
Weight Concern and Body Image Dissatisfaction among Hispanic and African American Women
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.3. Measures
2.3.1. Health Survey
2.3.2. Stunkard Figure Rating Scale (SFRS) [25]
2.4. Statistical Analysis
3. Results
3.1. Sample Descriptive Characteristics
3.2. Ethnic Differences in Body Size Ideal, BID, and Weight Concern
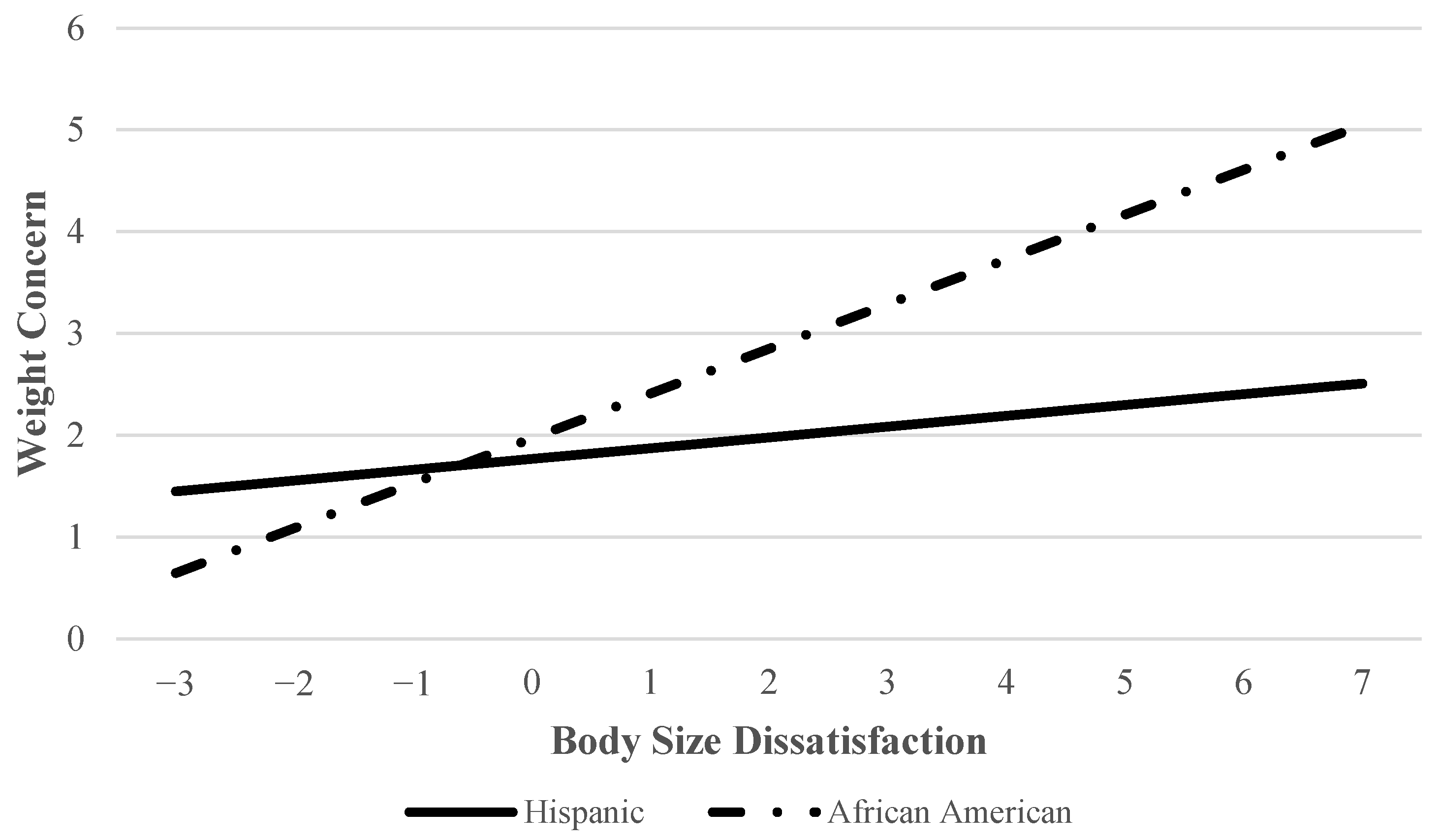
3.3. Contribution of Key Variables to Weight Concern and Interaction Effect
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hales, C.M.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Prevalence of obesity and severe obesity among adults: United States, 2017–2018. NCHS Data Brief 2020, 360, 1–8. [Google Scholar]
- Wang, Y.; Beydoun, M.A.; Min, J.; Xue, H.; Kaminsky, L.A.; Cheskin, L.J. Has the prevalence of overweight, obesity, and central obesity leveled off in the United States? Trends, patterns, disparities, and future projections for the obesity epidemic. Int. J. Epidemiol. 2020, 49, 810–823. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, L.M.; Burke, N.L.; Anderson, L.M.; Thompson, J.K.; Heinberg, L.J.; Bardone-Cone, A.M.; Higgins Neyland, M.K.; Frederick, D.A.; Anderson, D.A.; Schaumberg, K.; et al. Comparing internalization of appearance ideals and appearance-related pressures among women from the United States, Italy, England, and Australia. Eat. Weight Disord. 2019, 24, 947–951. [Google Scholar] [CrossRef]
- Bibiloni, M.D.M.; Coll, J.L.; Pich, J.; Pons, A.; Tur, J.A. Body image satisfaction and weight concern among a Mediterranean adult population. BMC Public Health 2017, 17, 39. [Google Scholar] [CrossRef] [PubMed]
- Almenara, C.A.; Machackova, H.; Smahel, D. Sociodemographic, attitudinal, and behavioral correlates of using nutrition, weight loss, and fitness websites: An online survey. J. Med. Internet Res. 2019, 21, e10189. [Google Scholar] [CrossRef]
- Bouzas, C.; Bibiloni, M.D.M.; Tur, J.A. Relationship between body image and body weight control in overweight ≥ 55-year-old adults: A systematic review. Int. J. Environ. Res. Public Health 2019, 16, 1622. [Google Scholar] [CrossRef]
- Higgins, E.T. Beyond pleasure and pain. Am. Psychol. 1997, 52, 1280–1300. [Google Scholar] [CrossRef] [PubMed]
