
AmnioClip-Plus as Sutureless Alternative to Amniotic Membrane Transplantation to Improve Healing of Ocular Surface Disorders

 , and
, and
Abstract
:1. Introduction
1.1. Anti-Inflammatory and Anti-Angiogenic Properties of the Amniotic Membrane Support Wound Healing and Reconstruction of the Ocular Surface
1.2. Disadvantages of Suture-Associated Amniotic Membrane Transplantation
2. Materials and Methods
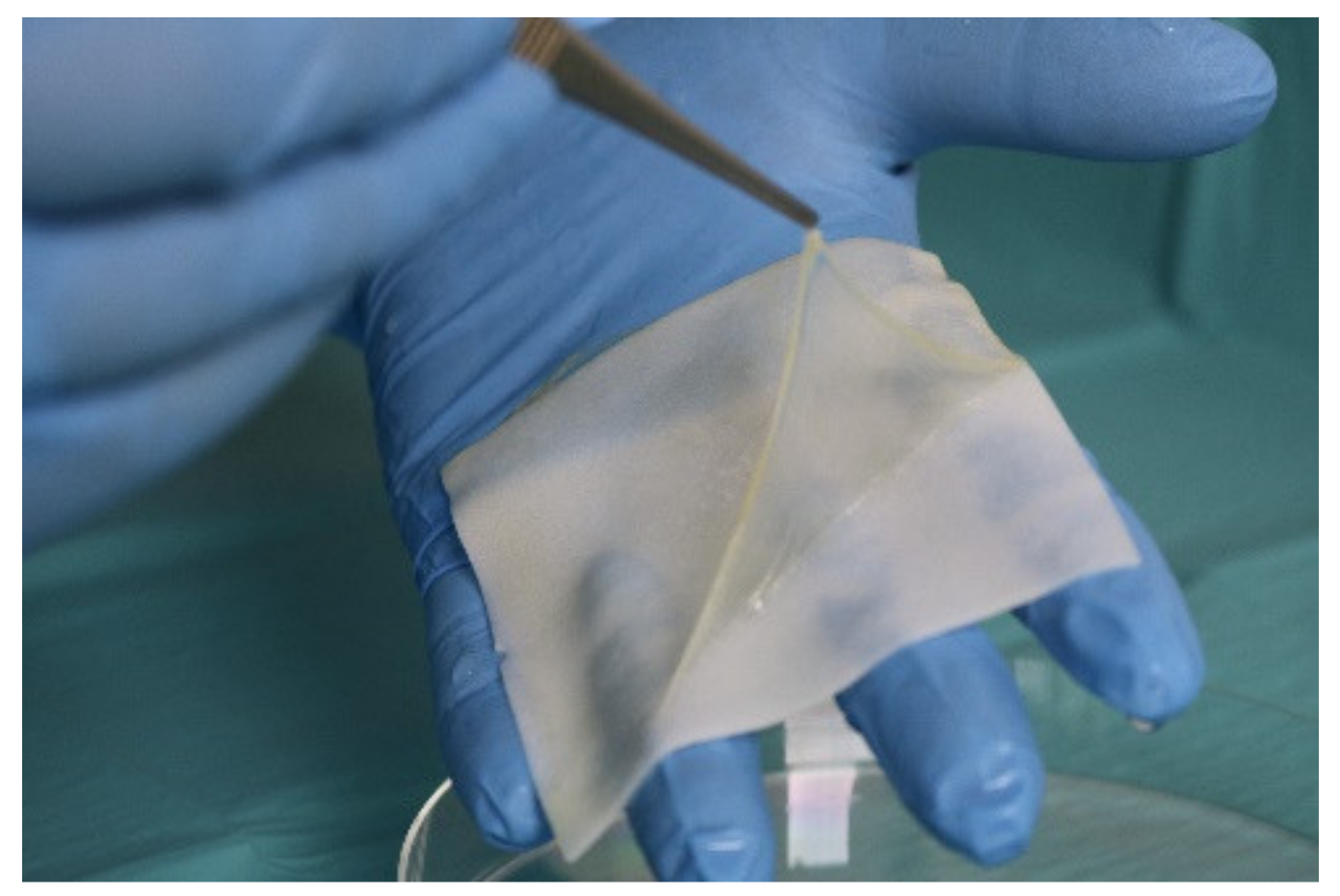
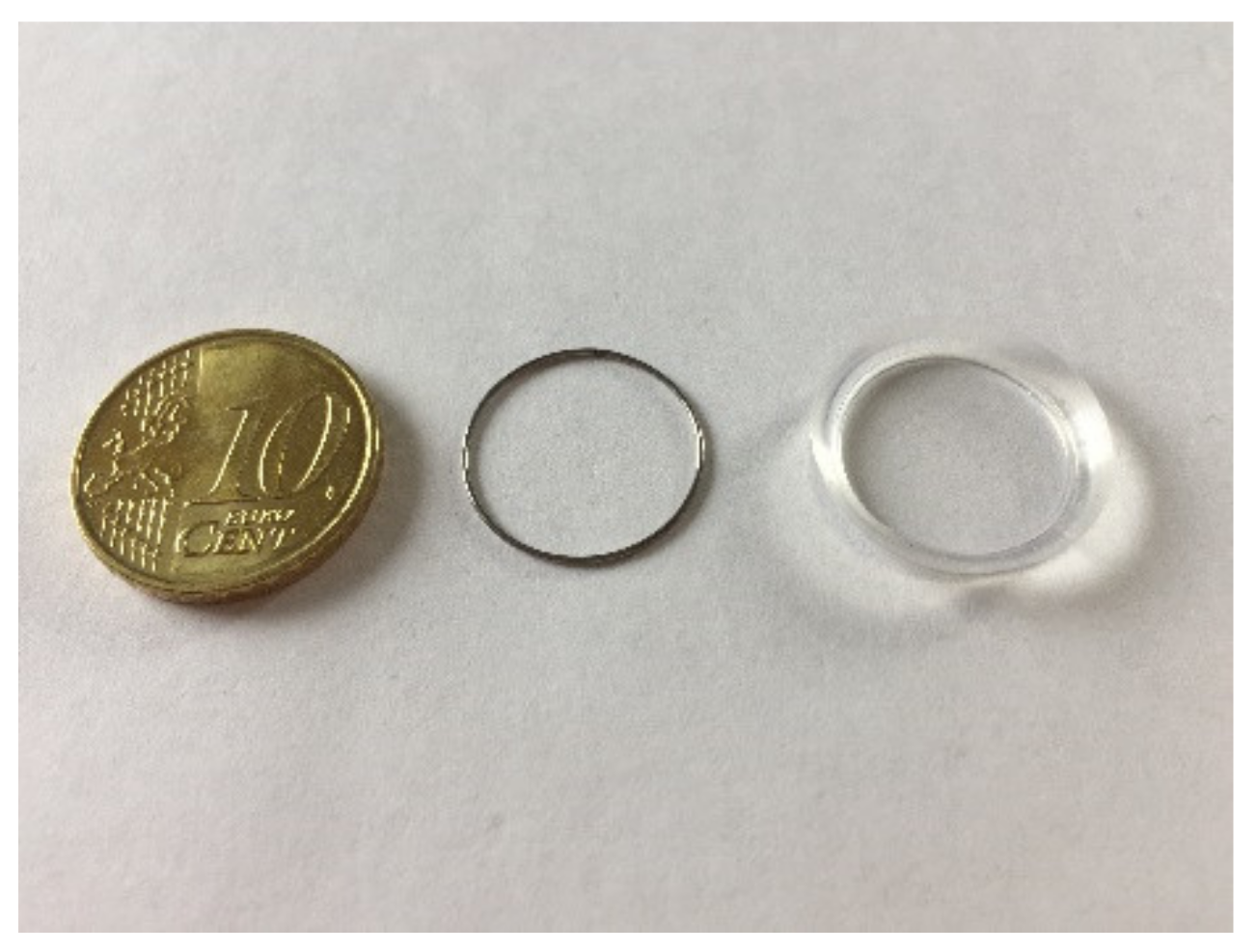
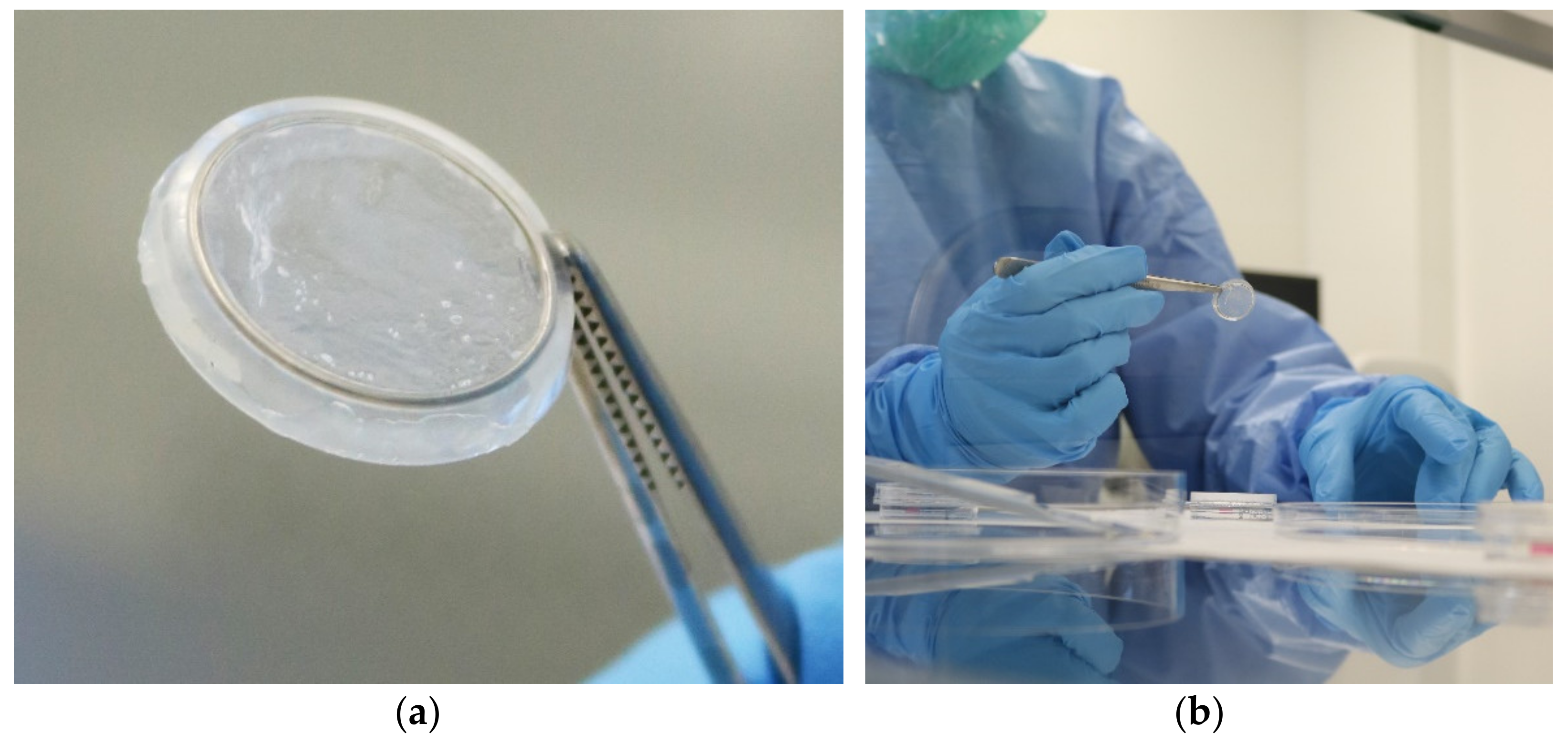
2.1. Development of the AmnioClip-Plus Ring System for Minimally Invasive Application without Sutures
2.2. The AmnioClip-Plus Is an Authority-Approved Tissue Preparation
3. Results
3.1. Clinical Experience Demonstrates the Easy Handling and Good Tolerability of the AmnioClip-Plus
3.2. The AC+ Improves the Clinical Picture and Well-Being of the Patient
4. Discussion and Conclusions
Summary of Clinical Advantages of the AmnioClip-Plus
- -
- Avoidance of surgical trauma for the patient;
- -
- No costly anesthetic procedures;
- -
- Minimizing an accompanying surgical risk;
- -
- Extensive absence of pain;
- -
- Easy handling of the amniotic membrane;
- -
- Consumer protection by providing the quality-tested combination product;
- -
- Safe production in the clean room of a tissue bank;
- -
- Short-term repetition of application possible;
- -
- Cost saving because of ambulant application;
- -
- Enabling extended therapy for prolonged/chronic defects such as “dry-eye syndrome”.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zazzo, A.D.; Kheirkhah, A.; Abud, T.B.; Goyal, S.; Dana, R. Management of high-risk corneal transplantation. Surv. Ophthalmol. 2017, 62, 816–827. [Google Scholar] [CrossRef] [PubMed]
- De Röth, A. Plastic repair of conjunctival defects with fetal membranes. Arch. Ophthalmol. 1946, 23, 522–525. [Google Scholar] [CrossRef]
