
The Relationship of Internalized Weight Bias to Weight Change in Treatment-Seeking Overweight Adults


1
Department of Psychology, University of Hawai‘i at Mānoa, Honolulu, HI 96822, USA
2
School of Social Sciences, Monash University, Melbourne 3800, Australia
*
Author to whom correspondence should be addressed.
Obesities 2022, 2(1), 21-34; https://0-doi-org.brum.beds.ac.uk/10.3390/obesities2010003
Submission received: 26 August 2021
/
Revised: 22 December 2021
/
Accepted: 23 December 2021
/
Published: 19 January 2022
(This article belongs to the Special Issue Weight Stigma: Experiences, Consequences, Causes and Remedies)
Abstract
:The present study examined data from a randomized controlled trial exploring whether behavioral weight loss treatment was associated with changes in internalized weight bias. The relationship between internalized weight bias and psychological functioning was also assessed. Participants were 106 men and women with overweight or obesity enrolled in a treatment outcome study using the Lifestyle Balance Program. Participants completed measures of internalized weight bias, anti-fat attitudes, self-esteem, body image concern, depressive symptoms, anxiety, and stress. Variables were assessed at baseline, post-treatment, and six-month follow-up. Weight bias internalization significantly decreased over the course of treatment. Baseline and follow-up internalized weight bias scores predicted change in body weight. Participants reporting the lowest levels of internalized weight bias at baseline lost nearly twice as much weight as participants reporting the highest levels of internalized weight bias. Significant associations were found between internalized weight bias, body image concern, and self-esteem. Findings indicate a relationship between internalized weight bias and weight change during behavioral weight loss treatment, highlighting the importance of assessing baseline levels of internalized weight bias in weight loss treatment studies. Higher internalized weight bias predicted poorer weight loss outcomes, indicating a need for tailored treatment approaches.
1. Introduction
More than 70% of the adult United States population is categorized as having overweight or obesity [1]. A range of weight loss protocols has been developed to reduce obesity [2], including behavioral weight loss programs. Among studies of comprehensive behavioral weight loss programs, more than half of participants lose at least 5% of initial body weight within a year, with nearly 3 in 10 participants losing at least 10% of initial weight [3]. Notably, however, most studies report that by five years post-treatment, a significant proportion of participants have either returned to or surpassed their baseline weight [4,5].
Researchers studying the efficacy of weight loss protocols have examined whether changes in body weight correspond to improvements in several psychological variables, most often body image concern, depressive symptoms, and self-esteem. Significant improvements in body image have been demonstrated among individuals enrolled in behavioral weight loss treatment [6], and these improvements appear to be maintained up to one-year follow-up [7]. A systematic review of 14 studies that examined body image in the context of behavioral weight loss found that six studies reported a positive association between body image improvement and weight loss, while the majority of the other studies did not directly assess the relationship of body image and weight change [6]. Behavioral weight loss treatment also improves symptoms of depression and anxiety among treatment-seeking samples of men and women with overweight and obesity [8,9]. A meta-analysis of weight loss treatment studies found significant improvement in symptoms of depression among groups treated with lifestyle modification interventions, reporting a medium-sized effect averaged across 27 groups [10]. However, changes in depressive symptoms have generally been shown to be unrelated to the amount of weight lost during treatment [6,10,11].
As with body image and depressive symptoms, studies suggest that weight loss treatment has a positive effect on self-esteem [11,12,13,14]. Some studies [11,15] suggest that at least some weight loss needs to occur in order to yield improvements in self-esteem. However, a systematic review of 12 weight loss studies found that despite improvements in self-esteem across most interventions, changes in self-esteem were generally not directly associated with the amount of weight lost [6].
Internalized weight bias, which involves believing negative weight-related attributions and stereotypes and applying them to oneself [16], has demonstrated harmful effects on physical and psychological health. Studies have found positive associations between internalized weight bias and eating disturbances (e.g., binge eating), depression, anxiety, and stress [17,18,19,20]. Additionally, internalized weight bias was negatively associated with general health and self-esteem [17,18,19]. Across 27 studies in a systematic review, internalized weight was correlated with greater body image concerns and more body dissatisfaction [20].
Several studies have examined the construct of internalized weight bias among overweight adults seeking behavioral weight loss treatment. Carels and colleagues explored changes in internalized weight bias among 54 men and women who completed either of two 14 week behavioral weight loss programs [17]. Other studies examined changes in internalized weight bias among adults with obesity during 3 month [21] and 6 month behavioral weight loss interventions [22,23,24]. Across studies, internalized weight bias was related to higher rates of disordered eating and poorer body image at baseline, and internalized weight bias significantly decreased over the course of treatment [17,22,23].
Literature on the relationship between internalized weight bias and weight change during and after treatment has been inconclusive. A systematic review found no association between internalized weight bias and weight change across four short-term behavioral weight loss studies [20]. However, a prospective study of individuals who successfully lost weight found that weight loss was associated with reduced internalized weight bias at one year follow-up [25]. Additionally, a recent multinational study of individuals in behavioral weight loss treatment found a significant association between internalized weight bias and weight change, such that higher internalized weight bias was linked with greater self-reported weight gain [26]. Among studies that have examined weight loss outcomes following bariatric surgery, one found that higher levels of internalized weight bias predicted less postoperative weight loss [27], while a second reported no association between internalized weight bias and postoperative weight change [28]. Altogether, these studies provide an important first step in understanding the relationship of internalized weight bias to weight change. Expanding upon existing research, the present study examines the prospective relationship between internalized weight bias and weight change within the context of a long-term behavioral weight loss intervention with long-term follow-up.
The current research is a cross-sectional and longitudinal examination of data from a randomized controlled trial. One primary objective of this study is to determine whether behavioral weight loss treatment is related to changes in internalized weight bias among treatment-seeking adults with overweight and obesity. Additionally, this study seeks to examine the relationship of internalized weight bias to weight change and psychological functioning. With these objectives in mind, this study presents one formal research hypothesis and two research questions:
Central Hypothesis: Based on evidence from previous studies showing improvements in body image, depressive symptoms, self-esteem and anti-fat attitudes across weight loss treatment, and shorter-term findings that internalized weight bias decreases over the course of behavioral weight loss treatment, it is hypothesized that levels of internalized weight bias at post-treatment and follow-up will be significantly lower than at baseline.
Research Question 1 (RQ1): What is the relationship of internalized weight bias to weight change?
Research Question 2 (RQ2): Is internalized weight bias associated with additional outcome measures, including body image, depression, anxiety, and self-esteem?
2. Materials and Methods
2.1. Study Participants
To be considered for the present study, participants were required to have a BMI greater than or equal to 27 kg/m2. Participants were excluded from participation in this study if they were currently in another weight control program, if they had a current or past obesity-related or other medical health disorder (e.g., diabetes), if they were taking medications affecting weight and had not been on a stable dose for at least two months, if they had a current or past severe psychiatric disorder or if they were pregnant, had been pregnant in the past year or were planning to become pregnant in the two years following treatment.
