
Socioeconomic Differences between Sexes in Surgically Treated Carpal Tunnel Syndrome and Ulnar Nerve Entrapment


Abstract
:1. Introduction
2. Materials and Methods
Statistics
3. Results
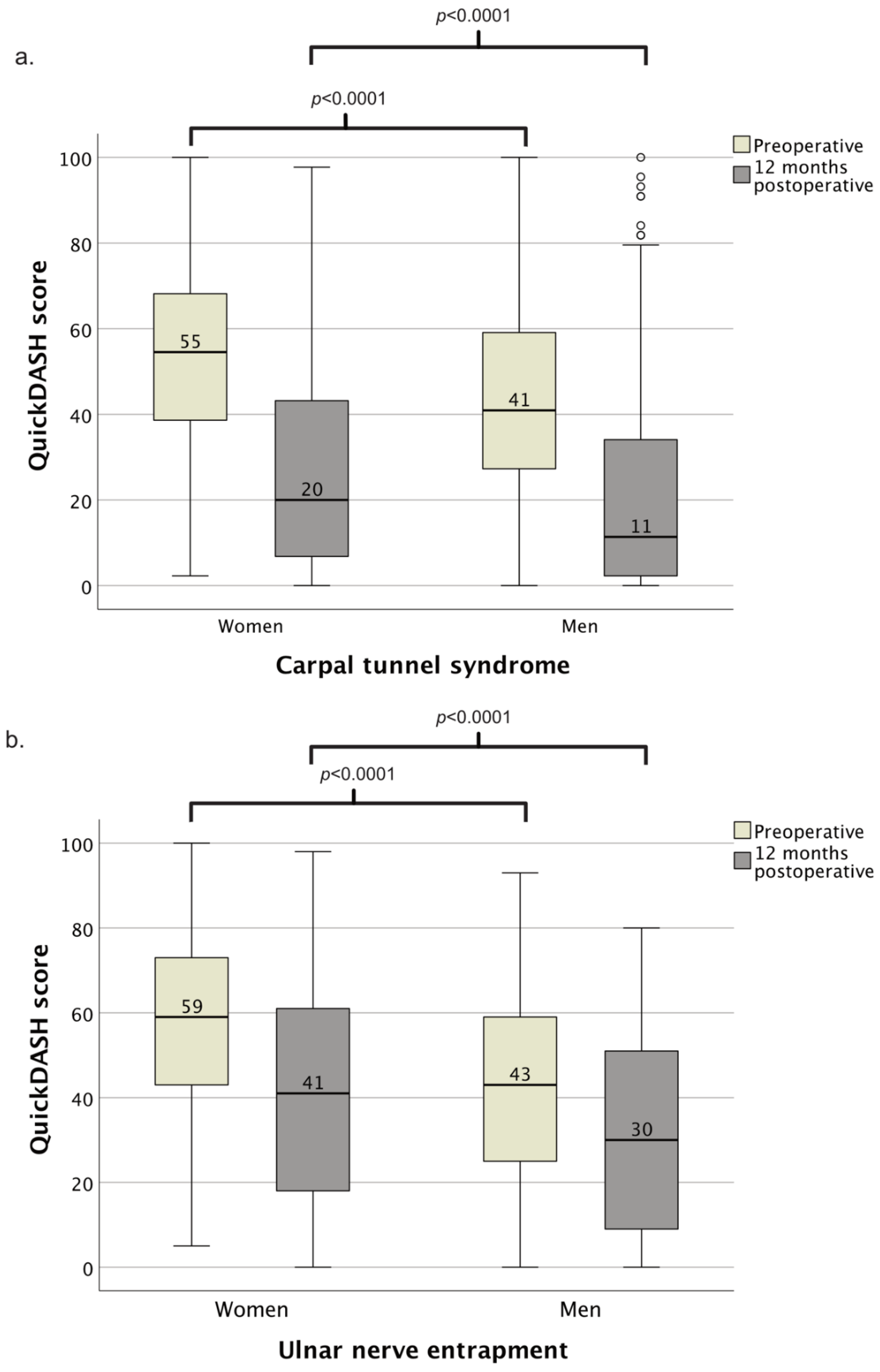
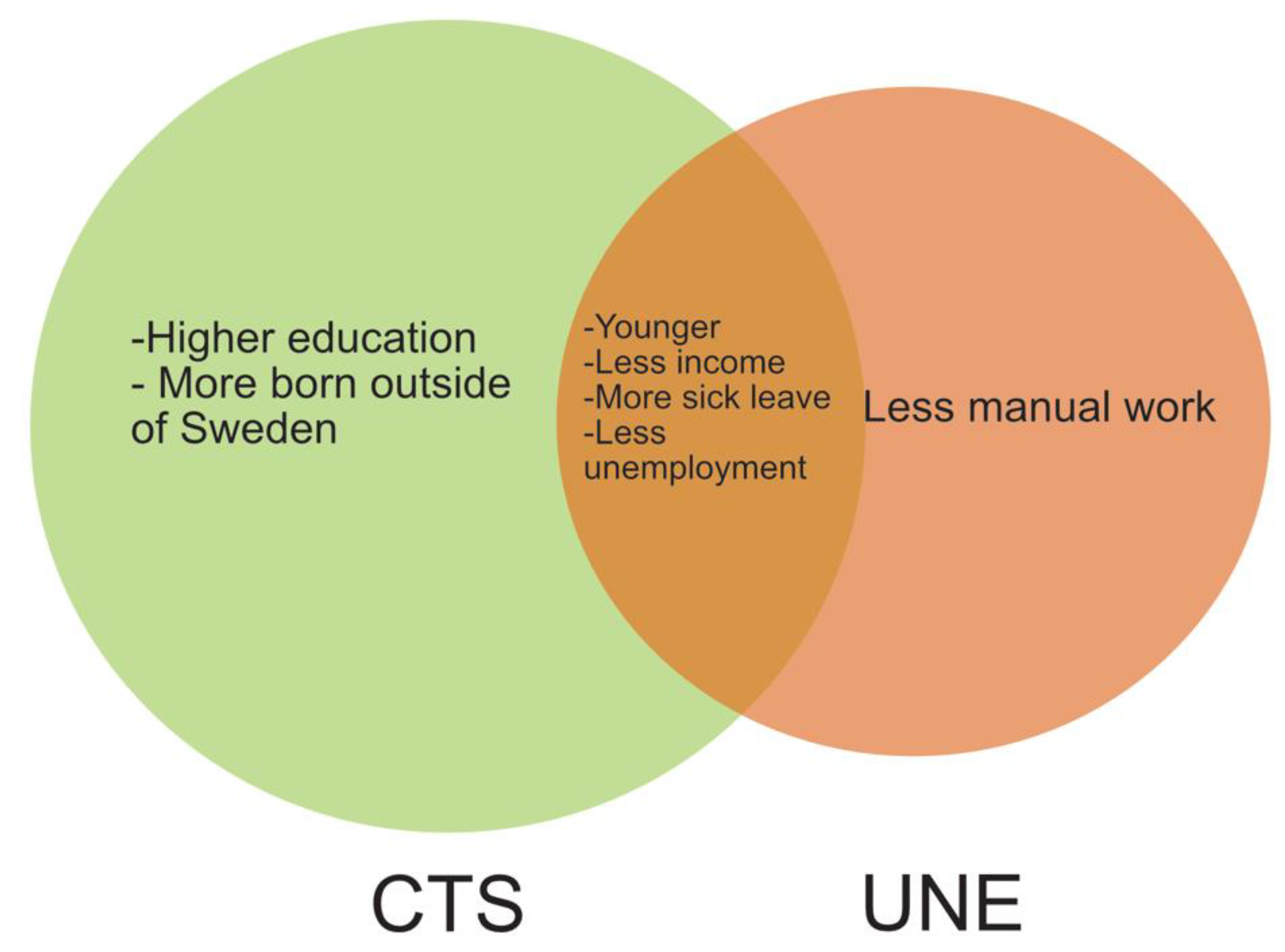
3.1. Carpal Tunnel Syndrome
3.2. Ulnar Nerve Entrapment at the Elbow
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Atroshi, I.; Gummesson, C.; Johnsson, R.; Ornstein, E.; Ranstam, J.; Rosen, I. Prevalence of carpal tunnel syndrome in a general population. JAMA 1999, 282, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Tadjerbashi, K.; Åkesson, A.; Atroshi, I. Incidence of referred carpal tunnel syndrome and carpal tunnel release surgery in the general population: Increase over time and regional variations. J. Orthop. Surg. 2019, 27, 2309499019825572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hobby, J.L.; Venkatesh, R.; Motkur, P. The effect of age and gender upon symptoms and surgical outcomes in carpal tunnel syndrome. J. Hand Surg. Br. 2005, 30, 599–604. [Google Scholar] [CrossRef] [PubMed]
- Padua, L.; Padua, R.; Aprile Tonali, P. Italian multicentre study of carpal tunnel syndrome. Differences in the clinical and neurophysiological features between male and female patients. J. Hand Surg. Br. 1999, 24, 579–582. [Google Scholar] [CrossRef] [PubMed]
- Greenslade, J.R.; Mehta, R.L.; Belward, P.; Warwick, D.J. Dash and Boston questionnaire assessment of carpal tunnel syndrome outcome: What is the responsiveness of an outcome questionnaire? J. Hand Surg. Br. 2004, 29, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Atroshi, I.; Johnsson, R.; Ornstein, E. Patient satisfaction and return to work after endoscopic carpal tunnel surgery. J. Hand Surg. 1998, 23, 58–65. [Google Scholar] [CrossRef]
