Management of Uncomplicated Type B Aortic Dissection


1
Cardiology and Aortic Centre, Royal Brompton and Harefield Hospital NHS Foundation Trust, London SW3 6NP, UK
2
Department of Cardiology, National Heart and Lung Institute, Faculty of Medicine, Imperial College London, London SW3 6LY, UK
3
School of Biomedical Engineering and Imaging Science, King’s College London, St Thomas’ Hospital, London SE1 7EH, UK
4
Department of Vascular Surgery, St George’s Hospital, London SW17 0QT, UK
*
Author to whom correspondence should be addressed.
Hearts 2020, 1(1), 14-24; https://0-doi-org.brum.beds.ac.uk/10.3390/hearts1010004
Submission received: 16 April 2020
/
Revised: 9 May 2020
/
Accepted: 14 May 2020
/
Published: 18 May 2020
(This article belongs to the Special Issue Thoracic Aorta)
{kind=link}
{kind=link}
{kind=link}
Abstract
:Acute aortic dissection has an incidence of approximately half that of symptomatic abdominal and thoracic aneurysm of the aorta and more than twice the mortality of population-based controls. While urgent undelayed open surgery is the strategy of choice in proximal dissection, medical management has been the mainstay of treatment for uncomplicated distal or type B aortic dissection, but endovascular intervention is now considered a potential treatment option for all type B dissection due to its success in complicated cases. Endovascular repair can be technically demanding in aortic dissection, and timing of the repair can have a significant influence on anatomical and clinical outcome. Observational reports of feasibility and reasonable safety are flanked by only two randomised trials; the Acute Dissection Stent Grafting or Best Medical Treatment (ADSORB) trial demonstrated improved remodelling in acute dissection and the INvestigation of STEnt grafts in patients with type B Aortic Dissections (INSTEAD) trial showed better long-term survival in patients treated endovascularly in the subacute phase. Meta-analyses and other large clinical studies have demonstrated mixed results. Due to some risks associated endovascular repair and the requirement of specialist aortic care (which is not always available), a pragmatic approach for current management could involve high intensity serial imaging in the acute phase of a type B aortic dissection, thereby identifying complicated cases for early intervention and selection of patients at high risk of disease progression for deferred endovascular management in the subacute phase within 90 days.
1. Introduction
Hospital-based studies suggest an incidence of acute aortic dissection of three or four cases per 100,000 patients per year, which is approximately half the incidence of symptomatic aortic aneurysm [1,2]. A 2018 epidemiological study demonstrated that patients with aortic dissection have more than twice the mortality at five, 10 and 20 years compared with population-based controls [3].
Type B aortic dissection was previously classified into acute and chronic, where acute dissection was up to 14 days since symptom onset, and chronic dissection was more than 14 days. This distinction was made before the advent of modern diagnostic imaging modalities; more recently, the International Registry of Acute Aortic Dissection (IRAD) and VIRTUE study groups have revised this classification. The IRAD group analysed the survival data in its registry and identified four separate time periods: hyperacute (0–24 h), acute (2–7 days), subacute (8–30 days) and chronic (≥30 days). In the VIRTUE study, patients were defined as having acute (14 days from symptom onset), subacute (15–92 days) or chronic (>92 days) dissection [4,5]. Computed tomography (CT) imaging is the preferred imaging modality and usually used in the investigation and management of acute type B aortic dissection, because it is widely available.
Complications in acute type B aortic dissection were defined by the expert consensus group as mal-perfusion, resulting in end-organ ischaemia (critically affecting organ or limb perfusion), persistent hypertension despite full medical therapy, periaortic haematoma with blood collection, haemorrhagic pleural effusion and aortic rupture [6]. Approximately 25% of affected patients have complications already at the time of presentation or with the onset of symptoms. For these cases with signs or evidence of early complications, interventional thoracic endovascular repair (TEVAR) has become the standard treatment of choice both in the acute and even in the chronic stage [7,8,9]. However, in the absence of these features, a type B aortic dissection is termed uncomplicated, and management of this type of acute aortic dissection is challenging and controversial in the medical community and, thus, ideally, requires a multidisciplinary team approach. As a rule, a widely agreed upon an initial adjunct medical management approach, regardless of any potential later intervention, is always essential; medical therapy is needed to control both the initial pain syndrome and any documented hypertensive state. The aim of medical therapy in the initial phase is to reduce shear stress on the dissected segment of the aorta by effectively reducing systemic blood pressure and cardiac contractility. Blood pressure control is an essential component for all patients with any acute aortic dissection regardless of location and should be maintained throughout the entire treatment and follow-up surveillance.
Intravenous beta-blocking agents such as metoprolol or labetalol are useful to both reduce heart rate and lower systolic blood pressure to 100–120 mm Hg and should be considered in the acute phase [10] and administered in absence of any contraindication. The initial intravenous phase should swiftly be followed by an oral combination therapy as beta-blocking agents, calcium blockers or vasodilating agents. In addition to medical management, further strategic endovascular interventions are established and optional in the context of aortic dissection. Especially for type B aortic dissection management, even regardless of persisting complications, thoracic endovascular aortic repair (TEVAR) has been gaining momentum, as it has been proven to exclude the false lumen from the circulation by use of a stent graft with fabric across the tear. Conceptually, the aim of endovascular repair is to stent-graft the true lumen of the dissection, inducing aortic remodelling and false lumen thrombosis; the latter is obviously a prerequisite to long-term stability of the aorta and has been shown to result in good long-term outcomes. With such observational evidence in the setting of a mal-perfusion and imminent rupture, interventional TEVAR has been accepted as the treatment of choice for such complicated type B aortic dissections (Class I, level of evidence C), even without any randomised trials. In the setting of “uncomplicated type B aortic dissection”, essentially meaning in the absence of mal-perfusion issues and imminent aortic ruptures, the management strategy may be less settled, but recent observations have indicated that, even in the setting of uncomplicated Type B dissection, pre-emptive TEVAR may be considered an endovascular treatment option with improved long-term outcomes (Class IIA, level of evidence B) [10].
The following sections provide information and an evaluation of the current treatment options for so-called uncomplicated type B aortic dissection based on the currently available database. All reported data are exclusively from human studies with a formal ethics committee approval (according to requirements in participating respective countries).