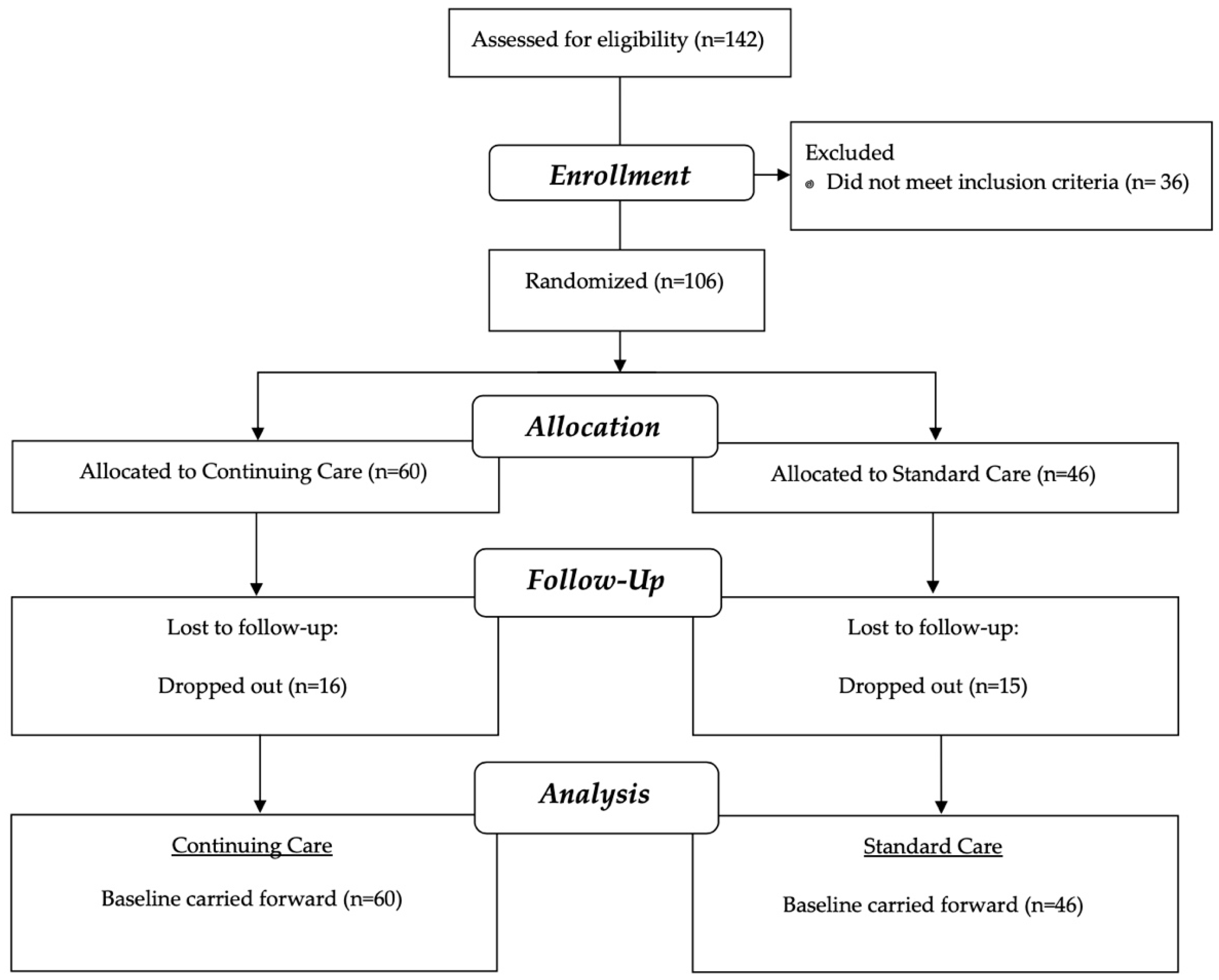
Participants were 106 men and women with overweight or obesity between the ages of 20 and 77 (M = 49.52, SD = 12.93) with a mean BMI of 35.66 (SD = 7.67) recruited from community organizations (e.g., Young Men’s Christian Association clubs) to be part of a separate study of the effectiveness of a self-help component added to a standard behavioral weight loss program [29]. The sample was 60.4% female (n = 64) and 32.1% male (n = 34). 29.2% Caucasian (n = 31), 29.2% mixed ethnic heritage (n = 31), 19.8% Asian American (n = 21), 9.4% Native Hawaiian/Pacific Islander (n = 10), 0.9% African American (n = 1), and 0.9% Latino/a (n = 1). The participant flow diagram is located in Figure 1.
2.2. Randomization
Block random assignment using a computer-generated sequence was used to assign participating community centers to one of two treatment conditions: (1) standard care, or (2) continuing care. To keep individuals at the same community center in the same treatment group, randomization was conducted by center. At one community center, two different treatment groups were conducted; at other centers, only one group was conducted. Because most community centers insisted on having advanced knowledge of whether they would need to provide meeting space for six months or two years, randomization took place following recruitment of community centers and prior to introductory meetings. Thus, allocation was known at the time of individual consent when participants learned the condition of their prospective group. The researchers, who provided treatment and assessed outcomes were also aware of assigned conditions.
2.3. Study Procedures
Prior to the first treatment session, persons meeting inclusion criteria for this study were randomized into two treatment conditions: (1) a standard behavioral weight loss treatment (n = 46), or (2) standard behavioral weight loss treatment with an added 18 month continuing care component (n = 60). This study was then explained to participants at an introductory meeting. All participants enrolled in this study received an intensive lifestyle intervention called the Lifestyle Balance Program, which included 20 sessions (two hours per session) over the course of six months at their respective community centers. The Lifestyle Balance Program included clearly defined weight loss and physical activity goals, self-monitoring, and coping strategies for addressing challenges, managing stress, and maintaining motivation [30]. All participants were assessed at baseline, at post-treatment, and at 6, 12, and 18 months post-treatment. Data from the first three of these assessments are included in the present study. These procedures were approved by the University of Hawai’i Institutional Review Board (Protocol #15527), and all participants gave informed consent. There were no harms or adverse effects reported during this study.
2.4. Measures
At each assessment point, participant weight was measured using a digital scale (Tanita, Inc., Arlington Heights, IL, USA). At baseline, height was measured using a stadiometer and demographic information was collected. In addition, the following questionnaires were administered.
2.4.1. Weight Bias Internalization Scale (WBIS)
The WBIS [16] was used to measure the degree to which a respondent believes that negative stereotypes and negative self-statements about being overweight or obese apply to him or her. Respondents are asked to rate their agreement with each of 11 items on a 7-point scale from “strongly disagree” to “strongly agree” (e.g., “As an overweight person, I feel that I am just as competent as anyone.”). The WBIS was found to have an internal consistency (Cronbach’s alpha) of 0.90 in a sample of treatment-seeking adults with overweight and obesity [16]. Convergent validity was demonstrated by significant relationships between internalized weight bias and measures of self-esteem, drive for thinness, and body image concern [16]. Cronbach’s alpha in the present sample was 0.67.
2.4.2. Anti-Fat Attitudes Questionnaire (AAQ)
To evaluate changes in internalized weight bias alongside changes in anti-fat attitudes, participants completed the AAQ [31]. This scale is a 13-item measure reflecting dislike of obese persons (Dislike subscale), fear of fat (Fear of Fat subscale), and beliefs about the controllability of weight (Willpower subscale). Items include such statements as, “I have a hard time taking fat people too seriously,” and respondents are asked to rate their agreement with the statements on a 0 to 9 Likert scale. The AAQ has been used among adult samples with overweight and obesity [32]. Internal consistency (Cronbach’s alpha) in the present sample was 0.79 for the Dislike subscale, 0.82 for the Fear of Fat subscale and 0.64 for the Willpower subscale.
