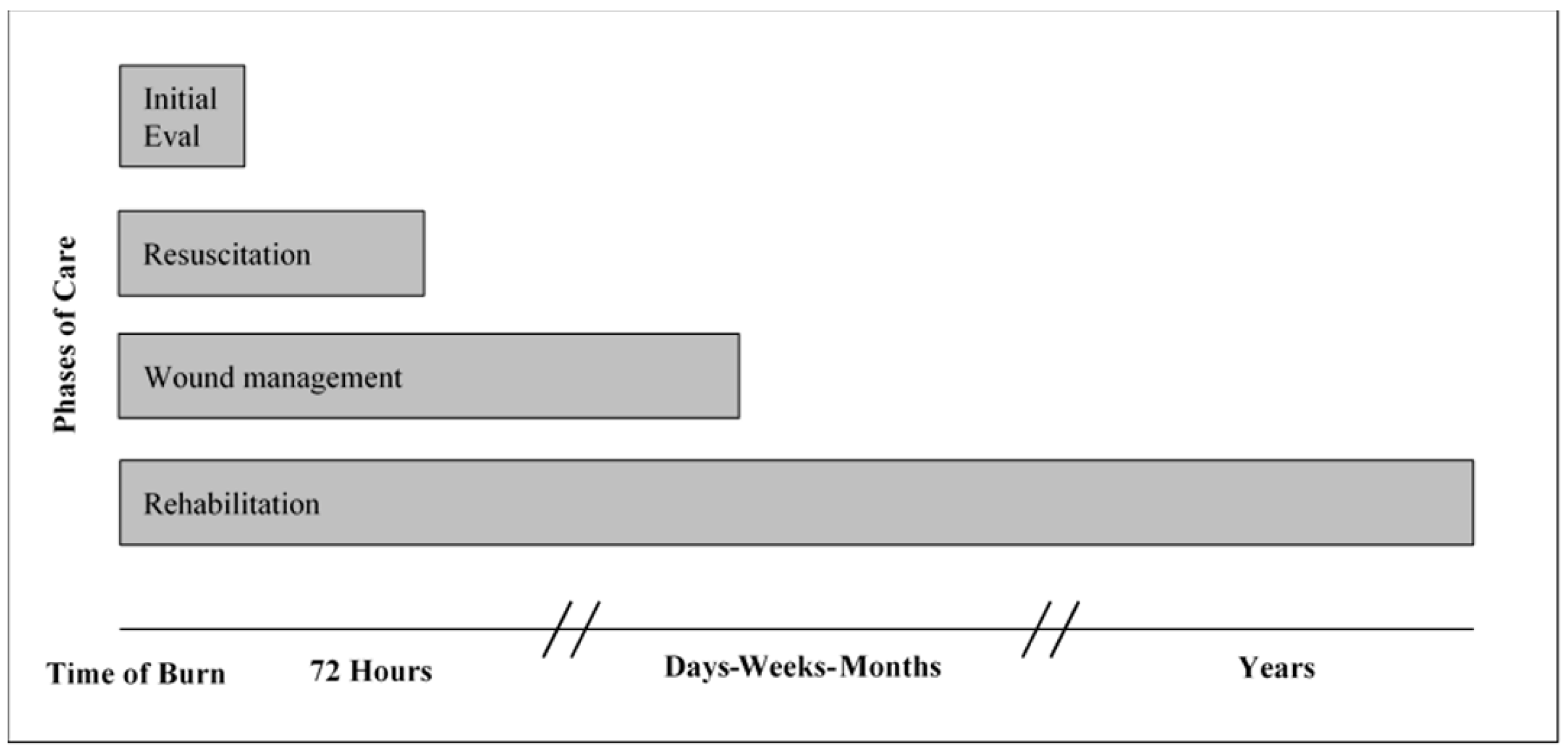
Burn injury represents a complex disease pattern with life-long effects not limited to the cutaneous injuries. The phases of burn care include the initial resuscitation, definitive wound management, and rehabilitation of the physical and psychological injuries. These phases of care should not be approached in a linear fashion; rather, they should be seen as overlapping phases that must all begin within the first postburn day (Figure 1). In other words, although the main effort on days one and two postburn is directed at initial assessment and fluid resuscitation as described in this article, wound care and rehabilitation management must also begin during this period.
3. Pathophysiology of Burn Shock
Burn injuries involving 20% or more of the total body surface area (TBSA), or 10% TBSA in children or the elderly, are likely to result in burn shock. This is a complex phenomenon that features the following major features: (1) increased microvascular permeability, causing the loss of fluid similar to plasma from the intravascular space into the interstitium, resulting in hypovolemic shock; (2) massive release of catecholamines, causing increased systemic vascular resistance; and (3) a variable degree of myocardial dysfunction. Collectively, these three processes contribute to decreased cardiac output and decreased end-organ perfusion. The mainstay of resuscitation is correction of hypovolemic shock by replacement of intravascular volume with intravenous crystalloid solution, augmented when needed by intravenous colloid solution. During the resuscitation period, which takes about 48 h to complete, a patient will pass through three phases with respect to hemodynamics. Successful management depends on understanding this trajectory (Table 1).
A complex interplay of inflammatory mediators steers the body’s transition through these phases in the response to injury. The immediate release of histamine and leukotrienes brings about peripheral vasodilation and contributes to the early drop in cardiac output that occurs even before significant plasma volume is lost. Damage-associated molecular patterns (DAMPs) activate local and systemic inflammatory responses. Release of reactive oxygen species, cytokines, prostaglandins, and other mediators follows. The most rapid period of plasma volume loss occurs in the immediate postburn hours, reflecting a derangement of all of the Starling forces that mediate transvascular fluid flux, to include an increase in microvascular permeability. This occurs both in burned and, in larger burns (>25% TBSA), unburned tissue as well; the latter reflects the systemic effects of inflammatory mediators. It also reflects hypoproteinema, whereby loss of intravascular protein decreases the plasma oncotic pressure, worsening the systemic capillary leak and further promoting the formation of tissue edema. Plasma volume reaches its nadir around hours 12–18 postburn, and then with resuscitation gradually returns to normal at around postburn hour 48. Blood volume reaches a nadir at the same time as plasma volume, but typically does not return to baseline (reflecting red blood cell destruction—see below). Massive release of catecholamines begins during burn shock (and is sustained throughout the hospital stay); in the early postburn period this results in an increase in systemic vascular resistance (SVR). During the latter half of the first postburn day, with activation of inducible nitric oxide synthase (iNOS), peripheral vasodilation overcomes the effect of catecholamines on SVR [2,3,4,5]. Microvascular permeability begins to be repaired, at least in unburned tissue, during the first postburn day. At the end of a successful resuscitation, a patient with major burn injury is typically hyperdynamic, with a supranormal cardiac output, tachycardia in the range of 100–120/min (in adults), and a low SVR.
Studies have demonstrated a phenotype of burn shock involving reduced cardiac performance that is not responsive to fluid resuscitation alone. This burn-mediated myocardial injury is thought to be due to impaired isovolumic relaxation and decreased left ventricular contractility caused by release of potent negative inotropic mediators. The phenomenon was best demonstrated in ex-vivo small-animal models, in which the coronary arteries of the isolated heart are perfused in a retrograde fashion (Langendorff preparation). In otherwise healthy human patients with burns, the effects of circulating catecholamines usually mask any defect in intrinsic myocardial contractility. On the other hand, older or medically unfit burn patients may indeed fail to respond to injury in the expected fashion and may require additional monitoring and inotropic support [6].
Recognition of complex interactions at the endothelial level has led to a revision of the traditional Starling model of transvascular fluid flux. The endothelial glycocalyx (EGL) is a complex composed of proteoglycans and glycoproteins that play a pivotal role in maintaining homeostatic balance between the intravascular and extravascular spaces [7]. Physiologic insults cause degradation of the EGL, but evidence suggests that certain resuscitation fluids, such as plasma, promote EGL integrity and thus better maintain intravascular volume. The EGL is therefore the focus of a number of ongoing studies regarding burn shock and resuscitation [8].
4. Initial Assessment
Upon presentation, burn-injured patients must receive a thorough evaluation. Concomitant mechanical trauma occurs in 5–40% of burn patients, is associated with increased mortality, and should be addressed in a standard fashion while also treating the burn injury [9,10,11,12,13,14]. Incidence of accompanying traumatic injuries is much higher in burn patients with certain mechanisms of injury, such as motor-vehicle collisions, military combat, and jumping from a burning building [11,14,15,16,17].
Endotracheal intubation should be performed for all patients with burns >40% total body surface area (TBSA), regardless of anatomic location, since patients with larger burns are at risk of airway loss secondary to massive edema formation. Although patients with extensive facial burns and those with inhalation injury should be considered for intubation on a case-by-case basis, prophylactic intubation, especially before interfacility ground or air transport, is often prudent. Carbon monoxide and/or cyanide toxicity should be considered (and the carboxyhemoglobin level measured), especially in patients whose presentation or mechanism suggests exposure to smoke [18,19,20,21]. In the absence of carbon monoxide poisoning, efforts should be made to avoid hyperoxygenation [22].
