
Current Practices and Beliefs Regarding Screening Patients with Burns for Acute Stress Disorder and Posttraumatic Stress Disorder: A Survey of the American Burn Association Membership

Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Some Institutions Do Not Meet the American Burn Association’s Standards for ASD/PTSD Screening
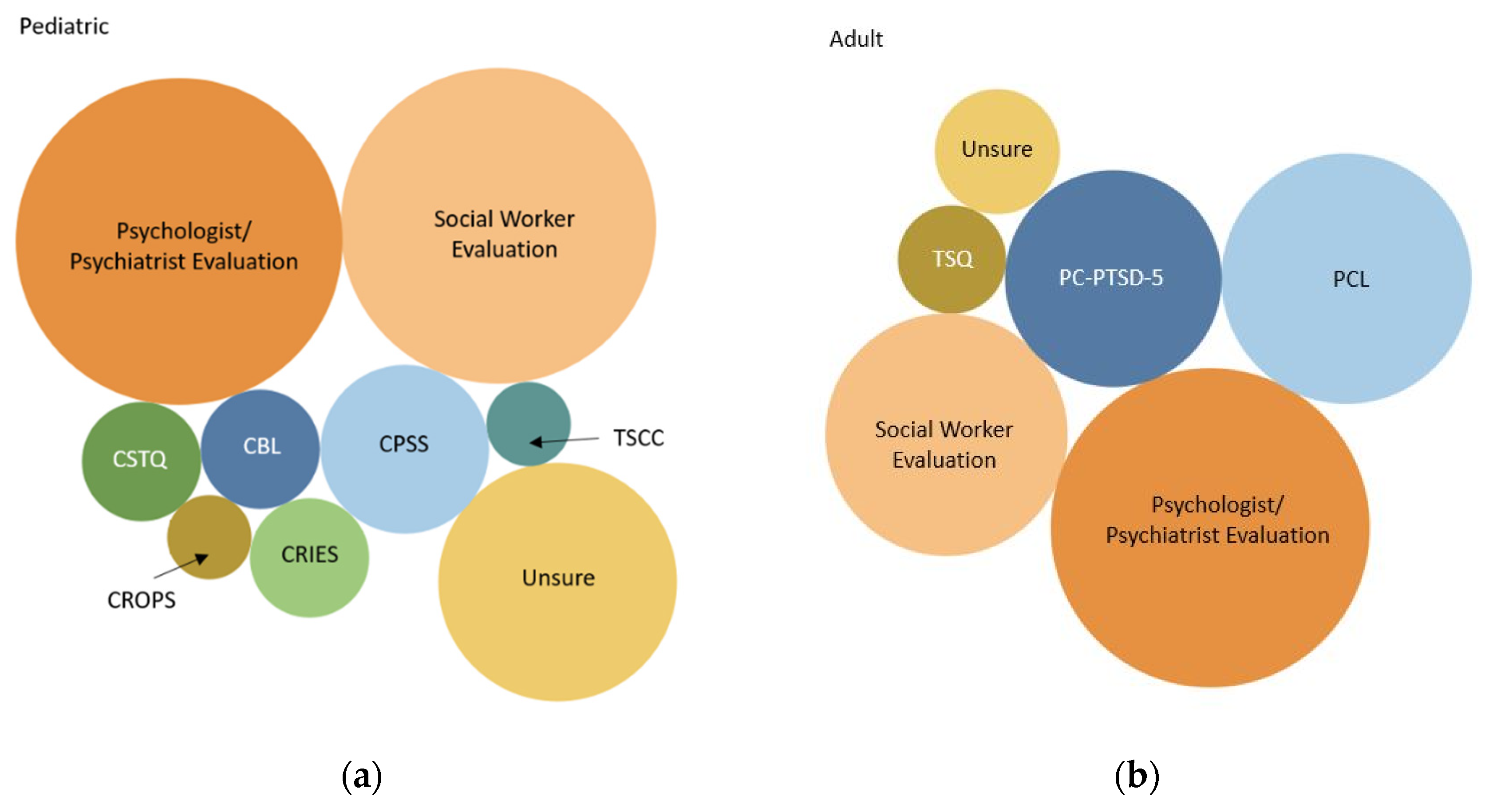
3.2. Screening Practices Vary between Institutions
3.3. Providers Who Care for Patients with Burn Injuries Support Screening for ASD/PTSD
3.4. Many Healthcare Professionals Are Uncomfortable Screening for Stress Disorders
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wolf, S.E.; Rose, J.K.; Desai, M.H.; Mileski, J.P.; Barrow, R.E.; Herndon, D.N. Mortality determinants in massive pediatric burns. An analysis of 103 children with > or = 80% TBSA burns (> or = 70% full-thickness). Ann. Surg. 1997, 225, 554–565. [Google Scholar] [CrossRef]
- Brusselaers, N.; Hoste, E.A.; Monstrey, S.; Colpaert, K.E.; De Waele, J.J.; Vandewoude, K.H.; Blot, S.I. Outcome and changes over time in survival following severe burns from 1985 to 2004. Intensive Care Med. 2005, 31, 1648–1653. [Google Scholar] [CrossRef]
- Ryan, C.M.; Schoenfeld, D.A.; Thorpe, W.P.; Sheridan, R.L.; Cassem, E.H.; Tompkins, R.G. Objective estimates of the probability of death from burn injuries. N. Engl. J. Med. 1998, 338, 362–366. [Google Scholar] [CrossRef]
- Gerber, L.H.; Bush, H.; Holavanahalli, R.; Esselman, P.; Schneider, J.; Heinemann, A.; Garfinkel, S.; Cai, C. A scoping review of burn rehabilitation publications incorporating functional outcomes. Burns 2019, 45, 1005–1013. [Google Scholar] [CrossRef] [PubMed]
- Ohrtman, E.A.; Shapiro, G.D.; Simko, L.C.; Dore, E.; Slavin, M.D.; Saret, C.; Amaya, F.; Lomelin-Gascon, J.; Ni, P.; Acton, A.; et al. Social Interactions and Social Activities After Burn Injury: A Life Impact Burn Recovery Evaluation (LIBRE) Study. J. Burn Care Res. 2018, 39, 1022–1028. [Google Scholar] [CrossRef] [PubMed]
- Brady, K.J.S.; Grant, G.G.; Stoddard, F.J.; Meyer, W.J.; Romanowski, K.S.; Chang, P.H.; Painting, L.E.; Fowler, L.A.; Nelson, J.K.; Rivas, P.; et al. Measuring the Impact of Burn Injury on the Parent-Reported Health Outcomes of Children 1 to 5 Years: A Conceptual Framework for Development of the Preschool Life Impact Burn Recovery Evaluation Profile CAT. J. Burn Care Res. 2020, 41, 84–94. [Google Scholar] [CrossRef] [PubMed]