2.4.3. Rosenberg Self-Esteem Scale (RSE)
Participants completed the RSE [33], a widely used measure of self-esteem which asks for respondents’ degree of agreement with 10 statements such as “I feel that I have a number of good qualities,” using a 4-point scale ranging from “strongly disagree” to “strongly agree.” Extensive research has been conducted on the psychometric properties of the RSE, such as demonstration of its discriminant and convergent validity [34]. The RSE has been used extensively among adults with overweight and obesity [35,36]. Cronbach’s alpha in the present sample was 0.87.
2.4.4. Depression Anxiety Stress Scales (DASS)
The 21-item version of the DASS [37] was used to measure participants’ depressive symptoms, level of anxiety and perceived stress. It consists of three subscales and produces a total score reflecting core symptoms of depression, anxiety, and stress. Respondents rate the degree to which each of the 21 statements applied to him/her over the past week. Item responses fall along a 4-point Likert scale, with agreement ranging from “Did not apply to me at all” to “Applied to me very much, or most of the time.” Previous research has demonstrated the concurrent validity of the 21-item version of the DASS by reporting significant associations between the DASS and established measures of depression and anxiety [38]. Additionally, this version of the DASS has been used in samples of adults with overweight and obesity [39,40]. Cronbach’s alpha in the present sample was 0.92 for the total DASS score, 0.86 for the Depression subscale, 0.77 for the Anxiety subscale, and 0.84 for the Stress subscale.
2.4.5. Body Shape Questionnaire (BSQ)
Finally, participants completed the Short Version of the BSQ [41,42], a 14-item measure of satisfaction and concern with body shape. Item responses fall on a 6-point scale ranging from “never” to “always” (sample item: “Have you felt ashamed of your body?”). The shortened version of the BSQ showed good construct validity in a sample of women with disordered eating by reporting significant correlations with scores on the Eating Attitudes Test, the Bulimia Investigatory Test and the Beck Depression Inventory [41]. The 14-item BSQ has been studied among adults with overweight and obesity [16]. Cronbach’s alpha in the present sample was 0.95.
2.5. Statistical Analyses
2.5.1. Weight Change at Post-Treatment and Follow-Up
To provide descriptive context for the sample, percent change in initial body weight (IBW) is reported along with baseline weight and demographic variables. To minimize the risk of bias, missing weight loss data were accounted for by Intention-to-Treat (ITT) analysis procedures using the last observation carried forward. Psychological variables were not imputed in the ITT analysis. A participant was considered to have dropped-out of this study if he/she missed five consecutive sessions or eight or more sessions, inclusive of the final two sessions of the program. In total, 70.8% of the sample completed treatment. Independent-samples t-tests demonstrated no significant differences between participants who completed treatment and participants who dropped out on any baseline measures of psychological functioning or baseline BMI.
2.5.2. Central Hypothesis: Change in Internalized Weight Bias over Time
A series of repeated-measures analysis of variance (ANOVAs) with post hoc simple contrasts was used to assess changes in internalized weight bias between baseline, post-treatment, and six-month follow-up as well as to compare changes in internalized weight bias to changes in body image concern, self-esteem, anti-fat attitudes, depressive symptoms, anxiety, and stress. Analyses were conducted using assessment time as the within-subjects factor (three levels) and treatment condition as the between-subjects factor (two levels).
2.5.3. RQ1: Relationship of Internalized Weight Bias to Weight Change
Change scores were calculated for each of the study variables (specifically, internalized weight bias, body image concern, self-esteem, anti-fat attitudes, depressive symptoms, anxiety, and stress,) by subtracting participants’ baseline scores from post-treatment scores (Time 2 minus Time 1), post-treatment scores from follow-up scores (Time 3 minus Time 2) and baseline scores from follow-up scores (Time 3 minus Time 1). The associations between these change scores and percent change in IBW from baseline to post-treatment, percent change from post-treatment to follow-up, and percent change from baseline to follow-up, were examined using Pearson’s product-moment correlations.
To assess whether participants’ baseline WBIS scores were related to the amount of weight change over treatment, participants were grouped according to baseline level of internalized bias by transforming the continuous WBIS variable into a categorical variable using a median split. An independent-samples t-test was conducted to assess whether percent change in IBW differed significantly between those participants reporting a high baseline WBIS score and those participants reporting a low baseline WBIS score at post-treatment and follow-up.
2.5.4. RQ2: Relationship of Internalized Weight Bias to Psychological Functioning
Finally, the relationships between internalized weight bias and body image concern, self-esteem, anti-fat attitudes, depressive symptoms, anxiety, and stress were explored using Pearson product-moment correlations calculated at baseline, post-treatment and follow-up.
3. Results
3.1. Weight Change at Post-Treatment and Follow-Up
Treatment completers lost a mean of 5.22% of initial body weight (IBW; SD = 4.83) from baseline to post-treatment, and an additional 0.50% IBW (SD = 6.21) from post-treatment to six-month follow-up (weight loss did not differ by treatment condition). Using ITT analysis (last observation carried forward), participants lost a mean of 3.87% IBW (SD = 4.75) from baseline to post-treatment and an additional 0.46% IBW (SD = 4.73) from post-treatment to follow-up.
3.2. Change in Internalized Weight Bias over Time
To address this study’s central hypothesis that WBIS scores would decline from baseline to post-treatment and follow-up, a repeated-measures ANOVA with simple contrasts was used to assess the effect of assessment time (3 factors) and treatment condition (2 factors). Cell means at the three timepoints, collapsed across treatment conditions, are shown in Table 1. Mauchley’s Test of Sphericity was found to be significant (χ2 = 13.05; p = 0.0001), indicating that the assumption of sphericity was violated. Therefore, the Greenhouse–Geisser correction was applied to the data (ε = 0.89). Tests of between-subject effects indicate no significant main effect for treatment condition (F(1, 104) = 1.24; p = 0.27). Tests of within-subject effects showed no significant interaction effect for assessment time x treatment condition (F(1.79, 185.89) = 0.45, p = 0.64). A significant main effect was found for assessment time (Table 1).
Simple contrasts demonstrated that WBIS scores declined significantly between baseline and post-treatment (F(1, 104) = 8.10, p = 0.005), between post-treatment and follow-up (F(1, 104) = 5.18, p = 0.03), and overall from baseline to follow-up (F(1, 104) = 19.40, p < 0.001). Effect sizes (Cohen’s d) for these changes were in the small range, at 0.27, 0.14, and 0.33, respectively [43].
As shown in Table 1, a significant main effect was found for assessment time for other study measures. Between pre-treatment and post-treatment assessments, participants reported reductions in anti-fat attitudes, depressive symptoms, anxiety, and stress, and increases in self-esteem. There were no significant changes in self-esteem from post-treatment to follow-up, but reported depressive symptoms and anxiety and stress levels significantly increased.