5. Resuscitation Calculations
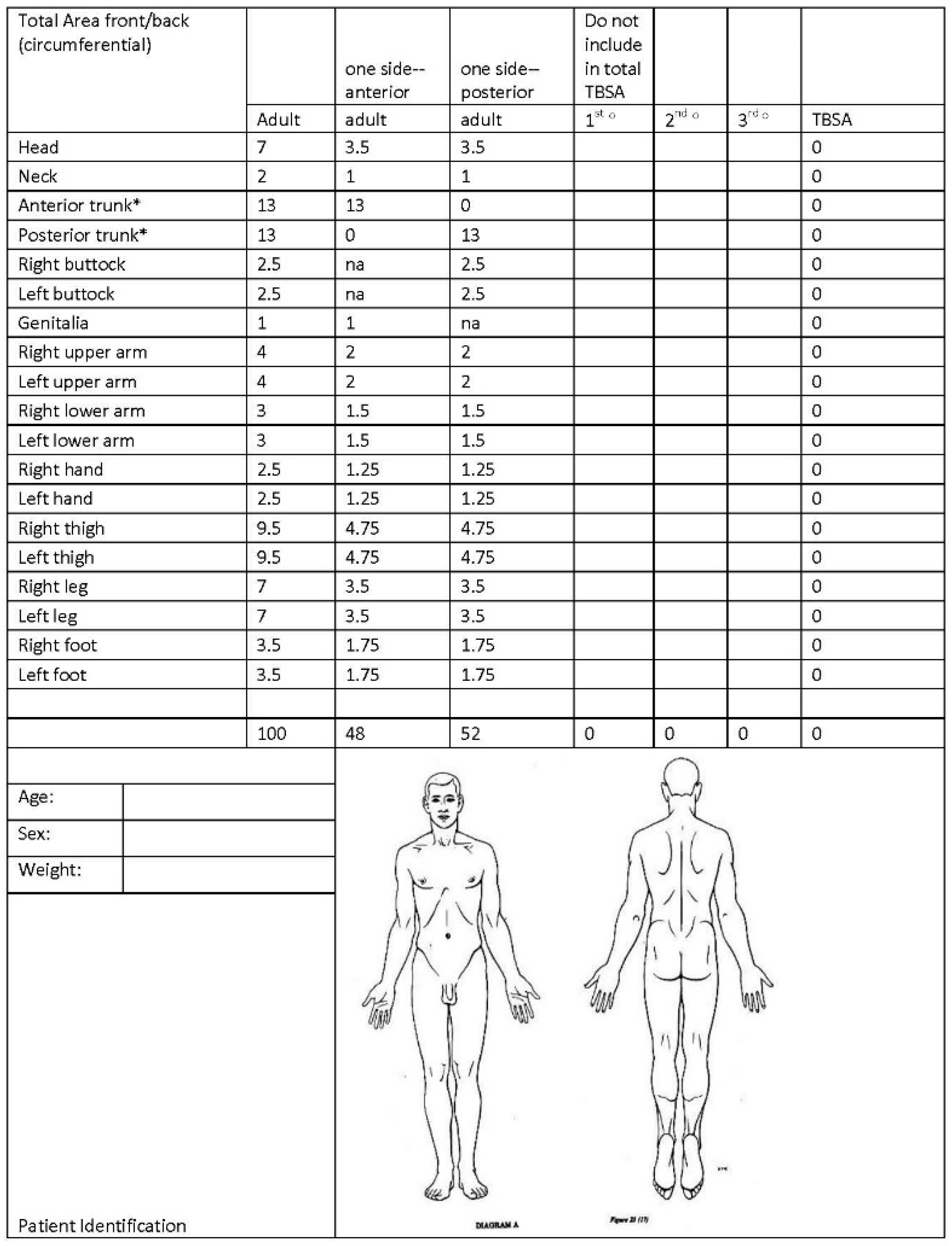
Calculation of the resuscitation fluid rate includes estimating the %TBSA covered by partial- or full-thickness burns utilizing methods such as Lund–Browder charts (Figure 2), the rule of 9 s, and the rule of hands. Accuracy suffers with the rule of 9 s and when burns are scattered or irregularly shaped, and improves when using a modified Lund–Browder chart and when calculations are performed by an experienced practitioner [23,24,25,26]. The development of three-dimensional computer modeling systems provides another strategy for calculating burn size. These programs construct a model based on input variables (height, BMI, gender, etc.) or scans of the actual patient, on which clinicians mark the locations of burns. They have been shown to accurately calculate burn size, but widespread implementation is limited by the need to calculate %TBSA expeditiously, often outside a burn unit, in order to initiate resuscitation [27,28,29].
There are several formulas to predict fluid resuscitation needs; the key is that these are estimates and that the infusion rate must be adjusted hourly based on individual responses. The modified Brooke formula predicts a conservative volume of 2 mL/kg/%TBSA of lactated Ringer’s solution (LR) over the first 24 h, with 50% of the total amount programmed for delivery during the first 8 h. The most frequently used is the Parkland formula, which estimates 4 mL/kg/%TBSA [2,30,31,32,33,34]. The original rationale for the higher dose prescribed by the Parkland formula was the theory that more rapid correction of a patient’s extracellular sodium deficit during shock would result in better outcomes. In 2008, the American Burn Association (ABA) published a “consensus” formula of 2–4 mL/kg/%TBSA based on the modified Brooke and Parkland formulas, respectively [4,31,35,36,37]. In 2019, the ABA included the Rule of 10 for adult burn resuscitation as part of disaster management guidance [38].
The Rule of 10 for adults, developed at the US Army Burn Center, estimates the initial infusion rate (in mL/h of LR) as 10× %TBSA, with an additional 100 mL/h for every 10 kg of body weight above 80 kg (Figure 3). For adult patients between 40 and 130 kg, this reliably produces an initial rate that falls within the Brooke and Parkland recommendations [39,40,41]. Many attempts have been made to improve upon existing equations by incorporating additional variables and calculations with the goal of accurately predicting ongoing fluid needs [42,43,44,45,46]. The Rule of Ten, however, was developed in response to calls for a simplified burn resuscitation formula that emphasizes the importance of precise titration over complex equations, minimizes recall and calculation errors, and is rapidly implemented during an emergency without delaying care [4,32,47,48,49].
6. Endpoints of Resuscitation
The treatment of burn shock requires the judicious infusion of crystalloid and colloid solutions in order to replace ongoing plasma volume losses and to defend against hypovolemic shock. Although the initial rate of fluid infusion is calculated based on burn size and patient weight as described above, the rate must subsequently be adjusted, often hourly, based on physiologic response. The primary indicator of the adequacy of resuscitation is the urine output (UOP), but other variables, including the heart rate, blood pressure, lactate, base deficit, and mental status, must be considered simultaneously [50].
The UOP goal is 30–50 mL/h in adults or 0.5–1 mL/kg/h, recognizing that the latter target may be excessive for many adults [30,34,35,51]. On the other hand, patients with gross pigmenturia, i.e., myoglobinuria or hemoglobinuria, require a higher UOP target—typically 70–100 mL/h. Complementary methods of monitoring hemodynamic status and perfusion should be considered for all patients, particularly those with comorbidities including renal, hepatic, or cardiovascular disease, the elderly, and in difficult resuscitations [35,52,53,54,55]. A variety of measurements have also been evaluated as alternatives to UOP, without identification of consistently superior performance [33,54,55,56].
Base excess and lactate, as well as the correction rate thereof, are reliable predictors of mortality [57,58,59]. However, these variables are not specific to burn shock alone, and lactate may remain elevated despite adequate resuscitation due to impaired hepatic or renal clearance, cyanide toxicity, or the infusion of epinephrine [33,35,60,61,62].
Small studies have demonstrated the usefulness of trending hemoglobin and hematocrit as markers of resuscitative efforts. Hemoconcentration is a common response to burn shock, and the resolution thereof can be used to evaluate the response to therapy. One study found that a lower hematocrit level (45% vs. 55%) was associated with increased urine output and decreased base deficit at 24 h, and a lower incidence of complications and of mortality [63]. This approach to monitoring must be tempered by the fact that patients with deeper burns may experience a decrease in hematocrit secondary to hemolysis.
Advanced hemodynamic monitoring is an expanding field of critical care of which some technologies have been studied in burn shock and some have not. Advanced hemodynamic monitoring generally includes modalities such as pulmonary artery catheterization, transpulmonary thermodilution (LiDCO, PiCCO), pulse-contour analysis of the arterial waveform, and echocardiographic evaluation [64]. Two meta-analyses have evaluated mortality with hemodynamic monitoring compared to UOP, and did not demonstrate a conclusive decrease in mortality [56,65]. Davenport et al. also reported “improved” UOP with hemodynamic monitoring, but three of five studies reported UOP in the hemodynamic monitoring group above 0.5–1 mL/kg/h, compared to only one above the goal in the UOP group.
Not all hemodynamic metrics are equally effective at guiding resuscitation. Improvements in cardiac and oxygen transport rate correlate more closely with intrathoracic blood volume index (ITBVI) than central venous pressure (CVP) or pulmonary capillary wedge pressure (PCWP), suggesting that the former may be a better representation of preload [66]. Paratz et al. noted that studies using preload tended to report increased or unchanged resuscitation volumes, while one study that used stroke volume variability reported decreased total volumes. This supports the assertion by Pham et al., that targeting preload contributes to over-resuscitation. Rather, “permissive hypovolemia”, in which a low or low–normal preload is targeted, may help mitigate this [35,56,67,68].
Point of care ultrasound (POCUS) can also be a valuable adjunct to determine intravascular volume status and fluid responsiveness. One meta-analysis of eight studies found the sensitivity and specificity of inferior vena cava (IVC) respiratory variation to be 0.76 and 0.86, respectively, in predicting fluid responsiveness. IVC variation is subject to extrinsic forces and must be interpreted carefully [69]. Cardiac output measurement by ultrasonography may provide additional assessment of preload status, though transthoracic echocardiography can be very challenging in burn-injured patients due to burns to the chest that interfere with image acquisition. Hemodynamic transesophageal echocardiography (hTEE) provides a low-risk means to monitor cardiac preload and contractility real-time throughout the resuscitative period [64].
7. Adjuncts to Resuscitation
Though volume resuscitation in burn shock primarily includes crystalloid fluid solutions such as LR, other fluids are often used as resuscitation adjuncts, primarily to “rescue” a patient who is receiving an excessive volume [70]. Of these fluids, albumin and plasma are the most frequently used in clinical practice [71,72,73,74,75,76]. Pruitt et al. reported in 1971 that varying doses of colloid provided during the first 24 h postburn had no apparent effect on the rate of plasma volume loss. This prompted the elimination of albumin from the modified Brooke formula during the first postburn day [77]. Goodwin and colleagues then conducted a randomized controlled trial comparing crystalloid vs. crystalloid and albumin, during the first 24 h postburn. These authors found an increase in extravascular lung water in the colloid group, but also reported that the colloid group received a lower resuscitation volume than the crystalloid group [78]. Demling and colleagues, in an ovine model, documented a decrease in the lymph flow rate and in the lymph-to-plasma protein ratio beginning around 8–12 h postburn in unburned tissue [79] This suggests that increased microvascular permeability to protein begins to resolve at that timepoint, and implies that colloid becomes more effective than crystalloid as a volume expander thereafter.