- Lee, S.H.; Tseng, S.C. Amniotic membrane transplantation for persistent epithelial defects with ulceration. Am. J. Ophthalmol. 1997, 123, 303–312. [Google Scholar] [CrossRef]
- Kruse, F.E.; Rohrschneider, K.; Völcker, H.E. Multilayer amniotic membrane transplantation for reconstruction of deep corneal ulcers. Ophthalmology 1999, 106, 1504–1510. [Google Scholar] [CrossRef]
- Seitz, B. Amnionmembrantransplantation. Unverzichtbare Therapieoption bei persistierenden cornealen Epitheldefekten. Z. Prakt. Augenheilkund. 2003, 24, 445–450. [Google Scholar]
- Schuerch, K.; Baeriswyl, A.; Frueh, B.E.; Christoph, T. Efficacy of Amniotic Membrane Transplantation for the Treatment of Corneal Ulcers. Cornea 2020, 39, 479–483. [Google Scholar] [CrossRef]
- Lacorzana, J.; Campos, A.; Brocal-Sánchez, M.; Marín-Nieto, J.; Durán-Carrasco, O.; Fernández-Núñez, E.C.; López-Jiménez, A.; González-Gutiérrez, J.L.; Petsoglou, C.; García Serrano, J.L. Visual Acuity and Number of Amniotic Membrane Layers as Indicators of Ef-ficacy in Amniotic Membrane Transplantation for Corneal Ulcers: A Multicenter Study. J. Clin. Med. 2021, 10, 3234. [Google Scholar] [CrossRef]
- Dua, H.S.; Azuara-Blanco, A. Amniotic membrane transplantation. Br. J. Ophthalmol. 1999, 83, 748–752. [Google Scholar] [CrossRef] [Green Version]
- Kruse, F.S.; Meller, D. Die Amnionmembrantransplantation zur Rekonstruktion der Augenoberfläche. Ophthalmologe 2001, 98, 801–810. [Google Scholar] [CrossRef]
- Meller, D.; Pauklin, M.; Thomasen, H.; Westekemper, H.; Steuhl, K.-P. Amniotic Membrane Transplantation in the Human Eye. Dtsch. Arztebl. Int. 2011, 108, 243–248. [Google Scholar] [CrossRef]