3.3. RQ1: How Is Internalized Weight Bias Related to Weight Change?
3.3.1. Relationship of Baseline WBIS Score to Weight Change
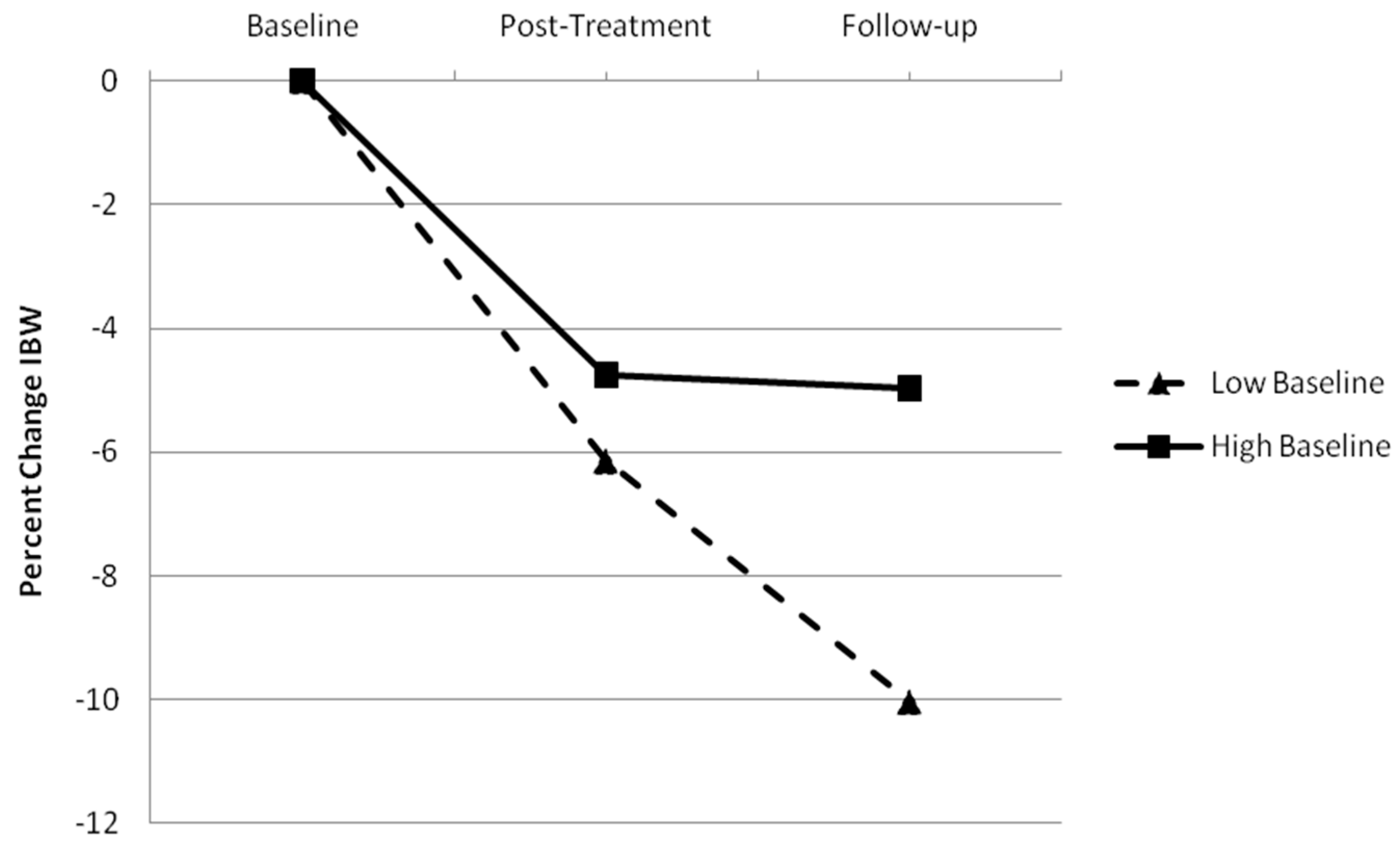
Using the ITT sample, no significant difference in percent change in IBW from baseline to post-treatment (t(94) = 0.98, p = 0.33) was found between participants with low baseline WBIS scores (M = 4.50%; SD = 5.05) and participants with high baseline WBIS scores (M = 3.54%; SD = 4.51). The difference between these groups in additional percent change in IBW from post-treatment to follow-up trended toward significance (t(94) = 1.94, p = 0.06). However, significant differences between the groups emerged when considering the overall study period from baseline to follow-up (t(95) = 2.13, p = 0.04), as shown in Figure 2. Participants reporting low baseline WBIS scores lost significantly more weight than participants reporting high baseline WBIS scores (M (SD) = 5.98% (7.75) and 3.26% (4.55), respectively).
Among treatment completers, there were no significant differences between the two groups in percent change in IBW between baseline and post-treatment (t(69) = 1.21, p = 0.23; M (SD) = 6.14% (4.97); M (SD) = 4.76% (4.64). Similarly, no significant difference between the groups was found in percent change in IBW from post-treatment to follow-up (t(41) = 1.59, p = 0.12). Significant differences between the groups emerged in percent change in IBW from baseline to follow-up (t(42) = 2.42, p = 0.02), as shown in Figure 3. For the overall study period, participants with the lowest baseline WBIS scores lost significantly more weight than participants reporting the highest baseline WBIS scores (M (SD) = 10.03% (8.48) and 4.97% (4.90), respectively).
3.3.2. Correlation between Change in IBW and Internalized Weight Bias and Psychological Functioning
As shown in Table 2, baseline RSE scores were significantly related to percent change in IBW between baseline and post-treatment. Baseline WBIS, RSE and BSQ scores were significantly related to percent change in IBW from baseline to follow-up.
3.4. RQ2: Do Levels of Internalized Weight Bias Predict Psychological Functioning?
Correlation between Internalized Weight Bias and Psychological Functioning
Pearson product-moment correlations were calculated to assess the strength of the relationships between internalized weight bias and measures of body image concern, self-esteem, anti-fat attitudes, depressive symptoms, anxiety, and stress. Table A1 (Appendix A) shows the correlations between baseline WBIS scores, post-treatment WBIS scores, follow-up WBIS scores and post-treatment and follow-up scores of each of the psychological variables.
Baseline WBIS scores were significantly and positively correlated with post-treatment BSQ scores and Fear of Fat scores, and negatively correlated with post-treatment RSE scores. Post-treatment WBIS scores were significantly and positively correlated with post-treatment BSQ scores, AAQ Dislike scores, AAQ Fear of Fat scores, DASS Total scores and DASS Depression scores. Post-treatment WBIS scores were significantly and negatively correlated with post-treatment RSE scores. Baseline and post-treatment WBIS scores were significantly and negatively correlated with follow-up RSE scores.
4. Discussion
The present study demonstrated that levels of internalized weight bias decrease over time among participants enrolled in behavioral weight loss treatment. The significant decrease in internalized weight bias occurred from pre-treatment to post-treatment, consistent with previous research [17,22,23], but it also continued to decrease from post-treatment to six-month follow-up. Similar to results from Mensinger and colleagues [22], these findings suggest that positive changes in internalized weight bias can be maintained, and even further improved, after the active treatment phase. In addition to reductions in internalized weight bias, participants also experienced other positive psychological changes during treatment. However, in contrast to the pattern of change in internalized weight bias, improvements in other psychological variables were either maintained at follow-up (e.g., self-esteem) or were reduced at follow-up (e.g., depressive symptoms), rather than further improved.
There might be specific components of behavioral treatment which alleviate internalized weight bias. For example, the intervention’s group-based methodology may normalize participants’ experiences and concerns about being overweight, and in turn reduce the negative attributions individuals make about themselves. Alternatively, strategies included in behavioral weight loss treatment, such as self-monitoring or identification of triggers for overeating, may increase participants’ degree of self-awareness and sense of internal locus of control. An increase in the belief that participants can exert control over their thoughts and actions may directly challenge negative self-statements associated with internalized weight bias. To resolve this dissonance, participants may lessen their degree of belief in negative self-statements. Future research could address these hypotheses to explore possible mechanisms of change.
