
Testosterone Boosters Intake in Athletes: Current Evidence and Further Directions


1
High Performance Sports Laboratory, Moscow Witte University, 115432 Moscow, Russia
2
Department of Sports Medicine and Medical Rehabilitation, Sechenov First Moscow State Medical University (Sechenov University), 119991 Moscow, Russia
3
Russian Football Union, 115172 Moscow, Russia
*
Author to whom correspondence should be addressed.
Endocrines 2021, 2(2), 109-120; https://0-doi-org.brum.beds.ac.uk/10.3390/endocrines2020011
Submission received: 16 March 2021
/
Revised: 11 May 2021
/
Accepted: 13 May 2021
/
Published: 17 May 2021
(This article belongs to the Special Issue Exercise Endocrinology)
{kind=link}
Abstract
:“Testosterone boosters” (TB)—are supplements that are claimed to increase testosterone levels in the human body. While the consumption of TB may be popular among athletes, there is insufficient evidence both about the safety and the real efficacy of TB. In our review, we searched MEDLINE/PubMed and Cochrane Library for studies on the effects of 15 substances that are claimed to increase testosterone levels Anacyclus pyrethrum; Bulbine natalensis; Epimedium (horny goat weed); L-arginine; L-carnitine; magnesium; Mucuna pruriens; pantothenic acid; selenium; shilajit Eurycoma longifolia (Tongkat Ali); Serenoa repens (saw palmetto); boron; Withania somnifera (ashwagandha); and Trigonella foenum-graecum (fenugreek) in athletes and healthy adults under 55 years of age. We found such studies regarding 10 out of 15 substances: L-arginine (3 studies); L-carnitine (2); magnesium (1); selenium (2); shilajit (1); Tongkat Ali (2); Serenoa repens (1); boron (3); ashwagandha root (2); and fenugreek (7). Many of them fail to prove the efficacy of these substances to increase testosterone levels. Tongkat Ali, ashwagandha, and fenugreek were the substances with the strongest evidence. The positive effect of magnesium and shilajit on testosterone concentration was shown in single studies. Conflicting data found that L-arginine, L-carnitine, Serenoa repens, selenium and boron do not appear to increase testosterone levels. There are almost no data on the safety profile of various TB components; however, certain TB components may be linked to coagulation, and pancreatic and hepatic disorders. Based on the review, the authors conclude that at present TB cannot be recommended for use by athletes due to insufficient data on their efficacy and safety.
Keywords:
androgens; athletes; Eurycoma longifolia; fenugreek; ashwagandha; shilajit; magnesium; boron1. Introduction
At the moment, there is a wide variety of supplements that, according to manufacturers, “increase serum testosterone level”—these supplements are called “testosterone boosters” (TB). Typically, TB contain a combination of a variety of natural substances but do not contain testosterone or other anabolic agents. The consumption of TB may be popular among athletes due to understanding the importance of testosterone in various aspects of sports performance, especially strength [1,2], and with the ever-improving detection of anabolic agents, which are on the WADA Prohibited List [3]. Another reason for the popularity of TB is the increasing recognition of RED-S (Relative energy deficiency in sport) syndrome, which includes low testosterone levels in athletes, and the constant seeking for legal strategies for increasing testosterone among such athletes [4]. At the same time, there is insufficient evidence, both about the safety and the real effectiveness of TB as agents of increasing testosterone levels in the body. In this regard, the study of data on the effectiveness of various components of TB is of great interest.
Most research on TB focuses on the treatment of erectile dysfunction [5], decreased libido [6], late-onset hypogonadism [7], and benign prostatic hyperplasia [8]. Several components of TB may be effective in the treatment of these diseases. In addition, there is a growing interest in the effects of TB on muscle strength and power. One of the first such studies was performed in Bulgaria, where Tribulus terrestris was promoted among weightlifters [9,10]. Other substances are also being actively researched. For example, Chen et al. showed that the combination of Eurycoma longifolia and resistance training improved peak power output in young males [11]. The relationship between boron intake and lean body-mass changes was discussed in another study [12]. Ashwagandha may help to increase muscle mass [13] as well as velocity, power, and maximal oxygen uptake (VO2 max) in healthy young men [14]. It is assumed that if TB increases testosterone levels, then they may also improve strength, power, and other parameters related to testosterone [10,11].
However, at the same time, there is very little evidence that a particular substance contained in TB actually increases serum testosterone concentration. In one of the largest studies on this topic, Clemesha et al. analyzed the available evidence base of the effectiveness of 109 substances contained in the 50 most popular TB, which were given by the Google search engine [15]. In 90% (n = 45) of the cases, the manufacturer claimed that their TB “increases testosterone levels” or “increases free testosterone levels”. In 62% of cases (n = 31), the manufacturer stated that the supplement “helps to build muscle mass”, and in 50% (n = 25) that the supplement “increases libido”. On average, one TB contained 8.3 individual substances. The most commonly found substances were zinc, fenugreek, vitamin B6, Tribulus terrestris, magnesium, boron, diindolmethane, Eurycoma longifolia, and maca. Clemesha et al. found that 67 out of 109 individual substances had no studies on their effects. For 19 substances (17.4%), there was only 1 study that examined their effect on testosterone levels; for 13 supplements (11.9%) there were 2 studies; for 3 supplements (2.8%) 3 studies; for 4 supplements (3.7%) 4 studies, for 1 supplement (0.9%) 5 studies; and for 1 supplement (0.9%) 6 studies were conducted. According to Clemesha et al., only in relation to 12 substances, all confirmed an increase in the concentration of testosterone: Anacyclus pyrethrum; Bulbine natalensis; Eurycoma longifolia (Tongkat Ali); fenugreek; horny goat weed; L-arginine; L-carnitine; magnesium; Mucuna pruriens; pantothenic acid; selenium; and shilajit [15].
Another review by Balasubramanian et al. analyzed the 5 most popular TB sold on Amazon.com and identified the 10 most common substances in them: Eurycoma longifolia (Tongkat Ali); horny goat weed; maca; nettle; ashwagandha root; Serenoa repens; boron; fenugreek; bioperine; and diindolylmethane [16]. According to these authors, only 5 out of 10 substances have scientific evidence that they can increase testosterone levels: Eurycoma longifolia (Tongkat Ali), Serenoa repens, boron, ashwagandha root, and fenugreek [16].
Our study aimed to evaluate the available evidence on the efficacy of individual TB components on healthy adults or athletes in order to establish the existing evidence base behind their use. The main hypothesis was that, for the vast majority of TB components, there is currently no high-quality evidence of efficacy in increasing testosterone levels in a group of healthy adults or athletes.
2. Materials and Methods
We used the following methodology for our narrative review: (1) the configuration of a working group: two operators skilled in sports supplementation; (2) formulation of the revision question based on considerations made in the abstract: “for the vast majority of TB components, there is currently no high-quality evidence of efficacy in increasing testosterone levels in a group of healthy adults or athletes”; (3) identification of relevant studies on PUBMED and Cochrane Library; and, (4) analysis and presentation of the outcomes: the data extrapolated from the revised studies were carried out in the form of a narrative review.