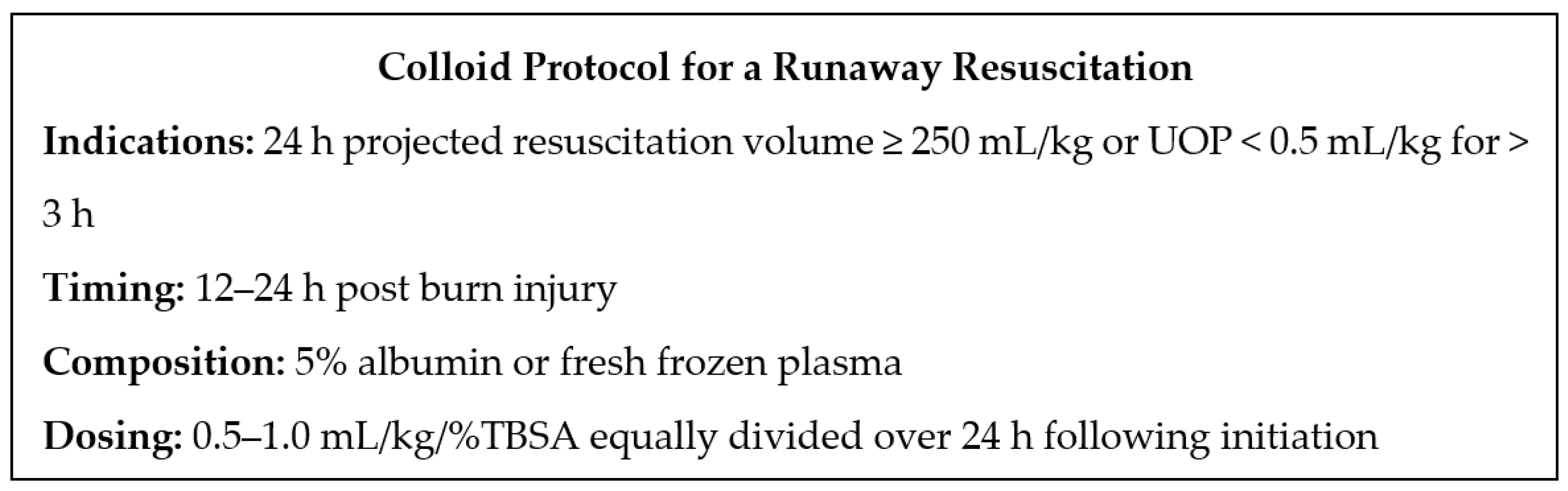
Several recent studies have suggested that colloid is useful in decreasing total fluid administration, thereby reducing the risk of “fluid creep,” edema formation, and compartment syndrome, especially when started on an as-needed basis later during the first postburn day. But there is little consensus with respect to indications or dosing, and use of colloid has not been demonstrated to have a mortality benefit [8,55,70,80,81,82]. The approach to colloid rescue currently utilized at the US Army Burn Center is offered in Figure 4.
Investigation is ongoing into the use of plasma, with some evidence suggesting that its use may result in reduction of resuscitation volumes by reversing glycocalyx damage [8,55,76,80,83]. High-dose ascorbic acid has also been associated with reducing total resuscitation volumes, but without demonstration of mortality benefit to date, and some evidence of increased risk of renal injury via oxalate nephropathy [73,74,75].
The gastrointestinal (GI) tract has been evaluated as an alternate route for fluid administration during burn shock. Historically, oral or enteral resuscitation has been performed mainly in resource-limited settings or mass casualty events [31,84,85]. Based on extensive experience with oral resuscitation of patients with cholera using the World Health Organization oral rehydration salt solution, it is reasonable to expect similar efficacy in burn patients. More research is needed to further define how best to employ GI resuscitation in burns.
Burn injury results in massive catecholamine release resulting in increased vascular tone and vasoconstriction, which complicates the use of vasopressors in this patient population. Recognizing that the main reason for hypotension during burn shock is hypovolemia, vasopressors should be used if hemodynamic instability persists in spite of efforts to provide adequate preload [86,87]. A recent retrospective review of 52 patients performed by Adibafar et al. revealed that vasopressors were more commonly used in patients who were older and had larger burns as well as a higher incidence of inhalation injury and use of mechanical ventilation [88]. However, the authors did not identify any significant difference in albumin use or in total volume of resuscitation at 24 h. When considering implementation of vasopressors, other causes of shock must be considered, such as identification of cardiomyopathy so as to tailor therapies, i.e., initiation of inotropic support versus increasing afterload [77].
High-volume hemofiltration (HVHF) is thought to mitigate cytokine-driven vasculopathy and has demonstrated promise in retrospective data analysis with respect to reduction of vasopressor requirements in septic shock and in burn-injured patients [89,90,91,92,93]. Studies are ongoing regarding application of HVHF in the treatment of burn shock as a volume-sparing adjunct.
Lastly, computerized decision-support systems have been designed and implemented wherein data such as urine output and resuscitation fluid rate are inputted hourly and, utilizing advanced modeling, a fluid rate for the next hour is recommended. These burn resuscitation decision-support systems (BRDSS) have been shown to decrease resuscitation volumes and are associated with decreased ventilator days and hospital mortality [94] (Figure 5). BRDSS may help identify appropriate use of adjuncts to mitigate the risk of complications associated with over-resuscitation. It may also reduce the tendency to tolerate UOP above the goal, by reassuring clinicians who may otherwise have hesitated to decrease the fluid rate [55].
8. Complications of Resuscitation
Precise titration of fluid rate is critical due to high morbidity of both under-resuscitation and over-resuscitation. Under-resuscitation leads to uncontrolled burn shock, inadequate organ perfusion, and eventually organ failure and death. Over-resuscitation increases the risk of massive edema formation, causing elevated compartment pressures including the abdominal, ocular and extremity compartments, conversion of superficial to deep burns, and acute respiratory distress syndrome (ARDS). Over-resuscitation is recognized as a frequent hazard even in burn units with experienced staff. Interestingly, this appears to be a relatively recent phenomenon. Earlier literature reports that the Parkland formula accurately predicts total resuscitation volume, while more recent data reflect Parkland as almost always underestimating total volumes [24,33,35,37,52,54,95]. Possible mechanisms include increasing use of opioids and sedatives that counter the stress response and promote vasodilation, increasing proportion of patients with large burns, more intravenous fluids in the prehospital setting, decreased use of colloids, overestimation of burn size and depth, higher rates of comorbidities, and use of alternate endpoints that require higher volumes to normalize. Clinicians also tend to increase fluids without hesitation when endpoints are below the goal, but tolerate parameters above the goal without decreasing fluid rate. This preference for erring on the side of more fluids is exacerbated by monitoring multiple endpoints since one parameter dipping below the goal may precipitate an increase in the fluid rate, even if all others are within the goal range [8,35,54]. Appropriate titration of fluids, use of adjuncts, ensuring accurate %TBSA calculation, and judicious use of medications with hemodynamic effects can all help avoid or mitigate the effects of over-resuscitation.
The following complications may be seen during resuscitation. Avoidance of over-resuscitation will likely prevent the worst of these problems.
Thoracic eschar syndrome occurs when thoracic compliance is impaired due to large areas of eschar resulting in decreased chest excursion and increased inspiratory pressure, which may progress to cardiopulmonary arrest if not promptly treated. Treatment is urgent escharotomy of the chest [96].
Extremity eschar syndromes are caused by tight, inelastic eschar encircling an extremity, with progressive edema formation in the subjacent tissue. They are diagnosed by hourly Doppler flowmetry of distal pulses. By elevating burned extremities above the level of the heart during burn shock resuscitation, transvascular hydrostatic pressure and the risk of this syndrome can be reduced but not eliminated. Treatment is escharotomy of circumferential full-thickness burns of involved limbs, hands, and/or fingers.
Both thoracic and extremity escharotomies are usually done at the bedside under semi-sterile conditions using intravenous sedation and electrocautery.
Extremity intramuscular compartment syndromes are caused by edema within the investing fascia and should not be confused with extremity eschar syndromes. Performance of an extremity escharotomy does not guarantee that the patient will not develop an intramuscular compartment syndrome requiring operative fasciotomy. Thus, continued monitoring of the extremities even after an escharotomy is mandatory [97].
Abdominal compartment syndrome (ACS) is more likely to occur when 24 h fluid resuscitation exceeds 250 mL/kg. Abdominal compartment syndrome is heralded by intra-abdominal hypertension, diagnosed by measurement of bladder pressures. Treatment includes paracentesis and/or decompressive laparotomy. Death is likely in burn patients who develop ACS, despite laparotomy, due to loss of domain and inability to close the abdomen. Thus, ACS must be avoided by infusing less than 250 mL/kg [98].
Orbital compartment syndrome (OCS) is also common in patients following large-volume resuscitation, but can occur within hours of injury in patients with deep burns of the periorbital region. Immediate ophthalmology consultation for these patients is indicated. Diagnosis of OCS is by measurement of intraocular pressures using a tonometer. Treatment is lateral canthotomy and cantholysis [99].