- Olson, K.L.; Lillis, J.; Panza, E.; Wing, R.R.; Quinn, D.M.; Puhl, R.R. Body shape concerns across racial and ethnic groups among adults in the United States: More similarities than differences. Body Image 2020, 35, 108–113. [Google Scholar] [CrossRef]
- Chen, J.Y.; Berner, L.A.; Brown, T.A.; Wierenga, C.E.; Kaye, W.H. Associations of elevated weight status with symptom severity and treatment outcomes in binge/purge eating disorders. Int. J. Eat. Disord. 2021, 54, 621–626. [Google Scholar] [CrossRef]
- Nightingale, B.A.; Cassin, S.E. Disordered eating among individuals with excess weight: A review of recent research. Curr. Obes. Rep. 2019, 8, 112–127. [Google Scholar] [CrossRef]
- Ahmed, M.S.; Anee, K.F.; Abid, M.T.; Hridoy, M.O.; Hasan, A.R.; Marufa, M.T.; Hassan, T.; Munmun, S. Prevalence of obesity and dietary habits of university students: A cross-sectional study. Asian J. Med. Biol. Res. 2019, 5, 180–185. [Google Scholar] [CrossRef]
- Vannucci, A.; Ohannessian, C.M. Body image dissatisfaction and anxiety trajectories during adolescence. J. Clin. Child Adolesc. Psychol. 2017, 47, 785–795. [Google Scholar] [CrossRef] [PubMed]
- Flores-Comejo, F.; Kamego-Tome, M.; Zapata-Pachas, M.A.; Alvarado, G.F. Association between body image dissatisfaction and depressive symptoms in adolescents. Braz. J. Psychiatry 2017, 39, 316–322. [Google Scholar] [CrossRef] [PubMed]
- Awad, G.H.; Kashubeck-West, S.; Bledman, R.A.; Coker, A.D.; Stinson, R.D.; Mintz, L.B. The role of enculturation, racial identity, and body mass index in the prediction of body dissatisfaction in African American women. J. Black Psychol. 2020, 46, 3–28. [Google Scholar] [CrossRef]
- Watson, L.B.; Lewis, J.A.; Moody, A.T. A sociocultural examination of body image among black women. Body Image 2019, 31, 280–287. [Google Scholar] [CrossRef] [PubMed]
- Markova, I.; Azocar, C. The influence of social media and fashion magazines on body image of culturally and racially diverse young women. In International Textile and Apparel Association Annual Conference Proceedings; Iowa State University Digital Press: Ames, IA, USA, 2018; Volume 75, Available online: https://lib.dr.iastate.edu/itaa_proceedings/2018/posters/.15 (accessed on 2 June 2022).
- Grabe, S.; Hyde, J.S. Ethnicity and body dissatisfaction among women in the United States: A meta-analysis. Psychol. Bull. 2006, 132, 622–640. [Google Scholar] [CrossRef]