The keywords for our search included 12 substances that previously showed increased testosterone levels [15]. These are Anacyclus pyrethrum; Bulbine natalensis; Eurycoma longifolia (Tongkat Ali); fenugreek; horny goat weed; L-arginine; L-carnitine; magnesium; Mucuna pruriens; pantothenic acid; selenium; and shilajit [15]. In addition, three substances commonly found in TB from a study by Balasubramanian et al. [16], which had evidence that they may increase testosterone levels—saw palmetto, boron, and ashwagandha root—were analyzed separately. We used the names of the substances that produced the most results, grouped in inverted commas (“…”). The Boolean operator AND that allows the establishment of logical relations among concepts was used. Thus, a typical search was: “Testosterone” AND “substance name” (e.g., “fenugreek”).
The relevant studies were identified using advancing search modality; no time limits were applied. Only studies in English were searched. The selected studies were checked out based on title and abstract (AL, EB) to exclude irrelevant records. The remaining abstracts and subsequent remaining full-text articles were independently screened by 2 authors (AL and EB) for eligibility.
The inclusion criteria for eligible studies were as follows: (1) recruited an adult (age 18–54), healthy male, human population; (2) examined the effects of a single TB component; (3) published in English; and, (4) had pre- and post-testing of testosterone concentrations in male participants. The exclusion criteria were: (1) mean age equal or more than 55 years; (2) combination with other substances used; (3) participation of patients with any disease, including late-onset hypogonadism, obesity, and infertility, etc.; and (4) the studies did not report the required data for analyzing.
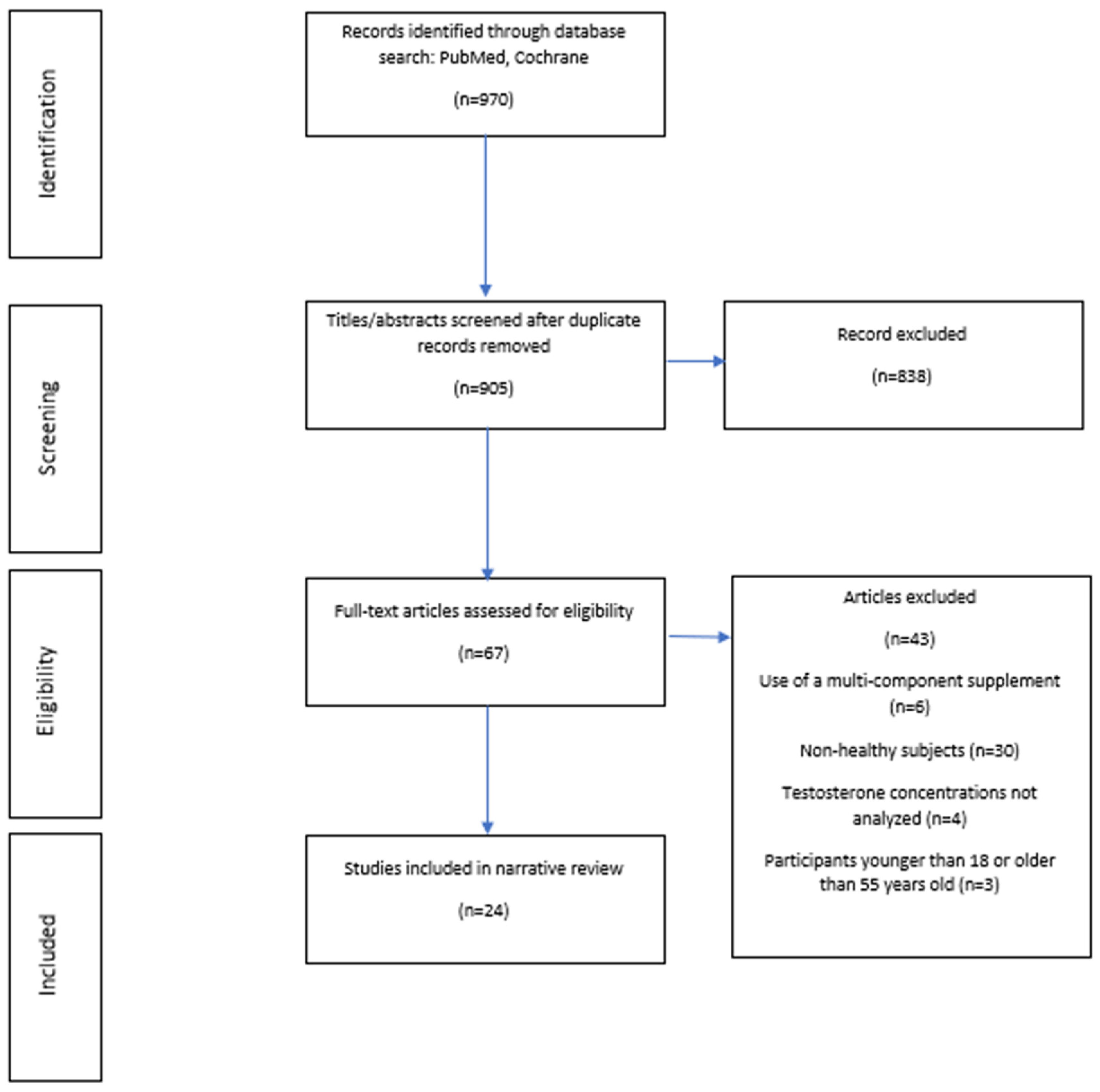
The data extrapolated from the revised studies were carried out in the form of a narrative review. The flow diagram of this narrative review has been reported in Figure 1. In our article, we first examined each of the TB components separately and then summarized our review in the discussion.
3. Results
The initial search identified 970 studies, of which 24 studies’ trials were identified as eligible following assessment using the selection criteria (Figure 1).
As a result of the search—only for 10 out of 15 substances (L-arginine; L-carnitine; magnesium; selenium; shilajit; Tongkat Ali; Serenoa repens; boron; ashwagandha root; and fenugreek—24 studies were found that met the inclusion criteria. No such studies were found for five analyzed substances (Anacyclus pyrethrum, Bulbine natalensis, Epimedium (horny goat weed), Pantothenic acid, and Mucuna pruriens).
3.1. L-Arginine
L-arginine is a semi-essential amino acid that performs several important functions in the body, such as nitric oxide production, the release of various hormones, immune function, etc. [17,18]. There are only three studies available that have examined the effect of isolated L-arginine intake on serum testosterone level in healthy, physically active adults.
In a randomized controlled trial, Abel et al. divided the volunteers into three groups: the high-concentration group (n = 10, age 38.6 ± 10.0 years) received 5.7 g L-arginine and 8.7 g aspartate; the low concentration group (n = 10, age 34.4 ± 8.6 years) received 2.8 g arginine and 2.2 g aspartate; and the placebo group (n = 10, age 36.1 ± 10.7 years) received placebo for four weeks. The authors concluded that the intake of arginine aspartate showed no influence on testosterone concentration [19].
In another RCT, Andrade et al. studied the effect of L-arginine on post-exercise recovery using a testosterone/cortisol ratio to assess the effect [20]. Healthy adults (n = 20, age 22.8 ± 3.4) were divided into two equal groups. The main group took 6 g of L-arginine after a session of high-intensity exercise. The control group took a placebo supplement after performing resistance exercise. The analysis showed that there was no significant difference in testosterone/cortisol ratio in both groups [20].