- Davydow, D.S.; Katon, W.J.; Zatzick, D.F. Psychiatric morbidity and functional impairments in survivors of burns, traumatic injuries, and ICU stays for other critical illnesses: A review of the literature. Int. Rev. Psychiatry 2009, 21, 531–538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Baar, M.E.; Essink-Bot, M.L.; Oen, I.M.; Dokter, J.; Boxma, H.; van Beeck, E.F. Functional outcome after burns: A review. Burns 2006, 32, 1–9. [Google Scholar] [CrossRef]
- Spronk, I.; Legemate, C.; Oen, I.; van Loey, N.; Polinder, S.; van Baar, M. Health related quality of life in adults after burn injuries: A systematic review. PLoS ONE 2018, 13, e0197507. [Google Scholar] [CrossRef] [Green Version]
- Cakir, U.; Terzi, R.; Abaci, F.; Aker, T. The prevalence of post-traumatic stress disorder in patients with burn injuries, and their quality of life. Int. J. Psychiatry Clin. Pract. 2015, 19, 56–59. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Giannoni-Pastor, A.; Eiroa-Orosa, F.J.; Fidel Kinori, S.G.; Arguello, J.M.; Casas, M. Prevalence and Predictors of Posttraumatic Stress Symptomatology Among Burn Survivors: A Systematic Review and Meta-Analysis. J. Burn Care Res. 2016, 37, e79–e89. [Google Scholar] [CrossRef]
- McKibben, J.B.; Bresnick, M.G.; Wiechman Askay, S.A.; Fauerbach, J.A. Acute stress disorder and posttraumatic stress disorder: A prospective study of prevalence, course, and predictors in a sample with major burn injuries. J. Burn Care Res. 2008, 29, 22–35. [Google Scholar] [CrossRef]
- Zheng, H.; Wu, K.; Zhou, Y.; Fu, L.; Zhang, D.; Liu, Z. Prevalence and associated factors of post-traumatic stress disorder in burned patients and their family members. Burns 2020, 47, 1102–1109. [Google Scholar] [CrossRef]
- Oaie, E.; Piepenstock, E.; Williams, L. Risk factors for peri-traumatic distress and appearance concerns in burn-injured inpatients identified by a screening tool. Scars Burn. Heal. 2018, 4, 2059513118765294. [Google Scholar] [CrossRef] [Green Version]
- Gibran, N.; Wiechman, S.; Meyer, W. Summary of the 2012 ABA Burn Quality Consensus Conference. J. Burn. Care Res. 2013, 34, 361–385. [Google Scholar] [CrossRef] [PubMed]
- Gehlbach, H.; Artino, A.R., Jr. The Survey Checklist (Manifesto). Acad. Med. 2018, 93, 360–366. [Google Scholar] [CrossRef] [PubMed]
- Dillman, D.A.; Smyth, J.D.; Christian, L.M. Internet, Phone, Mail, and Mixed-Mode Surveys: The Tailored Design Method. John Wiley & Sons, Incorporated, 2014. ProQuest Ebook Central. Available online: https://0-ebookcentral-proquest-com.brum.beds.ac.uk/lib/washington/detail.action?docID=1762797 (accessed on 13 December 2020).
