

Safety and Effectiveness of Naproxen 220 mg + Paracetamol 300 mg + Pamabrom 25 mg Fixed Dose Combination in Women with Premenstrual Syndrome: A Post-Marketing, Open-Label, Uncontrolled, Prospective, Multicenter, Observational Study
 ,
,
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
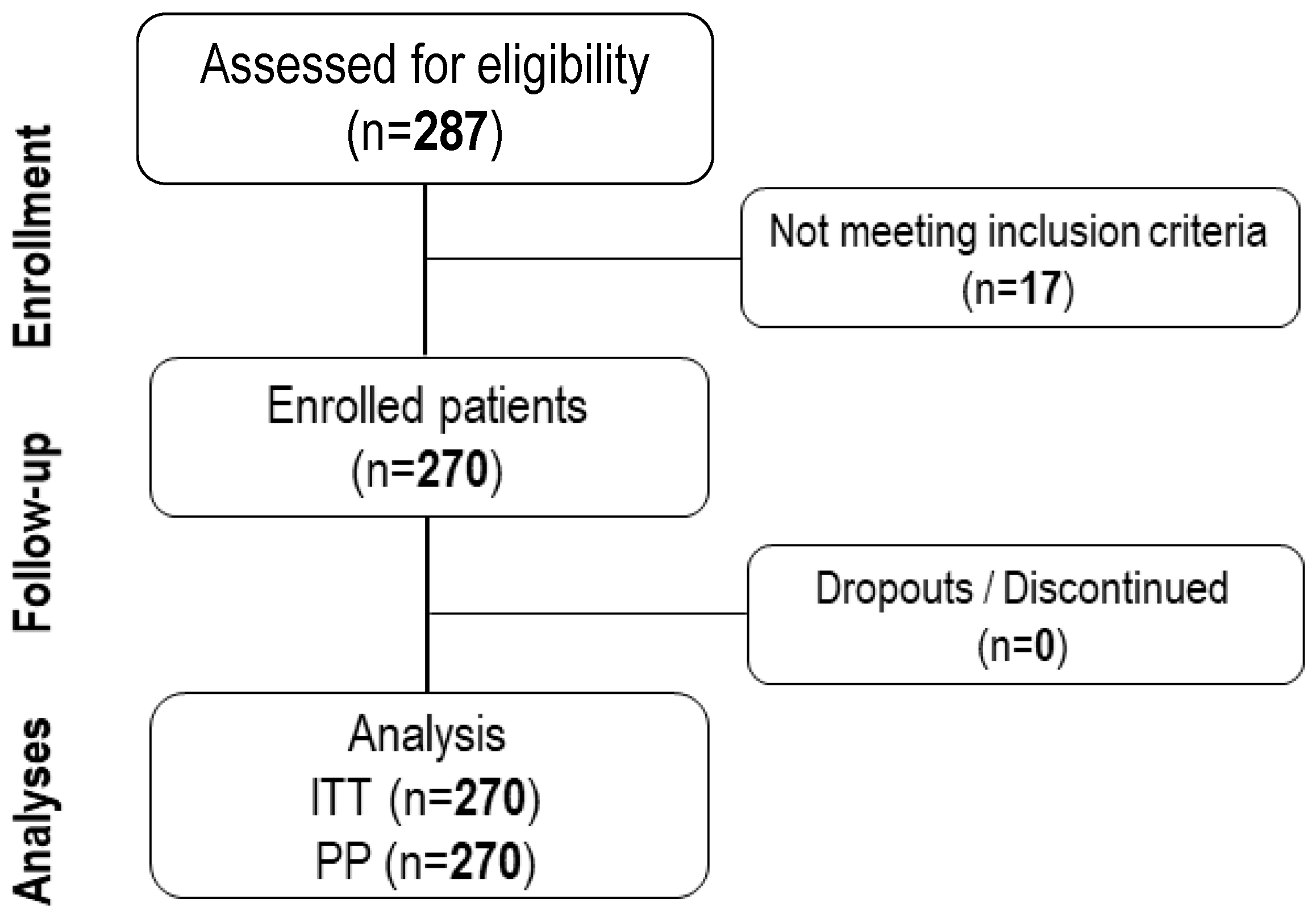
4.1. Study Design and Patients
4.2. Ethics
4.3. Study Medication
4.4. Safety and Effectiveness Variables
- (a)
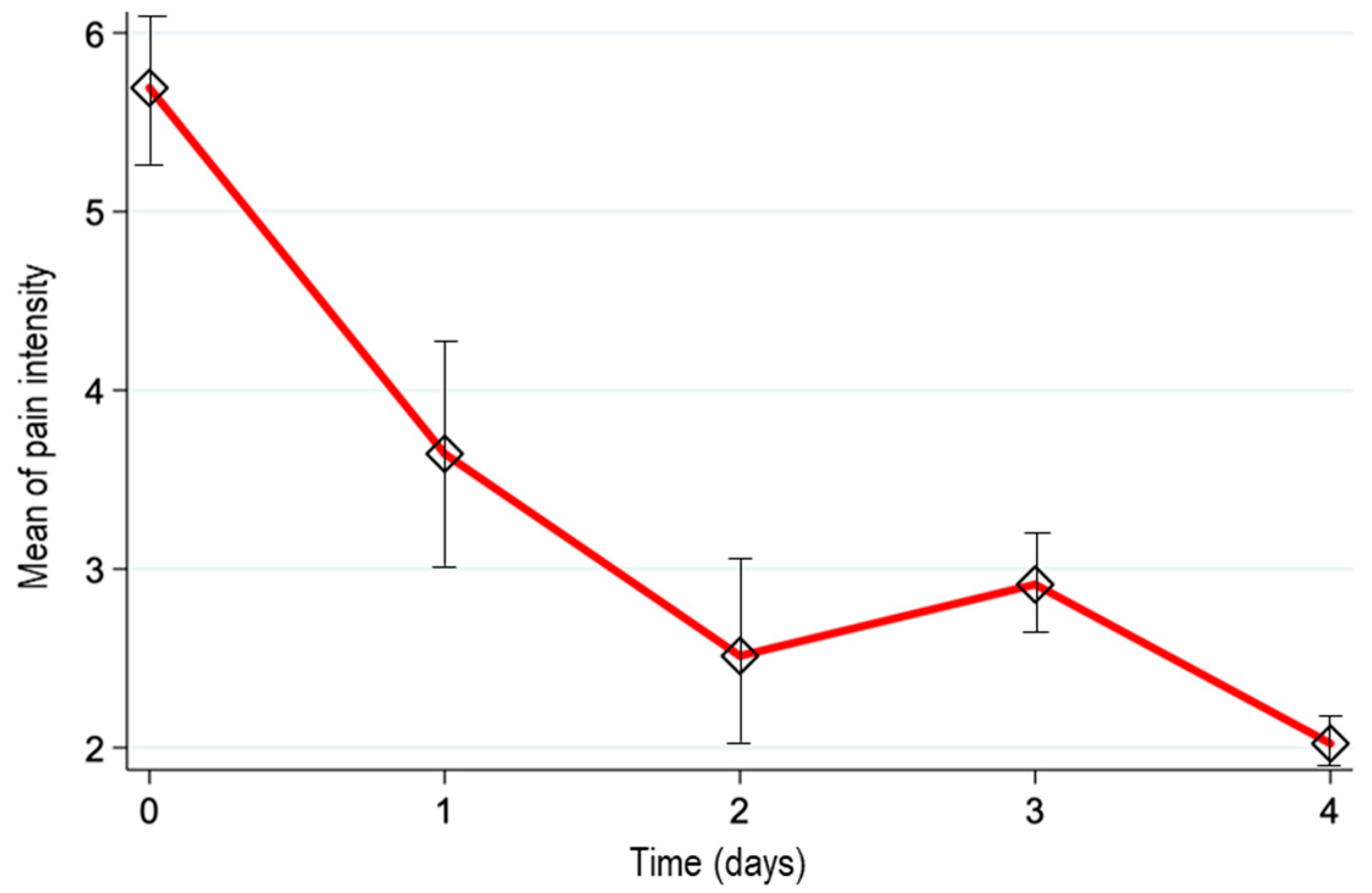
- Pain intensity determined by a numerical rating scale (NRS) [12], where 0 = no pain at all, 1–3 = mild, 4–6 = moderate, and 7–10 = severe.