2. Optimal Medical Treatment (OMT)
At least initial medical management is currently the mainstay of treatment for uncomplicated type B aortic dissection and usually consists of a combination of beta-blockers, medications to inhibit the renin-angiotensin system or calcium channel blockers. In IRAD, 89% of patients with type B aortic dissection were treated with beta-blockers, 47% with angiotensin-converting enzyme inhibitors, 50% with calcium channel blockers, 29% with diuretics and 22% with other vasodilators. In practice, the specific regimen prescribed is usually determined by a combination of personal experience, expert opinion and the results of historic observational studies. Beta-blockers are commonly used to reduce both the aortic pulse pressure and heart rate, as the American College of Cardiology guidelines recommend a target heart rate of 60 beats per minute to achieve the best survival rates [11]. Such recommendations, however, are not necessarily based on strong evidence but, rather, on expert recommendation and previous experience; with the advent of registry data more recently, it became transparent that the in-hospital outcome in the first 30 days after onset of type B aortic dissection under medical management was not that great, with approximately 12% of patients who were receiving the best medical therapy developing significant complications, such as mal-perfusion, aortic rupture and early expansion. The so-called intervention-free survival rate of those patients managed conservatively was just 41% at six years [12]. Survival analyses demonstrate that approximately one-quarter of patients are dead at three years, and by five years, up to 50% of patients are dead in some series [13,14,15].
The importance of good blood pressure control cannot be overestimated as the major component of conservative management; from trials such as the INvestigation of STEnt grafts in patients with type B Aortic Dissections (INSTEAD) and Acute Dissection Stent Grafting or Best Medical Treatment (ADSORB), we have learned that the majority of patients required at least three different antihypertensive medications to achieve a satisfactory blood pressure control [16]. Moreover, a recent observational study performed outside of a trial setting demonstrated that the majority of patients adhere poorly to a combination antihypertensive therapy [17]. Guidelines from the American College of Cardiology and the European Society of Cardiology suggest further studies should be undertaken to refine the therapeutic approaches required for early medical management in patients with type B aortic dissection [8,11].
3. Thoracic Endovascular Aortic Repair (TEVAR)
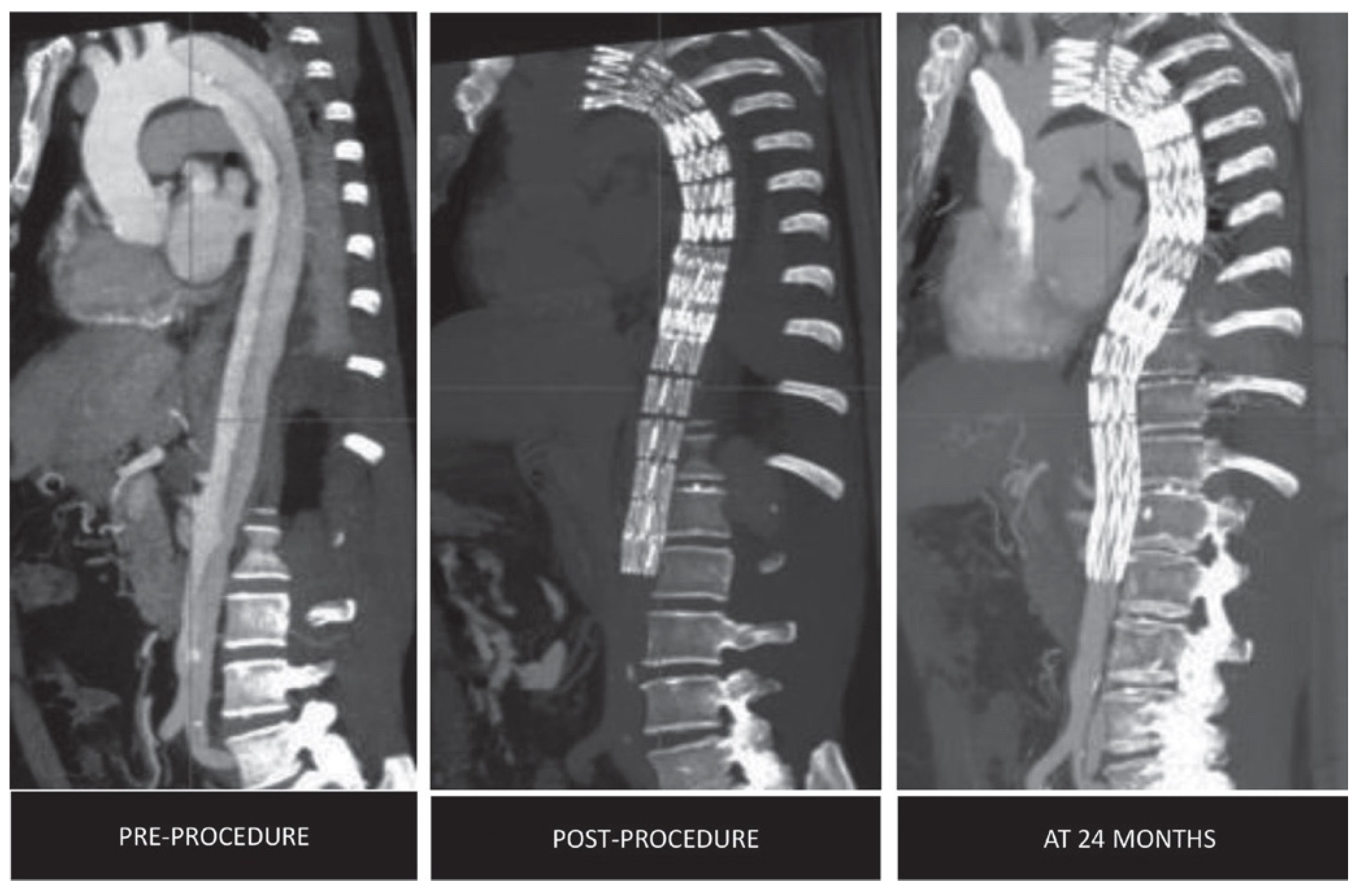
For type B aortic dissection, the endovascular revolution began with the pioneering early work of Nienaber et al. [18] and Dake et al. [10]. Almost two decades later, the expertise of physicians and the evolution of these devices have extended the indications of this interventional strategy in a broader spectrum of patients with aortic dissection. Clearly, today, the use of endovascular treatment to manage the complications of acute aortic dissection, such as rupture and mal-perfusion, is well-established, despite the lack of randomised level 1 data [1,2,3] The global interest in the endovascular concept to manage aortic dissection has helped to establish the notion that stent grafts, when properly and timely placed, help to induce aortic remodelling by expanding the true lumen, by sealing big entry tears to the false lumen and thereby inducing false lumen thrombosis and remodelling long-term (Figure 1).