- Borderie, V.M.; Levy, O.; Georgeon, C.; Bouheraoua, N. Simultaneous penetrating keratoplasty and amniotic membrane transplantation in eyes with a history of limbal stem cell deficiency. J. Fr. Ophtalmol. 2018, 41, 583–591. [Google Scholar] [CrossRef]
- Seitz, B.; Das, S.; Sauer, R.; Hofmann-Rummelt, C.; Beckmann, M.W.; Kruse, F.E. Simultaneous amniotic membrane patch in high-risk keratoplasty. Cornea 2011, 30, 269–272. [Google Scholar] [CrossRef]
- Dietrich, T.; Sauer, R.; Hofmann-Rummelt, C.; Langenbucher, A.; Seitz, B. Simultaneous amniotic membrane transplantation in emergency penetrating keratoplasty: A therapeutic option for severe corneal ulcerations and melting disorders. Br. J. Ophthalmol. 2011, 95, 1034–1035. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, S.; Szentmáry, N.; Seitz, B. Amniotic Membrane Transplantation for the Treatment of Infectious Ulcerative Keratitis Before Elective Penetrating Keratoplasty. Cornea 2013, 32, 1321–1325. [Google Scholar] [CrossRef] [PubMed]
- Paolin, A.; Cogliati, E.; Trojan, D.; Griffoni, C.; Grassetto, A.; Elbadawy, H.M.; Ponzin, D. Amniotic membranes in ophthalmology: Long term data on transplantation outcomes. Cell Tissue Bank. 2015, 17, 51–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adinolfi, M.; Akle, C.A.; McColl, I.; Fensom, A.H.; Tansley, L.; Connolly, P.; Hsi, B.-L.; Faulk, W.P.; Travers, P.; Bodmer, W.F. Expression of HLA antigens, beta 2-microglobulin and enzymes by human amniotic epithelial cells. Nature 1982, 295, 325–327. [Google Scholar] [CrossRef]
- Akle, C.A.; Welsh, K.J.; Adinolfi, M.; Leibowitz, S.; Mccoll, I. Immunogenicity of human amniotic epithelial cells after transplantation into volunteers. Lancet 1981, 318, 1003–1005. [Google Scholar] [CrossRef]
- Robson, M.C.; Krizek, T.J. The effect of human amniotic membranes on the bacteria population of infected rat burns. Ann. Surg. 1973, 177, 144–149. [Google Scholar] [CrossRef]