Additional analyses demonstrated that baseline levels of internalized weight bias were significantly and positively related to change in body weight from baseline to follow-up, a result not found in a previous study using the WBIS [17]. This finding indicates that higher initial internalized weight bias is associated with poorer weight loss outcomes. This converges with the finding that among participants completing treatment, those individuals reporting the lowest levels of internalized weight bias at baseline lost just over 10% of IBW at follow-up while individuals reporting the highest baseline levels lost just over 5% of IBW. These results highlight the importance of assessing and reducing internalized weight bias among individuals with obesity who are seeking weight loss, as it is possible that a reduction in internalized weight bias will enable greater improvements in health outcomes.
The relationship between degree of internalized weight bias and amount of weight lost during behavioral weight loss treatment may be attributable to several factors. Participants who hold stronger negative beliefs about themselves due to their weight may also be more likely to hold a belief that because of their overweight status, they are less likely to succeed in weight loss treatment. Having higher levels of internalized weight bias may also make it harder for these participants to recover from perceived failures in treatment or make behavioral changes, such as improvements in healthy eating, which would result in additional weight loss. This possibility is consistent with multiple studies demonstrating a significant positive relationship between internalized weight bias and disordered eating behaviors [16,44]. Alternatively, high baseline levels of internalized weight bias may simply correlate with other markers of poor overall functioning (e.g., poor self-esteem, high body image concern) and this general factor of negative wellbeing may result in poorer weight loss outcomes. However, the relationships between these other psychological variables and weight loss appears to have been less robust in the present study than the relationship between internalized weight bias and weight loss.
The significant correlations found between baseline levels of internalized bias and subsequent weight change suggest a predictive relationship between internalized weight bias and weight change. These findings are similar to a study of bariatric surgery outcomes in which greater preoperative internalized weight bias was associated with less weight loss following surgery [27]. However, these results are not consistent across studies. In a yearlong study that followed individuals who successfully maintained intentional weight loss, higher baseline internalized weight bias predicted weight change (i.e., weight regain) among men but not women [25]. Additionally, previous research has established that psychological and behavioral variables are often weak predictors of weight change among participants enrolled in behavioral weight loss treatments [45]. Currently, the role of internalized weight bias predicting weight change over time remains unclear. Therefore, additional research is needed to assess whether the present study results demonstrate that internalized weight bias can be reliably used to predict long-term treatment outcome.
In addition to demonstrating a relationship between internalized weight bias and weight change, the present study also found a relationship between internalized weight bias and measures of psychological functioning. These findings are similar to results found by Carels et al. [17], who showed that internalized weight bias was significantly related to changes in body image concern but unrelated to levels of depressive symptoms.
The findings from the present study suggest that behavioral weight loss treatment may effect positive change on internalized weight bias, even without specific intervention strategies to specifically target these attitudes. Future research may look to augment behavioral weight loss treatment protocols with modules designed to reduce internalized weight bias, as has been done with interventions to improve body image, e.g., [7,46], and fat phobia, e.g., [47].
Because we found that participants with higher baseline levels of internalized weight bias lost significantly less weight than participants with lower baseline levels, treatments might do well to address internalized weight bias among participants, specifically those who endorse high levels at baseline, prior to or instead of taking part in a weight loss treatment protocol. The approach of addressing weight-related beliefs prior to modifying lifestyle habits has been taken in studies using non-dieting approaches to healthy eating and activity [48].
The heterogeneity of the sample is a strength of this study. Participants included men and women of varied ages and racial groups, increasing the generalizability of findings. Though multiple races were represented, the number of participants from several minority groups (e.g., African American and Latino/a) was small. Additional research with racial and ethnic minority groups is needed to confirm that present findings extend to these populations.
The use of self-report questionnaires is a limitation of the present study, as this method can introduce self-report bias resulting from scale construction and presentation of items and participant characteristics [49]. Each of the self-report questionnaires that were used have been studied among adults with overweight and obesity; however, more research is needed to provide further evidence of validity in overweight samples. The present study is also limited by participant attrition and the use of imputation methods to account for missing data, though the rate presented is comparable to other behavioral weight loss treatment studies [50]. It is not known if variables that were not assessed in the present study, such as level of social support or social media usage, might have confounded results or modified the observed effects. Finally, though results indicate a statistically significant difference for changes in internalized weight bias, it is unknown whether this change represents a clinically meaningful improvement. Additional research is needed to ensure that quantitative changes on self-report measures translate into real-world outcomes, particularly studies designed to directly address and manipulate internalized bias. Considering these limitations and the multiplicity of analyses, cautious overall interpretation of results is encouraged.
Future research in this area could further explore the nature of observed changes in internalized weight bias across behavioral weight loss treatment. It is particularly important to include follow-up assessment points after the active treatment phase, given the challenge with maintenance of weight loss following behavioral treatment. Despite potential challenges to reducing the internalization of weight bias among persons with overweight and obesity, the field continues to move forward with the development of interventions to change these types of beliefs. Recent interventions have successfully reduced internalized weight bias using techniques found in traditional cognitive-behavioral therapy [51,52]. Other researchers have targeted internalized weight bias using mindfulness- and acceptance-based principles [53,54,55,56]. For example, Lillis and colleagues facilitated a one-day weight bias intervention using Acceptance and Commitment Therapy [56]. As research continues to identify and understand the correlates and effects of weight-based stigmatization and the internalization of stereotypes, future studies should prioritize further exploration and development of interventions to address the negative impact of internalized weight bias.
Author Contributions
Conceptualization, J.D.L. and K.S.O.; methodology and investigation, J.D.L.; formal analysis and writing, R.D.M.; manuscript review and editing, J.D.L. and K.S.O. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted according to the guidelines of the Declaration of Helsinki and was approved by the Institutional Review Board of the University of Hawai‘i at Mānoa (Protocol #15527; Approval Date: September 2009).
Informed Consent Statement
Informed consent was obtained from all participants involved in this study.
Data Availability Statement
Data supporting reported results will be provided upon request to the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A

{kind=link}
{kind=link}
{kind=link}
Table A1.
Pearson product-moment correlations among internalized weight bias scores at post-treatment and follow-up and psychological functioning.
Table A1.
Pearson product-moment correlations among internalized weight bias scores at post-treatment and follow-up and psychological functioning.