Recent observational studies have concluded that thrombosis of the false lumen and subsequent thrombosis and remodelling of dissected aorta is likely associated with improved survival [17,18,19]. By all means, endovascular repair of type B aortic dissection can be technically challenging and may require not only suitable anatomic features but also state-of-the-art imaging and safe vascular access; there may also be difficulty navigating and tracking the device through the dissected aorta and finding a good proximal landing zone of 20 mm in a healthy parallel-walled aorta. In the early phase of an institutional learning curve, TEVAR procedures tend to be associated with some risks, such as retrograde type A aortic dissection and distal stent graft-induced new entry tears, problems that will be overcome with better skills and experience and improved devices. Nevertheless, a recent systematic meta-analysis has shown that endovascular repair is associated with substantially lower early mortality, stroke and spinal cord ischaemia rates and lower incidences of respiratory complications compared to open surgical repairs [20].
Endovascular treatment in different phases of the disease (acute, subacute or chronic) has been associated with different patient outcomes, as demonstrated in the VIRTUE study. In all three groups compared in VIRTUE, the true lumen of the dissection significantly expanded after interventional endovascular repair and continued to expand over time, with the majority of remodelling complete by three months. Patients treated in the subacute phase showed aortic remodelling that was analogous to the acute group without any incidence of retrograde type A aortic dissection; this occurred in one patient in the acute group. The amount of false lumen area reduction was significantly greater in the acute and subacute groups compared with the chronic group; this observation forms essentially the basis for the concept of a three-month window of plasticity of the dissected aorta to successfully remodel with TEVAR during this window of opportunity. There was no difference in the amount of false lumen thrombosis between the acute and subacute groups in the thorax, but in the abdomen segment, there was significantly less thrombosis in the chronic group, which also presented with a higher rate of reinterventions. This temporal variation in outcomes was also found in a 2018 analysis of the Japan Adult Cardiovascular Surgery database. Operative mortality and severe complications were significantly more common in patients treated within 24 h of dissection compared with those treated in the acute (1–14 days) and subacute (2–6 weeks) phases [21].
Due to the survival advantages seen with thoracic endovascular repair in complicated cases, attention within the vascular community has turned to the use of this technology in uncomplicated cases as a pre-emptive measure to avoid later problems, such as aneurysmal degeneration, which is a difficult long-term scenario to treat. Notably optimal medical treatment alone has been shown to be associated with a considerable risk of disease progression to complicated dissection later on during follow-up or aneurysmal degeneration of the affected aortic segment, which is the most feared long-term complication, with an unknown rupture risk affecting about 30%–40% of patients [22,23].
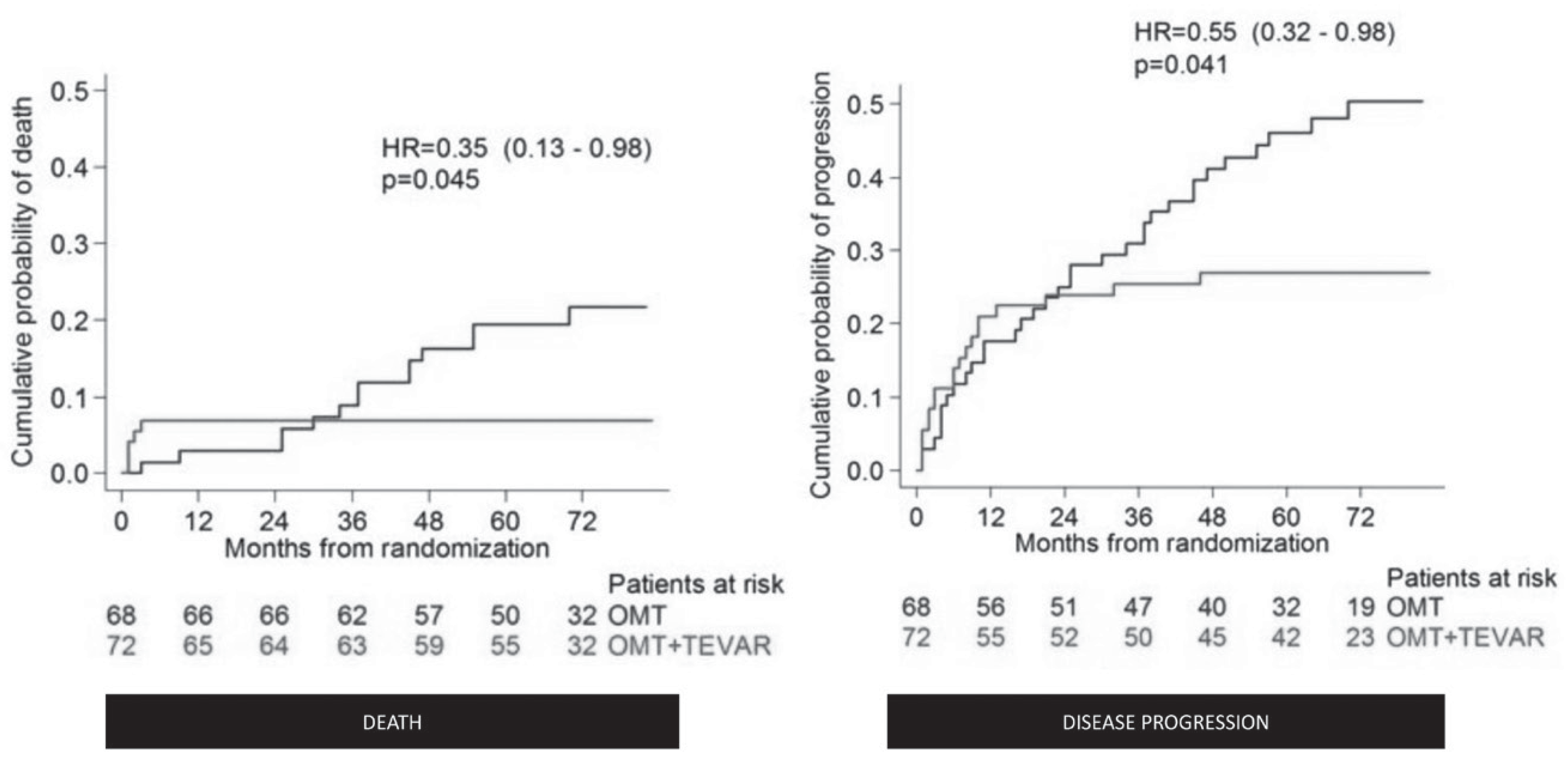
Two randomised controlled trials have been conducted to determine whether endovascular repair combined with optimal medical treatment for uncomplicated type B aortic dissection would give benefit over optimal medical treatment alone. In the INSTEAD trial, the majority of patients were treated in the subacute phase (which means within 90 days of onset); while the two-year follow-up data failed to show a significant advantage in outcomes compared to medical management only, the longer-term outcomes after five years demonstrated both better aortic remodelling and late survival in patients receiving endovascular repair in the initial setting of uncomplicated type B aortic dissection (Figure 2) [23]. However, there were eight deaths in the endovascular repair group, four of which were aortic-related, but none beyond two years of follow-up.