In a study by Moosakhani et al., the authors investigated the effects of 7 days of L-arginine alpha-ketoglutarate supplementation with 7 g/day L-arginine or placebo on endurance male swimmers (n = 24, age 30 ± 5 years) performing a 1500 m exhaustive swimming test. The authors found that testosterone increased (p < 0.05) in swimmers who received L-arginine [21].
There are also two studies in which L-arginine was used either in BCAA drinks or in combination with L-ornithine. Hsu et al. studied healthy adults (n = 14, age 23.4 ± 0.8) performing the aerobic exercise: the exposure group included subjects consuming a BCAA drink containing L-arginine (0.5 g) after exercise on two sessions, separated by 2 weeks [22]. The subjects from the control group ingested a placebo. The authors evaluated the changes in the testosterone/cortisol ratio in the exposure and control groups. The authors found that the testosterone/cortisol ratio was significantly higher in the exposure group than in the control group 120 min after the exercise. However, this difference may be explained by other components in the drink [22].
Zajac et al. analyzed the change in serum testosterone concentration in two groups of healthy volunteers performing resistance exercise [23]. Subjects in the exposure group (n = 9, age 23.5 ± 2.1) consumed L-ornithine (2.2 g) and L-arginine (3 g) for 3 weeks, and subjects in the placebo group (n = 8, age 22.8 ± 1.7 years) consumed placebo. The authors did not find any difference in the change in serum concentration of total testosterone between groups [23].
Thus, there are currently no sufficient data on the positive effect of isolated intake of L-arginine on serum testosterone concentration.
3.2. L-Carnitine
There were two studies on the effects of L-carnitine intake and testosterone levels during various exercise protocols. Kraemer et al. investigated the relationship between 3 weeks of L-carnitine L-tartrate (LCLT) supplementation and post-resistance-exercise feeding on hormonal response [24]. Resistance-trained men (n = 10, age 22 ± 1 year) took LCLT (equivalent to 2 g of L-carnitine per day) or a placebo (PL) for 21 days and then performed two exercise protocols: one followed by water intake, and one followed by feeding. The authors found that LCLT plus water produced the highest T concentration (compared to protocols with placebo and/or feeding). However, in another work, the same authors studied the influence of LCLT intake on testosterone in healthy, recreationally weight-trained men (n = 10, age 23.7 ± 2.3 years) during and after the squat exercise protocol. In this study, the authors concluded that there were no differences between the placebo and LCLT treatment conditions. To summarize, at the moment, there is no clear data on the effect of L-carnitine on testosterone levels [25].
3.3. Magnesium
We could find only one RCT by Cinar et al., which studied the relationship between isolated intake of magnesium and testosterone level [26]. In this study, 30 participants were divided into 3 equal groups (n = 10): exercising subjects receiving 10 mg magnesium per kg body weight for 4 weeks, sedentary subjects receiving 10 mg magnesium per kg body weight for 4 weeks, and exercising subjects without supplementation. As a result, in both groups that took magnesium, free and total testosterone increased. At the same time, the highest level of testosterone was seen in the group that exercised and took magnesium [26].
3.4. Selenium
There are two studies on the interaction between selenium intake and testosterone levels. In one RCT, Neek et al. selected male road cyclists (n = 32) into four groups: to take placebo; zinc supplement (30 mg/day); selenium supplement (200 μg/day); or zinc and selenium supplement for 4 weeks [27]. After treatment, free and total testosterone were determined before and after exhaustive exercise. Resting total, free testosterone was increased by exercise (p > 0.05). Total testosterone and free testosterone levels in the zinc group were even higher than in the selenium group after exercise (p < 0.05). The authors concluded that selenium supplementation for 4 weeks had no significant effect on testosterone levels [27].
In another RCT, El-Bayoumy et al. investigated the effect of selenium supplementation (247 μg/day) over 9 months in healthy adult males (n = 36, age 19–43) [28]. Interestingly, even such a long-term intake of selenium did not lead to an increase in testosterone: no differences were observed in testosterone levels for both the selenium and placebo groups between baseline and any of the time points. Thus, we found no evidence that isolated selenium intake may increase testosterone levels.
3.5. Shilajit
We were able to find only one RCT regarding shilajit that met the inclusion criteria. In a study by Pandit et al., healthy adults in the treatment group (n = 38, age 49.4 years) received purified shilajit (250 mg twice a day for 90 days) and 37 healthy adults in the control group (age 48.9 years) received a placebo [29]. As a result, the authors concluded, that the treatment with shilajit for a consecutive 90 days significantly increased total testosterone, free testosterone, and dehydroepiandrosterone (DHEAS) compared with a placebo [29].
3.6. Eurycoma Longifolia
Eurycoma longifolia (Tongkat Ali) contains some biologically active substances that may increase testosterone levels [30,31]. TB contain Tongkat Ali in various dosages. There is no single standard for the extraction. Almost all studies of Eurycoma longifolia have been carried out on non-healthy or elderly adults [5,7,32,33].
We found only two studies that investigated the change in serum testosterone concentration in healthy volunteers with an isolated intake of Tongkat Ali. Talbott et al. assessed changes in cortisol and testosterone levels and mood status using the POMS questionnaire in 63 subjects (32 men and 31 women) with moderate stress [34]. They were given a standardized hot water extract of Tongkat Ali root or placebo for 4 weeks. In men and women taking Tongkat Ali, cortisol showed a decrease (-16%) and testosterone increased (+37%) [34].
In another RCT, Chan et al. analyzed the influence of the intake of 600 mg Eurycoma on testosterone levels in healthy men (n = 32, mean age 24.4 ± 4.7 years) and found a significant increase in testosterone in the study group (from 8.0 ± 1.6 ng/mL) [35]. Free testosterone also increased significantly (from 9.4 ± 3.3 to 12.6 ± 5.9 pg/mL). Moreover, LH and FSH did not change, from which the researchers concluded that taking Eurycoma stimulates the hypothalamus–pituitary–adrenal axis to a greater extent [35].
3.7. Serenoa Repens
The only study we found on Serenoa repens effects on testosterone levels was an RCT by Strauch et al. [36], in which healthy male volunteers (n = 32, age 20–30 years) were divided into three groups: finasteride (5 mg/day) group, Serenoa extract (Permixon) 80 mg × 2 twice a day or a placebo for 7 days. During the study, the testosterone levels remained within the normal ranges. No significant between-group difference was detected in serum testosterone, except on days 3 and 6, respectively (p < 0.05) [36].
3.8. Boron
Boron may increase testosterone levels in men due to the uncoupling of the interactions between sex hormone-binding globulin (SHBG) and estrogen and testosterone [37]. However, only a few studies have examined the effects of boron supplementation on serum testosterone levels.
In a study by Naghii et al., the authors examined the effect of the intake of boron (10 mg daily) in healthy men (n = 8, mean age 41.3 ± 7.5) for a week. As a result, the authors found a statistically significant increase in the level of free testosterone, from 11.8 pg/mL to 15.2 pg/mL. At the same time, the level of total testosterone did not change significantly [38]. Total testosterone levels also did not change in another study by the same authors with a similar design [39].