- (b)
- The proportion of patients with a baseline pain score reduction of at least 50%.
- (c)
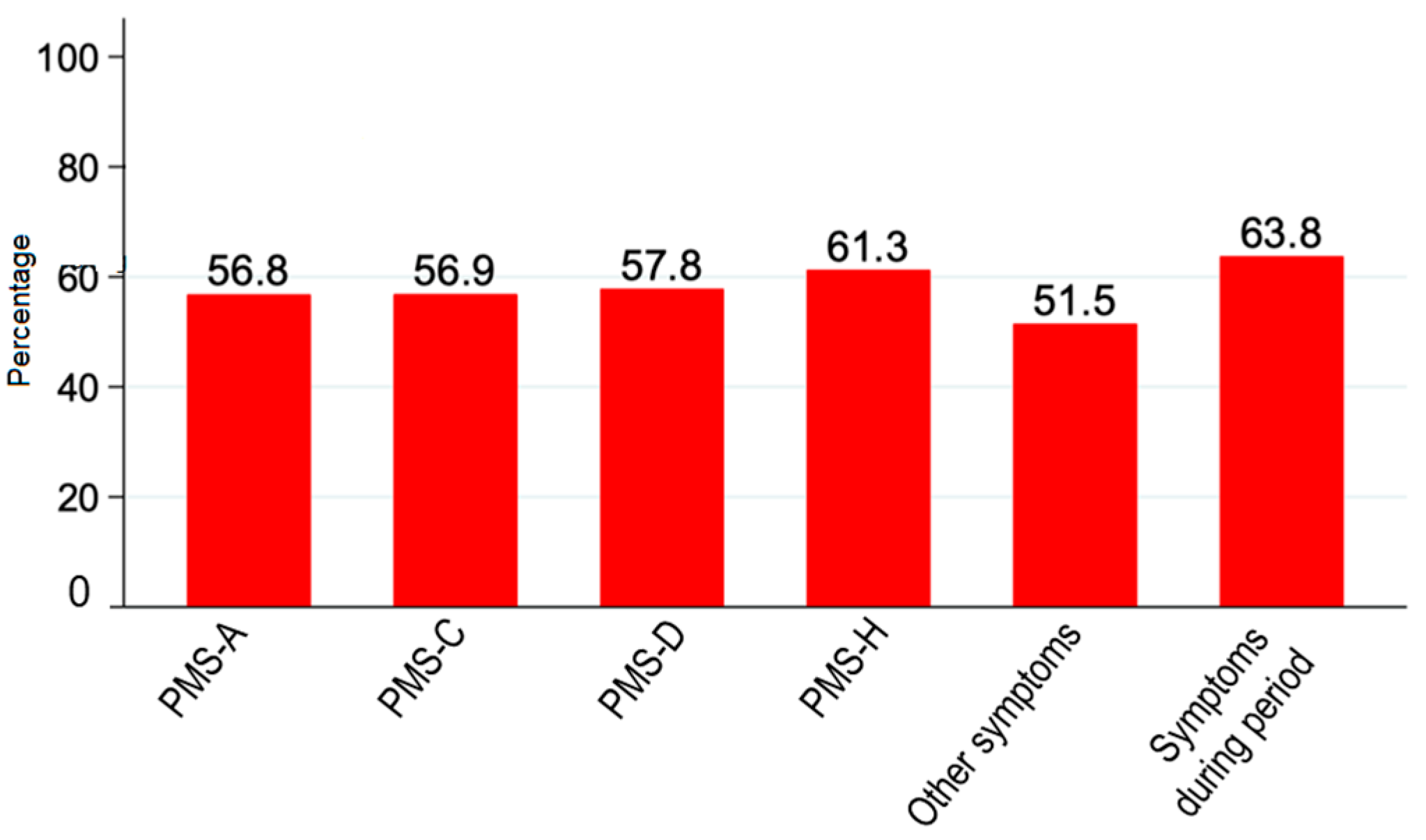
- The premenstrual questionnaire (PMSQ) as applied to determine the presence of the following symptoms: PMS-A (anxiety, irritability, and nervous tension); PMS-C (headaches, increased appetite, desire for sweets, fatigue, palpitations, and tremors); PMS-D (depression, insomnia, tearfulness, forgetfulness, and confusion); PMS-H (water retention, swelling, breast tenderness, bloating, and weight gain). Patients were asked to evaluate their symptoms as follows (Barboza et al., 2014): 0 = symptom was absent; 1 = symptom was barely noticeable; 2 = symptom inhibited activities; 3 = symptom altered my lifestyle.