- Tseng, C.H.; Liao, C.C.; Kuo, C.M.; Sung, F.C.; Hsieh, D.P.; Tsai, C.H. Medical and non-medical correlates of carpal tunnel syndrome in a Taiwan cohort of one million. Eur. J. Neurol. 2012, 19, 91–97. [Google Scholar] [CrossRef]
- Zimmerman, M.; Hall, E.; Carlsson, K.S.; Nyman, E.; Dahlin, L.B. Socioeconomic factors predicting outcome in surgically treated carpal tunnel syndrome: A national registry-based study. Sci. Rep. 2021, 11, 2581. [Google Scholar] [CrossRef]
- Osei, D.A.; Groves, A.P.; Bommarito, K.; Ray, W.Z. Cubital Tunnel Syndrome: Incidence and Demographics in a National Administrative Database. Neurosurgery 2017, 80, 417–420. [Google Scholar] [CrossRef]
- Uzunkulaoğlu, A.; Ikbali Afsar, S.; Karataş, M. Association Between Gender, Body Mass Index, and Ulnar Nerve Entrapment at the Elbow: A Retrospective Study. J. Clin. Neurophysiol. 2016, 33, 545–548. [Google Scholar]
- Shi, Q.; MacDermid, J.; Grewal, R.; King, G.J.; Faber, K.; Miller, T.A. Predictors of Functional Outcome Change 18 Months After Anterior Ulnar Nerve Transposition. Arch. Phys. Med. Rehabil. 2012, 93, 307–312. [Google Scholar] [CrossRef] [PubMed]
- Descatha, A.; Leclerc, A.; Chastang, J.F.; Roquelaure, Y. Incidence of ulnar nerve entrapment at the elbow in repetitive work. Scand. J. Work. Environ. Health 2004, 30, 234–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fadel, M.; Lancigu, R.; Raimbeau, G.; Roquelaure, Y.; Descatha, A. Occupational prognosis factors for ulnar nerve entrapment at the elbow: A systematic review. Hand Surg. Rehabil. 2017, 36, 244–249. [Google Scholar] [CrossRef]