At the same time, Ferrando et al. evaluated the effect of a daily intake of 2.5 mg of boron for 7 weeks in male bodybuilders (n = 10, age 20–27 years) [12]. The control group included nine people who received a placebo. Both groups performed strength training. Both groups showed significant increases in total testosterone, lean body mass, and squat and bench-press scores. The results showed that boron supplementation did not affect plasma total and free testosterone, plasma boron, lean body mass, and strength compared to a placebo. Analysis of variance showed no difference in the increase in total testosterone between the groups taking (from 5.4 ± 1.6 to 7.2 ± 2.7 ng/mL, p < 0.01) and those who did not take boron (from 5.4 ± 2.1 to 6.5 ± 1.9 ng/mL, p < 0.01) [12].
To conclude, at the moment there are no unambiguous data on how boron intake affects the level of testosterone in physically active healthy adults.
3.9. Ashwagandha Root
In a study by Smith et al., ashwagandha root and fenugreek are among the substances with the most evidence on the effect of their use on testosterone levels [40]. We found two studies on the effect of a course intake of ashwagandha root on serum testosterone concentration.
In the RCT by Wankhede et al., conducted with male subjects (n = 57, age 18–50 years), those who took ashwagandha significantly increased muscle strength and muscle size, as well as serum testosterone concentration. The T level increased from 630.5 ± 231.9 to 726.6 ± 171.6 ng/dl, (p < 0.001) in those who took ashwagandha, while in those who did not take it, it did not change [13]. Compared to the placebo subjects, the group treated with ashwagandha had significantly greater increases in muscle strength on the bench-press exercise and the leg-extension exercise, and significantly greater muscle-size increase at the arms and chest [13].
In another RCT, Lopresti et al. examined the effect of a daily intake of 240 mg ashwagandha for 60 days on total testosterone levels in men (n = 19) and women (n = 11) (mean age 42.2 ± 2.4) [41]. Total testosterone increased from 472.9 ± 45.0 to 526.9 ± 48.0 ng/dl (p = 0.038). The testosterone level did not change statistically significantly in women. It should be noted that the increase in testosterone level in the exposure group was not statistically significant compared to the placebo group (p = 0.158) [41].
3.10. Fenugreek
Certain fenugreek (or Trigonella foenum-graecum) compounds may inhibit aromatase and 5-alpha reductase activity, leading to decreased testosterone breakdown [40]. However, the effectiveness of fenugreek in increasing testosterone levels and the safety profile is still unclear [42].
Rao et al. conducted an RCT on healthy men (n = 120, age 54.8 ± 6.9 years) who used a standardized extract of fenugreek seeds at a dose of 600 mg daily for 12 weeks [6]. Sexual function improved in this group, including such indicators as the number of morning erections and the frequency of intercourse. In the main group, the levels of total testosterone increased from 12.3 ± 4.4 to 13.8 ± 5.1 nmol/L, (p = 0.001). Free testosterone increased from 241.0 ± 68.9 to 264.8 ± 78.9 pmol/L, (p = 0.002) [6].
Wilborn et al. also conducted an RCT in which resistance-trained men (n = 30) took 500 mg of fenugreek extract for 8 weeks and participated in a resistance training program. The authors’ results are interesting: although some parameters changed significantly (percent body fat, total testosterone, and bioavailable testosterone), other parameters, important for athletes, did not change (Wingate peak or mean power, total body weight) [43].
In another work, Rao et al. compared fenugreek extract and a placebo in an 8-week calisthenic program. Male participants (n = 138, 25–47 years) were randomized into three groups: 600 mg fenugreek/day, 300 mg fenugreek/day or placebo. The 600 mg group showed decreases in body mass of 1.2 kg, −1.4% body fat, and an increase in lean mass (1.8%) at 8 weeks. This group also improved their maximal leg press more than the placebo group (p < 0.05) and demonstrated a significant increase in total testosterone both between baseline and groups (from 17.2 ± 6.9 to 18.5 ± 6.7 nmol/L) [44].
Wankhede et al. compared the effects of taking 300 mg fenugreek extract twice daily versus placebo during a resistance-training program for 8 weeks in healthy males (n = 60). The fenugreek group showed significant improvements in body fat. Levels of free but not total testosterone increased more with fenugreek (p < 0.05) (17.8 to 35.3 ng/dL, p < 0.001) than in the placebo group (21.3 to 31.7 ng/dL, p < 0.01). The increase in total testosterone from baseline was not significant between the treatment groups [45].
Mokashi et al. investigated the effects of a single 600 mg fenugreek seed-extract dose in healthy volunteers (n = 16, age 18–45 years). The authors found a significant increase in testosterone levels as compared with the placebo group. In particular, total testosterone differed (p < 0.05) between 3 and 10 h after taking fenugreek. Ten hours later, total testosterone was 501.1 ± 144.6 ng/mL for the placebo group and 519.0 ± 189.3 ng/mL for those on fenugreek (473.6 ± 185.3 and 405.5 ± 142.9 ng/mL per baseline, respectively) [46].
In another study, Maheshwari et al. noted an increase in the concentration of free testosterone but not total testosterone in those who received 500 mg of fenugreek extract once a day for 12 weeks [47]. This study involved healthy men (n = 50, age 43.1 years). Free testosterone changed from 8.2 ± 5.0 to 12.0 ± 5.7 pg/mL (p = 0.0004) [47].
One of the highest-quality studies on fenugreek is the meta-analysis by Mansoori et al., which included 4 studies performed on healthy volunteers, a total of 105 adults in exposure groups and 101 control subjects. The mean age in these studies ranged from 21 to 55.6 years [48]. The authors concluded that fenugreek affects the level of total testosterone; however, they noted a great heterogeneity of the studies included.
In summary, fenugreek is one of the most well-studied components of TB, and virtually all studies show increased testosterone levels in healthy adults, but further high-quality research is recommended.
4. Discussion
In our review, we analyzed studies on the effect of individual TB components on testosterone levels. With regard to 15 analyzed substances, we were able to find only 24 studies evaluating the effect of their isolated course intake on testosterone serum concentration in athletes and healthy adults under 55 years of age. Such studies were carried out in relation to 10 out of 15 substances: L-arginine (3 studies); L-carnitine (2); magnesium (1); selenium (2); shilajit (1); Tongkat Ali (2); Serenoa repens (1); boron (3); ashwagandha root (2); and fenugreek (7). For Anacyclus pyrethrum, Bulbine natalensis, Mucuna pruriens, Epimedium (horny goat weed), and Pantothenic acid, no studies meeting the inclusion criteria were found. Tongkat Ali, ashwagandha, and fenugreek were the substances with the strongest evidence. The positive effect of magnesium and shilajit on testosterone concentration was shown in single studies. Conflicting data were found for L-arginine, L-carnitine, and Serenoa repens. Selenium and boron do not appear to increase testosterone levels.
However, during the search, we found studies that examined the effect of several analyzed substances on serum testosterone concentration among patients with various diseases. For example, several studies have shown the effectiveness of isolated intake of Mucuna pruriens, Serenoa repens, and Eurycoma longifolia on serum testosterone concentration in people with infertility [49], benign prostatic hyperplasia [8], and hypogonadism [7], respectively. There are also studies in which substances were used in combination with other substances [22,23,50]. However, the combined use does not allow assessing the effect of each of the components, and therefore one cannot assert the effectiveness of a particular substance on any parameter.