In the randomised ADSORB trial, patients were treated within 14 days of dissection onset, and the data showed a benefit of endovascular repair in terms of aortic remodelling at one year, as derived from CT imaging. There were no deaths within 30 days, and one death in the endovascular repair group during follow-up from cardiac arrest; no autopsy was performed, but the death was not reported as dissection-related. The primary endpoints in ADSORB were incomplete false lumen thrombosis, aortic dilatation and aortic rupture. Analysis of this composite endpoint revealed that incomplete thrombosis, aortic dilation or rupture occurred significantly more frequently in the group receiving medical treatment only (100% vs. 50%; p < 0.001) [16]. However, both the INSTEAD and ADSORB trials failed to generate enough statistical power required for a true outcome analysis.
A meta-analysis of studies evaluating endovascular treatment with adjunct optimal medical treatment vs. optimal medical treatment alone demonstrated no difference in short, intermediate and mid-term mortality but showed that TEVAR was associated with a lower likelihood of aortic rupture at one year [24]. A multi-institutional retrospective study with a cohort of more than 300 patients showed that optimal medical treatment with endovascular repair results in significantly fewer all-cause and aortic-related deaths compared to optimal medical treatment alone, with higher early mortality in the optimal medical treatment group compared with the optimal medical treatment plus TEVAR group [25]. On aggregate, lower morbidity and mortality rates long-term after endovascular procedures have finally generated scientific evidence in favour of TEVAR in uncomplicated type B aortic dissection as a pre-emptive measure in suitable patients.
This recognition was recently shared by another meta-analysis supporting the notion of a risk reduction of both late all-cause and aortic-related mortality and late aortic-related adverse events with TEVAR compared with optimal medical treatment alone but, on the downside, an increased early risk of stroke [26]. Thus, as not all patients with uncomplicated type B aortic dissection treated medically will die of aortic-related causes, we need a better strategy to offer customised endovascular management for those that eventually benefit from it and avoid exposure to the risks associated with TEVAR for those candidates who will not benefit. Such a selection algorithm will probably incur variables ranging from anatomic features, over age and comorbidities, to features closely related to experience and volume of a given aortic centre.
4. Selection of Patients for Endovascular Intervention
Uncomplicated type B aortic dissections are traditionally treated with medical management alone, at least in the initial phase, with a focus on strict blood pressure control. However, with medical treatment alone, the morbidity, including aneurysm degeneration of the affected segment, is 30%, and mortality is 10% over five years [27,28,29]. Recent studies suggest that a subset of patients with uncomplicated type B aortic dissection but features of high risk may benefit from thoracic endovascular aortic repair.
The first randomised trial of elective TEVAR in patients with chronic uncomplicated TBAD, the INvestigation of STEnt grafts in patients with type B Aortic Dissections (INSTEAD) trial, did not demonstrate a significant difference in the two-year survival between optimal medical treatment and endovascular repair [30,31]. However, the INSTEAD–XL trial, which is essentially a five-year follow-up study of surviving patients in INSTEAD, showed that stent-graft treatment can improve aortic-specific survival at five years; thus, pre-emptive TEVAR should be considered in these patients to improve late outcomes. This trial also showed that endovascular repair is still associated with complications, such as stroke and paraplegia, and that aortic events continue to occur even after endovascular treatment [32]. The ADSORB trial was the first randomised trial on acute dissection and compares optimal medical treatment with OMT plus thoracic stent grafting of the primary entry tear in patients with acute uncomplicated type B aortic dissection. The study showed that uncomplicated aortic dissection can be safely treated with the stent grafts. Remodelling with thrombosis of the false lumen and reduction of its diameter is induced by the stent graft, but long-term results are still needed [16]. A recent imaging focused analysis of the ADSORB trial patients helped to identify which patients with uncomplicated type B aortic dissection are likely at higher risk for aortic events and should therefore receive TEVAR or be monitored closely during follow-up. The analysis identified the number of vessels originating from the false lumen as an independent predictor of false lumen growth in initially uncomplicated type B aortic dissection patients. Finally, increasing age was a negative predictor of aortic growth [33].
Besides some guidance from those two randomised trials, the vascular community has tried to identify additional features that may identify patients with acute so-called uncomplicated type B aortic dissection that are at high risk of aneurysm formation, extension of the dissection and subsequent rupture; if the risk of disease progression was known, then this could be balanced against the relatively small risks of TEVAR.
Recently, the UTHealth team from Houston, Texas studied the predictors of intervention and mortality in patients with uncomplicated type B aortic dissection. According to their findings, a total aortic diameter > 44 mm is considered a predictor of mortality after adjustment for other significant risk factors. Age > 60 years on admission is also a predictor of mortality. A false lumen diameter > 22 mm, as well as those with maximum aortic diameter > 44 mm on admission, were associated with decreased intervention-free survival, as an increased diameter of the patent false lumen has been demonstrated to be a significant, independent predictor of rupture and aneurysmal degeneration. It is highly likely that patients with these high-risk criteria may benefit from thoracic endovascular aortic repair, as long as the procedure itself is performed at low risk [34]. Another high-risk characteristic that has been reported as an independent predictor of mortality in uncomplicated type B aortic dissection is the partial thrombosis of the false lumen; patients with incomplete false lumen thrombosis or with patent false lumen have worse outcomes (compared to patients with complete false lumen thrombosis of their dissection), because they are threatened by the further expansion of total aortic dimension and possible rupture; in a recent analysis from IRAD, the risk of death in the patients with partial thrombosis was almost three times higher in comparison with the patients with a thrombosed false lumen [35]. A recent large meta-analysis has shown that aortic growth rate among patients with uncomplicated type B aortic dissection with a partially thrombosed false lumen appears to be higher during follow-up compared to patients with complete thrombosis or a patent false lumen. These patients may require more intensive follow-up imaging and timely prophylactic aortic interventions [12].
Increasing aortic diameter and a large single-entry tear are considered important risk factors for dissection and rupture. Prophylactic descending thoracic aortic repair is generally recommended for a descending thoracic aortic diameter of 5.5 cm or 6 cm [36]. However, recently, a total aortic diameter greater than 44 mm and a false lumen diameter of greater than 22 mm have been used to identify patients at risk of low intervention-free survival [37]; thus, repair should be considered at an earlier stage in these patients.
