
Rural-Urban Differences in Prevalence and Associated Factors of Underweight and Overweight/Obesity among Bangladeshi Adults: Evidence from Bangladesh Demographic and Health Survey 2017–2018

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
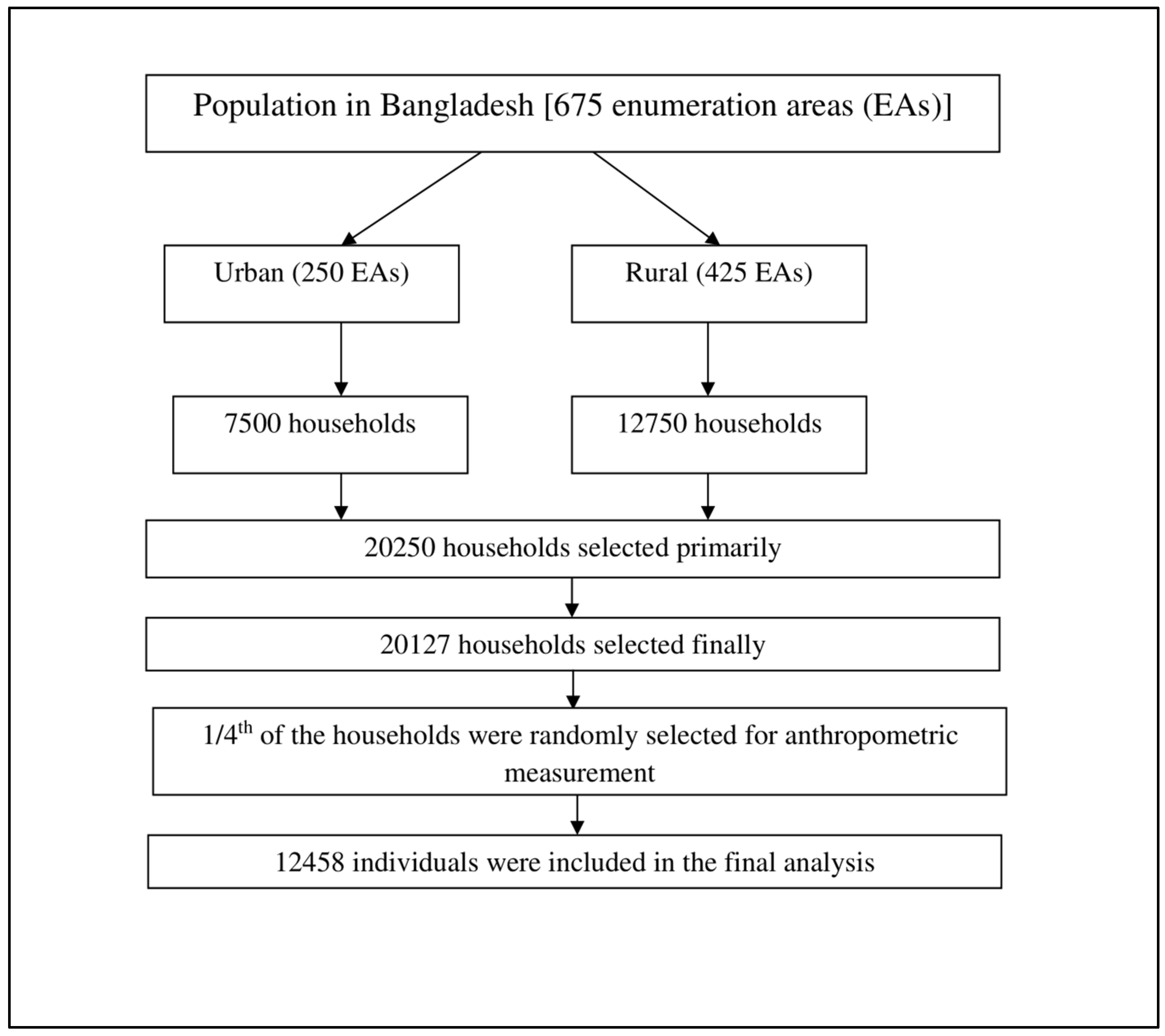
2.1. Study Design
2.2. Data Collection Tools
2.3. Data Collection
2.4. Outcome of Interest
2.5. Explanatory Variables
2.6. Statistical Analysis
- Log(Odds of Underweight) = β1*Age_30–49 + β2*Age_50–69 + β3*Age_70+ + β4*Education_Primary + β5*Education_Secondary + β6*Education_CollegeAndHigher + β7*WealthIndex_Poorer + β8*WealthIndex_Middle + β9*WealthIndex_Richer + β10*WealthIndex_Richest + β11*CurrentWorkingStatus_Yes + β12*DivisionOfResidence_Chattogram + β13*DivisionOfResidence_Dhaka + β14*DivisionOfResidence_Khulna + β15*DivisionOfResidence_Mymensingh + β16*DivisionOfResidence_Rajshahi + β17*DivisionOfResidence_Rangpur + β18*DivisionOfResidence_Sylhet + β19*MaritalStatus_CurrentlyMarried + β20*MaritalStatus_SeparatedDivorcedWidowed
- Log(Odds of Overweight/Obesity) = β1*Age_30–49 + β2*Age_50–69 + β3*Age_70+ + β4*Sex_Female + β5*Education_Primary + β6*Education_Secondary + β7*Education_CollegeAndHigher + β8*WealthIndex_Poorer + β9*WealthIndex_Middle + β10*WealthIndex_Richer + β11*WealthIndex_Richest + β12*CurrentWorkingStatus_Yes + β13*DivisionOfResidence_Chattogram + β14*DivisionOfResidence_Dhaka + β15*DivisionOfResidence_Khulna + β16*DivisionOfResidence_Mymensingh + β17*DivisionOfResidence_Rajshahi + β18*DivisionOfResidence_Rangpur + β19*DivisionOfResidence_Sylhet + β20*MaritalStatus_CurrentlyMarried + β21*MaritalStatus_SeparatedDivorcedWidowed
- Log(Odds of Underweight) = γ1*Age_30–49 + γ2*Age_50–69 + γ3*Age_70+ + γ4*Education_Primary + γ5*Education_Secondary + γ6*Education_CollegeAndHigher + γ7*WealthIndex_Poorer + γ8*WealthIndex_Middle + γ9*WealthIndex_Richer + γ10*WealthIndex_Richest + γ11*DivisionOfResidence_Chattogram + γ12*DivisionOfResidence_Dhaka + γ13*DivisionOfResidence_Khulna + γ14*DivisionOfResidence_Mymensingh + γ15*DivisionOfResidence_Rajshahi + γ16*DivisionOfResidence_Rangpur + γ17*DivisionOfResidence_Sylhet + γ18*MaritalStatus_CurrentlyMarried + γ19*MaritalStatus_SeparatedDivorcedWidowed
- Log(Odds of Overweight/Obesity) = γ1*Age_30–49 + γ2*Age_50–69 + γ3*Age_70+ + γ4*Sex_Female + γ5*Education_Primary + γ6*Education_Secondary + γ7*Education_CollegeAndHigher + γ8*WealthIndex_Poorer + γ9*WealthIndex_Middle + γ10*WealthIndex_Richer + γ11*WealthIndex_Richest + γ12*CurrentWorkingStatus_Yes + γ13*DivisionOfResidence_Chattogram + γ14*DivisionOfResidence_Dhaka + γ15*DivisionOfResidence_Khulna + γ16*DivisionOfResidence_Mymensingh + γ17*DivisionOfResidence_Rajshahi + γ18*DivisionOfResidence_Rangpur + γ19*DivisionOfResidence_Sylhet + γ20*MaritalStatus_CurrentlyMarried + γ21*MaritalStatus_SeparatedDivorcedWidowed
2.7. Ethical Consideration
3. Results