Smith et al., in their systematic review of the effects of 13 herbs on testosterone concentration, concluded that fenugreek and ashwagandha have positive effects on testosterone concentrations in men [40]. We also found that these substances are most likely to increase testosterone. Also, according to the authors, Tongkat Ali was not classified as a substance with positive effects on testosterone concentration based on one study, while in our work we identified additional studies indicating that Tongkat Ali appears to increase testosterone levels. The main difference from our study was in the analyzed TB components (Smith et al. did not analyze magnesium; selenium; boron; L-arginine; Anacyclus pyrethrum; Bulbine natalensis; Mucuna pruriens; Epimedium; Pantothenic acid; L-carnitine; or Serenoa repens, but did analyze Panax ginseng; Tribulus terrestris; maca; rhodiola; musali; garcinia; forskohlii; reishi; stinging nettle; and Cordyceps sinensis) [40].
Clemesha et al. found 12 substances with nonconflicting data regarding the increase in testosterone levels [15]. The main difference of this work was that the authors looked for studies in men without specific inclusion criteria, while we tried to find studies in healthy men of a specific age group. Among these 12 substances, according to our work, only Tongkat Ali, Ashwagandha, and fenugreek can be classified as substances with the strongest evidence [15].
An interesting novel approach was used by Balasubramanian et al. These authors analyzed the most popular TB on the Amazon website [16]. It is important to note that substances such as Tongkat Ali, ashwagandha, and fenugreek were among the 10 most common components of popular TB, but other components of the most popular TB raise questions about effectiveness. According to the authors, 5 out of 10 of these ingredients (nettle, maca, horny goat weed, Bioperine, and diindolylmethane) had no evidence of any positive effects on testosterone levels at all [16].
It is important to understand the possible mechanisms for increasing testosterone in substances such as Tongkat Ali, ashwagandha, and fenugreek. There are several potential mechanisms for how Tongkat Ali may increase testosterone. First, Eurycoma longifolia contains some biologically active substances (eurycomanones and eurycomanols) that may inhibit the conversion of testosterone to estradiol by the aromatase enzyme, thereby increasing testosterone levels. Second, these substances can increase the release rate of “free” testosterone from the sex-hormone-binding-globulin (SHBG) [34,51]. Possible mechanisms for increasing testosterone by ashwagandha intake are well described in the work of Lopresti et al. [52]. Some studies have shown that ashwagandha can stimulate the release of gonadotropin-releasing hormone (GnRH) and thereby stimulate the secretion of testosterone from Leydig cells [53]. On the other hand, since ashwagandha has antioxidant and anti-inflammatory activity [54], testosterone levels may increase due to a decrease in oxidative stress [52]. A third hypothesis is that ashwagandha can inhibit aromatase, the enzyme that converts testosterone to estradiol [52]. Fenugreek contains a variety of sapogenins such as diosgenin and yamogenin. In particular, diosgenin may be an important precursor in testosterone synthesis [48]. On the other hand, it is suggested that fenugreek can increase testosterone through an aromatase and 5α reductase inhibition [45].
Thus, despite the fact that at the moment there is no unambiguous idea of how Tongkat Ali, ashwagandha, and fenugreek realize their effects, the general mechanisms should be noted as potentially: inhibition of the conversion of testosterone to estradiol by aromatase (all three substances); free testosterone release from the SHBG (Eurycoma); stimulation of the GnRH release (ashwagandha); reduction in overall oxidative stress (ashwagandha); and also being precursors in steroidogenesis (fenugreek).
It is noteworthy that there is still only sporadic evidence of possible side effects associated with the intake of the analyzed substances. For example, there are case reports describing various complications of TB intake [42,55,56,57]. Nguyen et al. described a case of pulmonary embolism in a previously healthy 51-year-old man secondary to fenugreek-containing TB [42]. The patient started taking TB 3 months before he was admitted to the hospital and stopped taking these supplements 1 week before the admission. Interestingly, his total testosterone levels were low [42]. In another case report, Bui et al. reported bilateral pulmonary embolism in a 65-year-old man taking diindolylmethane for 3 months [57]. However, this patient had other thromboembolism risk factors, such as a suspected prior PE, history of tobacco use, age, and obesity [57]. In addition, TB have been linked to pancreatic and hepatic diseases [55,56]. Thus, Almaiman et al. reported a case of abdominal pain and elevation in liver transaminases (AST, ALT) in a 30-year-old athlete taking multicomponent TB [55]. In another case report, authors described acute pancreatitis in a 65-year-old man taking 160 mg of saw palmetto extract for 1 week [56]. The patient had a history of diabetes, hypertension, hyperlipidemia, gout, Barrett esophagitis, and chronic gastritis; however, the further workup excluded cholelithiasis and hypertriglyceridemia as possible causes. The patient denied recent alcohol intake. Despite the fact that the most likely cause of pancreatitis in this case was saw palmetto, the underlying mechanism is unknown [56].
The fact that certain substances reviewed can increase various aspects of physical performance and increase testosterone levels could potentially lead to the inclusion of these substances in the WADA Monitoring program. [57,58]. For example, the steroidlike substance ecdysterone [59], which is present in some TB, is already on the Monitoring list, and some authors demand to prohibit ecdysterone on the basis of single studies conducted on animals and healthy volunteers [60,61].
The limitations of our review include the exclusion of non-English studies, the heterogeneity of individual TB components and their preparations used, and the use of only PubMed and Cochrane Library databases. It should also be noted that almost in all studies meeting the inclusion criteria, serum testosterone analysis was performed using various modifications of the immunoassay method, while more accurate techniques such as mass spectrometry (MS) and liquid chromatography–tandem mass spectrometry (LC–MS) are now available [61].
Our results clearly indicate the need for further high-quality studies assessing the effect of isolated intake of substances contained in TB on serum testosterone concentration in groups of healthy adults. Of particular interest are studies carried out among athletes, even at an amateur level, since potentially TB can fall under the WADA Monitoring program and Prohibited List criteria. It would be very interesting to assess the prevalence of TB consumption among athletes of all levels. Also, it is crucial to examine the safety profile of at least the most popular individual components of TB.
5. Conclusions
Currently, there are only a few studies on the effect of the most popular components of TB on serum testosterone concentration. Most of these studies are of high quality (RCTs), but most often are not performed on athletes.
There is almost no data on the safety profile of various TB components. However, several components may cause coagulation, and hepatic and pancreatic problems; as such, caution is warranted with their use.
Since most TB contain several substances, a substance with unproven efficacy and safety may probably be ingested during TB course intake.
There is a need for further high-quality studies (e.g., RCTs with a structured approach using LC–MS/MS hormonal measurements) assessing the effect of isolated intake of substances contained in TB on serum testosterone concentration in groups of healthy adults.
Based on the review, the authors conclude that at present TB cannot be recommended for use by athletes due to insufficient data on their efficacy and safety.