| Baseline WBIS | Post-Treatment WBIS | Follow-Up WBIS | |
|---|---|---|---|
| Post-Treatment Scores | |||
| BMI | 0.07 | 0.15 | 0.06 |
| BSQ | 0.53 ** | 0.60 ** | 0.72 ** |
| RSE | −0.41 ** | −0.67 ** | −0.65 ** |
| AAQ Dislike | −0.07 | 0.37 * | a. |
| AAQ Fear of Fat | 0.37 * | 0.66 ** | a. |
| AAQ Willpower | 0.11 | 0.21 | 0.11 |
| DASS Total | 0.19 | 0.30 * | 0.25 |
| DASS Depression | 0.23 | 0.43 ** | 0.37 * |
| DASS Anxiety | 0.25 | 0.21 | 0.2 |
| DASS Stress | 0.06 | 0.15 | 0.11 |
| Follow-Up Scores | |||
| BMI | 0.12 | 0.18 | 0.15 |
| BSQ | 0.28 | 0.15 | a. |
| RSE | −0.47 ** | −0.35 * | a. |
| AAQ Dislike | a. | a. | a. |
| AAQ Fear of Fat | a. | a. | a. |
| AAQ Willpower | a. | a. | a. |
| DASS Total | 0.03 | 0.11 | a. |
| DASS Depression | 0.13 | 0.25 | a. |
| DASS Anxiety | −0.06 | −0.08 | a. |
| DASS Stress | 0.02 | 0.1 | a. |
Note. Data presented are from the Intention-to-Treat analysis. Cells containing the a. superscript had an n of less than 30 and were eliminated due to limited generalizability. BMI = Body Mass Index; WBIS = Weight Bias Internalization Scale; BSQ = Body Shape Questionnaire; RSE = Rosenberg Self-Esteem Scale; AAQ Dislike = Anti-Fat Attitudes Questionnaire Dislike subscale; AAQ Fear of Fat = Anti-Fat Attitudes Questionnaire Fear of Fat subscale; AAQ Willpower = Anti-Fat Attitudes Questionnaire Willpower subscale; DASS Total = Depression Anxiety Stress Scales Total Score; DASS Depression = Depression Anxiety Stress Scales Depression subscale; DASS Anxiety = Depression Anxiety Stress Scales Anxiety subscale; DASS Stress = Depression Anxiety Stress Scales Stress subscale. * p < 0.05. ** p < 0.01.
References
- Fryar, C.D.; Carroll, M.; Afful, J. Prevalence of Overweight, Obesity, and Severe Obesity among Adults Aged 20 and Over: United States, 1960–1962 through 2017–2018. Available online: https://www.cdc.gov/nchs/data/hestat/obesity-adult-17-18/obesity-adult.htm (accessed on 5 December 2021).
- Varkevisser, R.D.M.; van Stralen, M.M.; Kroeze, W.; Ket, J.C.F.; Steenhuis, I.H.M. Determinants of weight loss maintenance: A systematic review. Obes. Rev. 2019, 20, 171–211. [Google Scholar] [CrossRef] [Green Version]
- Christian, J.G.; Tsai, A.G.; Bessesen, D.H. Interpreting weight losses from lifestyle modification trials: Using categorical data. Int. J. Obes. 2010, 34, 207–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wadden, T.A.; Butryn, M.L.; Byrne, K.J. Efficacy of Lifestyle Modification for Long-Term Weight Control. Obes. Res. 2004, 12, 151S–162S. [Google Scholar] [CrossRef]
- Sarwer, D.B.; von Sydow Green, A.; Vetter, M.L.; Wadden, T.A. Behavior therapy for obesity: Where are we now? Curr. Opin. Endocrinol. Diabetes Obes. 2009, 16, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Lasikiewicz, N.; Myrissa, K.; Hoyland, A.; Lawton, C.L. Psychological benefits of weight loss following behavioural and/or dietary weight loss interventions. A systematic research review. Appetite 2014, 72, 123–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramirez, E.M.; Rosen, J.C. A comparison of weight control and weight control plus body image therapy for obese men and women. J. Consult. Clin. Psychol. 2001, 69, 440–446. [Google Scholar] [CrossRef] [PubMed]
- Halyburton, A.K.; Brinkworth, G.D.; Wilson, C.J.; Noakes, M.; Buckley, J.D.; Keogh, J.B.; Clifton, P.M. Low- and high- carbohydrate weight-loss diets have similar effects on mood but not cognitive performance. Am. J. Clin. Nutr. 2007, 86, 580–587. [Google Scholar] [CrossRef] [PubMed]
- Foster, G.D.; Wadden, T.A.; Kendall, P.C.; Stunkard, A.J.; Vogt, R.A. Psychological effects of weight loss and regain: A prospective evaluation. J. Consult. Clin. Psychol. 1996, 64, 752–757. [Google Scholar] [CrossRef] [PubMed]
- Fabricatore, A.N.; Wadden, T.A.; Higginbotham, A.J.; Faulconbridge, L.F.; Nguyen, A.M.; Heymsfield, S.B.; Faith, M.S. Intentional weight loss and changes in symptoms of depression: A systematic review and meta-analysis. Int. J. Obes. 2011, 35, 1363–1376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blaine, B.E.; Rodman, J.; Newman, J.M. Weight loss treatment and psychological well-being: A review and meta-analysis. J. Health Psychol. 2007, 12, 66–82. [Google Scholar] [CrossRef] [PubMed]
- Grilo, C.M.; Masheb, R.M. A randomized controlled comparison of guided self-help cognitive behavioral therapy and behavioral weight loss for binge eating disorder. Behav. Res. Ther. 2005, 43, 1509–1525. [Google Scholar] [CrossRef] [PubMed]
- Wadden, T.A.; Foster, G.D.; Sarwer, D.B.; Anderson, D.A.; Gladis, M.; Sanderson, R.S.; Letchak, R.V.; Berkowitz, R.I.; Phelan, S. Dieting and the development of eating disorders in obese women: Results of a randomized controlled trial. Am. J. Clin. Nutr. 2004, 80, 560–568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palmeira, A.L.; Branco, T.L.; Martins, S.C.; Minderico, C.S.; Silva, M.N.; Vieira, P.N.; Barata, J.T.; Serpa, S.O.; Sardinha, L.B.; Teixeira, P.J. Change in body image and psychological well-being during behavioral obesity treatment: Associations with weight loss and maintenance. Body Image 2010, 7, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Palmeira, A.L.; Markland, D.A.; Silva, M.N.; Branco, T.L.; Martins, S.C.; Minderico, C.S.; Vieira, P.N.; Barata, J.T.; Serpa, S.O.; Sardinha, L.B.; et al. Reciprocal effects among changes in weight, body image, and other psychological factors during behavioral obesity treatment: A mediation analysis. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durso, L.E.; Latner, J.D. Understanding self-directed stigma: Development of the weight bias internalization scale. Obesity 2008, 16 (Suppl. 2), S80–S86. [Google Scholar] [CrossRef]
- Carels, R.A.; Wott, C.B.; Young, K.M.; Gumble, A.; Koball, A.; Oehlhof, M.W. Implicit, explicit, and internalized weight bias and psychosocial maladjustment among treatment-seeking adults. Eat. Behav. 2010, 11, 180–185. [Google Scholar] [CrossRef] [PubMed]
- Durso, L.E.; Latner, J.D.; Ciao, A.C. Weight bias internalization in treatment-seeking overweight adults: Psychometric validation and associations with self-esteem, body image, and mood symptoms. Eat. Behav. 2016, 21, 104–108. [Google Scholar] [CrossRef] [PubMed]
- Pearl, R.L.; White, M.A.; Grilo, C.M. Weight bias internalization, depression, and self-reported health among overweight binge eating disorder patients. Obesity 2014, 22, E142–E148. [Google Scholar] [CrossRef] [Green Version]
- Pearl, R.L.; Puhl, R.M. Weight bias internalization and health: A systematic review. Obes. Rev. 2018, 19, 1141–1163. [Google Scholar] [CrossRef] [Green Version]
- Lillis, J.; Thomas, J.G.; Levin, M.E.; Wing, R.R. Self-stigma and weight loss: The impact of fear of being stigmatized. J. Health Psychol. 2020, 25, 922–930. [Google Scholar] [CrossRef]
- Mensinger, J.L.; Calogero, R.M.; Tylka, T.L. Internalized weight stigma moderates eating behavior outcomes in women with high BMI participating in a healthy living program. Appetite 2016, 102, 32–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mensinger, J.L.; Meadows, A. Internalized weight stigma mediates and moderates physical activity outcomes during a healthy living program for women with high body mass index. Psychol. Sport Exerc. 2017, 30, 64–72. [Google Scholar] [CrossRef] [Green Version]