3.1. Characteristics of the Study Sample
3.2. Factors Associated with Underweight
3.3. Factors Associated with Overweight and Obesity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| BMI Categories | WHO-Cut Off | Asia-Specific Cut Off |
|---|---|---|
| Underweight | <18.5 | <18.5 |
| Normal BMI | 18.5 to <25.0 | 18.5 to <23.0 |
| Overweight | 25.0 to 30.0 | 23.0 to <27.5 |
| Obesity | ≥30.0 | ≥27.5 |
| Variables | Prevalence (%) | Differences (%) | 95% CI, LL | 95% CI, UL | p Value | |
|---|---|---|---|---|---|---|
| Urban | Rural | |||||
| Age (in Years) | ||||||
| 18–29 | 18.7 | 21.7 | −2.9 | −7.7 | 1.8 | 0.228 |
| 30–49 | 9.9 | 17.3 | −7.3 | −9.4 | −5.3 | <0.001 |
| 50–69 | 13.6 | 20.7 | −7.1 | −10.1 | −4.2 | <0.001 |
| 70+ | 12.5 | 21.4 | −8.9 | −15.0 | −2.8 | 0.004 |
| Sex | ||||||
| Male | 14.2 | 22 | −7.7 | −10.3 | −5.2 | <0.001 |
| Female | 10.6 | 17.3 | −6.7 | −8.7 | −4.8 | <0.001 |
| Education | ||||||
| No Formal Schooling | 16.2 | 27.1 | −10.9 | −14.5 | −7.2 | <0.001 |
| Primary | 15.4 | 19.5 | −4.1 | −7.2 | −1.0 | 0.009 |
| Secondary | 9.5 | 14.1 | −4.6 | −7.1 | −2.2 | <0.001 |
| College and Higher | 8.7 | 13.4 | −4.7 | −7.9 | −1.5 | 0.004 |
| Wealth Index | ||||||
| Poorest | 24.2 | 28.5 | −4.3 | −9.5 | 0.9 | 0.104 |
| Poorer | 20 | 22.7 | −2.6 | −7.6 | 2.3 | 0.294 |
| Middle | 16.6 | 16.9 | −0.3 | −4.3 | 3.7 | 0.884 |
| Richer | 13.1 | 12.9 | 0.2 | −3.2 | 3.5 | 0.917 |
| Richest | 7.8 | 7.8 | 0.0 | −2.7 | 2.7 | 0.996 |
| Current Working Status | ||||||
| No | 11.5 | 18.2 | −6.7 | −9.1 | −4.3 | <0.001 |
| Yes | 12.7 | 20 | −7.3 | −9.4 | −5.1 | <0.001 |
| Division of Residence | ||||||
| Barisal | 11.2 | 18 | −6.8 | −11.7 | −1.9 | 0.007 |
| Chittagong | 13.6 | 13.9 | −0.3 | −3.9 | 3.4 | 0.89 |
| Dhaka | 10.7 | 20.8 | −10.1 | −15.1 | −5.0 | <0.001 |
| Khulna | 11.3 | 16.2 | −4.9 | −8.5 | −1.3 | 0.008 |
| Mymensingh | 14.9 | 27.4 | −12.5 | −17.9 | −7.1 | <0.001 |
| Rajshahi | 12.8 | 19.5 | −6.7 | −11.8 | −1.6 | 0.01 |
| Rangpur | 12.6 | 20.2 | −7.7 | −12.4 | −2.9 | 0.002 |
| Sylhet | 19.8 | 23.1 | −3.3 | −9.2 | 2.6 | 0.268 |
| Marital Status | ||||||
| Never Married | 23.1 | 26.4 | −3.2 | −8.9 | 2.4 | 0.256 |
| Currently Married | 10.1 | 17.9 | −7.8 | −9.5 | −6.1 | <0.001 |
| Separated/Divorced/Widowed | 17.2 | 24.8 | −7.7 | −12.8 | −2.5 | 0.004 |
| Variables | Prevalence (%) | Differences (%) | 95% CI, LL | 95% CI, UL | p Value | |
|---|---|---|---|---|---|---|
| Urban | Rural | |||||
| Age (in Years) | ||||||
| 18–29 | 38 | 28.1 | 9.9 | 2.5 | 17.2 | 0.009 |
| 30–49 | 53.8 | 37.5 | 16.3 | 12.8 | 19.8 | <0.001 |
| 50–69 | 49.7 | 35.5 | 14.2 | 10.1 | 18.2 | <0.001 |
| 70+ | 45.4 | 38.1 | 7.3 | −1.6 | 16.3 | 0.108 |
| Sex | ||||||
| Male | 42.2 | 28.9 | 13.2 | 9.5 | 17.0 | <0.001 |
| Female | 57.1 | 41.4 | 15.6 | 12.7 | 18.5 | <0.001 |
| Education | 0.0 | 0.0 | 0.0 | <0.001 | ||
| No Formal Schooling | 40.5 | 25.3 | 15.2 | 10.8 | 19.6 | <0.001 |