Author Contributions
Conceptualization, A.L. and E.B.; methodology, A.L. and E.B.; software, A.L.; validation, A.L. and E.B.; formal analysis, A.L. and E.B.; investigation, A.L.; resources, A.L. and E.B.; data curation, A.L.; writing—original draft preparation, A.L.; writing—review and editing, E.B.; visualization, A.L.; supervision, E.B.; project administration, A.L.; funding acquisition, A.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author A.L. upon reasonable request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bhasin, S.; Woodhouse, L.; Casaburi, R.; Singh, A.B.; Bhasin, D.; Berman, N.; Chen, X.; Yarasheski, K.E.; Magliano, L.; Dzekov, C.; et al. Testosterone Dose-Response Relationships in Healthy Young Men. Am. J. Physiol. Endocrinol. Metab. 2001, 281, E1172–E1181. [Google Scholar] [CrossRef] [Green Version]
- Finkelstein, J.S.; Lee, H.; Burnett-Bowie, S.-A.M.; Pallais, J.C.; Yu, E.W.; Borges, L.F.; Jones, B.F.; Barry, C.V.; Wulczyn, K.E.; Thomas, B.J.; et al. Gonadal Steroids and Body Composition, Strength, and Sexual Function in Men. N. Engl. J. Med. 2013, 369, 1011–1022. [Google Scholar] [CrossRef] [Green Version]
- Geyer, H.; Schänzer, W.; Thevis, M. Anabolic Agents: Recent Strategies for Their Detection and Protection from Inadvertent Doping. Br. J. Sports Med. 2014, 48, 820–826. [Google Scholar] [CrossRef] [Green Version]
- Hooper, D.R.; Tenforde, A.S.; Hackney, A.C. Treating Exercise-Associated Low Testosterone and Its Related Symptoms. Physician Sportsmed. 2018, 46, 427–434. [Google Scholar] [CrossRef]
- Leitão, A.E.; de Souza Vieira, M.C.; Pelegrini, A.; da Silva, E.L.; de Azevedo Guimarães, A.C. A 6-Month, Double-Blind, Placebo-Controlled, Randomized Trial to Evaluate the Effect of Eurycoma Longifolia (Tongkat Ali) and Concurrent Training on Erectile Function and Testosterone Levels in Androgen Deficiency of Aging Males (ADAM). Maturitas 2021, 145, 78–85. [Google Scholar] [CrossRef]
- Rao, A.; Steels, E.; Inder, W.J.; Abraham, S.; Vitetta, L. Testofen, a Specialised Trigonella Foenum-Graecum Seed Extract Reduces Age-Related Symptoms of Androgen Decrease, Increases Testosterone Levels and Improves Sexual Function in Healthy Aging Males in a Double-Blind Randomised Clinical Study. Aging Male Off. J. Int. Soc. Study Aging Male 2016, 19, 134–142. [Google Scholar] [CrossRef]
- Tambi, M.I.B.M.; Imran, M.K.; Henkel, R.R. Standardised Water-Soluble Extract of Eurycoma Longifolia, Tongkat Ali, as Testosterone Booster for Managing Men with Late-Onset Hypogonadism? Andrologia 2012, 44 (Suppl. 1), 226–230. [Google Scholar] [CrossRef]
- Sudeep, H.V.; Thomas, J.V.; Shyamprasad, K. A Double Blind, Placebo-Controlled Randomized Comparative Study on the Efficacy of Phytosterol-Enriched and Conventional Saw Palmetto Oil in Mitigating Benign Prostate Hyperplasia and Androgen Deficiency. BMC Urol. 2020, 20, 86. [Google Scholar] [CrossRef]
- Koumanov, F.; Bozadjieva, E.; Andreeva, M.; Platonva, E.; Ankov, V. Clinical Trial of Tribestan. Exp. Med. 1982, 4, 211–215. [Google Scholar]
- Pokrywka, A.; Obmiński, Z.; Malczewska-Lenczowska, J.; Fijałek, Z.; Turek-Lepa, E.; Grucza, R. Insights into Supplements with Tribulus Terrestris Used by Athletes. J. Hum. Kinet. 2014, 41, 99–105. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.K.; Ooi, F.K.; Abu Kasim, N.A.; Asari, M.A. Effects of Eurycoma Longifolia Jack Supplementation Combined with Resistance Training on Isokinetic Muscular Strength and Power, Anaerobic Power, and Urinary Testosterone: Epitestosterone Ratio in Young Males. Int. J. Prev. Med. 2019, 10, 118. [Google Scholar] [CrossRef] [PubMed]
- Ferrando, A.A.; Green, N.R. The Effect of Boron Supplementation on Lean Body Mass, Plasma Testosterone Levels, and Strength in Male Bodybuilders. Int. J. Sport Nutr. 1993, 3, 140–149. [Google Scholar] [CrossRef] [PubMed]
- Wankhede, S.; Langade, D.; Joshi, K.; Sinha, S.R.; Bhattacharyya, S. Examining the Effect of Withania Somnifera Supplementation on Muscle Strength and Recovery: A Randomized Controlled Trial. J. Int. Soc. Sports Nutr. 2015, 12, 43. [Google Scholar] [CrossRef] [Green Version]
- Sandhu, J.S.; Shah, B.; Shenoy, S.; Chauhan, S.; Lavekar, G.S.; Padhi, M.M. Effects of Withania Somnifera (Ashwagandha) and Terminalia Arjuna (Arjuna) on Physical Performance and Cardiorespiratory Endurance in Healthy Young Adults. Int. J. Ayurveda Res. 2010, 1, 144–149. [Google Scholar] [CrossRef] [Green Version]
- Clemesha, C.G.; Thaker, H.; Samplaski, M.K. “Testosterone Boosting” Supplements Composition and Claims Are Not Supported by the Academic Literature. World J. Men’s Health 2020, 38, 115–122. [Google Scholar] [CrossRef]
- Balasubramanian, A.; Thirumavalavan, N.; Srivatsav, A.; Yu, J.; Lipshultz, L.I.; Pastuszak, A.W. Testosterone Imposters: An Analysis of Popular Online Testosterone Boosting Supplements. J. Sex. Med. 2019, 16, 203–212. [Google Scholar] [CrossRef]
- McConell, G.K. Effects of L-Arginine Supplementation on Exercise Metabolism. Curr. Opin. Clin. Nutr. Metab. Care 2007, 10, 46–51. [Google Scholar] [CrossRef]
- McRae, M.P. Therapeutic Benefits of L-Arginine: An Umbrella Review of Meta-Analyses. J. Chiropr. Med. 2016, 15, 184–189. [Google Scholar] [CrossRef] [Green Version]
- Abel, T.; Knechtle, B.; Perret, C.; Eser, P.; von Arx, P.; Knecht, H. Influence of Chronic Supplementation of Arginine Aspartate in Endurance Athletes on Performance and Substrate Metabolism—A Randomized, Double-Blind, Placebo-Controlled Study. Int. J. Sports Med. 2005, 26, 344–349. [Google Scholar] [CrossRef]
- Andrade, W.B.; Jacinto, J.L.; da Silva, D.K.; Roveratti, M.C.; Estoche, J.M.; Oliveira, D.B.; Balvedi, M.C.W.; da Silva, R.A.; Aguiar, A.F. L-Arginine Supplementation Does Not Improve Muscle Function during Recovery from Resistance Exercise. Appl. Physiol. Nutr. Metab. Physiol. Appl. Nutr. Metab. 2018, 43, 928–936. [Google Scholar] [CrossRef]