- Bartels, R.H.; Verbeek, A.L. Risk factors for ulnar nerve compression at the elbow: A case control study. Acta Neurochir. 2007, 149, 669–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hulkkonen, S.; Auvinen, J.; Miettunen, J.; Karppinen, J.; Ryhanen, J. Smoking is associated with ulnar nerve entrapment: A birth cohort study. Sci. Rep. 2019, 9, 9450. [Google Scholar] [CrossRef]
- Jensen, A.; Kaerlev, L.; Tüchsen, F.; Hannerz, H.; Dahl, S.; Nielsen, P.S.; Olsen, J. Locomotor diseases among male long-haul truck drivers and other professional drivers. Int. Arch. Occup. Environ. Health 2008, 81, 821–827. [Google Scholar] [CrossRef]
- Afşar, S.İ.; Cetin, N.; Şehri, A.; Mumcu, G.A.; Karataş, M. Ulnar nerve conduction abnormalities in Turkish taxi drivers. Arch. Rheumatol. 2014, 29, 110–117. [Google Scholar] [CrossRef] [Green Version]
- Zimmerman, M.; Nyman, E.; Steen Carlsson, K.; Dahlin, L.B. Socioeconomic Factors in Patients with Ulnar Nerve Compression at the Elbow: A National Registry-Based Study. BioMed Res. Int. 2020, 2020, 5928649. [Google Scholar] [CrossRef]
- Dahlin, E.; Zimmerman, M.; Bjorkman, A.; Thomsen, N.O.; Andersson, G.S.; Dahlin, L.B. Impact of smoking and preoperative electrophysiology on outcome after open carpal tunnel release. J. Plast. Surg. Hand Surg. 2016, 51, 329–335. [Google Scholar] [CrossRef] [Green Version]
- Anker, I.; Zimmerman, M.; Andersson, G.S.; Jacobsson, H.; Dahlin, L. Outcome and predictors in simple decompression of ulnar nerve entrapment at the elbow. J. Hand Microsurg. 2018, 7, 24–32. [Google Scholar] [CrossRef]
- The Swedish Translated Version of QuickDASH. Available online: http://www.dash.iwh.on.ca/assets/images/pdfs/QuickDASH_Swedish.pdf (accessed on 15 January 2019).