| Primary | 41.8 | 34.7 | 7.2 | 3.0 | 11.3 | 0.001 |
| Secondary | 54.6 | 44 | 10.6 | 6.2 | 15.0 | <0.001 |
| College and Higher | 63.2 | 45 | 18.2 | 12.9 | 23.5 | <0.001 |
| Wealth Index | ||||||
| Poorest | 24.6 | 23 | 1.6 | −4.6 | 7.7 | 0.618 |
| Poorer | 32.1 | 27.4 | 4.7 | −2.0 | 11.4 | 0.169 |
| Middle | 39 | 37.2 | 1.8 | −2.9 | 6.5 | 0.445 |
| Richer | 43.3 | 46.3 | −3.0 | −8.7 | 2.8 | 0.31 |
| Richest | 63.4 | 62.9 | 0.5 | −4.5 | 5.4 | 0.858 |
| Current Working Status | ||||||
| No | 57.6 | 39.2 | 18.4 | 14.7 | 22.0 | <0.001 |
| Yes | 45 | 34 | 10.9 | 7.8 | 14.1 | <0.001 |
| Division of Residence | ||||||
| Barisal | 53.6 | 36.4 | 17.2 | 8.1 | 26.4 | <0.001 |
| Chittagong | 49.8 | 44.6 | 5.3 | −1.5 | 12.0 | 0.127 |
| Dhaka | 52.8 | 38.3 | 14.5 | 7.8 | 21.2 | <0.001 |
| Khulna | 53.7 | 41.5 | 12.1 | 6.3 | 18.0 | <0.001 |
| Mymensingh | 41.4 | 26.3 | 15.1 | 5.8 | 24.5 | 0.002 |
| Rajshahi | 46.1 | 33.3 | 12.9 | 5.3 | 20.4 | 0.001 |
| Rangpur | 49.5 | 30.3 | 19.2 | 10.3 | 28.0 | <0.001 |
| Sylhet | 37.5 | 29.7 | 7.8 | 1.1 | 14.5 | 0.024 |
| Marital Status | ||||||
| Never Married | 29.8 | 23.1 | 6.8 | 0.7 | 12.8 | 0.028 |
| Currently Married | 53.8 | 38.5 | 15.4 | 12.5 | 18.3 | <0.001 |
| Separated/Divorced/Widowed | 45.5 | 27.5 | 18.0 | 11.8 | 24.2 | <0.001 |
References
- Blüher, M. Obesity: Global epidemiology and pathogenesis. Nat. Rev. Endocrinol. 2019, 15, 288–298. [Google Scholar] [CrossRef]
- Lahey, R.; Khan, S.S. Trends in Obesity and Risk of Cardiovascular Disease. Curr. Epidemiol. Rep. 2018, 5, 243–251. [Google Scholar] [CrossRef] [PubMed]
- Abdelaal, M.; le Roux, C.W.; Docherty, N.G. Morbidity and mortality associated with obesity. Ann. Transl. Med. 2017, 5, 161. [Google Scholar] [CrossRef] [PubMed]
- Bentham, J.; Di Cesare, M.; Bilano, V.; Lynne, M. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar]
- Hashan, M.R.; Das Gupta, R.; Day, B.; Al Kibria, G.M. Differences in prevalence and associated factors of underweight and overweight/obesity according to rural-urban residence strata among women of reproductive age in Bangladesh: Evidence from a cross-sectional national survey. BMJ Open 2020, 10, e034321. [Google Scholar] [CrossRef] [PubMed]
- Abdullah, A. The Double Burden of Undernutrition and Overnutrition in Developing Countries: An Update. Curr. Obes. Rep. 2015, 4, 337–349. [Google Scholar] [CrossRef] [PubMed]
- Matrins, V.J.B.; Toledo Florêncio, T.M.M.; Grillo, L.P.; Franco, M.D.C.P.; Martins, P.A.; Clemente, A.P.G.; Santos, C.D.L.; Vieira, M.d.F.A.; Sawaya, A.L. Long-lasting effects of undernutrition. Int. J. Environ. Res. Public Health 2011, 8, 1817–1846. [Google Scholar]
- World Bank. GDP Growth (Annual %)-Bangladesh|Data; World Bank Natl. Accounts Data, OECD Natl. Accounts Data Files; World Bank: Washington, DC, USA, 2021. [Google Scholar]