- Moosakhani, A.; Choobineh, S.; Soori, R. Effect of L-Arginine Alpha Ketoglutarate Supplementation on Hormonal Response during Recovery in Male Endurance Swimmers. Gazz. Med. Ital. Arch. Sci. Med. 2018, 177, 65–71. [Google Scholar] [CrossRef]
- Hsu, M.-C.; Chien, K.-Y.; Hsu, C.-C.; Chung, C.-J.; Chan, K.-H.; Su, B. Effects of BCAA, Arginine and Carbohydrate Combined Drink on Post-Exercise Biochemical Response and Psychological Condition. Chin. J. Physiol. 2011, 54, 71–78. [Google Scholar] [CrossRef]
- Zajac, A.; Poprzecki, S.; Zebrowska, A.; Chalimoniuk, M.; Langfort, J. Arginine and Ornithine Supplementation Increases Growth Hormone and Insulin-like Growth Factor-1 Serum Levels after Heavy-Resistance Exercise in Strength-Trained Athletes. J. Strength Cond. Res. 2010, 24, 1082–1090. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kraemer, W.J.; Spiering, B.A.; Volek, J.S.; Ratamess, N.A.; Sharman, M.J.; Rubin, M.R.; French, D.N.; Silvestre, R.; Hatfield, D.L.; van Heest, J.L.; et al. Androgenic Responses to Resistance Exercise: Effects of Feeding and L-Carnitine. Med. Sci. Sports Exerc. 2006, 38, 1288–1296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kraemer, W.J.; Volek, J.S.; French, D.N.; Rubin, M.R.; Sharman, M.J.; Gómez, A.L.; Ratamess, N.A.; Newton, R.U.; Jemiolo, B.; Craig, B.W.; et al. The Effects of L-Carnitine L-Tartrate Supplementation on Hormonal Responses to Resistance Exercise and Recovery. J. Strength Cond. Res. 2003, 17, 455–462. [Google Scholar] [CrossRef] [PubMed]
- Cinar, V.; Polat, Y.; Baltaci, A.K.; Mogulkoc, R. Effects of Magnesium Supplementation on Testosterone Levels of Athletes and Sedentary Subjects at Rest and after Exhaustion. Biol. Trace Elem. Res. 2011, 140, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Shafiei Neek, L.; Gaeini, A.A.; Choobineh, S. Effect of Zinc and Selenium Supplementation on Serum Testosterone and Plasma Lactate in Cyclist after an Exhaustive Exercise Bout. Biol. Trace Elem. Res. 2011, 144, 454–462. [Google Scholar] [CrossRef]
- El-Bayoumy, K.; Richie, J.P.; Boyiri, T.; Komninou, D.; Prokopczyk, B.; Trushin, N.; Kleinman, W.; Cox, J.; Pittman, B.; Colosimo, S. Influence of Selenium-Enriched Yeast Supplementation on Biomarkers of Oxidative Damage and Hormone Status in Healthy Adult Males. Cancer Epidemiol. Biomark. Prev. 2002, 11, 1459–1465. [Google Scholar]
- Pandit, S.; Biswas, S.; Jana, U.; De, R.K.; Mukhopadhyay, S.C.; Biswas, T.K. Clinical Evaluation of Purified Shilajit on Testosterone Levels in Healthy Volunteers. Andrologia 2016, 48, 570–575. [Google Scholar] [CrossRef]
- Ruan, J.; Li, Z.; Zhang, Y.; Chen, Y.; Liu, M.; Han, L.; Zhang, Y.; Wang, T. Bioactive Constituents from the Roots of Eurycoma Longifolia. Molecules 2019, 24, 3157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Low, B.-S.; Choi, S.-B.; Abdul Wahab, H.; Das, P.K.; Chan, K.-L. Eurycomanone, the Major Quassinoid in Eurycoma Longifolia Root Extract Increases Spermatogenesis by Inhibiting the Activity of Phosphodiesterase and Aromatase in Steroidogenesis. J. Ethnopharmacol. 2013, 149, 201–207. [Google Scholar] [CrossRef]
- Henkel, R.R.; Wang, R.; Bassett, S.H.; Chen, T.; Liu, N.; Zhu, Y.; Tambi, M.I. Tongkat Ali as a Potential Herbal Supplement for Physically Active Male and Female Seniors—A Pilot Study. Phytother. Res. PTR 2014, 28, 544–550. [Google Scholar] [CrossRef] [PubMed]
- Leitão, A.E.; Vieira, M.D.C.S.; Gomes, D.A.; Boing, L.; Pelegrini, A.; Luiz, E.; de Azevedo Guimarães, A.C. Exercise Associated or Not to the Intake of Eurycoma Longifolia Improves Strength and Cardiorespiratory Fitness in Men with Androgen Deficiency. Complement. Ther. Clin. Pract. 2021, 42, 101301. [Google Scholar] [CrossRef] [PubMed]
- Talbott, S.M.; Talbott, J.A.; George, A.; Pugh, M. Effect of Tongkat Ali on Stress Hormones and Psychological Mood State in Moderately Stressed Subjects. J. Int. Soc. Sports Nutr. 2013, 10, 28. [Google Scholar] [CrossRef] [Green Version]
- Chan, K.Q.; Stewart, C.; Chester, N.; Hamzah, S.H.; Yusof, A. The Effect of Eurycoma Longifolia on the Regulation of Reproductive Hormones in Young Males. Andrologia 2021, 53, e14001. [Google Scholar] [CrossRef] [PubMed]
- Strauch, G.; Perles, P.; Vergult, G.; Gabriel, M.; Gibelin, B.; Cummings, S.; Malbecq, W.; Malice, M.P. Comparison of Finasteride (Proscar) and Serenoa Repens (Permixon) in the Inhibition of 5-Alpha Reductase in Healthy Male Volunteers. Eur. Urol. 1994, 26, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Bello, M.; Guadarrama-García, C.; Velasco-Silveyra, L.M.; Farfán-García, E.D.; Soriano-Ursúa, M.A. Several Effects of Boron Are Induced by Uncoupling Steroid Hormones from Their Transporters in Blood. Med. Hypotheses 2018, 118, 78–83. [Google Scholar] [CrossRef]
- Naghii, M.R.; Mofid, M.; Asgari, A.R.; Hedayati, M.; Daneshpour, M.-S. Comparative Effects of Daily and Weekly Boron Supplementation on Plasma Steroid Hormones and Proinflammatory Cytokines. J. Trace Elem. Med. Biol. Organ Soc. Miner. Trace Elem. (GMS) 2011, 25, 54–58. [Google Scholar] [CrossRef]
- Naghii, M.R.; Samman, S. The Effect of Boron Supplementation on Its Urinary Excretion and Selected Cardiovascular Risk Factors in Healthy Male Subjects. Biol. Trace Elem. Res. 1997, 56, 273–286. [Google Scholar] [CrossRef]
- Smith, S.J.; Lopresti, A.L.; Teo, S.Y.M.; Fairchild, T.J. Examining the Effects of Herbs on Testosterone Concentrations in Men: A Systematic Review. Adv. Nutr. 2020. [Google Scholar] [CrossRef]