4.5. Statistical Analyses
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gnanasambanthan, S.; Datta, S. Premenstrual syndrome. Obstet. Gynaecol. Reprod. Med. 2019, 29, 281–285. [Google Scholar] [CrossRef]
- Yonkers, K.A.; Simoni, M.K. Premenstrual disorders. Am. J. Obstet. Gynecol. 2018, 218, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Armour, M.; Parry, K.; Manohar, N.; Holmes, J.; Ferfolja, T.; Curry, C.; Macmillan, F.; Smith, C.A. The prevalence and academic impact of dysmenorrhea in 21,573 young women: A systematic review and meta-analysis. J. Women’s Health 2019, 28, 1161–1171. [Google Scholar] [CrossRef]
- Gao, M.; Zhang, H.; Gao, Z.; Cheng, X.; Sun, Y.; Qiao, M.; Gao, D. Global and regional prevalence and burden for premenstrual syndrome and premenstrual dysphoric disorder: A study protocol for systematic review and meta-analysis. Medicine 2022, 7, e28528. [Google Scholar] [CrossRef] [PubMed]
- Ortiz, M.I. Primary dysmenorrhea among Mexican university students: Prevalence, impact and treatment. Eur. J. Obstet. Gynecol. Reprod. Biol. 2010, 152, 73–77. [Google Scholar] [CrossRef]
- Sima, R.M.; Sulea, M.; Radosa, J.C.; Findeklee, S.; Hamoud, B.H.; Popescu, M.; Gorecki, G.P.; Bobircă, A.; Bobirca, F.; Cirstoveanu, C.; et al. The Prevalence, Management and Impact of Dysmenorrhea on Medical Students’ Lives-A Multicenter Study. Healthcare 2022, 14, 157. [Google Scholar] [CrossRef]
- Dickerson, L.M.; Mazyck, P.J.; Hunter, M.H. Premenstrual syndrome. Am. Fam. Phys. 2003, 67, 1743–1752. [Google Scholar]
- Hofmeister, S.; Bodden, S. Premenstrual syndrome and premenstrual dysphoric disorder. Am. Fam. Phys. 2016, 94, 236–240. [Google Scholar]
- Green Top Guideline. Management of premenstrual syndrome: Green-top Guideline No. 48. BJOG Int. J. Obstet. Gynaecol. 2017, 124, 73–105. [Google Scholar]
- Janczura, M.; Kobus, M.; Sip, S.; Zarowski, M.; Warenczak, A.; Cielecka-Piontek, J. Fixed-dose combination of NSAIDs and spasmolytic agents in the treatment of different types of pain—A practical review. J. Clin. Med. 2021, 10, 3118. [Google Scholar] [CrossRef]
- Ortiz, M.I.; Murguía-Cánovas, G.; Vargas-López, L.C.; Silva, R.; González-de la Parra, M. Naproxen, paracetamol and pamabrom versus paracetamol, pyrilamine and pamabrom in primary dysmenorrhea: A randomized, double-blind clinical trial. Medwave 2016, 16, e6587. [Google Scholar] [CrossRef] [PubMed]
- Haefeli, M.; Elfering, A. Pain assessment. Eur Spine J. 2006, 15, S17–S24. [Google Scholar] [CrossRef] [PubMed]
- Barcikowska, Z.; Rajkowska-Labon, E.; Grzybowska, M.E.; Hansdorfer-Korzon, R.; Zorena, K. Inflammatory markers in dysmenorrhea and therapeutic options. Int. J. Environ. Res. Public Health 2020, 17, 1191. [Google Scholar] [CrossRef] [PubMed]
