1. Introduction
The end of 2020 was marked by the emergence of SARS-CoV-2 variants that presented increased public health risks on a global scale. As of November 2020, nearly 46 million cases and 1.2 million deaths have been reported globally [
1,
2]. Based on the potential impact of these variants on transmissibility, severity, clinical presentation, and the effectiveness of control and prevention measures (diagnostic tools, vaccination, therapeutic molecules), they have been classified by the World Health Organization (WHO) as variant of concern (VOC), variant of interest (VOI), or variant under monitoring (VUM) [
1].
Genomic sequencing activity directed at pathogen surveillance has shown, over the last decade, its contribution to the detection and control of infectious disease outbreaks, facilitating the production of diagnostics, drugs, and vaccines, and guiding response activities [
3]. The emergence of SARS-CoV-2 has further increased the importance of genomic surveillance data, with 4.8 million genomes deposited in the Global Initiative on Sharing All Influenza Data (GISAID) through 31 October 2021. Genomic surveillance has been very important to the early detect the mutations, to monitor the virus evolution, and to evaluate the degree of similarities between the different variants with vaccine strains [
4].
This SARS-CoV-2 genomic surveillance activity is a critical public health function. It facilitated research activities prioritization and guided informed response decisions which reflected the efficiency of investing in building capacities in this area [
5].
Implementation of genomic surveillance is cheaper and easier than before, but its large-scale implementation is still challenging, especially in low-income countries [
6]. Genomic surveillance is generally based on two complementary approaches: the first is to collect a representative sample of the confirmed COVID-19 cases; and the second is to apply a systematic identification of any phenotypic change in the virus genomic sequence or importation of a VOC from other country. Data from both approaches will be useful to generate indicators to better understand the evolution of the virus and its potential impact and to guide public health actions [
7].
The Alpha variant emerged in the UK in December 2020 [
8]. Alpha variant has a higher infectivity rate, so the risk of virus importation was higher. As a response to its emergence, the Ministry of health of Tunisia implemented a SARS-CoV-2 sequencing strategy. A committee was established of all stakeholders including the Ministry of Health, the National Observatory of New and Emerging Diseases, the virology laboratories involved in sequencing activities, and the Medical Biology Laboratory Unit. The recommendations and guidelines for sequencing SARS-CoV-2 for the purpose of Public Health Surveillance, which were prepared by the WHO, United States Centers for Disease Control and Prevention (CDC), African CDC, European CDC, and expert advisory groups (e.g., WHO Technical Advisory Group on Epidemiology), were summarized and adapted to national sequencing capacities by the “SARS-CoV-2 Sequencing Expert Group”. Accordingly, a national strategy for surveillance of SARS-CoV-2 variants of concern was developed and shared among stakeholders at central and regional levels. Updates of this strategy according to the evolution of the different phases of the epidemic, the emergence of new variants, and national capacities, as well as the possibilities of reinforcement by accessing international sequencing partnerships, were subsequently carried out.
The ongoing global circulation of SARS-CoV-2 and repeated emergence of new variants indicate the need for robust genomic surveillance to inform public health responses. Sampling bias or systematic differences in sample characteristics between COVID-19 cases with sequenced specimens and total COVID-19 cases is a concern and might produce inaccurate representations of variant distribution within the population.
To ensure generalizability and equity when using genomic and epidemiologic data for public health purposes, the methods for genomic surveillance must ensure a representative sample from the population of interest. In Tunisia, the implementation and application of this genomic surveillance in accordance with the national recommendations and the requirements of SARS-CoV-2 genomic surveillance for public health goals has encountered many difficulties. In fact, there were difficulties in managing missing data, making it impossible to characterize phenotypically the different variants. Moreover, we can mention the non-application of targeted and random sampling procedures causing bias in monitoring the proportional circulation of the different variants.
Thus, this study aimed to analyze the SARS-CoV-2 genomic surveillance data in Tunisia from January 2021 to February 2022 and to assess the implementation of the SARS-CoV-2 sequencing strategy in accordance with national recommendations and the guidance for SARS-CoV-2 genomic surveillance for public health goals.