- NDR Swedish National Diabetes Register. Available online: www.ndr.nu (accessed on 17 January 2020).
- Eliasson, B.; Gudbjornsdottir, S. Diabetes care—Improvement through measurement. Diabetes Res. Clin. Pract. 2014, 106 (Suppl. 2), S291–S294. [Google Scholar] [CrossRef]
- Hashmi, J.A.; Davis, K.D. Deconstructing sex differences in pain sensitivity. Pain 2014, 155, 10–13. [Google Scholar] [CrossRef] [PubMed]
- Phillips, S.P.; Hammarström, A. Relative health effects of education, socioeconomic status and domestic gender inequity in Sweden: A cohort study. PLoS ONE 2011, 6, e21722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruau, D.; Liu, L.Y.; Clark, J.D.; Angst, M.S.; Butte, A.J. Sex differences in reported pain across 11,000 patients captured in electronic medical records. J. Pain 2012, 13, 228–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitake, T.; Iwatsuki, K.; Hirata, H. Differences in characteristics of carpal tunnel syndrome between male and female patients. J. Orthop. Sci. 2019, 7, 24–32. [Google Scholar] [CrossRef]
- Bowman, A.; Rudolfer, S.; Weller, P.; Bland, J.D.P. A prognostic model for the patient-reported outcome of surgical treatment of carpal tunnel syndrome. Muscle Nerve 2018, 58, 784–789. [Google Scholar]
- Hendrich, J.; Alvarez, P.; Joseph, E.K.; Ferrari, L.F.; Chen, X.; Levine, J.D. In vivo and in vitro comparison of female and male nociceptors. J. Pain 2012, 13, 1224–1231. [Google Scholar] [CrossRef] [Green Version]
- Socialstyrelsen. Statistikdatabas för Ekonomiskt Bistånd. Available online: https://sdb.socialstyrelsen.se/if_ekb/val.aspx (accessed on 8 December 2021).
- Försäkringskassan. Statistikdatabas. 2021. Available online: https://www.forsakringskassan.se/statistik/statistikdatabas/!ut/p/z1/hY45D4JAFIR_iwUt73EZYkcgnGI8I25jwKwLZmEJIPx9CdqYeEw3k28yAwQSIFXaFyztClGlfPQnMj-ba1_3Q1RjdCMVN7HtmcYh0Bxbh-ME4BdZCORfn0yI7ju24tkYeWHgorXfroxAjRXcaS_gx0QIhHGRPe9aVaaZDEhDr7ShjXxvxjjvurpdSCjhMAwyE4JxKl9EKeGnSi7aDpJ3EuoywZvB-6U1mz0AEA_DBw!!/#!/sjuk (accessed on 2 November 2021).
- Socialstyrelsen. Statistikdatabasen 2021. Available online: https://www.socialstyrelsen.se/statistik-och-data/statistik/statistikdatabasen/ (accessed on 1 December 2021).
- Kjellsson, S. Do working conditions contribute differently to gender gaps in self-rated health within different occupational classes? Evidence from the Swedish Level of Living Survey. PLoS ONE 2021, 16, e0253119. [Google Scholar] [CrossRef]
- Boniol, M.; McIsaac, M.; Xu, L.; Wuliji, T.; Diallo, K.; Campbell, J. Gender Equity in the Health Workforce: Analysis of 104 Countries; World Health Organization: Geneva, Switzerland, 2019.