- Kuddus, M.A.; Tynan, E.; McBryde, E. Urbanization: A problem for the rich and the poor? Public Health Rev. 2020, 41, 1. [Google Scholar] [CrossRef] [PubMed]
- Joarder, T.; Sutradhar, I.; Hasan, M.I.; Bulbul, M.M.I. A Record Review on the Health Status of Rohingya Refugees in Bangladesh. Cureus 2020, 12, 6–13. [Google Scholar] [CrossRef]
- National Institute of Population Research and Training (NIPORT); ICF. Bangladesh Demographic and Health Survey 2017–18; National Institute of Population Research and Training (NIPORT): Dhaka, Bangladesh; ICF: Rockville, MD, USA, 2020. [Google Scholar]
- Tan, K.C.B. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 2004, 363, 157–163. [Google Scholar]
- Das Gupta, R.; Al Kibria, G.M. Prevalence and Associated Factors of Underweight, Overweight, and Obesity among Bangladeshi Adults: An Analysis of Demographic and Health Survey 2017–18. Obes. Med. 2021, 23, 100342. [Google Scholar] [CrossRef]
- Hashan, M.R.; Rabbi, M.F.; Haider, S.S.; Das Gupta, R. Prevalence and associated factors of underweight, overweight and obesity among women of reproductive age group in the Maldives: Evidence from a nationally representative study. PLoS ONE 2020, 15, e0241621. [Google Scholar] [CrossRef]
- Jolliffe, I.T.; Cadima, J. Principal component analysis: A review and recent developments. Philos. Trans. R. Soc. A Math. Phys. Eng. Sci. 2016, 374, 20150202. [Google Scholar] [CrossRef]
- Filmer, D.; Pritchett, L.H. Estimating wealth effects without expenditure data—Or tears: An application to educational enrollments in states of India. Demography 2001, 38, 115–132. [Google Scholar]
- Kolenikov, S.; Angeles, G. Socioeconomic status measurement with discrete proxy variables: Is principal component analysis a reliable answer? Rev. Income Wealth 2009, 55, 128–165. [Google Scholar] [CrossRef]
- Jakobsen, J.C.; Gluud, C.; Wetterslev, J.; Winkel, P. When and how should multiple imputation be used for handling missing data in randomised clinical trials–a practical guide with flowcharts. BMC Med. Res. Methodol. 2017, 17, 162. [Google Scholar] [CrossRef]
- Maldonado, G.; Greenland, S. Simulation study of confounder-selection strategies. Am. J. Epidemiol. 1993, 138, 923–936. [Google Scholar] [CrossRef]
- Khan, S.H.; Talukder, S.H. Nutrition transition in Bangladesh: Is the country ready for this double burden. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2013, 14 (Suppl. 2), 126–133. [Google Scholar] [CrossRef]
- Tanumihardjo, S.A.; Anderson, C.; Kaufer-Horwitz, M.; Bode, L.; Emenaker, N.J.; Haqq, A.M.; Satia, J.A.; Silver, H.J.; Stadler, D.D. Poverty, obesity, and malnutrition: An international perspective recognizing the paradox. J. Am. Diet. Assoc. 2007, 107, 1966–1972. [Google Scholar] [CrossRef]
- Das Gupta, R.; Sajal, I.H.; Hasan, M.; Sutradhar, I.; Haider, M.R.; Sarker, M. Frequency of television viewing and association with overweight and obesity among women of the reproductive age group in Myanmar: Results from a nationwide cross-sectional survey. BMJ Open 2019, 9, e024680. [Google Scholar] [CrossRef]