9. Pitfalls of Resuscitation
A number of conditions can complicate burn resuscitation (Table 2). Elderly burn patients have increased mortality and complication rates, and optimizing their care presents a number of challenges [20,100,101,102]. Age has most frequently been associated with an increased volume requirement during resuscitation (although Benicke et al. did note a non-significant decrease), likely driven by decreased physiologic reserve as well as pre-existing hypovolemia and hypoproteinemia from poor oral intake [42,100,101]. Decreased baseline cardiac and pulmonary function renders elderly patients more susceptible to sequelae of volume overload, so hemodynamic monitoring should be used in concert with UOP to optimize perfusion and cardiac function [99,100,101,102]. Nutrition management should be aggressive since pre-existing malnutrition, presbyphagia, and anorexia combine with age-related changes in immune function and skin proliferation to compromise healing capacity. Placement of a Dobhoff tube should be considered in patients who are unable to meet calorie or protein requirements [100,101,102,103,104]. Pain and anxiety control, judicious use of sedation, early rehabilitation, and delirium precautions mitigate deconditioning [100,101,105].
Obesity has frequently been associated with increased mortality and complication rates in burn patients [44,106,107,108,109,110,111]. However, when patients are stratified by class of obesity, there is evidence for a mortality benefit in mild obesity, although some smaller studies have failed to replicate this effect [112,113,114]. Methods for calculating burn size have been adjusted to account for body proportions of obese patients, but these have not been shown to result in significantly different calculations for most patients [44,114,115]. Overestimation of volume requirements when using actual body weight prompted the use of ideal body weight, but this led to underestimation [43,44]. Lindsey et al. demonstrated improved outcomes using an adjusted ideal body weight, but the benefit may be attributable using plasma, or to developments in practice over time, since historical controls were used [45]. Another proposed way to help optimize care is to admit obese patients to a burn unit regardless of whether they otherwise meet criteria [111].
Oliguric or anuric renal failure should prompt use of alternate endpoints for resuscitation. If acute, conversion to nonoliguric renal failure may be attempted with forced diuresis. The prevalence of acute kidney injury (AKI) in burn patients is a matter of some controversy. At the US Army Burn Center, Clemens et al. documented AKI of KDIGO Stage 1 or higher in 48% of 830 mechanically ventilated burn patients. AKI was an independent predictor of mortality in that study [116]. Prior to routine use of continuous renal replacement therapy (CRRT), burn-injured patients who developed an indication for renal replacement therapy demonstrated 50% to 90% mortality [117]. CRRT is now widely utilized and appears to be associated with a significant reduction in mortality in septic burn patients, but its utility in burn shock is unknown [118]. The managing team must also be wary of UOP that seemingly meets the goals of resuscitation but the patient demonstrates signs of hypoperfusion, as may occur in the setting of glucosuria or alcohol intoxication [119].
It has been demonstrated that the presence of inhalation injury may increase the total volume required for fluid resuscitation during burn shock. More recently, studies have suggested that the use of mechanical ventilation increases the resuscitation volume independent of concomitant inhalation injury. Mechanical ventilation increases intrathoracic pressure, thereby reducing venous return and increasing right ventricular afterload. This results in decreased left ventricular preload and diminished cardiac output [120]. In addition, mechanical ventilation is associated with biotrauma and systemic release of inflammatory mediators. It is possible that this also contributes to increased resuscitative fluid requirements during burn shock [121].
10. Analgesia and Sedation
Due to the painful nature of burn injuries and the need for invasive procedures, careful attention must be paid to managing analgesia and sedation so as to provide appropriate analgesia while avoiding hemodynamic compromise, delirium, and over-sedation. Because of the vasodilatory and sympatholytic properties of many analgesic and sedative medications, the hemodynamic effects of each medication must be scrutinized [122]. For example, the term ‘opioid creep’ has been used to attribute increased fluid resuscitation volumes to the overuse of narcotics during burn shock [123,124]. Ketamine has been shown to have an opiate-sparing effect in burn-injured patients, and a favorable hemodynamic profile (short of the anesthetic induction dose) in most patients with shock [125,126]. A multi-modal regimen is preferred so as to limit dose-dependent effects and to target multiple pain-transducing pathways [127]. It is also important to note alterations of pharmacokinetics and pharmacodynamics. The resuscitative phase is associated with changes in medication distribution, metabolism and availability. Plasma loss and decreased glomerular filtration rate result in a decreased volume of distribution, slower rate of distribution, and decreased drug clearance [128,129]
11. Wound Management during Resuscitation
As soon as possible after admission to the burn center, and while active resuscitation is ongoing, thorough debridement of nonviable tissue, debris, blistered skin, and exudate is performed. Significant variability in wound care management exists across burn centers; a surgical antiseptic such as chlorhexidine gluconate 4.0% should be used [30,34]. At the US Army Burn Center, debridement is done in a specially designed, temperature-controlled shower room. In other facilities, the operating theater is used for this purpose, but general anesthesia should be performed with care during burn shock. Following debridement, a topical antimicrobial is applied. A variety of topical agents are available. A good choice for patients with extensive burns is application of mafenide acetate cream in the morning, alternating with silver sulfadiazine cream in the evening. An option for patients with clean wounds is a silver-impregnated dressing such as silver nylon. In several countries, a combination of cerium nitrate and silver sulfadiazine cream (Flammacerium) is available. The cerium component is proposed to have immune-enhancing and anti-inflammatory effects, and also generates a tough protective layer of eschar. Daily assessment and cleaning of the burn wounds is paramount so as limit the risk of wound infection [20]. Patients with deep partial and/or full-thickness burns are prepared for operative excision and grafting, typically beginning as soon as the first postburn day if hemodynamic stability has been achieved.
12. Rehabilitation during Resuscitation
Physical and occupational rehabilitation must start as early as possible so as to promote favorable long-term outcomes, particularly in the most severely injured patients. Early mobilization may prove challenging in critically ill burn patients due to hemodynamic instability and interventions such as renal replacement therapy (RRT), mechanical ventilation, and deep sedation. Despite these challenges, our practice at the US Army Burn Center is for a burn rehabilitation therapist to perform initial evaluation within 24 h of admission for all burn patients and initiate early interventions. Thus, rehabilitation is a fundamental component of burn care, even during active resuscitation.
Rehabilitation interventions include elevation of burned extremities so as to reduce the risks of eschar and compartment syndrome following resuscitation, limb range-of-motion exercises and frequent re-positioning to reduce edema and the risk of contractures, as well as to optimize mobility and function [130]. Therapy should be escalated as the patient becomes increasingly able to participate [20,131]. More intensive interventions prepare patients for ambulation and include sitting position, sitting at the edge of bed, positioning via tilt table, and use of assistive devices [132]. Behavioral health providers should be involved early in the care of burn patients and this care should continue after discharge [20].
Nutritional support must also commence as soon as possible. Because of postburn hypermetabolism, patients with burn size >30% TBSA can rarely meet their nutritional needs by mouth. Thus, they routinely receive a Dobhoff feeding tube (placed post-pylorically if possible) with a goal of initiating enteral nutrition by the 24th postburn hour.
13. Conclusions
Care for the acute burn patient is complex and requires prompt wound assessment, as well as evaluation for other concomitant injuries, such as inhalation injury and traumatic wounds. Subsequent phases of burn management include aggressive volume administration utilizing one of the multiple available resuscitation formulas. Administration of colloid should be considered in the setting of massive fluid resuscitation or failed resuscitation, and vasopressors should be used judiciously to preserve mean arterial pressure. Proper selection of adequate analgesia and sedation is required to facilitate frequent wound care. Monitoring for complications of resuscitation is important, particularly life-threatening complications such as compartment syndrome. Further study is required to elucidate the mechanism of and role for resuscitation adjuncts, such as colloids, oral resuscitation and renal replacement therapy.
Author Contributions
Conceptualization, G.W.B.; methodology, G.W.B.; investigation, J.M.C., L.A.S., G.W.B., L.C.C.; data curation, J.M.C., L.A.S., G.W.B.; writing—original draft preparation, J.M.C., L.A.S., G.W.B.; writing—review and editing, J.M.C., L.A.S., A.P.B., G.W.B., L.C.C.; supervision, G.W.B., A.P.B., L.C.C.; project administration, G.W.B., A.P.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
L.C.C. is a coinventor of Burn Navigator; he has assigned his rights to the US Army. The authors report no other conflicts of interest or external funding source. The opinions expressed in this manuscript are solely those of the authors and do not necessarily represent the views of the Uniformed Services University, the US Army Institute of Surgical Research, the Army Medical Department, the US Army, or the United States Government.