- Brandsma, L.; Smith, G.; Barney, J.; Wolinsky, A.; Juarascio, A.S. Do I really look like that? Racial differences in the discrepancy between self and objective observer ratings of body size. J. Cult. Divers. 2019, 26, 49–53. [Google Scholar]
- Baruth, M.; Sharpe, P.A.; Magwood, G.; Wilcox, S.; Schlaff, R.A. Body size perceptions among overweight and obese African American women. Ethn. Dis. 2015, 25, 391–398. [Google Scholar] [CrossRef]
- Choi, J.; Bender, M.S.; Arai, S.; Fukuoka, Y. Factors associated with underestimation of weight status among Caucasian, Latino, Filipino, and Korean Americans—DiLH Survey. Ethn. Dis. 2015, 25, 200–207. [Google Scholar]
- Hughes, E. “I’m supposed to be thick”: Managing body image anxieties among Black American women. J. Black Stud. 2021, 52, 310–330. [Google Scholar] [CrossRef]
- Lewis, K.H.; Gudzune, K.A.; Fischer, H.; Yamamoto, A.; Young, D.R. Racial and ethnic minority patients report different weight-related care experiences than non-Hispanic Whites. Prev. Med. Rep. 2016, 4, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Fitzgibbon, M.L.; Blackman, L.R.; Avellone, M.E. The relationship between body image discrepancy and body mass index across ethnic groups. Obes. Res. 2000, 8, 582–589. [Google Scholar] [CrossRef] [PubMed]
- Mama, S.K.; Quill, B.E.; Fernandez-Esquer, M.E.; Reese-Smith, J.Y.; Banda, J.A.; Lee, R.E. Body image and physical activity among Latina and African American women. Ethn. Dis 2011, 21, 281–287. [Google Scholar] [PubMed]
- Stunkard, A.J.; Sørensen, T.; Schulsinger, F. Use of the Danish Adoption Register for the study of obesity and thinness. J. Nerv. Ment. Dis. 1983, 60, 115–120. [Google Scholar]
- Thompson, J.K.; Altabe, M.N. Psychometric qualities of the figure rating scale. Int. J. Eat. Disord. 1991, 10, 615–619. [Google Scholar] [CrossRef]
- Scagliusi, F.B.; Alvarenga, M.; Polacow, V.O.; Cordás, T.A.; de Oliveira Queiroz, G.K.; Coelho, D.; Philippi, S.T.; Lancha, A.H., Jr. Concurrent and discriminant validity of the Stunkard’s figure rating scale adapted into Portuguese. Appetite 2006, 47, 77–82. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Obesity Basics. Defining Adult Overweight & Obesity. Available online: https://www.cdc.gov/obesity/basics/adult-defining.html (accessed on 9 June 2022).