- Osmani, S.R.; Ahmed, T.; Hossain, N.; Huq, S. Strategic Review of Food Security and Nutrition in Bangladesh; World Food Programme: Rome, Italy, 2016. [Google Scholar]
- Luhar, S.; Timæus, I.M.; Jones, R.; Cunningham, S.; Patel, S.A.; Kinra, S.; Clarke, L.; Houben, R. Forecasting the prevalence of overweight and obesity in India to 2040. PLoS ONE 2020, 15, e0229438. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Wu, W.; Mao, Z.; Huo, W.; Tu, R.; Qian, X.; Zhang, X.; Tian, Z.; Zhang, H.; Jiang, J.; et al. Prevalence and influencing factors of overweight and obesity in a Chinese rural population: The Henan Rural Cohort Study. Sci. Rep. 2018, 8, 13101. [Google Scholar] [CrossRef] [PubMed]
- Rawal, L.B.; Kanda, K.; Mahumud, R.A.; Joshi, D.; Mehata, S.; Shrestha, N.; Poudel, P.; Karki, S.; Renzaho, A. Prevalence of underweight, overweight and obesity and their associated risk factors in Nepalese adults: Data from a Nationwide Survey, 2016. PLoS ONE 2018, 13, e0205912. [Google Scholar] [CrossRef] [PubMed]
- Kanter, R.; Caballero, B. Global gender disparities in obesity: A review. Adv. Nutr. 2012, 3, 491–498. [Google Scholar] [CrossRef] [PubMed]
- Al Kibria, G.M. Prevalence and factors affecting underweight, overweight and obesity using Asian and World Health Organization cutoffs among adults in Nepal: Analysis of the Demographic and Health Survey 2016. Obes. Res. Clin. Pract. 2019, 13, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Biswas, T.; Magalhaes, R.J.S.; Townsend, N.; Das, S.K.; Mamun, A. Double Burden of Underweight and Overweight among Women in South and Southeast Asia: A Systematic Review and Meta-analysis. Adv. Nutr. 2020, 11, 128–143. [Google Scholar] [CrossRef] [PubMed]
- Mkuu, R.S.; Epnere, K.; Chowdhury, M.A.B. Prevalence and Predictors of Overweight and Obesity among Kenyan Women. Prev. Chronic Dis. 2018, 15, E44. [Google Scholar] [CrossRef]
- Harris-Fry, H.; Azad, K.; Kuddus, A.; Shaha, S.; Nahar, B.; Hossen, M.; Younes, L.; Costello, A.; Fottrell, E. Socio-economic determinants of household food security and women’s dietary diversity in rural Bangladesh: A cross-sectional study. J. Health Popul. Nutr. 2015, 33, 2. [Google Scholar] [CrossRef]
- Biswas, T.; Garnett, S.P.; Pervin, S.; Rawal, L.B. The prevalence of underweight, overweight and obesity in Bangladeshi adults: Data from a national survey. PLoS ONE 2017, 12, e0177395. [Google Scholar] [CrossRef]
- Bari, M.; Islam, M.A.; Imam, M.F.; Hassan, M.F. Intra-Household Food Security Status among Ultra-Poor Communities in Mymensingh District. Bangladesh J. Agric. Econ. 2020, 41, 1–16. [Google Scholar]
- Bangladesh Bureau of Statistics. Poverty Maps of Bangladesh; Bangladesh Bureau of Statistics: Dhaka, Bangladesh, 2016.