References
- Pruitt, B.A. The effectiveness of fluid resuscitation. J. Trauma 1979, 19, S868–S870. [Google Scholar]
- Haberal, M.; Abali, A.E.S.; Karakayali, H. Fluid management in major burn injuries. Indian J. Plast. Surg. 2010, 43, 29–36. [Google Scholar] [CrossRef]
- Rowan, M.P.; Cancio, L.C.; Elster, E.A.; Burmeister, D.M.; Rose, L.F.; Natesan, S.; Chan, R.K.; Christy, R.J.; Chung, K.K. Burn wound healing and treatment: Review and advancements. Crit. Care 2015, 19, 243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, K.K.; Bacomo, F.K. A primer on burn resuscitation. J. Emergencies Trauma Shock 2011, 4, 109–113. [Google Scholar] [CrossRef]
- Snell, J.A.; Loh, N.-H.W.; Mahambrey, T.; Shokrollahi, K. Clinical review: The critical care management of the burn patient. Crit. Care 2013, 17, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Horton, J.W. Left ventricular contractile dysfunction as a complication of thermal injury. Shock 2004, 22, 495–507. [Google Scholar] [CrossRef]
- Woodcock, T.E. Revised Starling equation and the glycocalyx model of transvascular fluid exchange: An improved paradigm for prescribing intravenous fluid therapy. Br. J. Anaesth. 2012, 108, 384–394. [Google Scholar] [CrossRef] [Green Version]
- Gurney, J.M.; Kozar, R.A.; Cancio, L.C. Plasma for burn shock resuscitation: Is it time to go back to the future? Transfusion 2019, 59, 1578–1586. [Google Scholar] [CrossRef] [Green Version]
- Purdue, G.F.; Hunt, J.L. Multiple trauma and the burn patient. Am. J. Surg. 1989, 158, 536–539. [Google Scholar] [CrossRef]
- Pruitt, L.B.A. Management of Burns in the Multiple Injury Patient. Surg. Clin. N. Am. 1970, 50, 1283–1300. [Google Scholar] [CrossRef]
- Dougherty, W.; Waxman, K. The complexities of managing severe burns with associated trauma. Surg. Clin. N. Am. 1996, 76, 923–958. [Google Scholar] [CrossRef]
- Santaniello, J.M.; Luchette, F.; Esposito, T.J.; Gunawan, H.; Reed, R.L.; Davis, K.A.; Gamelli, R.L. Ten Year Experience of Burn, Trauma, and Combined Burn/Trauma Injuries Comparing Outcomes. J. Trauma Inj. Infect. Crit. Care 2004, 57, 696–701. [Google Scholar] [CrossRef] [PubMed]
- Brandt, C.P.; Yowler, C.J.; Fratianne, R.B. Burns with multiple trauma. Am. Surg. 2002, 68, 240–244. [Google Scholar]
- Hawkins, A.; MacLennan, P.A.; McGwin, G.; Cross, J.M.; Rue, L.W. The Impact of Combined Trauma and Burns on Patient Mortality. J. Trauma Inj. Infect. Crit. Care 2005, 58, 284–288. [Google Scholar] [CrossRef] [PubMed]
- Battaloglu, E.; Iniguez, M.F.; Lecky, F.; Porter, K. Incidence of combined burns and major trauma in England and Wales. Trauma 2018, 22, 51–55. [Google Scholar] [CrossRef]
- Purdue, G.F.; Hunt, J.L.; Layton, T.R.; Copeland, C.E.; Delmundo, A.G.; Baxter, C.R. Burns in Motor Vehicle Accidents. J. Trauma Inj. Infect. Crit. Care 1985, 25, 216–219. [Google Scholar] [CrossRef]
- Wolf, S.E.; Kauvar, D.S.; Wade, C.E.; Cancio, L.C.; Renz, E.P.; Horvath, E.E.; White, C.E.; Park, M.S.; Wanek, S.; Albrecht, M.A.; et al. Comparison Between Civilian Burns and Combat Burns from Operation Iraqi Freedom and Operation Enduring Freedom. Ann. Surg. 2006, 243, 786–795. [Google Scholar] [CrossRef]
- Harrington, D.T. Complicated Burn Resuscitation. Crit. Care Clin. 2016, 32, 577–586. [Google Scholar] [CrossRef] [PubMed]
- Clarey, A.; Trainor, D. Critical care management of severe burns and inhalational injury. Anaesth. Intensiv. Care Med. 2017, 18, 395–400. [Google Scholar] [CrossRef]
- Jeschke, M.G.; Van Baar, M.E.; Choudhry, M.A.; Chung, K.K.; Gibran, N.S.; Logsetty, S. Burn injury. Nat. Rev. Dis. Prim. 2020, 6, 11. [Google Scholar] [CrossRef]
- Woodson, L.C.; Branski, L.K.; Enkhbaatar, P.; Talon, M. Diagnosis and treatment of inhalation injury. In Total Burn Care, 5th ed.; Hernon, D., Ed.; Elsevier: Amsterdam, The Netherlands, 2018; pp. 184–194. [Google Scholar]
- Douin, D.; Schauer, S.G.; Anderson, E.L.; Jones, J.; DeSanto, K.; Cunningham, C.W.; Bebarta, V.S.; Ginde, A.A. Systematic review of oxygenation and clinical outcomes to inform oxygen targets in critically ill trauma patients. J. Trauma Acute Care Surg. 2019, 87, 961–977. [Google Scholar] [CrossRef]
- Wachtel, T.L.; Berry, C.C.; Wachtel, E.E.; Frank, H.A. The inter-rater reliability of estimating the size of burns from various burn area chart drawings. Burns 2000, 26, 156–170. [Google Scholar] [CrossRef]
- Giretzlehner, M.; Ganitzer, I.; Haller, H. Technical and Medical Aspects of Burn Size Assessment and Documentation. Medicina 2021, 57, 242. [Google Scholar] [CrossRef]
- Parvizi, D.; Kamolz, L.-P.; Giretzlehner, M.; Haller, H.L.; Trop, M.; Selig, H.; Nagele, P.; Lumenta, D.B. The potential impact of wrong TBSA estimations on fluid resuscitation in patients suffering from burns: Things to keep in mind. Burns 2014, 40, 241–245. [Google Scholar] [CrossRef]
- Murari, A.; Singh, K.N. Lund and Browder chart—modified versus original: A comparative study. Acute Crit. Care 2019, 34, 276–281. [Google Scholar] [CrossRef] [Green Version]
- Parvizi, D.; Giretzlehner, M.; Wurzer, P.; Klein, L.D.; Shoham, Y.; Bohanon, F.J.; Haller, H.L.; Tuca, A.; Branski, L.K.; Lumenta, D.B.; et al. BurnCase 3D software validation study: Burn size measurement accuracy and inter-rater reliability. Burns 2016, 42, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Sheng, W.-B.; Zeng, D.; Wan, Y.; Yao, L.; Tang, H.-T.; Xia, Z.-F. BurnCalc assessment study of computer-aided individual three-dimensional burn area calculation. J. Transl. Med. 2014, 12, 242. [Google Scholar] [CrossRef]
- Prieto, M.F.; Acha, B.; Gomez-Cia, T.; Fondón, I.; Serrano, C. A system for 3D representation of burns and calculation of burnt skin area. Burns 2011, 37, 1233–1240. [Google Scholar] [CrossRef] [PubMed]
- Greenhalgh, D.G. Burn resuscitation: The results of the ISBI/ABA survey. Burns 2010, 36, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Blumetti, J.; Hunt, J.L.; Arnoldo, B.D.; Parks, J.K.; Purdue, G.F. The Parkland formula under fire: Is the criticism justified? J. Burn Care Res. 2008, 29, 180–186. [Google Scholar] [CrossRef] [Green Version]
- Bhat, S.; Humphries, Y.M.; Gulati, S.; Rylah, B.; Olson, W.E.; Twomey, J. The problems of burn resuscitation formulas: A need for a simplified guideline. J. Burn. Wounds 2004, 3, 7. [Google Scholar]
- Boehm, D.; Menke, H. A History of Fluid Management—From “One Size Fits All” to an Individualized Fluid Therapy in Burn Resuscitation. Medicina 2021, 57, 187. [Google Scholar] [CrossRef]
- Al-Benna, S.; Leary, J.; Sheikh, Z.; Rodrigues, J. A survey of fluid resuscitation protocols of burns in intensive care units of the United Kingdom and Ireland. Burns 2009, 35, S14–S15. [Google Scholar] [CrossRef]
- Pham, T.N.; Cancio, L.C.; Gibran, N. American Burn Association Practice Guidelines Burn Shock Resuscitation. J. Burn Care Res. 2008, 29, 257–266. [Google Scholar] [CrossRef]
- Csontos, C.; Foldi, V.; Fischer, T.; Bogar, L. Factors affecting fluid requirement on the first day after severe burn trauma. ANZ J. Surg. 2007, 77, 745–748. [Google Scholar] [CrossRef]
- Klein, M.B.; Hayden, D.; Elson, C.; Nathens, A.B.; Gamelli, R.L.; Gibran, N.S.; Herndon, D.N.; Arnoldo, B.; Silver, G.; Schoenfeld, D.; et al. The Association Between Fluid Administration and Outcome Following Major Burn. Ann. Surg. 2007, 245, 622–628. [Google Scholar] [CrossRef] [PubMed]
- American Burn Association. Disaster Management. 2019. Available online: https://ameriburn.org/quality-care/disaster-response/disaster-management/ (accessed on 25 June 2021).
- Chung, K.K.; Salinas, J.; Renz, E.M.; Alvarado, R.A.; King, B.T.; Barillo, D.J.; Cancio, L.C.; Wolf, S.; Blackbourne, L.H. Simple Derivation of the Initial Fluid Rate for the Resuscitation of Severely Burned Adult Combat Casualties: In Silico Validation of the Rule of 10. J. Trauma Inj. Infect. Crit. Care 2010, 69, S49–S54. [Google Scholar] [CrossRef] [Green Version]
- Gueugniaud, P.Y.; Carsin, H.; Bertin-Maghit, M.; Petit, P. Current advances in the initial management of major thermal burns. Intensive Care Med. 2000, 26, 848–856. [Google Scholar] [CrossRef] [PubMed]
- Driscoll, I.R.; Gurney, J.; Stockinger, Z.T.; Renz, E.M.; Cancio, L.C.; Chung, K.K.; King, B.T.; Rizzo, J.A.; Graybill, J.C.; Peterson, W.C.; et al. Burn Care Clinical Practice Guideline. Available online: https://jts.amedd.army.mil/index.cfm/PI_CPGs/cpgs (accessed on 25 June 2021).