Connective tissue disorders such as the Marfan syndrome and other genetic aortopathies are considered to constitute important risk features for aortic dissection, especially in young patients, and thresholds for prophylactic aortic replacement are typically lower for these specific patient groups [14]. Due to the nature of the tissue disorder, interventional endovascular strategies are usually not considered a first-line therapy but may be necessary in an emergency setting. With growing experience and skills, endovascular interventions are likely to be used in the setting of type B dissection in the context of genetic aortopathies but probably preferentially in emergency settings rather than in uncomplicated type B dissection.
Evaluation of the data collected during the ADSORB study demonstrated using multivariate regression modelling, where the number of vessels originating from the false lumen is an independent predictor of false lumen growth (odds ratio: 22.1) [33]. Other studies have shown that partial false lumen thrombosis, a total aortic diameter greater than 4 cm, a large proximal entry tear and presence of the entry tear on the aortic concavity are associated with worse outcomes [38]. IRAD demonstrated that lower rates of aortic expansion are related to Caucasian race, an initial aortic diameter less than 4 cm, female sex, the presence of intramural haematoma and the use of calcium channel blockers [39]. Other studies from the same group identified age ≥70 years, a prior history of aortic aneurysm, atherosclerosis, renal failure, pleural effusion and in-hospital hypotension as independent predictors of mortality during follow-up [22].
In order to detect complications early in patients who present with initially uncomplicated acute type B aortic dissection, some experts now advocate high-intensity serial CT imaging in the first 14 days and, then, after three months, with as many as four CT angiograms during this time. If evidence of the development of complications is seen, such as rapid expansion of the aorta, extension of the dissection or end-organ ischaemia, then patients are put forward for endovascular repair, which is performed electively between two and 12 weeks after symptom onset in the optimal window of plasticity.
In a 2016 survey, 37% of respondents have performed TEVAR in uncomplicated type B aortic dissection based on certain morphological criteria, while 8% performed the procedure routinely for uncomplicated cases based on the expected progressive nature of type B aortic dissection [40]. The current European guidelines recommend TEVAR as the treatment of choice for complicated type B aortic dissection (class I, level of evidence C) and as a treatment that can be considered to prevent future aortic complications in uncomplicated acute type B aortic dissection (class IIA, level of evidence B) [9]. A multidisciplinary discussion would be recommended before proceeding with any invasive surgery or intervention.
5. Conclusions
Patients with aortic dissection have more than twice the mortality of population-based matched controls. Management of the condition is challenging and requires a multidisciplinary team approach. Optimal medical treatment is the mainstay of initial treatment for uncomplicated cases, but improvements in survival seen with endovascular management of complicated cases have driven interest in this treatment for uncomplicated cases in addition to medical management. Contemporary data on this approach are heterogenous but suggest there may be improved late all-cause and aortic-related mortality with TEVAR, in addition to optimal medical treatment. Close follow-up is sensible to identify those patients prone for developing complications. Again, early intervention may improve the overall long-term outcome for these patients [39]. Therefore, early detectable high-risk features for adverse events are essential to stratify patients who can be treated medically and those who will benefit from rigorous follow-up and, in the long-term, from timely prophylactic TEVAR.
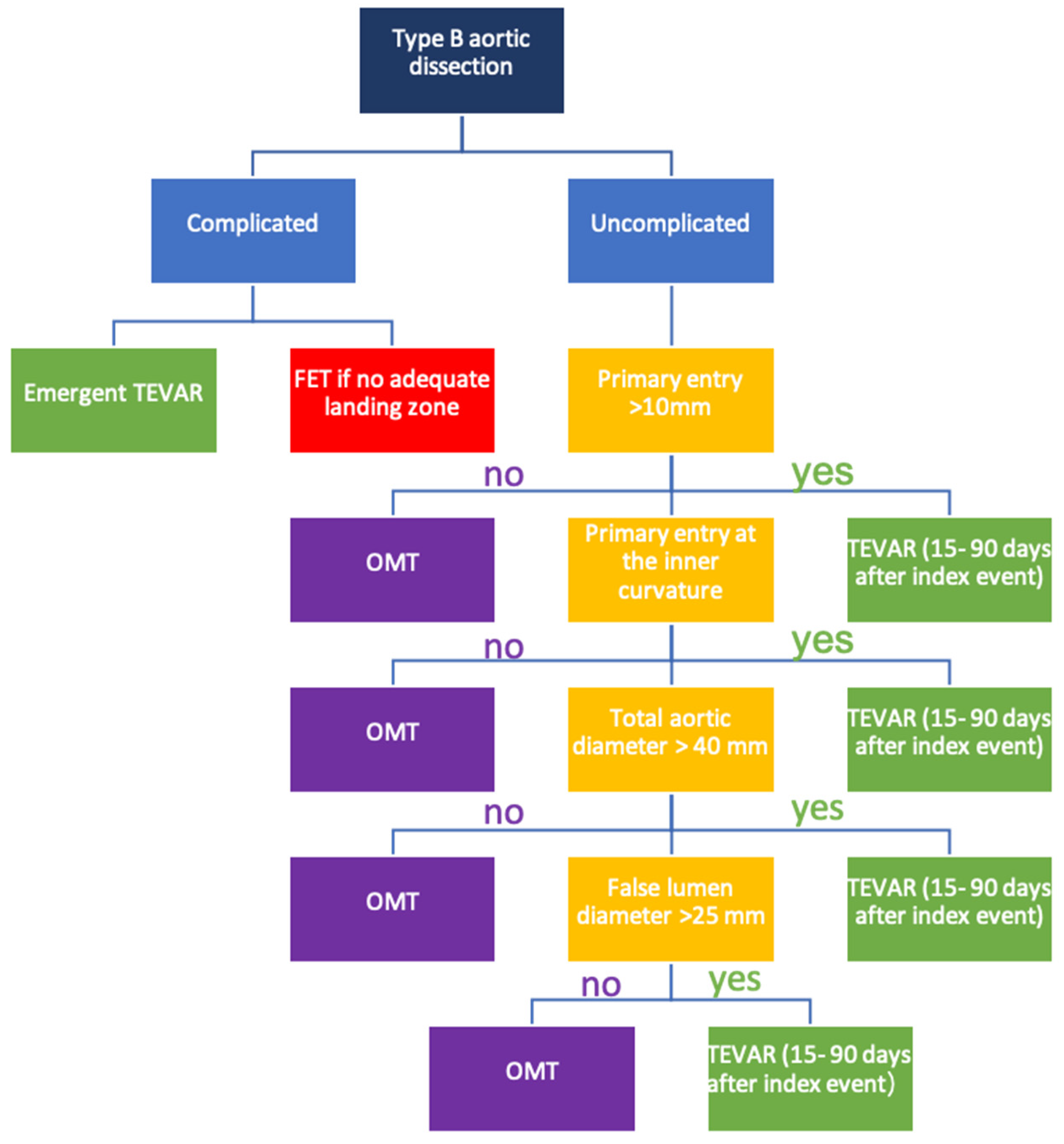
Thus, a pragmatic approach is the use of high-intensity serial imaging in the acute phase with a selection of uncomplicated patients for endovascular treatment in the subacute phase based on the presence of high-risk features (Figure 3). On aggregate, TEVAR has enriched the armamentarium to treat acute and subacute thoracic aortic dissection and has matured to a baseline strategy for many patients.