2. Materials and Methods
2.1. Study Design
To meet the two objectives of this work, a descriptive analysis was conducted on all RT-PCR sequenced SARS-CoV-2 genomic surveillance data from January 2021 to February 2022. Additionally, to evaluate the sequencing strategy, an internal audit assessing compliance with the implementation of the strategy was carried out compared to a reference framework which included the procedures of the national strategy and the requirements of SARS-CoV-2 genomic surveillance for public health purposes.
2.2. Study Population
We included all confirmed COVID-19 cases (SARS-CoV-2 RNA detected by molecular amplification) sequenced and reported to the National Observatory of New and Emerging Diseases from January 2021 through February 2022.
2.3. Genomic Surveillance System Design
In January 2021, the National Observatory of New and Emerging Diseases (with five reference SARS-CoV-2 laboratories) established a surveillance strategy to monitor the genomic epidemiology of SARS-CoV-2 in Tunisia. Partner laboratories were selected to maximize geographic coverage and specimen numbers. The initial proportion of randomly selected positive specimens submitted for sequencing was designed to balance geographic coverage regionally and match available sequencing capacity.
Specimens specifically selected for targeted sequencing as part of outbreak investigations because of travel history, known vaccine breakthrough status, or spike gene target failures were also selected outside the random selection process.
2.4. Audit Standards of the Tunisian Sequencing Strategy for SARS-CoV-2
The “audit standards” were designed by compiling the guidance for SARS-CoV-2 genomic surveillance for public health goals. A total of 12 requirements, distributed over five areas, were included in the audit standards, as shown in
Table 1.
2.5. Data Collection
The main sources of data were the national SARS-CoV-2 databases, including “genomic surveillance” and “Confirmed cases”. The variables extracted from the databases included demographic data (date of birth, sex, origin), the date of confirmation of COVID-19 infection, sequencing method(s), and the SARS-CoV-2 variant. The variables of interest in the different databases were cross-referenced and checked against the sequenced patient data.
2.6. Representativeness and Timeliness Evaluation
We assessed representativeness of genomic surveillance data by comparing COVID-19 cases with sequenced specimens to all COVID-19 cases during the same period according to sex and age; we represented the percentage of cases with sequenced specimens by governorate and month to visualize spatiotemporal sampling. We evaluated areas with high sequencing coverage to determine geographic representativeness.
We assessed timeliness of data by comparing the interval between initial specimen collection and genomic data transmission to the national observatory of New and Emerging Diseases. We assessed median timeliness by month and compared data transmitted within <14 days, 14–27 days, and >28 days after specimen collection.
2.7. Ethical Approval
This study included surveillance activity and was exempt from review and informed consent. Confidentiality of individuals was respected during data analysis and reporting.
2.8. Analysis
2.8.1. Analysis of SARS-CoV-2 Genomic Surveillance Data
Data were entered into MS Excel and analyzed using R Software. The following indicators were calculated: number of the total sample to be sequenced, number and proportion of the sequenced sample, number and proportion of classified variants, and proportional distribution of classified variants. Data were described as frequencies and percentages (N, %), and the evolution of the sequencing activity per ISO week and the evolution of the proportional distribution of VOCs per ISO week were presented graphically.
2.8.2. Evaluation of the National Sequencing Strategy
A qualitative assessment for compliance to different standards was done and the level of compliance was identified to be one of the following:
- -
If there is total lack of required information or activities, the level of compliance is considered as “not met”;
- -
If required information or activities are partially respected, the level of compliance is considered as “partially met”;
- -
If we disposed of all the information needed and the activity was well realized, the level of compliance is considered as “fully met”.