- Benicke, M.; Perbix, W.; Lefering, R.; Knam, F.; Ipaktchi, K.R.; Tannapfel, A.; Neugebauer, E.A.; Spilker, G. New multifactorial burn resuscitation formula offers superior predictive reliability in comparison to established algorithms. Burns 2009, 35, 30–35. [Google Scholar] [CrossRef]
- Rosenthal, J.; Clark, A.; Campbell, S.; McMahon, M.; Arnoldo, B.; Wolf, S.E.; Phelan, H. Effects of obesity on burn resuscitation. Burns 2018, 44, 1947–1953. [Google Scholar] [CrossRef]
- Rae, L.; Pham, T.N.; Carrougher, G.; Honari, S.; Gibran, N.S.; Arnoldo, B.D.; Gamelli, R.L.; Tompkins, R.G.; Herndon, D.N. Differences in Resuscitation in Morbidly Obese Burn Patients May Contribute to High Mortality. J. Burn Care Res. 2013, 34, 507–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindsey, L.; Purvis, M.; Miles, D.; Lintner, A.; Scott, V.; McGinn, K.; Bright, A.; Kahn, S. An Adjusted Ideal Body Weight Index Formula with Fresh Frozen Plasma (FFP) Rescue Decreases Fluid Creep During Burn Resuscitation. Ann. Burn. Fire Disasters 2020, 33, 216–223. [Google Scholar]
- Liu, N.T.; Fenrich, C.A.; Serio-Melvin, M.L.; Peterson, W.C.; Cancio, L.C.; Salinas, J. The impact of patient weight on burn resuscitation. J. Trauma Acute Care Surg. 2017, 83, S112–S119. [Google Scholar] [CrossRef] [PubMed]
- Gus, E.; Cleland, H. Burn fluid resuscitation formulae: Concept and misconception. Injury 2021, 52, 780–781. [Google Scholar] [CrossRef]
- Alvarado, R.; Chung, K.K.; Cancio, L.C.; Wolf, S.E. Burn resuscitation. Burns 2009, 35, 4–14. [Google Scholar] [CrossRef]
- Leclerc, T.; Potokar, T.; Hughes, A.; Norton, I.; Alexandru, C.; Haik, J.; Moiemen, N.; Almeland, S.K. A simplified fluid resuscitation formula for burns in mass casualty scenarios: Analysis of the consensus recommendation from the WHO Emergency Medical Teams Technical Working Group on Burns. Burns 2021. [Google Scholar] [CrossRef] [PubMed]
- Cancio, L.C. Initial Assessment and Fluid Resuscitation of Burn Patients. Surg. Clin. N. Am. 2014, 94, 741–754. [Google Scholar] [CrossRef] [PubMed]
- Herndon, D.N.; Culnan, D.M.; Sherman, W.C.; Chung, K.K.; Wolf, S.E. Critical Care in the Severely Burned: Organ Support and Management. In Total Burn Care; Elsevier: Amsterdam, The Netherlands, 2018; pp. 328–354. [Google Scholar]
- Diver, A.J. The evolution of burn fluid resuscitation. Int. J. Surg. 2008, 6, 345–350. [Google Scholar] [CrossRef] [Green Version]
- Holm, C.; Mayr, M.; Tegeler, J.; Hörbrand, F.; von Donnersmarck, G.H.; Mühlbauer, W.; Pfeiffer, U. A clinical randomized study on the effects of invasive monitoring on burn shock resuscitation. Burns 2004, 30, 798–807. [Google Scholar] [CrossRef] [PubMed]
- Tricklebank, S. Modern trends in fluid therapy for burns. Burns 2009, 35, 757–767. [Google Scholar] [CrossRef]
- Hodgman, E.I.; Subramanian, M.; Arnoldo, B.D.; Phelan, H.A.; Wolf, S.E. Future Therapies in Burn Resuscitation. Crit. Care Clin. 2016, 32, 611–619. [Google Scholar] [CrossRef]
- Paratz, J.D.; Stockton, K.; Paratz, E.D.; Blot, S.; Muller, M.; Lipman, J.; Boots, R. Burn Resuscitation—Hourly Urine Output Versus Alternative Endpoints. Shock 2014, 42, 295–306. [Google Scholar] [CrossRef]
- Andel, D.; Kamolz, L.-P.; Roka, J.; Schramm, W.; Zimpfer, M.; Frey, M.; Andel, H. Base deficit and lactate: Early predictors of morbidity and mortality in patients with burns. Burns 2007, 33, 973–978. [Google Scholar] [CrossRef]
- Kamolz, L.-P.; Andel, H.; Schramm, W.; Meissl, G.; Herndon, D.; Frey, M. Lactate: Early predictor of morbidity and mortality in patients with severe burns. Burns 2005, 31, 986–990. [Google Scholar] [CrossRef]
- Muthukumar, V.; Arumugam, P.K.; Narasimhan, A.; Kumar, S.; Sharma, U.; Sharma, S.; Kain, R. Blood Lactate and Lactate Clearance: Refined Biomarker and Prog-nostic Marker in Burn Resuscitation. Ann. Burn. Fire Disasters 2020, 33, 293–298. [Google Scholar]
- Sterling, S.A.; Puskarich, M.; Jones, A.E. The effect of liver disease on lactate normalization in severe sepsis and septic shock: A cohort study. Clin. Exp. Emerg. Med. 2015, 2, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Luft, F.C. Lactic Acidosis Update for Critical Care Clinicians. J. Am. Soc. Nephrol. 2001, 12, S15–S19. [Google Scholar] [CrossRef]
- Baud, F.J.; Borron, S.W.; Mégarbane, B.; Trout, H.; Lapostolle, F.; Vicaut, E.; Debray, M.; Bismuth, C. Value of lactic acidosis in the assessment of the severity of acute cyanide poisoning. Crit. Care Med. 2002, 30, 2044–2050. [Google Scholar] [CrossRef]
- Zhao, L.-P.; Huang, Y.-S.; He, T.; Hu, X.-G. Clinical study on hematocrit used as a predictor for evaluation of resuscitation effect in the early shock stage after burn. Zhonghua Shao Shang Za Zhi Zhonghua Shaoshang Zazhi Chin. J. Burn. 2013, 29, 235–238. [Google Scholar]
- Held, J.M.; Litt, J.; Kennedy, J.D.; McGrane, S.; Gunter, O.L.; Rae, L.; Kahn, S.A. Surgeon-Performed Hemodynamic Transesophageal Echo-cardiography in the Burn Intensive Care Unit. J. Burn Care Res. 2016, 37, e63–e68. [Google Scholar] [CrossRef]
- Davenport, L.; Dobson, G.P.; Letson, H.L. The role of invasive monitoring in the resuscitation of major burns: A systematic review and meta-analysis. Int. J. Burn. Trauma 2019, 9, 28–40. [Google Scholar]
- Holm, C.; Melcer, B.; Hörbrand, F.; Wörl, H.; Von Donnersmarck, G.H.; Mühlbauer, W. Intrathoracic Blood Volume as an End Point in Resuscitation of the Severely Burned: An Observational Study of 24 Patients. J. Trauma Inj. Infect. Crit. Care 2000, 48, 728–734. [Google Scholar] [CrossRef]
- Arlati, S.; Storti, E.; Pradella, V.; Bucci, L.; Vitolo, A.; Pulici, M. Decreased fluid volume to reduce organ damage: A new approach to burn shock resuscitation? A preliminary study. Resuscitation 2007, 72, 371–378. [Google Scholar] [CrossRef]
- Sánchez, M.; García-De-Lorenzo, A.; Herrero, E.; Lopez, T.; Galvan, B.; Asensio, M.J.; Cachafeiro, L.; Casado, C. A protocol for resuscitation of severe burn patients guided by transpulmonary thermodilution and lactate levels: A 3-year prospective cohort study. Crit. Care 2013, 17, R176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Z.; Xu, X.; Ye, S.; Xu, L. Ultrasonographic Measurement of the Respiratory Variation in the Inferior Vena Cava Diameter Is Predictive of Fluid Responsiveness in Critically Ill Patients: Systematic Review and Meta-analysis. Ultrasound Med. Biol. 2014, 40, 845–853. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Comish, P.; Walsh, M.; Castillo-Angeles, M.; Kuhlenschmidt, K.; Carlson, D.; Arnoldo, B.; Kubasiak, J. Adoption of rescue colloid during burn resuscitation decreases fluid administered and restores end-organ perfusion. Burns 2021. [Google Scholar] [CrossRef]
- Navickis, R.J.; Greenhalgh, D.G.; Wilkes, M.M. Albumin in Burn Shock Resuscitation. J. Burn Care Res. 2016, 37, e268–e278. [Google Scholar] [CrossRef] [Green Version]
- Vlachou, E.; Gosling, P.; Moiemen, N. Hydroxyethylstarch supplementation in burn resuscitation—A prospective randomised controlled trial. Burns 2010, 36, 984–991. [Google Scholar] [CrossRef]
- Tanaka, H.; Matsuda, T.; Miyagantani, Y.; Yukioka, T.; Matsuda, H.; Shimazaki, S. Reduction of Resuscitation Fluid Volumes in Severely Burned Patients Using Ascorbic Acid Administration. Arch. Surg. 2000, 135, 326–331. [Google Scholar] [CrossRef] [Green Version]
- Kahn, S.A.; Beers, R.J.; Lentz, C.W. Resuscitation after Severe Burn Injury Using High-Dose Ascorbic Acid: A Retrospective Review. J. Burn Care Res. 2011, 32, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Falwell, S.; Greenhalgh, D.; Palmieri, T.; Sen, S. High-Dose Ascorbic Acid for Burn Shock Resuscitation May Not Improve Outcomes. J. Burn Care Res. 2018, 39, 708–712. [Google Scholar] [CrossRef] [PubMed]
- Cruz, M.V.; Carney, B.C.; Luker, J.N.; Monger, K.W.; Vazquez, J.S.; Moffatt, L.T.; Johnson, L.S.; Shupp, J.W. Plasma Ameliorates Endothelial Dysfunction in Burn Injury. J. Surg. Res. 2018, 233, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Pruitt, B.A., Jr.; Mason, A.D., Jr.; Moncrief, J.A. Hemodynamic changes in the early postburn patient: The influence of fluid admin-istration and of a vasodilator (hydralazine). J. Trauma 1971, 11, 36–46. [Google Scholar] [CrossRef] [PubMed]
- Goodwin, C.W.; Dorethy, J.; Lam, V.; Pruitt, B.A. Randomized Trial of Efficacy of Crystalloid and Colloid Resuscitation on Hemodynamic Response and Lung Water Following Thermal Injury. Ann. Surg. 1983, 197, 520–531. [Google Scholar] [CrossRef]
- Demling, R.H.; Smith, M.; Bodai, B.; Harms, B.; Gunther, R.; Kramer, G. Comparison of Postburn Capillary Permeability in Soft Tissue and Lung. J. Burn. Care Rehabil. 1981, 2, 86–93. [Google Scholar] [CrossRef]
- O’Mara, M.; Slater, H.; Goldfarb, I.W.; Caushaj, P.F. A Prospective, Randomized Evaluation of Intra-abdominal Pressures with Crystalloid and Colloid Resuscitation in Burn Patients. J. Trauma Inj. Infect. Crit. Care 2005, 58, 1011–1018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kao, Y.; Loh, E.; Hsu, C.; Lin, H.; Huang, C.; Chou, Y.; Lien, C.; Tam, K. Fluid Resuscitation in Patients with Severe Burns: A Meta-analysis of Randomized Controlled Trials. Acad. Emerg. Med. 2018, 25, 320–329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eljaiek, R.; Heylbroeck, C.; Dubois, M.-J. Albumin administration for fluid resuscitation in burn patients: A systematic review and meta-analysis. Burns 2017, 43, 17–24. [Google Scholar] [CrossRef]