- Tanwi, T.S.; Chakrabarty, S.; Hasanuzzaman, S.; Saltmarsh, S.; Winn, S. Socioeconomic correlates of overweight and obesity among ever-married urban women in Bangladesh. BMC Public Health 2019, 19, 842. [Google Scholar] [CrossRef]
- Sobal, J.; Rauschenbach, B.S.; Frongillo, E.A.J. Marital status, fatness and obesity. Soc. Sci. Med. 1992, 35, 915–923. [Google Scholar] [CrossRef]
- Nisbett, N.; Davis, P.; Yosef, S.; Akhtar, N. Bangladesh’s story of change in nutrition: Strong improvements in basic and underlying determinants with an unfinished agenda for direct community level support. Glob. Food Sec. 2017, 13, 21–29. [Google Scholar] [CrossRef]
- NCD Risk Factor Collaboration (NCD-RisC). Diminishing benefits of urban living for children and adolescents’ growth and development. Nature 2023, 615, 874–883. [Google Scholar] [CrossRef]

| Variables | Urban (n = 3412) | Rural (n = 9047) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Underweight | Normal Weight | Overweight/Obesity | Underweight | Normal Weight | Overweight/Obesity | |||||||
| n | % | n | % | n | % | n | % | n | % | n | % | |
| Age (in Years) | ||||||||||||
| 18–29 | 66 | 18.7 | 153 | 43.3 | 134 | 38.0 | 181 | 21.7 | 420 | 50.2 | 235 | 28.1 |
| 30–49 | 168 | 9.9 | 614 | 36.3 | 910 | 53.8 | 695 | 17.3 | 1820 | 45.3 | 1506 | 37.5 |
| 50–69 | 155 | 13.6 | 420 | 36.7 | 569 | 49.7 | 677 | 20.7 | 1431 | 43.8 | 1160 | 35.5 |
| 70+ | 28 | 12.5 | 93 | 42.1 | 100 | 45.4 | 197 | 21.4 | 373 | 40.5 | 351 | 38.1 |
| Sex | ||||||||||||
| Male | 222 | 14.2 | 682 | 43.6 | 659 | 42.2 | 871 | 22.0 | 1947 | 49.1 | 1147 | 28.9 |
| Female | 195 | 10.6 | 599 | 32.4 | 1054 | 57.1 | 879 | 17.3 | 2097 | 41.3 | 2106 | 41.4 |
| Education | ||||||||||||
| No Formal Schooling | 110 | 16.2 | 294 | 43.3 | 275 | 40.5 | 690 | 27.1 | 1212 | 47.6 | 645 | 25.3 |
| Primary | 142 | 15.4 | 393 | 42.8 | 385 | 41.8 | 548 | 19.5 | 1290 | 45.8 | 975 | 34.7 |
| Secondary | 101 | 9.5 | 382 | 36.0 | 580 | 54.6 | 359 | 14.1 | 1069 | 41.9 | 1121 | 44.0 |
| College and Higher | 65 | 8.7 | 211 | 28.1 | 475 | 63.2 | 153 | 13.4 | 473 | 41.6 | 512 | 45.0 |
| Wealth Index | ||||||||||||
| Poorest | 51 | 24.2 | 108 | 51.2 | 52 | 24.6 | 616 | 28.5 | 1046 | 48.5 | 497 | 23.0 |
| Poorer | 46 | 20.0 | 111 | 47.9 | 74 | 32.1 | 498 | 22.7 | 1098 | 49.9 | 603 | 27.4 |
| Middle | 75 | 16.6 | 200 | 44.4 | 176 | 39.0 | 355 | 16.9 | 965 | 45.9 | 781 | 37.2 |
| Richer | 120 | 13.1 | 402 | 43.6 | 399 | 43.3 | 198 | 12.9 | 627 | 40.8 | 711 | 46.3 |
| Richest | 125 | 7.8 | 460 | 28.8 | 1013 | 63.4 | 82 | 7.8 | 307 | 29.2 | 661 | 62.9 |
| Current Working Status | ||||||||||||
| No | 164 | 11.5 | 440 | 30.9 | 819 | 57.6 | 614 | 18.2 | 1436 | 42.6 | 1321 | 39.2 |
| Yes | 253 | 12.7 | 841 | 42.3 | 894 | 45.0 | 1136 | 20.0 | 2608 | 46.0 | 1932 | 34.0 |
| Division of Residence | ||||||||||||