6. Outlook
The optimal treatment of patients with type B aortic dissection is challenging and requires a multidisciplinary team approach. The separation of the uncomplicated patients with type B aortic dissection to those with high-risk profiles seems reasonable. Prevention of chronic type B aortic dissection with aneurysmal degeneration and attainment of aortic remodelling with pre-emptive TEVAR are needed to free patients from the need for long-term strict control of blood pressure and periodic follow-ups involving radiological exposure and to avoid the eventual need for extensive open surgery. The results of studies like the INSTEAD-XL trial and the ADSORB trial have verified that pre-emptive TEVAR for uncomplicated type B aortic dissection improves prognosis. This is why many experts now advocate high-intensity imaging in the first 14 days to detect the development of complications early in the disease with planned elective treatment in the subacute phase. The indication for the preventive nature of the procedure is reportedly a maximum aortic diameter > 44 mm during the acute phase and a patent primary entry site in the thoracic aorta, while the optimal timing for TEVAR would be the subacute phase, from two weeks to three to six months after onset.
Furthermore, partial thrombosis of the false lumen, as compared with complete patency, is a significant independent predictor of post-discharge mortality in patients with acute type B aortic dissection, as continued patency, rather than complete thrombosis of the false lumen, is associated with aortic dilatation during follow-up and poorer outcomes. Other high-risk characteristics are currently under study, like vessel wall inflammation or flow pattern in the false lumen, both potentially useful harbingers or high-risk features. Vessel wall inflammation on a PET-scan may identify patients with uncomplicated aortic dissection at a higher risk for disease progression. Four-dimensional PC-MRI can be accurately applied to visualise and quantify flow characteristics in patients with aortic dissection. Stroke volume, velocity, distal dominant entry tears and helical flow are related to the rate of aortic expansion. Further studies are needed to further define those patients at the highest risk and, thus, most likely to benefit from early intervention and to design individualised, patient-centred treatment plans.
Author Contributions
Conceptualization—C.A.N. and X.Y.; resources—Y.X. and R.E.C.; data curation—C.A.N., X.Y. and R.E.C.; writing—original draft preparation, C.A.N., R.E.C., and X.Y.; writing—review and editing, X.Y. and C.A.N.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Olsson, C.; Thelin, S.; Stahle, E.; Ekbom, A.; Granath, F. Thoracic aortic aneurysm and dissection: Increasing prevalence and improved outcomes reported in a nationwide population-based study of more than 14,000 cases from 1987 to 2002. Circulation 2006, 114, 2611–2618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Acosta, S.; Ogren, M.; Bengtsson, H.; Bergqvist, D.; Lindblad, B.; Zdanowski, Z. Increasing incidence of ruptured abdominal aortic aneurysm: A population-based study. J. Vasc. Surg. 2006, 44, 237–243. [Google Scholar] [CrossRef] [Green Version]
- DeMartino, R.R.; Sen, I.; Huang, Y.; Bower, T.C.; Oderich, G.S.; Pochettino, A.; Greason, K.; Kalra, M.; Johnstone, J.; Shuja, F.; et al. Population-Based Assessment of the Incidence of Aortic Dissection, Intramural Hematoma, and Penetrating Ulcer, and Its Associated Mortality from 1995 to 2015. Circ. Cardiovasc. Qual. Outcomes 2018, 11, e004689. [Google Scholar] [CrossRef]
- Booher, A.M.; Isselbacher, E.M.; Nienaber, C.A.; Trimarchi, S.; Evangelista, A.; Montgomery, D.G.; Froehlich, J.B.; Ehrlich, M.; Oh, J.K.; Januzzi, J.L.; et al. The IRAD classification system for characterizing survival after aortic dissection. Am. J. Med. 2013, 126, 730.e19–730.e24. [Google Scholar] [CrossRef] [PubMed]
- Virtue Registry, I. The VIRTUE Registry of type B thoracic dissections—Study design and early results. Eur. J. Vasc. Endovasc. Surg. 2011, 41, 159–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fattori, R.; Cao, P.; De Rango, P.; Czerny, M.; Evangelista, A.; Nienaber, C.; Rousseau, H.; Schepens, M. Interdisciplinary expert consensus document on management of type B aortic dissection. J. Am. Coll. Cardiol. 2013, 61, 1661–1678. [Google Scholar] [CrossRef] [Green Version]
- Grabenwoger, M.; Alfonso, F.; Bachet, J.; Bonser, R.; Czerny, M.; Eggebrecht, H.; Evangelista, A.; Fattori, R.; Jakob, H.; Lönn, L.; et al. Thoracic Endovascular Aortic Repair (TEVAR) for the treatment of aortic diseases: A position statement from the European Association for Cardio-Thoracic Surgery (EACTS) and the European Society of Cardiology (ESC), in collaboration with the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur. Heart J. 2012, 33, 1558–1563. [Google Scholar]
- Erbel, R.; Aboyans, V.; Boileau, C.; Bossone, E.; Di Bartolomeo, R.; Eggebrecht, H.; Evangelista, A.; Falk, V.; Frank, H.; Gaemperli, O.; et al. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). Eur. Heart J. 2014, 35, 2873–2926. [Google Scholar]
- Riambau, V.; Bockler, D.; Brunkwall, J.; Cao, P.; Chiesa, R.; Coppi, G.; Czerny, M.; Fraedrich, G.; Haulon, S.; Jacobs, M.J.; et al. Editor’s Choice—Management of Descending Thoracic Aorta Diseases: Clinical Practice Guidelines of the European Society for Vascular Surgery (ESVS). Eur. J. Vasc. Endovasc. Surg. 2017, 53, 4–52. [Google Scholar] [CrossRef] [Green Version]