- Cartotto, R.; Greenhalgh, D. Colloids in Acute Burn Resuscitation. Crit. Care Clin. 2016, 32, 507–523. [Google Scholar] [CrossRef]
- Kramer, G.C.; Michell, M.W.; Oliveira, H.; Brown, T.L.H.; Herndon, D.; Baker, R.D.; Muller, M. Oral and Enteral Resuscitation of Burn Shock the Historical Record and Implications for Mass Casualty Care. Eplasty 2010, 10, e56. [Google Scholar]
- Moghazy, A.; Adly, O.; Elbadawy, M.; Hashem, R. Evaluation of who oral rehydration solution (ORS) and salt tablets in resuscitating adult patients with burns covering more than 15% of total body surface area (TBSA). Ann. Burn. Fire Disasters 2016, 29, 43–47. [Google Scholar]
- Brownson, E.G.; Pham, T.N.; Chung, K.K. How to Recognize a Failed Burn Resuscitation. Crit. Care Clin. 2016, 32, 567–575. [Google Scholar] [CrossRef] [PubMed]
- Cancio, L.C.; Bohanon, F.J.; Kramer, G.C. Burn Resuscitation. In Total Burn Care, 5th ed.; Elsevier: Edinburgh, UK, 2018; pp. 77–86. [Google Scholar]
- Adibfar, A.; Camacho, F.; Rogers, A.D.; Cartotto, R. The use of vasopressors during acute burn resuscitation. Burns 2021, 47, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Payen, D.; Mateo, J.; Cavaillon, J.M.; Fraisse, F.; Floriot, C.; Vicaut, E. Impact of continuous venovenous hemofiltration on organ failure during the early phase of severe sepsis: A randomized controlled trial. Crit. Care Med. 2009, 37, 803–810. [Google Scholar] [CrossRef]
- Gaudry, S.; Hajage, D.; Schortgen, F.; Martin-Lefevre, L.; Pons, B.; Boulet, E.; Boyer, A.; Chevrel, G.; Lerolle, N.; Carpentier, D.; et al. Initiation Strategies for Renal-Replacement Therapy in the Intensive Care Unit. N. Engl. J. Med. 2016, 375, 122–133. [Google Scholar] [CrossRef]
- Chung, K.K.; Lundy, J.B.; Matson, J.R.; Renz, E.M.; White, C.E.; King, B.T.; Barillo, D.J.; Jones, J.A.; Cancio, L.C.; Blackbourne, L.H.; et al. Continuous venovenous hemofiltration in severely burned patients with acute kidney injury: A cohort study. Crit. Care 2009, 13, R62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, K.K.; Coates, E.C.; Smith, D.J.; Karlnoski, R.A.; Hickerson, W.L.; Arnold-Ross, A.L.; Mosier, M.J.; Halerz, M.; Sprague, A.M.; Mullins, R.F.; et al. High-volume hemofiltration in adult burn patients with septic shock and acute kidney injury: A multicenter randomized controlled trial. Crit. Care 2017, 21, 289. [Google Scholar] [CrossRef] [Green Version]
- You, B.; Zhang, Y.L.; Luo, G.X.; Dang, Y.M.; Jiang, B.; Huang, G.T.; Liu, X.Z.; Yang, Z.C.; Chen, Y.; Chen, J.; et al. Early application of continuous high-volume haemofiltration can reduce sepsis and improve the prognosis of patients with severe burns. Crit. Care 2018, 22, 173. [Google Scholar] [CrossRef] [Green Version]
- Salinas, J.; Chung, K.K.; Mann, E.A.; Cancio, L.C.; Kramer, G.C.; Serio-Melvin, M.L.; Renz, E.M.; Wade, C.E.; Wolf, S. Computerized decision support system improves fluid resuscitation following severe burns: An original study. Crit. Care Med. 2011, 39, 2031–2038. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sullivan, S.R.; Ahmadi, A.J.; Singh, C.N.; Sires, B.S.; Engrav, L.H.; Gibran, N.S.; Heimbach, D.M.; Klein, M.B. Elevated Orbital Pressure: Another Untoward Effect of Massive Resuscitation after Burn Injury. J. Trauma Inj. Infect. Crit. Care 2006, 60, 72–76. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Hughes, P.G. Escharotomy; StatPearls Publishing: Treasure Island, FL, USA, 2021. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK482120/ (accessed on 21 January 2021).
- Boccara, D.; Lavocat, R.; Soussi, S.; Legrand, M.; Chaouat, M.; Mebazaa, A.; Mimoun, M.; Blet, A.; Serror, K. Pressure guided surgery of compartment syndrome of the limbs in burn patients. Ann. Burn. Fire Disasters 2017, 30, 193–197. [Google Scholar]
- Ivy, M.E.; Atweh, N.A.; Palmer, J.; Possenti, P.P.; Pineau, M.; D’Aiuto, M. Intra-abdominal Hypertension and Abdominal Compartment Syndrome in Burn Patients. J. Trauma Inj. Infect. Crit. Care 2000, 49, 387–391. [Google Scholar] [CrossRef]
- Singh, C.N.; Klein, M.B.; Sullivan, S.R.; Sires, B.S.; Hutter, C.M.; Rice, K.; Jian-Amadi, A. Orbital Compartment Syndrome in Burn Patients. Ophthalmic Plast. Reconstr. Surg. 2008, 24, 102–106. [Google Scholar] [CrossRef]
- Hundeshagen, G.; Lee, J.O.; Norbury, W.B.; Herndon, D.N. Care of Geriatric Patients. In Total Burn Care, 5th ed.; Hernon, D., Ed.; Elsevier: Amsterdam, The Netherlands, 2018; pp. 381–385. [Google Scholar]
- Abu-Sittah, G.; Chahine, F.; Janom, H. Management of burns in the elderly. Ann. Burn. Fire Disasters 2016, 29, 249. [Google Scholar]
- Pereira, C.T.; Barrow, R.E.; Sterns, A.M.; Hawkins, H.K.; Kimbrough, C.W.; Jeschke, M.G.; Lee, J.O.; Sanford, A.P.; Herndon, D.N. Age-Dependent Differences in Survival after Severe Burns: A Unicentric Review of 1,674 Patients and 179 Autopsies over 15 Years. J. Am. Coll. Surg. 2006, 202, 536–548. [Google Scholar] [CrossRef] [PubMed]
- Keck, M.; Lumenta, D.; Andel, H.; Kamolz, L.-P.; Frey, M. Burn treatment in the elderly. Burns 2009, 35, 1071–1079. [Google Scholar] [CrossRef]
- Rehou, S.; Shahrokhi, S.; Thai, J.; Stanojcic, M.; Jeschke, M.G. Acute Phase Response in Critically Ill Elderly Burn Patients. Crit. Care Med. 2019, 47, 201–209. [Google Scholar] [CrossRef]
- Romanowski, K.; Curtis, E.; Barsun, A.; Palmieri, T.; Greenhalgh, D.; Sen, S. The frailty tipping point: Determining which patients are targets for intervention in a burn population. Burns 2019, 45, 1051–1056. [Google Scholar] [CrossRef] [PubMed]
- Purdue, G.F.; Hunt, J.L.; Lang, E.D. Obesity: A Risk Factor in the Burn Patient. J. Burn. Care Rehabil. 1990, 11, 32–34. [Google Scholar] [CrossRef] [PubMed]
- Gottschlich, M.M.; Mayes, T.; Khoury, J.C.; Warden, G.D. Significance of obesity on nutritional, immunologic, hormonal, and clinical outcome parameters in burns. J. Am. Diet. Assoc. 1993, 93, 1261–1268. [Google Scholar] [CrossRef]
- Sheridan, R.L.; Rue, L.W.; McManus, W.F.; Pruitt, B.A. Burns in morbidly obese patients. J. Trauma Inj. Infect. Crit. Care 1992, 33, 818–820. [Google Scholar] [CrossRef]
- Ghanem, A.M.; Sen, S.; Philp, B.; Dziewulski, P.; Shelley, O. Body Mass Index (BMI) and mortality in patients with severe burns: Is there a “tilt point” at which obesity influences outcome? Burns 2011, 37, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, A.M.; Hollett, L.P.; Jeng, J.C.; Wu, J.; Turner, D.G.; Jordan, M.H. How Long a Shadow Does Epidemic Obesity Cast in the Burn Unit? A Dietitian’s Analysis of the Strengths and Weaknesses of the Available Data in the National Burn Repository. J. Burn Care Res. 2008, 29, 97–101. [Google Scholar] [CrossRef]
- Liodaki, E.; Senyaman, Ö.; Stollwerck, P.L.; Möllmeier, D.; Mauss, K.L.; Mailänder, P.; Stang, F. Obese patients in a burn care unit: A major challenge. Burns 2014, 40, 1738–1742. [Google Scholar] [CrossRef] [PubMed]
- Jeschke, M.G.; Finnerty, C.C.; Emdad, F.; Rivero, H.G.; Kraft, R.; Williams, F.N.; Gamelli, R.L.; Gibran, N.; Klein, M.B.; Arnoldo, B.D.; et al. Mild Obesity Is Protective After Severe Burn Injury. Ann. Surg. 2013, 258, 1119–1129. [Google Scholar] [CrossRef] [Green Version]
- Keshavarzi, A.; Kardeh, S.; Dehghankhalili, M.; Varahram, M.H.; Omidi, M.; Zardosht, M.; Mehrabani, D. Mortality and Body Mass Index in Burn Patients: Experience from a Tertiary Referral Burn Center in Southern Iran. World J. Plast. Surg. 2019, 8, 382–387. [Google Scholar]
- Yim, G.H.; Pujji, O.J.S.; Bharj, I.S.; Farrar, E.; La, J.S. The value of a bariatric specific chart to initiate resuscitation of adult bariatric burns. Burns 2019, 45, 1783–1791. [Google Scholar] [CrossRef] [PubMed]
- Neaman, K.C.; Andres, L.A.; McClure, A.M.; Burton, M.E.; Kemmeter, P.R.; Ford, R.D. A New Method for Estimation of Involved BSAs for Obese and Normal-Weight Patients with Burn Injury. J. Burn Care Res. 2011, 32, 421–428. [Google Scholar] [CrossRef]
- Clemens, M.S.; Stewart, I.J.; Sosnov, J.A.; Howard, J.T.; Belenkiy, S.M.; Sine, C.R.; Henderson, J.L.; Buel, A.R.; Batchinsky, A.I.; Cancio, L.C.; et al. Reciprocal Risk of Acute Kidney Injury and Acute Respiratory Distress Syndrome in Critically Ill Burn Patients. Crit. Care Med. 2016, 44, e915–e922. [Google Scholar] [CrossRef] [PubMed]
- Basel, A.P.; Britton, G.W.; Chung, K.K. Acute Kidney Injury in Burns. In Handbook of Critical Care Nephrology; Koyner, J.L., Topf, J., Lerma, E., Eds.; Wolters Kluwer: Alphen aan den Rijn, The Netherlands, 2021. [Google Scholar]
- Chung, K.K.; Juncos, L.A.; Wolf, S.; Mann, E.E.; Renz, E.M.; White, C.E.; Barillo, D.J.; Clark, R.A.; Jones, J.A.; Edgecombe, H.P.; et al. Continuous Renal Replacement Therapy Improves Survival in Severely Burned Military Casualties with Acute Kidney Injury. J. Trauma Inj. Infect. Crit. Care 2008, 64, S179–S187. [Google Scholar] [CrossRef] [PubMed]
- Robert, I.; Oliver, J. Burn Resuscitation and Early Management: Background, Pathophysiology, Initial Evaluation and Treatment. Medscape. 2021. Available online: https://emedicine.medscape.com/article/1277360-overview (accessed on 25 June 2021).