- Tacani, P.M.; de Oliveira Ribeiro, D.; Guimarães, B.E.B.; Perez-Machado, A.F.; Tacani, R.E. Characterization of symptoms and edema distribution in premenstrual syndrome. Int. J. Women’s Health 2015, 7, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Jarvis, C.I.; Lynch, A.M.; Morin, A.K. Management strategies for premenstrual syndrome/premenstrual dysphoric disorder. Ann. Pharmacother. 2008, 42, 967–978. [Google Scholar] [CrossRef] [PubMed]
- Moore, N.; Pollack, C.; Butkerait, P. Adverse drug reactions and drug–drug interactions with over-the-counter NSAIDs. Ther. Clin. Risk Manag. 2015, 11, 1061–1075. [Google Scholar] [PubMed]
- Marjoribanks, J.; Ayeleke, R.O.; Farquhar, C.; Proctor, M. Nonsteroidal anti-inflammatory drugs for dysmenorrhoea. Cochrane Database Syst. Rev. 2015, 2015, CD001751. [Google Scholar] [CrossRef]
- Ali, Z.; Burnett, I.; Eccles, R.; North, M.; Jawad, M.; Jawad, S.; Clarke, G.; Milsom, I. Efficacy of a paracetamol and caffeine combination in the treatment of the key symptoms of primary dysmenorrhoea. Curr. Med. Res. Opin. 2007, 23, 841–851. [Google Scholar] [CrossRef]
- Nie, W.; Xu, P.; Hao, C.; Yingying, C.; Yanling, Y.; Lisheng, W. Efficacy and safety of over-the-counter analgesics for primary dysmenorrhea. J. Med. 2020, 99, e19881. [Google Scholar] [CrossRef]
- Angiolillo, D.J.; Weisman, S.M. Clinical pharmacology and cardiovascular safety of naproxen. Am. J. Cardiovasc. Drugs 2017, 17, 97–107. [Google Scholar] [CrossRef]
- Anderson, B.J. Paracetamol (Acetaminophen): Mechanisms of action. Paediatr. Anaesth. 2008, 18, 915–921. [Google Scholar] [CrossRef] [PubMed]
- Eccles, R.; Holbrook, A.; Jawad, M. A double-blind, randomised, crossover study of two doses of a single-tablet combination of ibuprofen/paracetamol and placebo for primary dysmenorrhoea. Curr. Med. Res. Opin. 2020, 26, 2689–2699. [Google Scholar] [CrossRef] [PubMed]
- Ong, C.K.S.; Seymour, R.A.; Lirk, P.; Merry, A.F. Combining paracetamol (acetaminophen) with nonsteroidal antiinflammatory drugs: A qualitative systematic review of analgesic efficacy for acute postoperative pain. Anesth. Anal. 2010, 110, 1170–1179. [Google Scholar] [CrossRef] [PubMed]
- Landazuri, I.G.; Rivera, V.; González, Y.; Campoverde, J.; Contreras, S.; Roque, R.; Córdova, C. Dexketoprofen plus pamabrom versus acetaminophen in primary dysmenorrhea: A controlled, randomized, double-blind, multicenter study. Rev. Med. Electrón. 2020, 42, 1–20. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Study Population (n = 270) | |
|---|---|
| Age, years (mean ± S.D.) | 28.9 ± 8.8 |
| BMI, kg/m2 (mean ± S.D.) | 28.1 ± 1.4 |
| Students (n, %) | 93, 34.4 |
| Workers (n, %) | 148, 54.8 |
| Presence of comorbidities (n, %) | 12, 4.4 |
| Diabetes (type 2) | 1 |
| Allergic rhinitis | 2 |
| Epilepsy | 1 |
| Atopic dermatitis | 1 |
| Anemia | 1 |
| Obesity | 4 |
| Asthma | 1 |