- Nulty, D.D. The adequacy of response rate to online and paper survey: What can be done? Assess. Eval. High. Educ. 2008, 33, 301–314. [Google Scholar] [CrossRef] [Green Version]
- Asch, D.A.; Jedrziewski, M.K.; Christakis, N.A. Response rates to mail surveys published in medical journals. J. Clin. Epidemiol. 1997, 50, 1129–1136. [Google Scholar] [CrossRef]
- Zimmerman, M.; Eeg-Olofsson, K.; Svensson, A.; Astrom, M.; Arner, M.; Dahlin, L. Open carpal tunnel release and diabetes: A retrospective study using PROMs and national quality registries. BMJ Open 2019, 9, e030179. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Women (n = 5988) | Men (n = 3012) | p-Value | |
|---|---|---|---|
| Age (years; mean, 95% CI) | 55 (55–56) | 59 (58–60) | <0.0001 |
| Diabetes at surgery (n, %) | 715 (12) | 544 (18) | <0.0001 |
| Tertiary education (n, %) | 2827 (47) | 1164 (39) | <0.0001 |
| Mean annual earnings, SEK 1000 (mean, 95% CI) | 174 (171–177) | 248 (243–254) | <0.0001 |
| Born outside Sweden (n, %) | 1108 (19) | 403 (13) | <0.0001 |
| Manual occupation (n, %) | 2288 (38) | 1203 (40) | 0.001 |
| Unemployed days (mean/year; mean, 95% CI) | 12 (12–13) | 14 (13–15) | 0.001 |
| Social assistance (total amount; SEK 100, mean, 95% CI) | 212 (185–239) | 173 (134–211) | <0.001 |
| Sick leave (mean days/employed year; mean, 95% CI) | 42 (38–45) | 24 (22–26) | <0.0001 |
| Preoperative QuickDASH score (median, IQR) | 55 (39–68) n = 2342 | 43 (27–59) n = 1241 | <0.0001 |
| Postoperative QuickDASH score at 12 months (median, IQR) | 20 (5–41) n = 1379 | 11 (2–34) n = 653 | <0.0001 |
| Women (n = 556) | Men (n = 270) | |||
|---|---|---|---|---|
| Unstandardized B-Coefficient (95% Confidence Interval) | p-Value | Unstandardized B-Coefficient (95% Confidence Interval) | p-Value | |
| Age at surgery (years) | 0.13 (−0.06–0.33) | 0.17 | −0.18 (−0.45–0.13) | 0.25 |
| Diabetes at surgery | 3.4 (−2.0–8.7) | 0.22 | 2.3 (−4.5–9.1) | 0.51 |
| Migrant status | ||||
| Born in Sweden (reference) | ||||
| Born outside Sweden | 8.5 (3.1–13.8) | 0.002 | −0.01 (−9.1–9.0) | 1.0 |
| Occupation | ||||
| Nonmanual work (reference) | ||||
| Manual work | −1.6 (−6.2–3.0) | 0.49 | −0.3 (−7.8–7.1) | 0.93 |
| Level of education | ||||
| Low (reference) | ||||
| Middle | −4.9 (−10.3–0.3) | 0.07 | −3.4 (−9.8–2.9) | 0.29 |
| High | −10.5 (−16.2–−4.8) | <0.001 | −0.75 (−8.2–6.7) | 0.84 |
| Earnings (mean/year) | ||||
| ≤39,100 (reference) | ||||
| 39,200–183,100 | −6.9 (−13.1–−0.7) | 0.029 | −7.5 (−18.6–3.6) | 0.18 |
| 183,200–280,700 | −7.1 (−14.0–−0.2) | 0.045 | −13.3 (−24.7–−1.9) | 0.022 |
| >280,800 | −10.3 (−18.5–−2.1) | 0.014 | −16.5 (−28.6–−4.4) | 0.008 |
| Social assistance (total amount, SEK 100) | 0.007 (0.0–0.01) | 0.052 | 0.008 (0.0–0.02) | 0.056 |
| Unemployment (mean days/year) | 0.065 (−0.038–0.17) | 0.22 | −0.08 (−0.23–0.06) | 0.26 |
| Sick leave (mean days/year) | 0.06 (0.02–0.1) | 0.003 | 0.10 (0.02–0.18) | 0.019 |
| Women (n = 604) | Men (n = 662) | p-Value | |
|---|---|---|---|