- Mackie, D.P.; Spoelder, E.J.; Paauw, R.J.; Knape, P.; Boer, C. Mechanical Venti-lation and Fluid Retention in Burn Patients. J. Trauma Inj. Infect. Crit. Care 2009, 67, 1233–1238. [Google Scholar] [CrossRef] [PubMed]
- Curley, G.F.; Laffey, J.G.; Zhang, H.; Slutsky, A.S. Biotrauma and Ventilator-Induced Lung Injury: Clinical Implications. Chest 2016, 150, 1109–1117. [Google Scholar] [CrossRef] [PubMed]
- McGuinness, S.K.; Wasiak, J.; Cleland, H.; Symons, J.; Hogan, L.; Hucker, T.; Mahar, P.D. A Systematic Review of Ketamine as an Analgesic Agent in Adult Burn Injuries. Pain Med. 2011, 12, 1551–1558. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, S.R.; Friedrich, J.B.; Engrav, L.H.; Round, K.A.; Heimbach, D.M.; Heckbert, S.R.; Carrougher, G.J.; Lezotte, D.C.; Wiechman, S.A.; Honari, S.; et al. Opioid creep “is real and may be the cause of” fluid creep. Burns 2004, 30, 583–590. [Google Scholar] [CrossRef]
- Wibbenmeyer, L.; Sevier, A.; Liao, J.; Williams, I.; Light, T.; Latenser, B.; Lewis, R.; Kealey, P.; Rosenquist, R. The impact of opioid ad-ministration on resuscitation volumes in thermally injured patients. J. Burn Care Res. 2010, 31, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Owens, V.F.; Palmieri, T.L.; Comroe, C.M.; Conroy, J.M.; Scavone, J.A.; Greenhalgh, D.G. Ketamine: A safe and effective agent for painful procedures in the pediatric burn patient. J. Burn Care Res. 2006, 27, 211–216. [Google Scholar] [CrossRef]
- Miller, M.; Kruit, N.; Heldreich, C.; Ware, S.; Habig, K.; Reid, C.; Burns, B. Hemodynamic Response After Rapid Sequence Induction with Ketamine in Out-of-Hospital Patients at Risk of Shock as Defined by the Shock Index. Ann. Emerg. Med. 2016, 68, 181–188.e2. [Google Scholar] [CrossRef]
- Kim, D.; Pruskowski, K.A.; Ainsworth, C.R.; Linsenbardt, H.R.; Rizzo, J.A.; Cancio, L.C. A Review of Adjunctive Therapies for Burn Injury Pain During the Opioid Crisis. J. Burn Care Res. 2019, 40, 983–995. [Google Scholar] [CrossRef]
- Blanchet, B.; Jullien, V.; Vinsonneau, C.; Tod, M. Influence of Burns on Pharmacokinetics and Pharmacodynamics of Drugs Used in the Care of Burn Patients. Clin. Pharm. 2008, 47, 635–654. [Google Scholar] [CrossRef]
- Steele, A.N.; Grimsrud, K.N.; Sen, S.; Palmieri, T.L.; Greenhalgh, D.G.; Tran, N. Gap Analysis of Pharmacokinetics and Pharmacodynamics in Burn Patients. J. Burn Care Res. 2015, 36, e194–e211. [Google Scholar] [CrossRef]
- Serghiou, M.; Niszczak, J.; Parry, I.; Richard, R. Clinical practice recommendations for positioning of the burn patient. Burns 2016, 42, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Esselman, P.C.; Thombs, B.; Magyar-Russell, G.; Fauerbach, J.A. Burn Rehabilitation. Am. J. Phys. Med. Rehabil. 2006, 85, 383–413. [Google Scholar] [CrossRef] [PubMed]
- Cambiaso-Daniel, J.; Parry, I.; Rivas, E.; Kemp-Offenberg, J.; Sen, S.; Rizzo, J.A.; Serghiou, M.A.; Kowalske, K.; Wolf, S.E.; Herndon, D.N.; et al. Strength and Cardiorespiratory Exercise Rehabilitation for Severely Burned Patients During Intensive Care Units: A Survey of Practice. J. Burn Care Res. 2018, 39, 897–901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Figure 1.
Overlapping phases of burn care.

Figure 2.
Lund–Browder Diagram used to document location of burns and to calculate %TBSA *. From Driscoll LR et al. Burn Care Clinical Practice Guideline. Available online: https://jts.amedd.army.mil/index.cfm/PI_CPGs/cpgs (accessed on 25 June 2021).
Figure 2.
Lund–Browder Diagram used to document location of burns and to calculate %TBSA *. From Driscoll LR et al. Burn Care Clinical Practice Guideline. Available online: https://jts.amedd.army.mil/index.cfm/PI_CPGs/cpgs (accessed on 25 June 2021).

Figure 3.
Using the Rule of 10 to calculate initial fluid rate. TBSA, total body surface area burned. LR, lactated Ringer’s solution.
Figure 3.
Using the Rule of 10 to calculate initial fluid rate. TBSA, total body surface area burned. LR, lactated Ringer’s solution.

Figure 4.
Proposed colloid protocol for failed or runaway resuscitation utilized at the US Army Institute of Surgical Research Burn Center.
Figure 4.
Proposed colloid protocol for failed or runaway resuscitation utilized at the US Army Institute of Surgical Research Burn Center.

Figure 5.
Burn Navigator, an example of BRDSS used at the US Army Burn Center.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Time course of key variables during a typical successful resuscitation.
| Scheme | Postburn Hour | Cardiac Output | SVR | Plasma Volume | Urine Output | Fluid Infusion Rate |
|---|---|---|---|---|---|---|
| 1 | 0–12 | Rapidly reaches nadir | Rapidly reaches peak | Decreases at its most rapid rate | Oliguria is common | May peak at hour 8–10 |
| 2 | 12–36 | Slightly less than normal | Decreases towards normal | Nadir at hour 12–18, then slowly increases | Adequate | Slowly decreases |
| 3 | 36-beyond | Supranormal | Subnormal | Normal | Often above target | Reaches a maintenance rate |
SVR, systemic vascular resistance. Adopted from Cancio, L.C. Initial management and resuscitation. In Essential Burn Care for Non-Burn Specialists, Lee, J., Ed.; Springer Nature: Cham, Switzerland, in press.
Table 2.
Common pitfalls of resuscitation.
| Resuscitation Pitfalls |
|---|
| Advanced age |
| Obesity |
| Existing cardiomyopathy |
| Renal failure |
| Osmotic diuresis (glycosuria, alcohol consumption) |
| Active hemorrhage |
| Inhalation injury |
| Mechanical Ventilation |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Causbie, J.M.; Sattler, L.A.; Basel, A.P.; Britton, G.W.; Cancio, L.C. State of the Art: An Update on Adult Burn Resuscitation. Eur. Burn J. 2021, 2, 152-167. https://0-doi-org.brum.beds.ac.uk/10.3390/ebj2030012
AMA Style
Causbie JM, Sattler LA, Basel AP, Britton GW, Cancio LC. State of the Art: An Update on Adult Burn Resuscitation. European Burn Journal. 2021; 2(3):152-167. https://0-doi-org.brum.beds.ac.uk/10.3390/ebj2030012
Chicago/Turabian StyleCausbie, Jacqueline M., Lauren A. Sattler, Anthony P. Basel, Garrett W. Britton, and Leopoldo C. Cancio. 2021. "State of the Art: An Update on Adult Burn Resuscitation" European Burn Journal 2, no. 3: 152-167. https://0-doi-org.brum.beds.ac.uk/10.3390/ebj2030012