- Okop, K.J.; Mukumbang, F.C.; Mathole, T.; Levitt, N.; Puoane, T. Perceptions of body size, obesity threat and the willingness to lose weight among Black South African adults: A qualitative study. BMC Public Health 2016, 16, 365. [Google Scholar] [CrossRef]
- Sánchez-Johnsen, L.A.P.; Fitzgibbon, M.L.; Martinovich, Z.; Stolley, M.R.; Dyer, A.R.; Van Horn, L. Ethnic differences in correlates of obesity between Latin-American and Black women. Obes. Res. 2004, 12, 652–660. [Google Scholar] [CrossRef]
- Greaney, M.L.; Cohen, S.A.; Xu, F.; Ward-Ritacco, C.L.; Riebe, D. Healthcare provider counselling for weight management behaviours among adults with overweight or obesity: A cross-sectional analysis of National Health and Nutrition Examination Survey, 2011–2018. BMJ Open 2020, 10, e039295. [Google Scholar] [CrossRef]
- Gowers, S.G.; Shore, A. Development of weight and shape concerns in the aetiology of eating disorders. Br. J. Psychiatry 2001, 179, 236–242. [Google Scholar] [CrossRef]
- Menon, C.V.; Harter, S.L. Examining the impact of acculturative stress on body image disturbance among Hispanic college students. Cult. Divers. Ethn. Minor. Psychol. 2012, 18, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Kops, N.L.; Bessel, M.; Knauth, D.R.; Caleffi, M.; Wendland, E.M. Body image (dis)satisfaction among low-income adult women. Clin. Nutr. 2019, 38, 1317–1323. [Google Scholar] [CrossRef] [PubMed]
- Thoma, M.E.; Hediger, M.L.; Sunadram, R.; Stanford, J.B.; Peterson, C.M.; Croughan, M.S.; Chen, Z.; Buck Louis, G.M.; ENDO Study Working Group. Comparing apples and pears: Women’s perceptions of their body size and shape. J. Women’s Health 2012, 21, 1074–1081. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Total Sample N = 477 | Hispanic Women N = 366 | African American Women N = 111 | df | t | χ2 | p | Cramer’s V |
|---|---|---|---|---|---|---|---|---|
| Age M (SD) | 43.7 (15.9) | 40.3 (13.2) | 54.7 (19.0) | 144 | −7.44 | <0.001 | ||
| Household income n (%) | 2 | 36.13 | <0.001 | 0.30 | ||||
| ≤USD 2500/month | 212 (44.4) | 178 (48.6) | 34 (30.6) | |||||
| >USD 2500/month | 87 (18.2) | 46 (12.6) | 41 (36.9) | |||||
| Not sure | 113 (23.7) | 93 (25.4) | 20 (18.0) | |||||
| Did not answer | 65 (13.6) | 49 (13.4) | 16 (14.4) | |||||
| Perceived weight status n (%) | 3 | 4.01 | 0.26 | 0.10 | ||||
| Underweight | 2 (0.4) | 2 (0.5) | 0 (0.0) | |||||
| Healthy weight | 93 (19.5) | 64 (17.5) | 29 (26.1) | |||||
| Overweight | 122 (25.6) | 97 (26.5) | 25 (22.5) | |||||
| Obese | 171 (35.8) | 125 (34.2) | 46 (41.4) | |||||
| Did not answer | 89 (18.7) | 78 (21.3) | 11 (9.9) | |||||