| Barisal | 14 | 11.2 | 44 | 35.2 | 67 | 53.6 | 102 | 18.0 | 258 | 45.6 | 206 | 36.4 |
| Chattogram | 84 | 13.6 | 226 | 36.6 | 308 | 49.8 | 212 | 13.9 | 634 | 41.6 | 680 | 44.6 |
| Dhaka | 153 | 10.7 | 522 | 36.5 | 754 | 52.8 | 322 | 20.8 | 635 | 41.0 | 593 | 38.3 |
| Khulna | 39 | 11.3 | 122 | 35.0 | 187 | 53.7 | 192 | 16.2 | 500 | 42.3 | 491 | 41.5 |
| Mymensingh | 25 | 14.9 | 74 | 43.8 | 70 | 41.4 | 232 | 27.4 | 394 | 46.4 | 223 | 26.3 |
| Rajshahi | 45 | 12.8 | 146 | 41.2 | 163 | 46.1 | 276 | 19.5 | 671 | 47.3 | 472 | 33.3 |
| Rangpur | 28 | 12.6 | 85 | 38.0 | 110 | 49.5 | 260 | 20.2 | 636 | 49.5 | 390 | 30.3 |
| Sylhet | 28 | 19.8 | 62 | 42.8 | 54 | 37.5 | 154 | 23.1 | 315 | 47.3 | 198 | 29.7 |
| Marital Status | ||||||||||||
| Never Married | 96 | 23.1 | 195 | 47.1 | 123 | 29.8 | 223 | 26.4 | 427 | 50.6 | 195 | 23.1 |
| Currently Married | 272 | 10.1 | 978 | 36.1 | 1459 | 53.8 | 1305 | 17.9 | 3191 | 43.7 | 2812 | 38.5 |
| Separated/Divorced/Widowed | 50 | 17.2 | 108 | 37.3 | 131 | 45.5 | 222 | 24.8 | 426 | 47.7 | 246 | 27.5 |
| Variables | Urban | Rural | ||
|---|---|---|---|---|
| AOR (95% CI) | p-Value | AOR (95% CI) | p-Value | |
| Age (in Years) | ||||
| 18–29 | Ref | Ref | ||
| 30–49 | 0.6 (0.4–0.8) | 0.001 | 0.8 (0.7–1.0) | 0.094 |
| 50–69 | 0.8 (0.6–1.1) | 0.104 | 1.1 (0.9–1.3) | 0.521 |
| 70+ | 0.7 (0.4–1.0) | 0.08 | 1.2 (0.9–1.6) | 0.208 |
| Education | ||||
| No Formal Schooling | Ref | Ref | ||
| Primary | 1.0 (0.8–1.3) | 0.887 | 0.8 (0.7–0.9) | 0.001 |
| Secondary | 0.8 (0.6–1.0) | 0.094 | 0.7 (0.5–0.8) | <0.001 |
| College and Higher | 0.6 (0.4–0.9) | 0.019 | 0.6 (0.5–0.8) | <0.001 |
| Wealth Index | ||||
| Poorest | Ref | Ref | ||
| Poorer | 0.9 (0.6–1.4) | 0.768 | 0.8 (0.7–0.9) | 0.007 |
| Middle | 0.8 (0.6–1.2) | 0.254 | 0.7 (0.6–0.8) | <0.001 |
| Richer | 0.6 (0.4–0.8) | 0.001 | 0.6 (0.5–0.7) | <0.001 |
| Richest | 0.5 (0.4–0.8) | 0.001 | 0.5 (0.3–0.6) | <0.001 |
| Current Working Status | ||||
| No | Ref | |||
| Yes | 0.8 (0.7–1.0) | 0.045 | Not included in the final model | |
| Division of Residence | ||||
| Barisal | Ref | Ref | ||
| Chattogram | 1.3 (0.9–2.1) | 0.178 | 0.9 (0.7–1.2) | 0.449 |
| Dhaka | 1.2 (0.8–1.8) | 0.457 | 1.3 (1.0–1.8) | 0.084 |
| Khulna | 1.2 (0.8–1.8) | 0.479 | 1.1 (0.8–1.4) | 0.666 |
| Mymensingh | 1.2 (0.7–1.9) | 0.482 | 1.4 (1.1–1.8) | 0.018 |
| Rajshahi | 1.0 (0.7–1.6) | 0.83 | 1.1 (0.8–1.5) | 0.479 |
| Rangpur | 1.0 (0.6–1.6) | 0.958 | 1.0 (0.7–1.3) | 0.865 |
| Sylhet | 1.4 (0.9–2.2) | 0.124 | 1.2 (0.9–1.6) | 0.163 |
| Marital Status | ||||
| Never Married | Ref | Ref | ||
| Currently Married | 0.6 (0.4–0.7) | <0.001 | 0.7 (0.5–0.8) | <0.001 |
| Separated/Divorced/Widowed | 0.8 (0.5–1.2) | 0.218 | 0.8 (0.6–1.1) | 0.153 |
| Variables | Urban | Rural | ||
|---|---|---|---|---|
| AOR (95% CI) | p-Value | AOR (95% CI) | p-Value | |
| Age (in Years) | ||||
| 18–29 | Ref | Ref | ||