- Hao, Y.; Ma, D.H.-K.; Hwang, D.G.; Kim, W.-S.; Zhang, F. Identification of antiangiogenic and antiinflammatory proteins in human amniotic membrane. Cornea 2000, 19, 348–352. [Google Scholar] [CrossRef]
- Solomon, A.; Rosenblatt, M.; Monroy, D.; Ji, Z.; Pflugfelder, S.; Tseng, S. Suppression of Interleukin-1α and Interleukin-1β in the human corneal epithelial cells cultured on the amniotic membrane matrix. Br. J. Ophthalmol. 2001, 85, 444–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimmura, S.; Shimazaki, J.; Ohashi, Y.; Tsubota, K. Antiinflammatory effects of amniotic membrane transplantation in ocular surface disorders. Cornea 2001, 20, 408–413. [Google Scholar] [CrossRef]
- Shao, C.; Sima, J.; Zhang, S.X.; Jin, J.; Reinach, P.; Wang, Z.; Ma, J.-X. Suppression of corneal neovascularization by PEDF release from human amniotic membrans. Investig. Ophthalmol. Vis. Sci. 2004, 45, 1758–1762. [Google Scholar] [CrossRef] [Green Version]
- Koizumi, N.; Inatomi, T.; Sotozono, C.; Fullwood, H.J.; Quantock, A.J.; Kinoshita, S. Growth factor mRNA and protein in preserved human amniotic membrane. Curr. Eye Res. 2000, 20, 173–177. [Google Scholar] [CrossRef]
- Engelmann, K.; Kotomin, I.; Knipper, A.; Werner, C. Suture-free amniotic membrane transplantation. Ophthalmologe 2013, 110, 675–680. [Google Scholar] [CrossRef]
- Kotomin, I.; Valtink, M.; Hofmann, K.; Frenzel, A.; Morawietz, H.; Werner, C.; Funk, R.H.W.; Engelmann, K. Sutureless fixation of amniotic membrane for therapy of ocular surface disorders. PLoS ONE 2015, 10, e0125035. [Google Scholar] [CrossRef] [PubMed]
- Thomasen, H.; Schroeter, J.; Reinhard, T.; Seitz, B.; Steuhl, K.-P.; Meller, D. Good practice procedures for acquisition and preparation of cryopreserved human amniotic membranes from donor placentas. Ophthalmologe 2018, 115, 855–867. [Google Scholar] [CrossRef] [PubMed]