| Age (years; mean, 95% CI) | 51 (40–52) | 53 (52–54) | 0.004 |
| Diabetes at surgery (n, %) | 57 (9) | 91 (14) | 0.018 |
| Tertiary education (n, %) | 161 (27) | 146 (22) | 0.066 |
| Mean annual earnings, SEK 1000 (mean, 95% CI) | 148 (138–159) | 206 (197–220) | <0.0001 |
| Born outside Sweden (n, %) | 101 (17) | 113 (17) | 0.88 |
| Manual occupation (n, %) | 215 (36) | 275 (42) | 0.033 |
| Unemployed days (mean/year; mean, 95% CI) | 17 (15–19) | 21 (18–23) | 0.027 |
| Social assistance (total amount, SEK 100, mean, 95% CI) | 581 (406–756) | 376 (264–488) | 0.021 |
| Sick leave (mean days/employed year, mean, 95% CI) | 33 (30–36) | 23 (21–26) | <0.0001 |
| Preoperative QuickDASH score (median, IQR) | 59 (43–73) (n = 199) | 43 (25–59) (n = 227) | <0.001 |
| Postoperative QuickDASH score at 12 months (median, IQR) | 41 (18–61) (n = 161) | 30 (9–52) (n = 140) | 0.002 |
| Women (n = 122) | Men (n = 110) | |||
|---|---|---|---|---|
| Unadjusted B- Coefficient (95% ConfidenceInterval) | p-Value | Unadjusted B- Coefficient (95% Confidence Interval) | p-Value | |
| Age at surgery (years) | 0.2 (−0.2–0.7) | 0.34 | 0.60 (0.06–1.1) | 0.031 |
| Diabetes at surgery | −11.5 (−27.3–4.2) | 0.15 | 8.4 (−2.8–19.7) | 0.14 |
| Migrant status | ||||
| Born in Sweden (reference) | ||||
| Born outside Sweden | −0.35 (−15.6–14.9) | 0.15 | −0.29 (−14.1–13.6) | 0.97 |
| Occupation | ||||
| Non-manual work (reference) | ||||
| Manual work | −8.9 (−19.1–1.4) | 0.089 | 5.4 (−4.1–15.0) | 0.26 |
| Level of education | ||||
| Low (reference) | ||||
| Middle | −3.4 (−14.9–8.1) | 0.57 | 2.7 (−9.1–14.6) | 0.65 |
| High | −9.3 (−22.7–4.2) | 0.18 | −4.5 (−17.8–8.7) | 0.50 |
| Earnings (mean/year) | ||||
| ≤39,100 (reference) | ||||
| 39,200–183,100 | −10.9 (−26.5–4.6) | 0.14 | 1.6 (−18.2–21.4) | 0.87 |
| 183,200–280,700 | −9.7 (−26.5–7.1) | 0.25 | 7.0 (−12.5–26.5) | 0.48 |
| >280,800 | −16.7 (−34.0- 0.7) | 0.06 | 3.6 (−15.1–22.3) | 0.70 |
| Social assistance (total amount, SEK 100) | 0.5 (−0.9–1.8) | 0.49 | 1.0 (−0.52–2.6) | 0.19 |
| Unemployment (mean days/year) | 0.01 (−0.27–0.29) | 0.93 | −0.02 (−0.2–0.2) | 0.85 |
| Sick leave (mean days/year) | 0.14 (−0.02–0.29) | 0.084 | 0.25 (0.09–0.4) | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zimmerman, M.; Anker, I.; Nyman, E. Socioeconomic Differences between Sexes in Surgically Treated Carpal Tunnel Syndrome and Ulnar Nerve Entrapment. Epidemiologia 2022, 3, 353-362. https://0-doi-org.brum.beds.ac.uk/10.3390/epidemiologia3030027
Zimmerman M, Anker I, Nyman E. Socioeconomic Differences between Sexes in Surgically Treated Carpal Tunnel Syndrome and Ulnar Nerve Entrapment. Epidemiologia. 2022; 3(3):353-362. https://0-doi-org.brum.beds.ac.uk/10.3390/epidemiologia3030027
Chicago/Turabian StyleZimmerman, Malin, Ilka Anker, and Erika Nyman. 2022. "Socioeconomic Differences between Sexes in Surgically Treated Carpal Tunnel Syndrome and Ulnar Nerve Entrapment" Epidemiologia 3, no. 3: 353-362. https://0-doi-org.brum.beds.ac.uk/10.3390/epidemiologia3030027