- Dake, M.D.; Kato, N.; Mitchell, R.S.; Semba, C.P.; Razavi, M.K.; Shimono, T.; Hirano, T.; Takeda, K.; Yada, I.; Miller, D. Endovascular stent-graft placement for the treatment of acute aortic dissection. N. Engl. J. Med. 1999, 340, 1546–1552. [Google Scholar] [CrossRef]
- Hiratzka, L.F.; Bakris, G.L.; Beckman, J.A.; Bersin, R.M.; Carr, V.F.; Casey, D.E.; Eagle, K.A.; Hermann, L.K.; Isselbacher, E.M.; Kazerooni, E.A.; et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with Thoracic Aortic Disease: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. Circulation 2010, 121, e266–e369. [Google Scholar] [PubMed] [Green Version]
- Durham, C.A.; Cambria, R.P.; Wang, L.J.; Ergul, E.A.; Aranson, N.; Patel, V.I.; Conrad, M.F. The natural history of medically managed acute type B aortic dissection. J. Vasc. Surg. 2015, 61, 1192–1198. [Google Scholar] [CrossRef] [Green Version]
- Tsai, T.T.; Fattori, R.; Trimarchi, S.; Isselbacher, E.; Myrmel, T.; Evangelista, A.; Hutchison, S.; Sechtem, U.; Cooper, J.V.; Smith, D.E.; et al. Long-term survival in patients presenting with type B acute aortic dissection: Insights from the International Registry of Acute Aortic Dissection. Circulation 2006, 114, 2226–2231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coady, M.A.; Ikonomidis, J.S.; Cheung, A.T.; Matsumoto, A.H.; Dake, M.D.; Chaikof, E.L.; Cambria, R.; Mora-Mangano, C.T.; Sundt, T.M.; Sellke, F. Surgical management of descending thoracic aortic disease: Open and endovascular approaches: A scientific statement from the American Heart Association. Circulation 2010, 121, 2780–2804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, X.; Mitsis, A.; Ghonem, M.; Iakovakis, I.; Nienaber, C.A. Conservative management versus endovascular or open surgery in the spectrum of type B aortic dissection. J. Vis. Surg. 2018, 4, 59. [Google Scholar] [CrossRef] [Green Version]
- Brunkwall, J.; Kasprzak, P.; Verhoeven, E.; Heijmen, R.; Taylor, P.; Alric, P.; Canaud, L.; Janotta, M.; Raithel, D.; Malina, M.; et al. Endovascular repair of acute uncomplicated aortic type B dissection promotes aortic remodelling: 1 year results of the ADSORB trial. Eur. J. Vasc. Endovasc. Surg. 2014, 48, 285–291. [Google Scholar] [CrossRef] [Green Version]
- Martin, G.; Patel, N.; Grant, Y.; Jenkins, M.; Gibbs, R.; Bicknell, C. Antihypertensive medication adherence in chronic type B aortic dissection is an important consideration in the management debate. J. Vasc. Surg. 2018, 68, 693–699.e2. [Google Scholar] [CrossRef]
- Nienaber, C.A.; Fattori, R.; Lund, G.; Dieckmann, C.; Wolf, W.; Von Kodolitsch, Y.; Nicolas, V.; Pierangeli, A. Nonsurgical reconstruction of thoracic aortic dissection by stent-graft placement. N. Engl. J. Med. 1999, 340, 1539–1545. [Google Scholar] [CrossRef]
- Mani, K.; Clough, R.E.; Lyons, O.T.; Bell, R.E.; Carrell, T.W.; Zayed, H.A.; Waltham, M.; Taylor, P.R. Predictors of outcome after endovascular repair for chronic type B dissection. Eur. J. Vasc. Endovasc. Surg. 2012, 43, 386–391. [Google Scholar] [CrossRef] [Green Version]
- Boufi, M.; Patterson, B.O.; Loundou, A.D.; Boyer, L.; Grima, M.; Loftus, I.M.; Holt, P.J. Endovascular Versus Open Repair for Chronic Type B Dissection Treatment: A Meta-Analysis. Ann. Thorac. Surg. 2019, 107, 1559–1570. [Google Scholar] [CrossRef] [Green Version]
- Miyairi, T.; Miyata, H.; Chiba, K.; Nishimaki, H.; Ogawa, Y.; Motomura, N.; Takamoto, S. Influence of Timing after Thoracic Endovascular Aortic Repair for Acute Type B Aortic Dissection. Ann. Thorac. Surg. 2018, 105, 1392–1396. [Google Scholar] [CrossRef] [Green Version]
- Tsai, T.T.; Evangelista, A.; Nienaber, C.A.; Trimarchi, S.; Sechtem, U.; Fattori, R.; Myrmel, T.; Pape, L.; Cooper, J.V.; Smith, D.E.; et al. Long-term survival in patients presenting with type A acute aortic dissection: Insights from the International Registry of Acute Aortic Dissection (IRAD). Circulation 2006, 114, I350–I356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nienaber, C.A.; Kische, S.; Rousseau, H.; Eggebrecht, H.; Rehders, T.C.; Kundt, G.; Glass, A.; Scheinert, D.; Czerny, M.; Kleinfeldt, T.; et al. Endovascular repair of type B aortic dissection: Long-term results of the randomized investigation of stent grafts in aortic dissection trial. Circ. Cardiovasc. Interv. 2013, 6, 407–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Enezate, T.H.; Omran, J.; Al-Dadah, A.S.; White, C.J.; Patel, M.; Mahmud, E.; Fattori, R.; Goldstein, J.A.; Goswami, N.; Gray, W.A.; et al. Thoracic endovascular repair versus medical management for acute uncomplicated type B aortic dissection. Catheter. Cardiovasc. Interv. 2018, 91, 1138–1143. [Google Scholar] [CrossRef] [PubMed]
- Qin, Y.L.; Wang, F.; Li, T.X.; Ding, W.; Deng, G.; Xie, B.; Teng, G.-J. Endovascular Repair Compared with Medical Management of Patients with Uncomplicated Type B Acute Aortic Dissection. J. Am. Coll. Cardiol. 2016, 67, 2835–2842. [Google Scholar] [CrossRef] [PubMed]
- Hossack, M.; Patel, S.; Gambardella, I.; Neequaye, S.; Antoniou, G.A.; Torella, F. Endovascular vs. Medical Management for Uncomplicated Acute and Sub-acute Type B Aortic Dissection: A Meta-analysis. Eur. J. Vasc. Endovasc. Surg. 2019, 59, 794–807. [Google Scholar] [CrossRef]
- Kato, N.; Shimono, T.; Hirano, T.; Suzuki, T.; Ishida, M.; Sakuma, H.; Yada, I.; Takeda, K. Midterm results of stent-graft repair of acute and chronic aortic dissection with descending tear: The complication-specific approach. J. Thorac. Cardiovasc. Surg. 2002, 124, 306–312. [Google Scholar] [CrossRef] [Green Version]