3. Results
3.1. Surveillance Sequencing Data of SARS-CoV-2
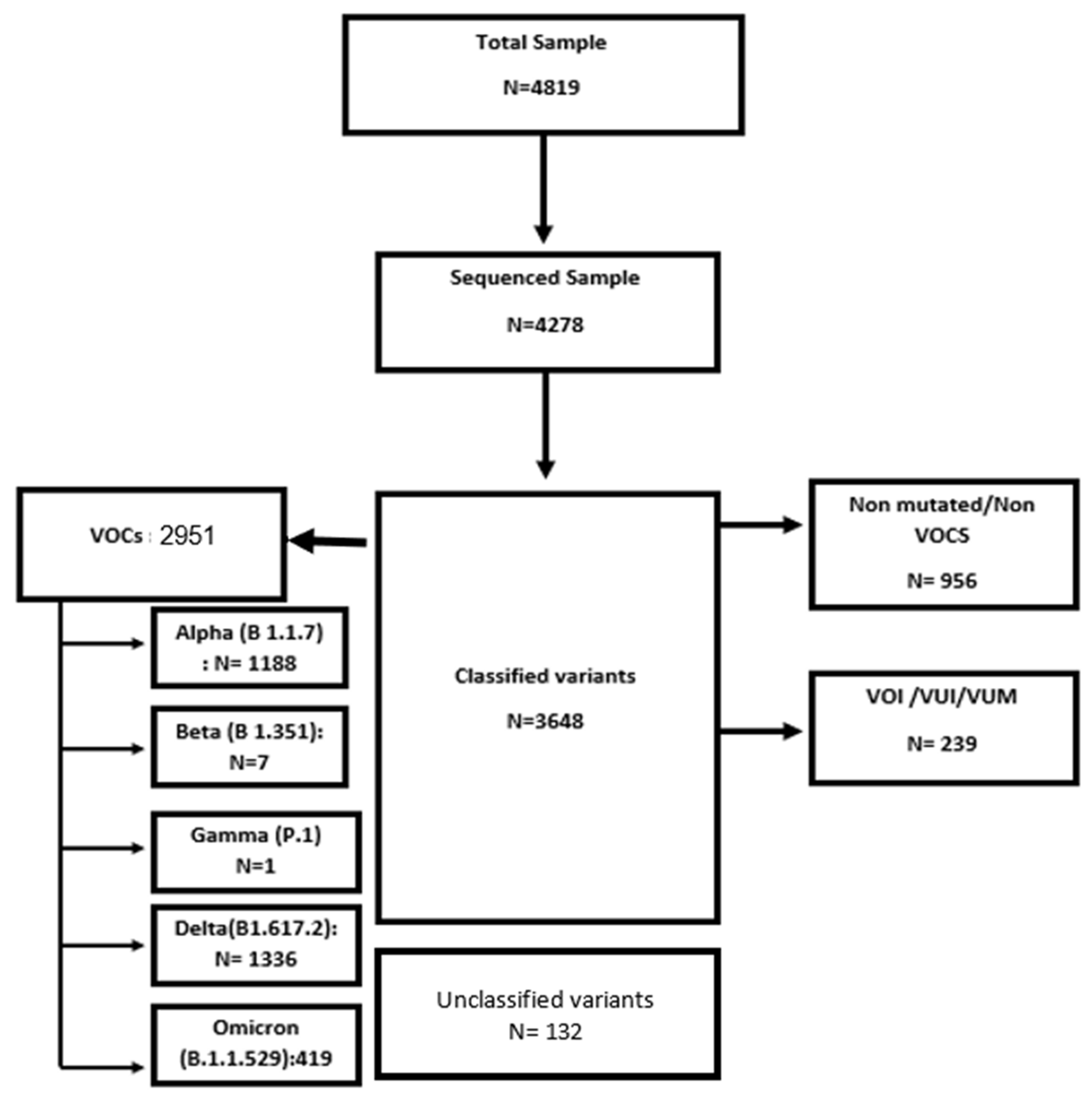
A total of 4819 samples were sent to sequencing laboratories during the study period and 4278 (75.7%) samples were sequenced. Of those, 85.2% of samples were classified. Positive VOC samples came to 80.9%, differentiated as Alpha (1187.88, 40.24%); Beta (7.085, 0.24%); Gamma (0.886, 0.03%); Delta (1336.07, 45.26%); and Omicron (419, 14.19%) (
Figure 1).
The sequencing methods used are reported in
Table 2. Screening was the method used for the majority, followed by partial genomic sequencing.