- Carels, R.A.; Selensky, J.C.; Rossi, J.; Solar, C.; Hlavka, R. A novel stepped-care approach to weight loss: The role of self-monitoring and health literacy in treatment outcomes. Eat. Behav. 2017, 26, 76–82. [Google Scholar] [CrossRef]
- Olson, K.L.; Lillis, J.; Graham Thomas, J.; Wing, R.R. Prospective evaluation of internalized weight bias and weight change among successful weight-loss maintainers. Obesity 2018, 26, 1888–1892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pearl, R.L.; Puhl, R.M.; Lessard, L.M.; Himmelstein, M.S.; Foster, G.D. Prevalence and correlates of weight bias internalization in weight management: A multinational study. SSM Popul. Health 2021, 13, 100755. [Google Scholar] [CrossRef] [PubMed]
- Lent, M.R.; Napolitano, M.A.; Wood, G.C.; Argyropoulos, G.; Gerhard, G.S.; Hayes, S.; Foster, G.D.; Collins, C.A.; Still, C.D. Internalized weight bias in weight-loss surgery patients: Psychosocial correlates and weight loss outcomes. Obes. Surg. 2014, 24, 2195–2199. [Google Scholar] [CrossRef]
- Raves, D.M.; Brewis, A.; Trainer, S.; Han, S.-Y.; Wutich, A. Bariatric surgery patients’ perceptions of weight-related stigma in healthcare settings impair post-surgery dietary adherence. Front. Psychol. 2016, 7, 1497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Latner, J.D.; Ciao, A.C.; Wendicke, A.U.; Murakami, J.M.; Durso, L.E. Community-based behavioral weight-loss treatment: Long-term maintenance of weight loss, physiological, and psychological outcomes. Behav. Res. Ther. 2013, 51, 451–459. [Google Scholar] [CrossRef]
- Group, D.P.P.R. The Diabetes Prevention Program (DPP): Description of lifestyle intervention. Diabetes Care 2002, 25, 2165–2171. [Google Scholar] [CrossRef] [Green Version]
- Crandall, C.S. Prejudice against fat people: Ideology and self-interest. J. Pers. Soc. Psychol. 1994, 66, 882–894. [Google Scholar] [CrossRef]
- Elison, Z.M.; Çiftçi, A. Digesting antifat attitudes: Locus of control and social dominance orientation. Transl. Issues Psychol. Sci. 2015, 1, 262–270. [Google Scholar] [CrossRef]
- Rosenberg, M. Society and the Adolescent Self-Image; Princeton University Press: Princeton, NJ, USA, 1965; pp. 16–38. [Google Scholar]
- Lucas, R.E.; Diener, E.; Suh, E. Discriminant validity of well-being measures. J. Pers. Soc. Psychol. 1996, 71, 616–628. [Google Scholar] [CrossRef] [PubMed]
- Jones, M.; Grilo, C.M.; Masheb, R.M.; White, M.A. Psychological and behavioral correlates of excess weight: Misperception of obese status among persons with class II obesity. Int. J. Eat. Disord. 2010, 43, 628–632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herbozo, S.; Schaefer, L.M.; Thompson, J.K. A comparison of eating disorder psychopathology, appearance satisfaction, and self-esteem in overweight and obese women with and without binge eating. Eat. Behav. 2015, 17, 86–89. [Google Scholar] [CrossRef] [PubMed]
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Antony, M.M.; Bieling, P.J.; Cox, B.J.; Enns, M.W.; Swinson, R.P. Psychometric properties of the 42-item and 21-item versions of the Depression Anxiety Stress Scales in clinical groups and a community sample. Psychol. Assess. 1998, 10, 176–181. [Google Scholar] [CrossRef]
- Setayesh, L.; Ebrahimi, R.; Pooyan, S.; Yarizadeh, H.; Rashidbeygi, E.; Badrooj, N.; Imani, H.; Mirzaei, K. The possible mediatory role of adipokines in the association between low carbohydrate diet and depressive symptoms among overweight and obese women. PLoS ONE 2021, 16, e0257275. [Google Scholar] [CrossRef]
- Coffino, J.A.; Spoor, S.P.; Drach, R.D.; Hormes, J.M. Food insecurity among graduate students: Prevalence and association with depression, anxiety and stress. Public Health Nutr. 2021, 24, 1889–1894. [Google Scholar] [CrossRef]
- Dowson, J.; Henderson, L. The validity of a short version of the body shape questionnaire. Psychiatry Res. 2001, 102, 263–271. [Google Scholar] [CrossRef]
- Cooper, P.J.; Taylor, M.J.; Cooper, Z.; Fairburn, C.G. The development and validation of the body shape questionnaire. Int. J. Eat. Disord. 1987, 6, 485–494. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: New York, NY, USA, 1988; pp. 20–27. [Google Scholar]
- Marshall, R.D.; Latner, J.D.; Masuda, A. Internalized weight bias and disordered eating: The mediating role of body image avoidance and drive for thinness. Front. Psychol. 2020, 10, 2999. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, P.J.; Going, S.B.; Sardinha, L.B.; Lohman, T.G. A review of psychosocial pre-treatment predictors of weight control. Obes. Rev. 2005, 6, 43–65. [Google Scholar] [CrossRef] [PubMed]
- Katzer, L.; Bradshaw, A.J.; Horwath, C.C.; Gray, A.R.; O’Brien, S.; Joyce, J. Evaluation of a “nondieting” stress reduction program for overweight women: A randomized trial. Am. J. Health Promot. 2008, 22, 264–274. [Google Scholar] [CrossRef] [PubMed]
- Robinson, B.E.; Bacon, J.G. The “If only I were thin…” treatment program: Decreasing the stigmatizing effects of fatness. Prof. Psychol. Res. Pract. 1996, 27, 175–183. [Google Scholar] [CrossRef]
- Bacon, L.; Keim, N.L.; Van Loan, M.D.; Derricote, M.; Gale, B.; Kazaks, A.; Stern, J.S. Evaluating a ‘non-diet’ wellness intervention for improvement of metabolic fitness, psychological well-being and eating and activity behaviors. Int. J. Obes. Relat. Metab. Disord. 2002, 26, 854–865. [Google Scholar] [CrossRef] [Green Version]
- Podsakoff, P.M.; MacKenzie, S.B.; Lee, J.Y.; Podsakoff, N.P. Common method biases in behavioral research: A critical review of the literature and recommended remedies. J. Appl. Psychol. 2003, 88, 879–903. [Google Scholar] [CrossRef] [PubMed]
- Dansinger, M.L.; Tatsioni, A.; Wong, J.B.; Chung, M.; Balk, E.M. Meta-analysis: The effect of dietary counseling for weight loss. Ann. Intern. Med. 2007, 147, 41–50. [Google Scholar] [CrossRef]
- Pearl, R.L.; Wadden, T.A.; Bach, C.; Gruber, K.; Leonard, S.; Walsh, O.A.; Tronieri, J.S.; Berkowitz, R.I. Effects of a cognitive-behavioral intervention targeting weight stigma: A randomized controlled trial. J. Consult. Clin. Psychol. 2020, 88, 470–480. [Google Scholar] [CrossRef] [PubMed]
- Pearl, R.L.; Hopkins, C.; Berkowitz, R.; Wadden, T. Group cognitive-behavioral treatment for internalized weight stigma: A pilot study. Eat. Weight Disord. 2018, 23, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Levin, M.E.; Potts, S.; Haeger, J.; Lillis, J. Delivering acceptance and commitment therapy for weight self-stigma through guided self-help: Results from an open pilot trial. Cogn. Behav. Pract. 2018, 25, 87–104. [Google Scholar] [CrossRef] [Green Version]
- Palmeira, L.; Pinto-Gouveia, J.; Cunha, M. Exploring the efficacy of an acceptance, mindfulness & compassionate-based group intervention for women struggling with their weight (Kg-Free): A randomized controlled trial. Appetite 2017, 112, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Berman, M.I.; Morton, S.N.; Hegel, M.T. Uncontrolled pilot study of an acceptance and commitment therapy and health at every size intervention for obese, depressed women: Accept yourself! Psychotherapy 2016, 53, 462–467. [Google Scholar] [CrossRef] [PubMed]
- Lillis, J.; Hayes, S.C.; Bunting, K.; Masuda, A. Teaching acceptance and mindfulness to improve the lives of the obese: A preliminary test of a theoretical model. Ann. Behav. Med. 2009, 37, 58–69. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Participant flow through this study.