- Thomasen, H.; Pauklin, M.; Noelle, B.; Geerling, G.; Vetter, J.; Steven, P.; Steuhl, K.-P.; Meller, D. The effect of long-term storage on the biological and histological properties of cryopreserved amniotic membranes. Curr. Eye Res. 2011, 36, 247–255. [Google Scholar] [CrossRef]
- Hofmann, N.; Salz, A.-K.; Becke, K.; Möhle, N.; Börgel, M.; Diedenhofen, N.; Engelmann, K. AmnioClip-plus—Die nahtlose Amnionmembranbehandlung. Ophthalmo-Chir. 2020, 32, 179–183. [Google Scholar]
- Costa, E.; Murta, J.N. Amniotic Membrane in Ophthalmology. In Amniotic Membrane, 1st ed.; Mamede, A.C., Botelho, M.F., Eds.; Springer: Dordrecht, The Netherlands, 2015; pp. 105–122. [Google Scholar]
- Pachigolla, G.; Prasher, P.; Pascuale, M.; McCulley, J.; McHenry, J.G.; Mootha, V.V. Evaluation of the role of ProKera in the management of ocular surface and orbital disorders. Eye Contact Lens 2009, 35, 172–175. [Google Scholar] [CrossRef]
- Brocks, D.; Mead, O.G.; Tighe, S.; Tseng, S.C.G. Self-Retained Cryopreserved Amniotic Membrane for the Management of Corneal Ulcers. Clin. Ophthalmol. 2020, 14, 1437–1443. [Google Scholar] [CrossRef]
- Ozcan, A.; Esen, E.; Ciloglu, E. Sutureless amniotic membrane transplantation following excision of ocular surface neoplasia. Int. J. Ophthalmol. 2015, 8, 637–640. [Google Scholar] [PubMed]
- Kheirkhah, A.; Casas, V.; Blanco, G.; Li, W.; Hayashida, Y.; Chen, Y.-T.; Tseng, S.C.G. Amniotic membrane transplantation with fibrin glue for conjunctivochalasis. Am. J. Ophthalmol. 2007, 144, 311–313. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Indication | Mention for X [Number] Patients |
|---|---|
| Ulcer | 21 |
| Inflammation/keratitis | 16 |
| Keratoconjunctivitis sicca | 9 |
| Corneal erosion | 4 |
| Corneal chemical burn | 5 |
| Corneal scars * | 2 |