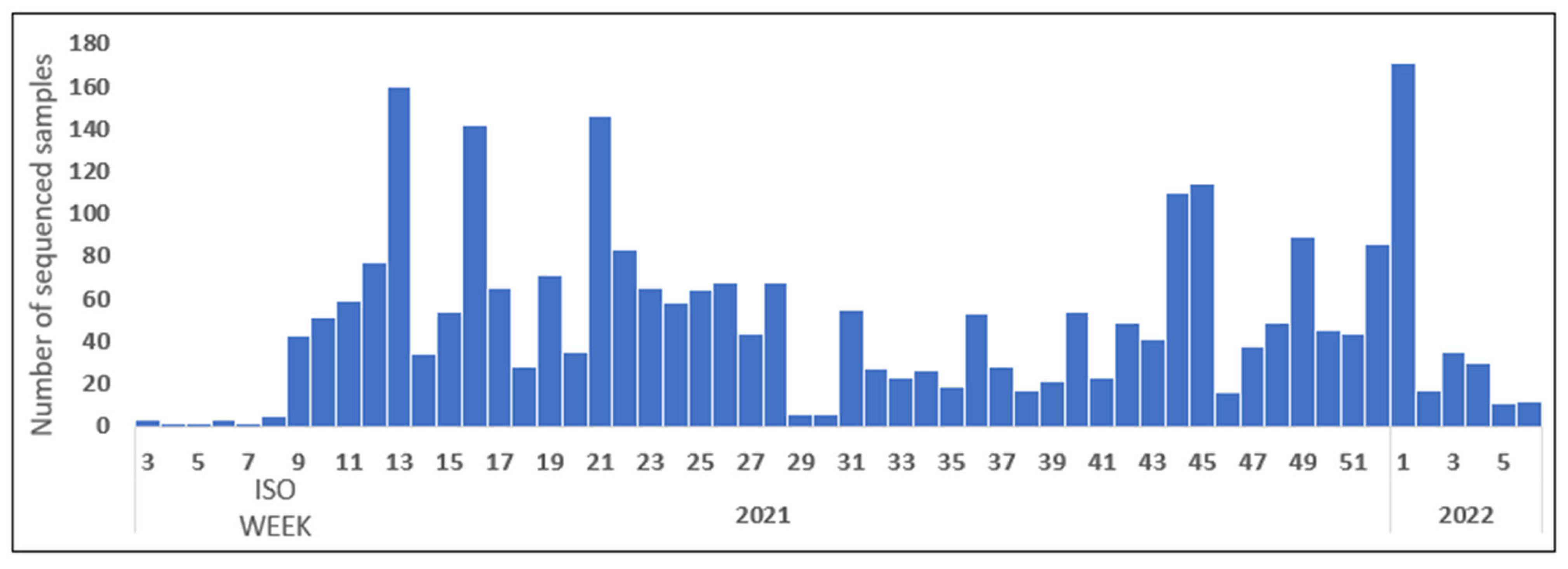
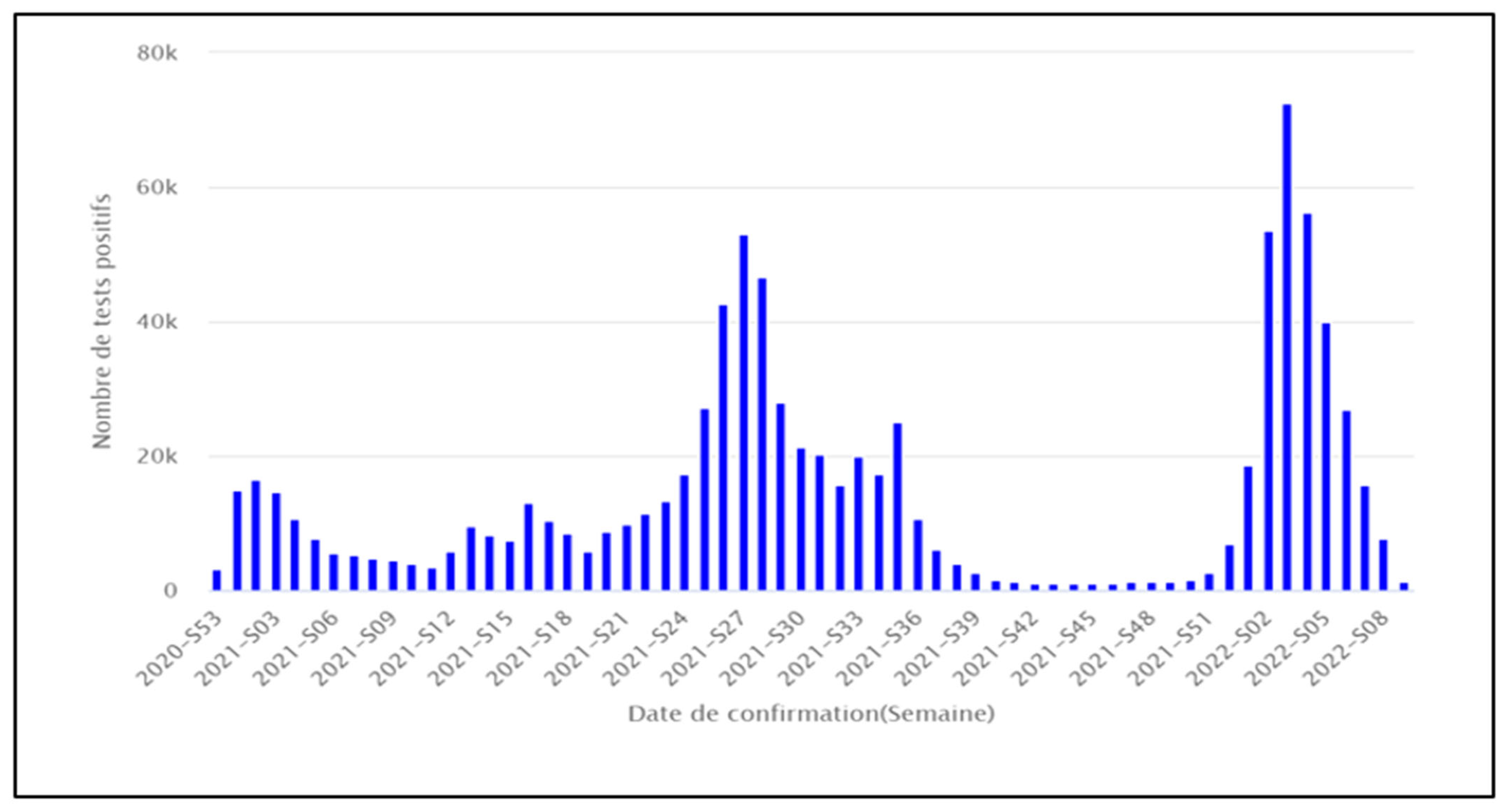
The Sequencing activity varied throughout the period of the epidemic’s evolution, as shown in
Figure 2, compared to the confirmed cases per ISO week, as shown in
Figure 3.
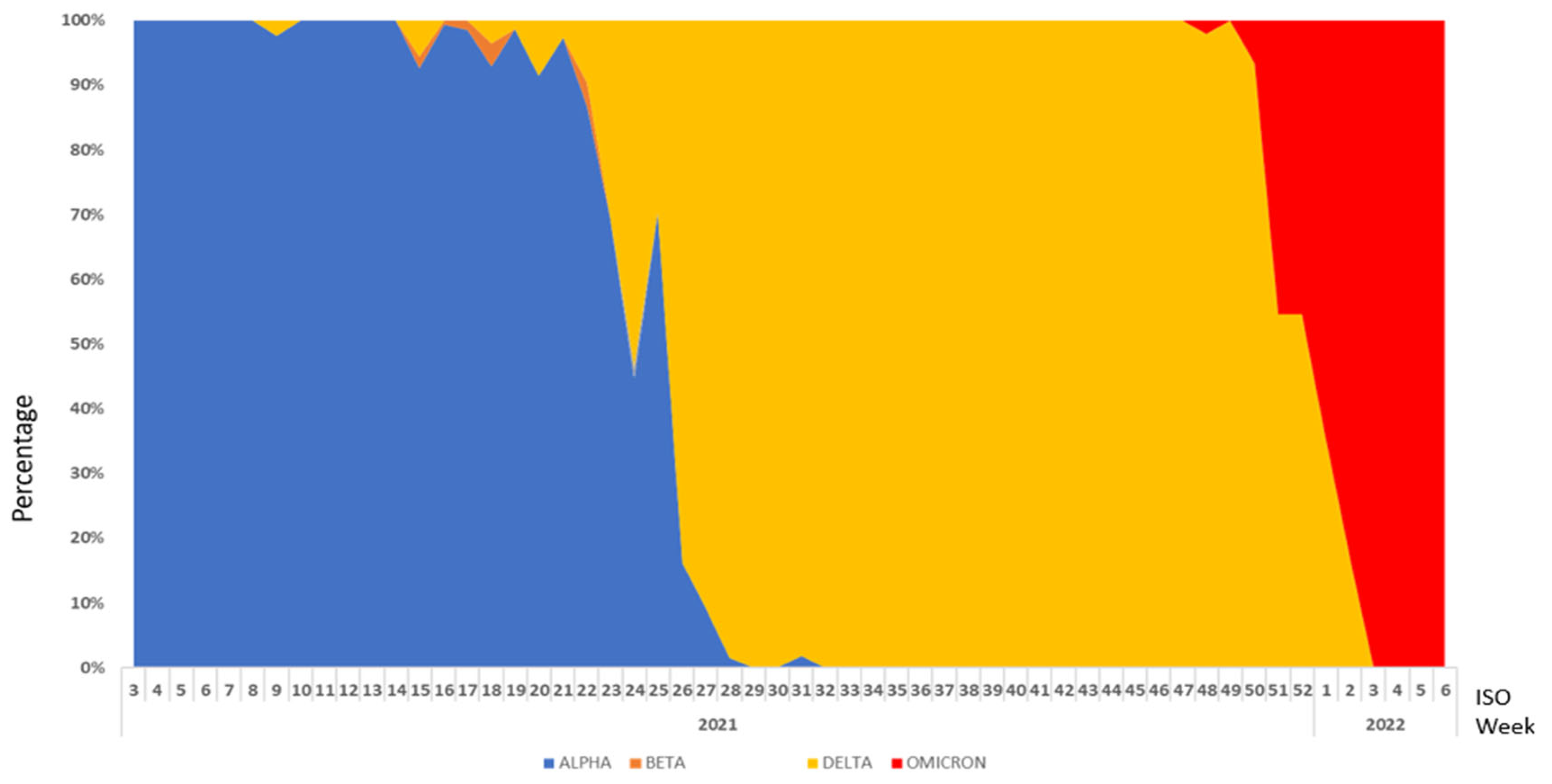
The study of the evolution of VOC’s predominance showed three phases: (1) Alpha variant predominance from ISO week 3/2021 to ISO week 25/2021; (2) Delta variant predominance from ISO week 26/2021 to ISO week 2/2022; and (3) Omicron variant predominance from ISO week 3/2022 to ISO week 6/2022 (
Figure 4).
3.2. Results of the Internal Audit of the Tunisian Strategy of SARS-CoV-2 Genomic Surveillance
The conformity of the implementation of the national SARS-CoV-2 sequencing strategy with the requirements of the SARS-CoV-2 genomic surveillance for public health purposes is detailed in the
Table 2. Of the 12 requirements; 7 were “not met”, 4 were “partially met”, and 1 was “fully met” but including not totally achieved objectives.
4. Discussion
This study is the first exhaustive national analysis of SARS-CoV-2 genomic sequencing surveillance data in Tunisia, with an assessment of implementation and compliance with SARS-CoV-2 genomic surveillance sequencing strategy requirements for public health purposes. By performing this evaluation, we provide information regarding the populations of sampled cases and limitations on inference affecting genomic data use. More broadly, we raise awareness regarding sampling bias in convenience-based genomic surveillance systems and support the development of robust genomic surveillance systems.
The results of the analysis of the surveillance data showed that the study of the proportional distribution of the VOCs made it possible to identify the phases of predominance and inversion of the circulation of the different VOCs. This evolution should be interpreted with caution, considering the non-representativeness of the sequenced samples throughout the evolution of the epidemic in Tunisia. A similar study has been conducted to define the relative abundance of SARS-CoV-2 lineages and to identify novel SARS-CoV-2 variants in wastewater samples from October 2020 to March 2021 in Nice. It identified a switch that occurred between January and February 2021, characterized by a rapid onset of the Alpha variant representing more than 80% of all sequences and the subsequent appearance of the delta variant.