- Crowe, C.; Collie, C.; Johnson, C.; Wiltsey Stirman, S. An intervention mapping process to increase evidence-based psychotherapy within a complex healthcare system. Am. Psychol. 2020, 75, 1116–1129. [Google Scholar] [CrossRef] [PubMed]
- Malt, U.F.; Ugland, O.M. A long-term psychosocial follow-up study of burned adults. Acta Psychiatr. Scand Suppl. 1989, 355, 94–102. [Google Scholar] [CrossRef] [PubMed]
- Boersma-van Dam, E.; van de Schoot, R.; Hofland, H.W.C.; Engelhard, I.M.; Van Loey, N.E.E. Individual recovery of health-related quality of life during 18 months post-burn using a retrospective pre-burn measurement: An exploratory study. Qual. Life Res. 2021, 30, 737–749. [Google Scholar] [CrossRef]
- Rennick, J.E.; Johnston, C.C.; Dougherty, G.; Platt, R.; Ritchie, J.A. Children’s psychological responses after critical illness and exposure to invasive technology. J. Dev. Behav. Pediatr. 2002, 23, 133–144. [Google Scholar] [CrossRef]
- Xi, M.M.; Lei, F.; Xie, W.G. Advances in the research of psychological rehabilitation of pediatric burn patients. Zhonghua Shao Shang Za Zhi 2020, 36, 519–522. (In Chinese) [Google Scholar] [PubMed]
- Visser, E.; Gosens, T.; Den Oudsten, B.L.; De Vries, J. The course, prediction, and treatment of acute and posttraumatic stress in trauma patients: A systematic review. J. Trauma Acute Care Surg. 2017, 82, 1158–1183. [Google Scholar] [CrossRef] [PubMed]
- Daviss, W.B. The Child Trauma Screening Questionnaire predicts PTSD onset 6 months after traumatic accident better than the Children’s Impact of Events Scale. Evid. Based Ment. Health 2007, 10, 44. [Google Scholar] [CrossRef]
- van Meijel, E.P.; Gigengack, M.R.; Verlinden, E.; Opmeer, B.C.; Heij, H.A.; Goslings, J.C.; Bloemers, F.W.; Luitse, J.S.; Boer, F.; Grootenhuis, M.A.; et al. Predicting posttraumatic stress disorder in children and parents following accidental child injury: Evaluation of the Screening Tool for Early Predictors of Posttraumatic Stress Disorder (STEPP). BMC Psychiatry 2015, 15, 113. [Google Scholar] [CrossRef] [Green Version]
- Foa, E.B.; Steketee, G.; Olasov Rothbaum, B. Behavioral/cognitive conceptualizations of post-traumatic stress disorder. Behav. Ther. 1989, 20, 155–176. [Google Scholar] [CrossRef]
- Stein, M.B. Psychotherapy and Psychosocial Interventions for Posttraumatic Stress Disorder in Adults. 2021. Available online: https://www.uptodate.com/contents/psychotherapy-and-psychosocial-interventions-for-posttraumatic-stress-disorder-in-adults (accessed on 27 September 2021).