| Fuch’s endothelial dystrophy | 1 |
| Bullous cornea decompensation | 3 |
| Total of mentions | 61 |
| Surveyed Categories | Summarized Results |
|---|---|
| Insertion procedure | >73% easy and painless |
| occasionally experienced as unpleasant | |
| only complicated with uncommon anatomy of the eye | |
| Foreign body sensation | 52% none |
| if yes, usually until 1–3 days and only moderately | |
| Pain due to AC+ | >85% none |
| Stability of AC+ | loss and dislocation of the AC+ is only a rare event and if so, mostly due to the deviating anatomy (1 patient from 45)in individual cases hAM may dissolve before the end of the intended wearing time |
| Personal evaluation of the benefit | from ~68% regarded as helpful |
| only a few cases of discomfort |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hofmann, N.; Salz, A.-K.; Kleinhoff, K.; Möhle, N.; Börgel, M.; Diedenhofen, N.; Engelmann, K. AmnioClip-Plus as Sutureless Alternative to Amniotic Membrane Transplantation to Improve Healing of Ocular Surface Disorders. Transplantology 2021, 2, 425-432. https://0-doi-org.brum.beds.ac.uk/10.3390/transplantology2040040
Hofmann N, Salz A-K, Kleinhoff K, Möhle N, Börgel M, Diedenhofen N, Engelmann K. AmnioClip-Plus as Sutureless Alternative to Amniotic Membrane Transplantation to Improve Healing of Ocular Surface Disorders. Transplantology. 2021; 2(4):425-432. https://0-doi-org.brum.beds.ac.uk/10.3390/transplantology2040040
Chicago/Turabian StyleHofmann, Nicola, Anna-Katharina Salz, Kristin Kleinhoff, Niklas Möhle, Martin Börgel, Nancy Diedenhofen, and Katrin Engelmann. 2021. "AmnioClip-Plus as Sutureless Alternative to Amniotic Membrane Transplantation to Improve Healing of Ocular Surface Disorders" Transplantology 2, no. 4: 425-432. https://0-doi-org.brum.beds.ac.uk/10.3390/transplantology2040040