- Bogdan, Y.; Hines, G.L. Management of acute complicated and uncomplicated type B dissection of the aorta: Focus on endovascular stent grafting. Cardiol. Rev. 2010, 18, 234–239. [Google Scholar] [CrossRef]
- Umana, J.P.; Lai, D.T.; Mitchell, R.S.; Moore, K.A.; Rodriguez, F.; Robbins, R.C.; Oyer, P.E.; Dake, M.D.; Shumway, N.E.; Reitz, B.A.; et al. Is medical therapy still the optimal treatment strategy for patients with acute type B aortic dissections? J. Thorac. Cardiovasc. Surg. 2002, 124, 896–910. [Google Scholar] [CrossRef] [Green Version]
- Acosta, S.; Blomstrand, D.; Gottsater, A. Epidemiology and long-term prognostic factors in acute type B aortic dissection. Ann. Vasc. Surg. 2007, 21, 415–422. [Google Scholar] [CrossRef]
- Nienaber, C.A.; Zannetti, S.; Barbieri, B.; Kische, S.; Schareck, W.; Rehders, T.C. INvestigation of STEnt grafts in patients with type B Aortic Dissection: Design of the INSTEAD trial—A prospective, multicenter, European randomized trial. Am. Heart J. 2005, 149, 592–599. [Google Scholar] [CrossRef] [PubMed]
- Nienaber, C.A.; Rousseau, H.; Eggebrecht, H.; Kische, S.; Fattori, R.; Rehders, T.C.; Kundt, G.; Scheinert, D.; Czerny, M.; Kleinfeldt, T.; et al. Randomized comparison of strategies for type B aortic dissection: The INvestigation of STEnt Grafts in Aortic Dissection (INSTEAD) trial. Circulation 2009, 120, 2519–2528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamman, A.V.; Brunkwall, J.; Verhoeven, E.L.; Heijmen, R.H.; Trimarchi, S.; Kasprzak, P.; Alric, P.; Schumacher, H.; Fabiani, J.N.; Eckstein, H.-H.; et al. Predictors of aortic growth in uncomplicated type B aortic dissection from the Acute Dissection Stent Grafting or Best Medical Treatment (ADSORB) database. J. Vasc. Surg. 2017, 65, 964–971 e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, J.M.; Kim, S.D.; Kim, J.H.; Kim, M.-J.; Kang, D.H.; Seo, J.B.; Lim, T.-H.; Lee, J.W.; Song, M.G.; Song, J.-K. Long-term predictors of descending aorta aneurysmal change in patients with aortic dissection. J. Am. Coll. Cardiol. 2007, 50, 799–804. [Google Scholar] [CrossRef] [Green Version]
- Evangelista, A.; Salas, A.; Ribera, A.; Ferreira-González, I.; Cuellar-Calabria, H.; Pineda, V.; González-Alujas, T.; Bijnens, B.; Permanyer-Miralda, G.; Garcia-Dorado, D. Long-term outcome of aortic dissection with patent false lumen: Predictive role of entry tear size and location. Circulation 2012, 125, 3133–3141. [Google Scholar] [CrossRef] [Green Version]
- Trimarchi, S.; Jonker, F.H.; Froehlich, J.B.; Upchurch, G.R.; Moll, F.L.; Muhs, B.E.; Rampoldi, V.; Patel, H.J.; Eagle, K.A. Acute type B aortic dissection in the absence of aortic dilatation. J. Vasc. Surg. 2012, 56, 311–316. [Google Scholar] [CrossRef] [Green Version]
- Ray, H.M.; Durham, C.A.; Ocazionez, D.; Charlton-Ouw, K.M.; Estrera, A.L.; Miller, C.C.; Safi, H.J.; Azizzadeh, A. Predictors of intervention and mortality in patients with uncomplicated acute type B aortic dissection. J. Vasc. Surg. 2016, 64, 1560–1568. [Google Scholar] [CrossRef] [Green Version]
- Van Bogerijen, G.H.; Tolenaar, J.L.; Rampoldi, V.; Moll, F.L.; Van Herwaarden, J.A.; Jonker, F.H.W.; Eagle, K.A.; Trimarchi, S. Predictors of aortic growth in uncomplicated type B aortic dissection. J. Vasc. Surg. 2014, 59, 1134–1143. [Google Scholar] [CrossRef] [Green Version]
- Jonker, F.H.; Trimarchi, S.; Rampoldi, V.; Patel, H.J.; O’Gara, P.; Peterson, M.D.; Fattori, R.; Moll, F.L.; Voehringer, M.; Pyeritz, R.E.; et al. Aortic expansion after acute type B aortic dissection. Ann. Thorac. Surg. 2012, 94, 1223–1229. [Google Scholar] [CrossRef]
- Mussa, F.F.; Coselli, J.S.; Eagle, K.A. Feasibility of a proposed randomized trial in patients with uncomplicated descending thoracic aortic dissection: Results of worldwide survey. Am. Heart J. 2016, 181, 137–144. [Google Scholar] [CrossRef]
Figure 1.
Endovascular stent-graft placement induces aortic remodelling by expanding the true lumen, narrowing or obliterating the false lumen and inducing false lumen thrombosis.
Figure 1.
Endovascular stent-graft placement induces aortic remodelling by expanding the true lumen, narrowing or obliterating the false lumen and inducing false lumen thrombosis.

Figure 2.
Data from the INvestigation of STEnt grafts in patients with type B Aortic Dissections five-year follow-up trial (INSTEAD-XL) demonstrating a reduced disease progression and improved survival in patients receiving endovascular repair. TEVAR: thoracic endovascular repair and OMT: optical medical treatment.
Figure 2.
Data from the INvestigation of STEnt grafts in patients with type B Aortic Dissections five-year follow-up trial (INSTEAD-XL) demonstrating a reduced disease progression and improved survival in patients receiving endovascular repair. TEVAR: thoracic endovascular repair and OMT: optical medical treatment.

Figure 3.
Treatment algorithm for patients with acute type B aortic dissection.

© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Yuan, X.; Clough, R.E.; Nienaber, C.A. Management of Uncomplicated Type B Aortic Dissection. Hearts 2020, 1, 14-24. https://0-doi-org.brum.beds.ac.uk/10.3390/hearts1010004
AMA Style
Yuan X, Clough RE, Nienaber CA. Management of Uncomplicated Type B Aortic Dissection. Hearts. 2020; 1(1):14-24. https://0-doi-org.brum.beds.ac.uk/10.3390/hearts1010004
Chicago/Turabian StyleYuan, Xun, Rachel E. Clough, and Christoph A. Nienaber. 2020. "Management of Uncomplicated Type B Aortic Dissection" Hearts 1, no. 1: 14-24. https://0-doi-org.brum.beds.ac.uk/10.3390/hearts1010004