| 30–49 | 1.4 (1.1–1.9) | 0.004 | 1.5 (1.2–1.8) | <0.001 |
| 50–69 | 1.3 (1.0–1.7) | 0.025 | 1.4 (1.2–1.8) | 0.001 |
| 70+ | 1.2 (0.8–1.7) | 0.344 | 1.4 (1.1–1.8) | 0.01 |
| Sex | ||||
| Male | Ref | Ref | ||
| Female | 1.7 (1.4–2.0) | <0.001 | 2.0 (1.8–2.3) | <0.001 |
| Education | ||||
| No Formal Schooling | Ref | Ref | ||
| Primary | 1.2 (1.0–1.5) | 0.071 | 1.3 (1.1–1.5) | <0.001 |
| Secondary | 1.5 (1.2–1.9) | <0.001 | 1.6 (1.4–1.9) | <0.001 |
| College and Higher | 2.1 (1.7–2.7) | <0.001 | 1.7 (1.4–2.1) | <0.001 |
| Wealth Index | ||||
| Poorest | Ref | Ref | ||
| Poorer | 1.3 (0.9–1.8) | 0.22 | 1.1 (1.0–1.3) | 0.176 |
| Middle | 1.7 (1.2–2.3) | 0.002 | 1.6 (1.4–1.9) | <0.001 |
| Richer | 1.9 (1.4–2.5) | <0.001 | 2.1 (1.8–2.6) | <0.001 |
| Richest | 3.9 (2.8–5.3) | <0.001 | 4.1 (3.3–5.2) | <0.001 |
| Current Working Status | ||||
| No | Ref | Ref | ||
| Yes | 0.9 (0.8–1.1) | 0.183 | 1.2 (1.1–1.4) | 0.002 |
| Division of Residence | ||||
| Barisal | Ref | Ref | ||
| Chattogram | 0.8 (0.6–1.1) | 0.212 | 1.0 (0.8–1.3) | 0.954 |
| Dhaka | 0.8 (0.6–1.0) | 0.081 | 0.9 (0.7–1.2) | 0.591 |
| Khulna | 0.9 (0.7–1.2) | 0.555 | 1.0 (0.8–1.3) | 0.904 |
| Mymensingh | 0.6 (0.4–0.8) | 0.003 | 0.7 (0.5–0.8) | 0.001 |
| Rajshahi | 0.7 (0.5–1.0) | 0.073 | 0.8 (0.6–1.0) | 0.068 |
| Rangpur | 0.9 (0.7–1.3) | 0.676 | 0.8 (0.6–1.0) | 0.023 |
| Sylhet | 0.6 (0.4–0.9) | 0.006 | 0.7 (0.5–0.9) | 0.002 |
| Marital Status | ||||
| Never Married | Ref | Ref | ||
| Currently Married | 3.1 (2.5–3.9) | <0.001 | 2.2 (1.7–2.7) | <0.001 |
| Separated/Divorced/Widowed | 2.4 (1.7–3.4) | <0.001 | 1.4 (1.1–1.9) | 0.013 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gupta, R.D.; Frank, H.A.; Akonde, M.; Mazumder, A.; Siddika, N.; Apu, E.H.; Chakraborty, P.A. Rural-Urban Differences in Prevalence and Associated Factors of Underweight and Overweight/Obesity among Bangladeshi Adults: Evidence from Bangladesh Demographic and Health Survey 2017–2018. Epidemiologia 2023, 4, 505-520. https://0-doi-org.brum.beds.ac.uk/10.3390/epidemiologia4040042
Gupta RD, Frank HA, Akonde M, Mazumder A, Siddika N, Apu EH, Chakraborty PA. Rural-Urban Differences in Prevalence and Associated Factors of Underweight and Overweight/Obesity among Bangladeshi Adults: Evidence from Bangladesh Demographic and Health Survey 2017–2018. Epidemiologia. 2023; 4(4):505-520. https://0-doi-org.brum.beds.ac.uk/10.3390/epidemiologia4040042
Chicago/Turabian StyleGupta, Rajat Das, Hanna A. Frank, Maxwell Akonde, Ananna Mazumder, Nazeeba Siddika, Ehsanul Hoque Apu, and Promit Ananyo Chakraborty. 2023. "Rural-Urban Differences in Prevalence and Associated Factors of Underweight and Overweight/Obesity among Bangladeshi Adults: Evidence from Bangladesh Demographic and Health Survey 2017–2018" Epidemiologia 4, no. 4: 505-520. https://0-doi-org.brum.beds.ac.uk/10.3390/epidemiologia4040042