Figure 2.
Using the Intention-to-Treat analysis, figure represents the percent change in initial body weight at post-treatment and follow-up for participants reporting low baseline Weight Bias Internalization Scale scores and those reporting high baseline Weight Bias Internalization Scale scores.
Figure 2.
Using the Intention-to-Treat analysis, figure represents the percent change in initial body weight at post-treatment and follow-up for participants reporting low baseline Weight Bias Internalization Scale scores and those reporting high baseline Weight Bias Internalization Scale scores.

Figure 3.
Using treatment completers only, figure represents the percent change in initial body weight at post-treatment and follow-up for participants reporting low baseline Weight Bias Internalization Scale scores and those reporting high baseline Weight Bias Internalization Scale scores.
Figure 3.
Using treatment completers only, figure represents the percent change in initial body weight at post-treatment and follow-up for participants reporting low baseline Weight Bias Internalization Scale scores and those reporting high baseline Weight Bias Internalization Scale scores.

Table 1.
Mean scores of all study measures.
| Measure | Baseline | Post-Treatment | Six-Month Follow-Up | Univariate F (df1, df2) |
|---|---|---|---|---|
| BMI (Completers) | 35.66 (7.67) a | 32.43 (6.67) b | 31.92 (6.13) b | 22.83 (2, 60) * |
| BMI (ITT) | 35.66 (7.67) a | 34.73 (7.91) b | 34.21 (7.99) c | 30.27 (1.72, 169.74) *,† |
| WBIS | 3.83 (1.05) a | 3.55 (0.72) b | 3.40 (1.30) c | 12.05 (1.79, 185.89) *,† |
| BSQ | 3.61 (1.11) a | 2.86 (1.14) a | 2.95 (1.18) a | 0.26 (1.88, 184.12) † |
| RSE | 3.12 (0.51) a | 3.31 (0.51) b | 3.23 (0.54) b | 10.07 (1.81, 187.68) *,† |
| AAQ Dislike | 1.46 (1.19) a | 1.23 (1.45) b | 0.48 (0.57) c | 60.13 (2, 208) * |
| AAQ Fear of Fat | 4.93 (2.18) a | 4.74 (2.33) a | 3.81 (3.04) b | 21.37 (1.79, 186.63) *,† |
| AAQ Willpower | 4.68 (1.77) a | 4.66 (1.88) a | 3.69 (2.02) b | 32.58 (1.70, 176.34) *,† |
| DASS Total | 0.57 (0.44) a | 0.49 (0.44) a | 1.02 (0.62) b | 66.69 (2, 208) * |
| DASS Depression | 0.64 (0.51) a | 0.46 (0.50) b | 0.98 (0.67) c | 51.95 (2, 208) * |
| DASS Anxiety | 0.53 (0.43) a | 0.35 (0.40) b | 0.84 (0.61) c | 51.14 (2, 208) * |
| DASS Stress | 0.83 (0.51) a | 0.67 (0.60) b | 1.25 (0.72) c | 49.13 (2, 208) * |
Note. * p < 0.005. † Greenhouse–Geisser correction applied due to violation of the assumption of sphericity. Different superscripts across time points indicate significant contrasts between means. BMI = Body Mass Index; %IBW = percent change in initial body weight; ITT = Intention-to-Treat; WBIS = Weight Bias Internalization Scale; BSQ = Body Shape Questionnaire; RSE = Rosenberg Self-Esteem Scale; AAQ = Anti-Fat Attitudes Questionnaire; DASS = Depression Anxiety Stress Scales.
Table 2.
Pearson product-moment correlations among percent change in body weight and baseline internalized weight bias and psychological functioning.
Table 2.
Pearson product-moment correlations among percent change in body weight and baseline internalized weight bias and psychological functioning.
| % Change in Body Weight at Post-Treatment | % Change in Body Weight at Follow-Up | |
|---|---|---|
| Baseline Body Mass Index | 0.13 | 0.10 |
| Baseline Weight Bias Internalization Scale | 0.14 | 0.26 ** |
| Baseline Body Shape Questionnaire | 0.16 | 0.22 * |
| Baseline Rosenberg Self-Esteem Scale | −0.21 * | −0.28 ** |
| Baseline Anti-Fat Attitudes Scale Total Score | 0.02 | −0.02 |
| Baseline Anti-Fat Attitudes Scale Dislike subscale | −0.03 | −0.03 |
| Baseline Anti-Fat Attitudes Scale Fear of Fat subscale | 0.01 | 0.13 |
| Baseline Anti-Fat Attitudes Scale Willpower subscale | 0.03 | −0.15 |
| Baseline Depression Anxiety Stress Scale Total Score | 0.15 | 0.20 |
| Baseline Depression Anxiety Stress Scale Depression subscale | 0.05 | 0.11 |
| Baseline Depression Anxiety Stress Scale Anxiety subscale | 0.00 | 0.07 |
| Baseline Depression Anxiety Stress Scale Stress subscale | 0.22 | 0.22 |
Note. % Change in body weight at post-treatment = percent change in initial body weight from baseline to post-treatment; % change in body weight at follow-up = percent change in initial body weight from baseline to follow-up. * p < 0.05; ** p < 0.01.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Marshall, R.D.; O’Brien, K.S.; Latner, J.D. The Relationship of Internalized Weight Bias to Weight Change in Treatment-Seeking Overweight Adults. Obesities 2022, 2, 21-34. https://0-doi-org.brum.beds.ac.uk/10.3390/obesities2010003
AMA Style
Marshall RD, O’Brien KS, Latner JD. The Relationship of Internalized Weight Bias to Weight Change in Treatment-Seeking Overweight Adults. Obesities. 2022; 2(1):21-34. https://0-doi-org.brum.beds.ac.uk/10.3390/obesities2010003
Chicago/Turabian StyleMarshall, Rachel D., Kerry S. O’Brien, and Janet D. Latner. 2022. "The Relationship of Internalized Weight Bias to Weight Change in Treatment-Seeking Overweight Adults" Obesities 2, no. 1: 21-34. https://0-doi-org.brum.beds.ac.uk/10.3390/obesities2010003