The qualitative assessment for compliance with different standards showed that only one requirement was “fully met”, even though it included not totally achieved objectives. A study of 118 surveillance strategies of different countries based on predefined criteria showed that 45 countries (38.1% of the countries studied) had a high level of routine genomic surveillance, 17 (14.4%) had a moderate level of routine genomic surveillance, 25 (21.2%) implemented a low level of routine genomic surveillance, and 31 (26.3%) had limited genomic surveillance, such as the Eastern Mediterranean Region, followed by the African Region, the Americas, South-East Asia, and the Western Pacific Regions [
9].
The non-compliant requirements identified in the evaluation of SARS-CoV-2 genomic surveillance sequencing for public health purposes are mainly related to procedure and application of random and targeted sampling; missing metadata; non-availability of match vaccine data; investigation of first cases of variants of concern; notification of variant surveillance data; rapid sharing of information; and ethical considerations.
The SARS-CoV-2 sequencing data surveillance study based on consolidated data from many sources had several struggles: difficulties in managing missing data, particularly for death and hospitalization outcomes, making it impossible to characterize the different variants phenotypically in terms of severity; moreover, the sequenced samples are not representative because of their non-compliance with sampling requirements and non-application of targeted and random sampling procedures. In fact, the bias in monitoring the proportional circulation of the different variants accounts for the impossibility pf early detection of the introduction of new variants.
The implementation of the national sequencing strategy encountered several difficulties; in particular, weekly randomly selected samples that were not sent to the laboratories in time for sequencing as, according to a study of the turnaround time (TAT, defined as the time in days between sample collection and genome submission) of SARS-CoV-2 genome sequencing across 19 geographic regions, an average of 48 days after sampling was the time required to deposit virus sequences in public databases [
9].
Other epidemiologic information was of interest in assessing representativeness, including travel history, reinfection, and vaccine status. However, data for those variables were incomplete, limiting their usefulness. The full potential of genomic epidemiologic surveillance for improving public health requires pairing epidemiologic, vaccine, and clinical metadata with genomic data.
5. Conclusions
The sequencing of SARS-CoV-2 has made it possible to detect the introduction of variants of concern and to describe the circulation of the different viral strains throughout the evolution of the epidemic. The implementation of a sequencing strategy in line with the requirements of genomic surveillance of SARS-CoV-2 for public health purposes has encountered several problems for timely decision making. The results offer an opportunity to convene all involved stakeholders and discuss the development of an epidemiogenomic surveillance strategy for early detection and guidance as to the response measures for outbreaks caused by highly mutagenic pathogens.
Author Contributions
Conceptualization, N.B.B.A. and M.S.; Methodology, M.S. and A.N.; Software, M.S., A.N. and N.E.M.; Validation, N.B.B.A. and M.S.; Formal Analysis, M.S.; Investigation H.T., I.B., M.M. and L.F.B.; Data Curation W.K., C.A. and A.N.; Writing—Original Draft Preparation, A.N.; Writing—Review and Editing, M.S. and N.B.B.A.; Visualization, A.H., H.L. and S.D. (Sonia Dhaouadiand); Supervision, M.S.; Project Administration, L.B. and S.D. (Sondes Darouiche). All authors have read and agreed to the published version of the manuscript.
Funding
The SARS-CoV-2 sequencing strategy was funded by the Tunisian Ministry of Health.
Informed Consent Statement
Patient consent was waived; data collection and analysis were required by the Tunisia’s National multidisciplinary commission for COVID-19 as part of the public health outbreak investigation and response. As conducted in response to a public health emergency, this research was a part of epidemiological surveillance, analysis of data, and containment measures implemented in order to control the spread of the outbreak, and is exempted from ethical approval Law No. 2007–12 of 12 February 2007 amending and supplementing Law No. 92–71 of 27 July 1992 on communicable diseases stipulating. Article 11 (bis): all tracing and other epidemiological data were collected from National Observatory of New and Emerging Diseases of Tunis, Tunisia (Main National Structure of epidemiologic Surveillance in Tunisia: Decree No. 2005–3294 of 19 December 2005, Article 3). Administrative permissions were required to access and use the meta-data described in our study. Permission was granted from the National Observatory of New and Emerging Diseases. Data used in this study were anonymized before use. Neither ethical approval nor individual consent were applicable.
Data Availability Statement
The National Observatory of New and Emerging Diseases (Tunisia), as well as the corresponding author, have full access to all data. This data is not publicly accessible but are available from the corresponding author upon reasonable request.