- Harris, M.; Fallot, R.D. Envisioning a trauma-informed service system: A vital paradigm shift. New Dir. Ment. Health Serv. 2001, 89, 3–22. [Google Scholar] [CrossRef] [PubMed]
- Oral, R.; Ramirez, M.; Coohey, C.; Nakada, S.; Walz, A.; Kuntz, A.; Benoit, J.; Peek-Asa, C. Adverse childhood experiences and trauma informed care: The future of health care. Pediatr. Res. 2016, 79, 227–233. [Google Scholar] [CrossRef]
- O’Brien, K.H.; Lushin, V. Examining the Impact of Psychological Factors on Hospital Length of Stay for Burn Survivors: A Systematic Review. J. Burn Care Res. 2019, 40, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Kazis, L.E.; Marino, M.; Ni, P.; Soley Bori, M.; Amaya, F.; Dore, E.; Ryan, C.M.; Schneider, J.C.; Shie, V.; Acton, A.; et al. Development of the life impact burn recovery evaluation (LIBRE) profile: Assessing burn survivors’ social participation. Qual. Life Res. 2017, 26, 2851–2866. [Google Scholar] [CrossRef] [PubMed]
- Richard, R.; Baryza, M.J.; Carr, J.A.; Dewey, W.S.; Dougherty, M.E.; Forbes-Duchart, L.; Franzen, B.J.; Healey, T.; Lester, M.E.; Li, S.K.; et al. Burn rehabilitation and research: Proceedings of a consensus summit. J. Burn Care Res. 2009, 30, 543–573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moss, K.M.; Ziviani, J.; Newcombe, P.; Cobham, V.E.; McCutcheon, H.; Montague, G.; Kenardy, J. Pathways to increasing the use of psychosocial care with hospitalized children. Psychol. Serv. 2019, 16, 29–37. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Screened for ASD/PTSD N = 48 | Did Not Screen for ASD/PTSD N = 32 | Unsure If Institution Screened N = 11 | |
|---|---|---|---|
| Profession, n | |||
| Surgeon | 11 | 10 | 3 |
| Physician (non-surgeon) | 1 | 1 | 0 |
| APP 1 | 8 | 3 | 1 |
| Nurse | 13 | 8 | 2 |
| Psychologist/CLS 2/SW 3 | 5 | 4 | 0 |
| PT/OT | 3 | 4 | 4 |
| Other | 7 | 2 | 1 |
| Medical Director 4, n | 5 | 5 | 1 |
| Years of Experience, n | |||
| 0–5 years | 9 | 7 | 3 |
| 6–10 years | 13 | 8 | 3 |
| 11–15 years | 9 | 2 | 2 |
| >15 years | 17 | 14 | 2 |
| Adult | Pediatric | |
|---|---|---|
| N = 47 | N = 30 | |
| Which population does your institution screen?, n | ||
| All patients with a burn | 33 | 14 |
| Only patients admitted to the intensive care unit | 2 | 1 |
| Only patients admitted to the hospital | 11 | 7 |
| Only patients with a burn over a certain TBSA cut-off | 0 | 0 |
| Only patients with injury severity score cut-off | 1 | 1 |
| Only patients with a certain type of burn injury mechanism | 0 | 0 |
| I am unsure | 0 | 6 |
| Who performs the screening at your institution?, n | ||
| Attending Surgeon | 6 | 1 |
| Surgical Trainee | 2 | 1 |
| Advance Practice Provider | 15 | 5 |
| Nurse | 22 | 10 |
| Social Worker | 17 | 13 |
| Child Life Specialist | NA | 9 |
| Psychologist | 26 | 16 |
| Another Medical Team | 1 | 2 |