- Lopresti, A.L.; Smith, S.J.; Malvi, H.; Kodgule, R. An Investigation into the Stress-Relieving and Pharmacological Actions of an Ashwagandha (Withania Somnifera) Extract: A Randomized, Double-Blind, Placebo-Controlled Study. Medicine 2019, 98, e17186. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, S.M.; Ko, N.K.; Sattar, A.S.; Ipek, E.G.; Ali, S. Pulmonary Embolism Secondary to Testosterone-Enhancing Herbal Supplement Use. Cureus 2017, 9, e1545. [Google Scholar] [CrossRef] [Green Version]
- Wilborn, C.; Taylor, L.; Poole, C.; Foster, C.; Willoughby, D.; Kreider, R. Effects of a Purported Aromatase and 5α-Reductase Inhibitor on Hormone Profiles in College-Age Men. Int. J. Sport Nutr. Exerc. Metab. 2010, 20, 457–465. [Google Scholar] [CrossRef]
- Rao, A.J.; Mallard, A.R.; Grant, R. Testofen® (Fenugreek Extract) Increases Strength and Muscle Mass Compared to Placebo in Response to Calisthenics. A Randomized Control Trial. Transl. Sports Med. 2020, 3, 374–380. [Google Scholar] [CrossRef]
- Wankhede, S.; Mohan, V.; Thakurdesai, P. Beneficial Effects of Fenugreek Glycoside Supplementation in Male Subjects during Resistance Training: A Randomized Controlled Pilot Study. J. Sport Health Sci. 2016, 5, 176–182. [Google Scholar] [CrossRef] [Green Version]
- Mokashi, M.; Singh-Mokashi, R.; Mohan, V.; Thakurdesai, P. Effects of Glycosides based Fenugreek Seed Extract on Serum Testosterone Levels of Healthy Sedentary Male Subjects: A Exploratory Double Blind, Placebo Controlled, Crossover Study. Asian J. Pharm. Clin. Res. 2014, 7, 177–181. [Google Scholar]
- Maheshwari, A.; Verma, N.; Swaroop, A.; Bagchi, M.; Preuss, H.G.; Tiwari, K.; Bagchi, D. Efficacy of FurosapTM, a Novel Trigonella Foenum-Graecum Seed Extract, in Enhancing Testosterone Level and Improving Sperm Profile in Male Volunteers. Int. J. Med. Sci. 2017, 14, 58–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mansoori, A.; Hosseini, S.; Zilaee, M.; Hormoznejad, R.; Fathi, M. Effect of Fenugreek Extract Supplement on Testosterone Levels in Male: A Meta-Analysis of Clinical Trials. Phytother. Res. PTR 2020, 34, 1550–1555. [Google Scholar] [CrossRef] [PubMed]
- Shukla, K.K.; Mahdi, A.A.; Ahmad, M.K.; Shankhwar, S.N.; Rajender, S.; Jaiswar, S.P. Mucuna Pruriens Improves Male Fertility by Its Action on the Hypothalamus-Pituitary-Gonadal Axis. Fertil. Steril. 2009, 92, 1934–1940. [Google Scholar] [CrossRef] [PubMed]
- Saylam, B.; Çayan, S. Do Antioxidants Improve Serum Sex Hormones and Total Motile Sperm Count in Idiopathic Infertile Men? Turk. J. Urol. 2020, 46, 442–448. [Google Scholar] [CrossRef]
- Chaing, H.S.; Merino-chavez, G.; Yang, L.L.; Wang, F.N.; Hafez, E.S. Medicinal Plants: Conception/Contraception. Adv. Contracept. Deliv. Syst. CDS 1994, 10, 355–363. [Google Scholar] [PubMed]
- Lopresti, A.L.; Drummond, P.D.; Smith, S.J. A Randomized, Double-Blind, Placebo-Controlled, Crossover Study Examining the Hormonal and Vitality Effects of Ashwagandha (Withania Somnifera) in Aging, Overweight Males. Am. J. Men’s Health 2019, 13, 1557988319835985. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Qarawi, A.A.; Abdel-Rahman, H.A.; El-Badry, A.A.; Harraz, F.; Razig, N.A.; Abdel-Magied, E.M. The Effect of Extracts of Cynomorium Coccineum and Withania Somnifera on Gonadotrophins and Ovarian Follicles of Immature Wistar Rats. Phytother. Res. PTR 2000, 14, 288–290. [Google Scholar] [CrossRef]
- Mishra, L.C.; Singh, B.B.; Dagenais, S. Scientific Basis for the Therapeutic Use of Withania Somnifera (Ashwagandha): A Review. Altern. Med. Rev. J. Clin. Ther. 2000, 5, 334–346. [Google Scholar]
- Almaiman, A.A. Effect of Testosterone Boosters on Body Functions: Case Report. Int. J. Health Sci. 2018, 12, 86–90. [Google Scholar]
- Wargo, K.A.; Allman, E.; Ibrahim, F. A Possible Case of Saw Palmetto-Induced Pancreatitis. South. Med. J. 2010, 103, 683–685. [Google Scholar] [CrossRef] [PubMed]
- Bui, P.V.; Moualla, M.; Upson, D.J. A Possible Association of Diindolylmethane with Pulmonary Embolism and Deep Venous Thrombosis. Case Rep. Med. 2016, 2016, 7527098. [Google Scholar] [CrossRef] [PubMed]
- Bezuglov, E.; Talibov, O.; Butovskiy, M.; Khaitin, V.; Achkasov, E.; Waśkiewicz, Z.; Lazarev, A. The Inclusion in WADA Prohibited List Is Not Always Supported by Scientific Evidence: A Narrative Review. Asian J. Sports Med. 2021, in press. [Google Scholar] [CrossRef]
- Isenmann, E.; Ambrosio, G.; Joseph, J.F.; Mazzarino, M.; de la Torre, X.; Zimmer, P.; Kazlauskas, R.; Goebel, C.; Botrè, F.; Diel, P.; et al. Ecdysteroids as Non-Conventional Anabolic Agent: Performance Enhancement by Ecdysterone Supplementation in Humans. Arch. Toxicol. 2019, 93, 1807–1816. [Google Scholar] [CrossRef]
- Parr, M.K.; Botrè, F.; Naß, A.; Hengevoss, J.; Diel, P.; Wolber, G. Ecdysteroids: A Novel Class of Anabolic Agents? Biol. Sport 2015, 32, 169–173. [Google Scholar] [CrossRef] [Green Version]
- Gugoasa, L.A.; Staden, R.-I.S. Advanced Methods for the Analysis of Testosterone. Curr. Med. Chem. 2018, 25, 4037–4049. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Study selection process.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Lazarev, A.; Bezuglov, E. Testosterone Boosters Intake in Athletes: Current Evidence and Further Directions. Endocrines 2021, 2, 109-120. https://0-doi-org.brum.beds.ac.uk/10.3390/endocrines2020011
AMA Style
Lazarev A, Bezuglov E. Testosterone Boosters Intake in Athletes: Current Evidence and Further Directions. Endocrines. 2021; 2(2):109-120. https://0-doi-org.brum.beds.ac.uk/10.3390/endocrines2020011
Chicago/Turabian StyleLazarev, Artemii, and Eduard Bezuglov. 2021. "Testosterone Boosters Intake in Athletes: Current Evidence and Further Directions" Endocrines 2, no. 2: 109-120. https://0-doi-org.brum.beds.ac.uk/10.3390/endocrines2020011