| Polycystic ovarian syndrome | 1 |
| Daily activities limitation (n, %) | 170, 63.0 |
| School or work absence | 51.50% |
| Daily activities limitation | 60.00% |
| Hospitalization | 2.20% |
| Adverse Event by SOC and PT | n (%) | Severity | Treatment Related |
|---|---|---|---|
| Gastrointestinal disorders | |||
| Dyspepsia | 1 (0.4) | Moderate | Yes |
| Gastritis | 2 (0.7) | Mild (1) Moderate (1) | Yes Yes |
| Nausea | 1 (0.4) | Mild | Yes |
| Diarrhea | 1 (0.4) | Moderate | No |
| Nervous system disorders | |||
| Headache | 5 (1.9) | Mild (4) Moderate (1) | Yes (2) No (3) |
| Dimension of the PMS Questionnaire | Time (Days) | Mean ± SD | N |
|---|---|---|---|
| PMS-A | 0 | 6.3 ± 3.1 | 269 |
| 1 | 4.3 ± 3.4 | 269 | |
| 2 | 3.8 ± 2.5 | 140 | |
| 3 | 3.5 ± 2.5 | 60 | |
| 4 | 3.2 ± 1.8 | 37 | |
| PMS-C | 0 | 5.5 ± 3.4 | 269 |
| 1 | 3.8 ± 3.4 | 269 | |
| 2 | 3.8 ± 2.9 | 120 | |
| 3 | 3.3 ± 3.0 | 64 | |
| 4 | 3.2 ± 2.4 | 44 | |
| PMS-D | 0 | 4.7 ± 3.9 | 270 |
| 1 | 3.2 ± 3.8 | 269 | |
| 2 | 4.3 ± 3.0 | 91 | |
| 3 | 4.0 ± 2.4 | 38 | |
| 4 | 4.0 ± 2.0 | 26 | |
| PMS-H | 0 | 8.2 ± 4.2 | 270 |
| 1 | 5.3 ± 4.6 | 269 | |
| 2 | 4.9 ± 3.6 | 128 | |
| 3 | 4.3 ± 3.2 | 65 | |
| 4 | 4.1 ± 2.4 | 40 | |
| PMS—other symptoms | 0 | 5.5 ± 4.0 | 269 |
| 1 | 3.6 ± 3.9 | 269 | |
| 2 | 5.0 ± 3.5 | 97 | |
| 3 | 4.2 ± 3.4 | 47 | |
| 4 | 4.7 ± 3.2 | 33 | |
| PMS—symptoms during study period | 0 | 3.8 ± 2.4 | 270 |
| 1 | 2.6 ± 2.1 | 269 | |
| 2 | 2.5 ± 1.5 | 106 | |
| 3 | 2.2 ± 1.1 | 53 | |
| 4 | 1.6 ± 1.4 | 40 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peña-Jiménez, Á.E.; Benitez-Aguilar, O.; Villegas, J.E.; González-de la-Parra, M.; Delgado-Roche, L. Safety and Effectiveness of Naproxen 220 mg + Paracetamol 300 mg + Pamabrom 25 mg Fixed Dose Combination in Women with Premenstrual Syndrome: A Post-Marketing, Open-Label, Uncontrolled, Prospective, Multicenter, Observational Study. Women 2024, 4, 13-21. https://0-doi-org.brum.beds.ac.uk/10.3390/women4010002
Peña-Jiménez ÁE, Benitez-Aguilar O, Villegas JE, González-de la-Parra M, Delgado-Roche L. Safety and Effectiveness of Naproxen 220 mg + Paracetamol 300 mg + Pamabrom 25 mg Fixed Dose Combination in Women with Premenstrual Syndrome: A Post-Marketing, Open-Label, Uncontrolled, Prospective, Multicenter, Observational Study. Women. 2024; 4(1):13-21. https://0-doi-org.brum.beds.ac.uk/10.3390/women4010002
Chicago/Turabian StylePeña-Jiménez, Álvaro E., Omar Benitez-Aguilar, Jesús E. Villegas, Mario González-de la-Parra, and Livan Delgado-Roche. 2024. "Safety and Effectiveness of Naproxen 220 mg + Paracetamol 300 mg + Pamabrom 25 mg Fixed Dose Combination in Women with Premenstrual Syndrome: A Post-Marketing, Open-Label, Uncontrolled, Prospective, Multicenter, Observational Study" Women 4, no. 1: 13-21. https://0-doi-org.brum.beds.ac.uk/10.3390/women4010002