| I am unsure | 0 | 2 |
| Once a patient screens positive for stress disorder symptoms, what is the next step at your institution?, n | ||
| Continue to monitor and repeat screening | 23 | 12 |
| Treat with Trauma-Informed Care | 18 | 11 |
| Referral for inpatient therapies (recreation, music, pet, etc.) | 14 | 16 |
| Referral for inpatient Psychology/Psychiatry | 34 | 21 |
| Referral for outpatient Psychology/Psychiatry | 34 | 22 |
| Initiation of beta-blockers | 6 | 1 |
| Initiation of selective serotonin reuptake inhibitors | 15 | 3 |
| Initiation of other anti-depressants | 10 | 0 |
| Initiation of anti-psychotics | 5 | 0 |
| I am unsure | 1 | 3 |
| Surgeons | Medical Directors | Psychologists/ CLS 1/SW 2 | Other HCP 3 | |
|---|---|---|---|---|
| Should screening be standard of care? (%) | ||||
| Yes | 75 | 73 | 100 | 88 |
| No | 12.5 | 18 | 0 | 0 |
| Unsure | 12.5 | 9 | 0 | 12 |
| How much personal responsibility do you feel for screening? (%) | ||||
| Very Little | 0 | 0 | 0 | 2 |
| Little | 8 | 9 | 0 | 4 |
| Neutral | 8 | 0 | 0 | 22 |
| Some | 38 | 28 | 22 | 33 |
| A Lot | 46 | 64 | 78 | 39 |
| Prefer to not reply | 0 | 0 | 0 | 0 |
| Who do you believe should have the primary responsibility for screening? (%) | ||||
| Attending Surgeon | 50 | 55 | 0 | 31 |
| Surgical Trainee | 21 | 18 | 0 | 8 |
| Advanced Practice Provider | 46 | 64 | 11 | 29 |
| Nurse | 42 | 55 | 11 | 47 |
| Social Worker | 46 | 55 | 56 | 63 |
| Child Life Specialist | 42 | 28 | 22 | 45 |
| Psychologist/Psychiatrist | 71 | 64 | 44 | 63 |
| Another Physician Service | 8 | 9 | 0 | 8 |
| Primary Care Physician | 8 | 9 | 0 | 12 |
| Unsure | 4 | 0 | 11 | 6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smith, M.B.; Wiechman, S.A.; Mandell, S.P.; Gibran, N.S.; Vavilala, M.S.; Rivara, F.P. Current Practices and Beliefs Regarding Screening Patients with Burns for Acute Stress Disorder and Posttraumatic Stress Disorder: A Survey of the American Burn Association Membership. Eur. Burn J. 2021, 2, 215-225. https://0-doi-org.brum.beds.ac.uk/10.3390/ebj2040016
Smith MB, Wiechman SA, Mandell SP, Gibran NS, Vavilala MS, Rivara FP. Current Practices and Beliefs Regarding Screening Patients with Burns for Acute Stress Disorder and Posttraumatic Stress Disorder: A Survey of the American Burn Association Membership. European Burn Journal. 2021; 2(4):215-225. https://0-doi-org.brum.beds.ac.uk/10.3390/ebj2040016
Chicago/Turabian StyleSmith, Mallory B., Shelley A. Wiechman, Samuel P. Mandell, Nicole S. Gibran, Monica S. Vavilala, and Frederick P. Rivara. 2021. "Current Practices and Beliefs Regarding Screening Patients with Burns for Acute Stress Disorder and Posttraumatic Stress Disorder: A Survey of the American Burn Association Membership" European Burn Journal 2, no. 4: 215-225. https://0-doi-org.brum.beds.ac.uk/10.3390/ebj2040016