| BMI a M (SD) | 29.9 (6.6) | 29.7 (6.3) | 30.5 (7.5) | 151 | −0.95 | 0.344 | ||
| Underweight | 3 (0.6) | 3 (0.8) | 0 (0.0) | |||||
| Healthy weight | 172 (36.1) | 122 (33.3) | 50 (45.0) | |||||
| Overweight | 249(52.2) | 202 (55.2) | 47 (42.3) | |||||
| Obese | 22 (4.6) | 17 (4.6) | 5 (4.5) | |||||
| Did not answer | 31 (6.5) | 22 (6.0) | 9 (8.1) | |||||
| Weight concern n (%) | 4 | 26.69 | <0.001 | 0.25 | ||||
| Not at all | 74 (15.5) | 55 (15.0) | 19 (17.1) | |||||
| Slightly | 111 (23.3) | 96 (26.2) | 15 (13.5) | |||||
| Somewhat | 77 (16.1) | 69 (18.9) | 8 (7.2) | |||||
| Moderately | 67 (14.0) | 43 (11.7) | 24 (21.6) | |||||
| Extremely | 100 (21.0) | 65 (17.8) | 35 (31.5) |
| Step 1 | Step 2 | Step 3 | Step 4 | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variable | B | SE B | β | t | p | B | SE B | Β | t | p | B | SE B | β | t | p | B | SE B | β | t | p |
| Age | 0.00 | 0.01 | 0.00 | −0.05 | 0.964 | 0.00 | 0.01 | 0.01 | 0.19 | 0.853 | 0.00 | 0.01 | 0.00 | 0.03 | 0.978 | 0.00 | 0.01 | 0.00 | −0.02 | 0.981 |
| Ethnicity a | 0.60 | 0.19 | 0.18 | 3.24 | 0.001 | 0.63 | 0.18 | 0.19 | 3.47 | 0.001 | 0.69 | 0.18 | 0.21 | 3.83 | 0.001 | 0.20 | 0.25 | 0.06 | 0.79 | 0.43 |
| BMI b | 0.57 | 0.09 | 0.33 | 6.07 | <0.001 | 0.20 | 0.13 | 0.12 | 1.58 | 0.116 | 0.10 | 0.13 | 0.05 | 0.72 | 0.471 | 0.10 | 0.13 | 0.06 | 0.75 | 0.457 |
| Self-labeled weight status | 0.75 | 0.17 | 0.31 | 4.29 | <0.001 | 0.61 | 0.18 | 0.25 | 3.39 | 0.001 | 0.6 | 0.18 | 0.25 | 3.36 | 0.001 | |||||
| BID c | 0.18 | 0.07 | 0.18 | 2.68 | 0.008 | 0.11 | 0.07 | 0.11 | 1.5 | 0.135 | ||||||||||
| Ethnicity × BID c | 0.33 | 0.12 | 0.21 | 2.69 | 0.008 | |||||||||||||||
| Overall model adjusted R2 | 0.13 | 0.18 | 0.20 | 0.21 | ||||||||||||||||
| F for change in R2 | 16.21 *** | 18.38 *** | 7.19 ** | 7.22 ** | ||||||||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olvera, N.; Matthews-Ewald, M.; Zhang, R.; Scherer, R.; Fan, W.; Arbona, C. Weight Concern and Body Image Dissatisfaction among Hispanic and African American Women. Women 2023, 3, 486-496. https://0-doi-org.brum.beds.ac.uk/10.3390/women3040037
Olvera N, Matthews-Ewald M, Zhang R, Scherer R, Fan W, Arbona C. Weight Concern and Body Image Dissatisfaction among Hispanic and African American Women. Women. 2023; 3(4):486-496. https://0-doi-org.brum.beds.ac.uk/10.3390/women3040037
Chicago/Turabian StyleOlvera, Norma, Molly Matthews-Ewald, Rongfang Zhang, Rhonda Scherer, Weihua Fan, and Consuelo Arbona. 2023. "Weight Concern and Body Image Dissatisfaction among Hispanic and African American Women" Women 3, no. 4: 486-496. https://0-doi-org.brum.beds.ac.uk/10.3390/women3040037