Acknowledgments
Authors gratefully acknowledge the staff of the five virology laboratories involved in the national strategy of surveillance on SARS-CoV-2 variants of Concern: Charles Nicolles Tunis, Pasteur Institute Tunis, Habib Bourguiba Sfax, and Fattouma Bourguiba Monastir. The authors also would like to acknowledge the Eastern Mediterranean Public Health Network (EMPHNET) and the reviewers who suggested suitable modifications in the manuscript (Randa Saad and Ihab Basha). We are also grateful to all of the regional Public Health Surveillance Departments staff participating in sample and data collection, the medical biology laboratory unit, and all the staff participating in the development of the strategy, as well as staff of the National Observatory of New and Emerging Diseases (ONMNE)’s contribution in data entry.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Petersen, E.; Ntoumi, F.; Hui, D.S.; Abubakar, A.; Kramer, L.D.; Obiero, C.; Tambyah, P.A.; Blumberg, L.; Yapi, R.; Al-Abri, S. Emergence of new SARS-CoV-2 Variant of Concern Omicron (B.1.1.529)—Highlights Africa’s research capabilities, but exposes major knowledge gaps, inequities of vaccine distribution, inadequacies in global COVID-19 response and control efforts. Int. J. Infect. Dis. 2022, 114, 268–272. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. COVID-19 Weekly Epidemiological Update. Available online: https://apps.who.int/iris/bitstream/handle/10665/336478/nCoV-weekly-sitrep01Nov20-eng.pdf (accessed on 16 August 2022).
- World Health Organization. Genomic Sequencing of SARS-CoV-2: A Guide to Implementation for Maximum Impact on Public Health; World Health Organization: Geneva, Switzerland, 2021; 80 p. [Google Scholar]
- Chen, Z.; Azman, A.S.; Chen, X.; Zou, J.; Tian, Y.; Sun, R.; Xu, X.; Wu, Y.; Lu, W.; Ge, S.; et al. Global landscape of SARS-CoV-2 genomic surveillance and data sharing. Nat. Genet. 2022, 54, 499–507. [Google Scholar] [CrossRef] [PubMed]
- Brandt, C.; Spott, R.; Hölzer, M.; Kühnert, D.; Fuchs, S.; Lohde, M.; Marquet, M.; Viehweger, A.; Rimek, D.; Pletz, M.W. Molecular epidemiology of SARS-CoV-2—A regional to global perspective. medRxiv 2021. [Google Scholar] [CrossRef]
- Abid, S.; Ferjani, S.; El Moussi, A.; Ferjani, A.; Nasr, M.; Landolsi, I.; Saidi, K.; Gharbi, H.; Letaief, H.; Hechaichi, A.; et al. Assessment of sample pooling for SARS-CoV-2 molecular testing for screening of asymptomatic persons in Tunisia. Diagn. Microbiol. Infect. Dis. 2020, 98, 115125. [Google Scholar] [CrossRef] [PubMed]
- Eurosurveillance. Economic Evaluation of Whole Genome Sequencing for Pathogen Identification and Surveillance—Results of Case Studies in Europe and the Americas 2016 to 2019. Available online: https://www.eurosurveillance.org/content/10.2807/1560-7917.ES.2021.26.9.1900606?crawler=true (accessed on 10 August 2022).
- Ladhani, S.N.; Ireland, G.; Baawuah, F.; Beckmann, J.; Okike, I.O.; Ahmad, S.; Garstang, J.; Brent, A.J.; Brent, B.; Aiano, F.; et al. Emergence of SARS-CoV-2 Alpha (B.1.1.7) variant, infection rates, antibody seroconversion and seroprevalence rates in secondary school students and staff: Active prospective surveillance, December 2020 to March 2021, England. J. Infect. 2021, 83, 573–580. [Google Scholar] [CrossRef] [PubMed]
- Brito, A.F.; Semenova, E.; Dudas, G.; Hassler, G.W.; Kalinich, C.; Kraemer, M.; Ho, J.; Tegally, H.; Githinji, G.; Agoti, C.; et al. Global disparities in SARS-CoV-2 genomic surveillance. medRxiv 2021. [Google Scholar] [CrossRef] [PubMed]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 




{kind=link}
{kind=link}
{kind=link}
{kind=link}