
Beneficial Effects of the Ketogenic Diet in Metabolic Syndrome: A Systematic Review



1
Centre de Recherche de Biomédecine de Strasbourg, UR 3072 Mitochondrie, Stress Oxydant et Protection Musculaire, Université de Strasbourg, 67000 Strasbourg, France
2
Service de Physiologie et d’Explorations Fonctionnelles Respiratoires, Hôpitaux Universitaires de Strasbourg, 67000 Strasbourg, France
*
Author to whom correspondence should be addressed.
Diabetology 2022, 3(2), 292-309; https://0-doi-org.brum.beds.ac.uk/10.3390/diabetology3020020
Submission received: 15 March 2022
/
Revised: 13 April 2022
/
Accepted: 14 April 2022
/
Published: 24 April 2022
Abstract
:Metabolic syndrome (MetS) is a major societal concern due to its increasing prevalence and its high risk of cardiovascular complications. The ketogenic diet (KD), a high fat, low carbohydrate, and non-caloric restrictive diet, is a new popular weight loss intervention but its beneficial effects are controversial. This study aims to gather all of the relevant studies using KD for metabolic disease treatment to determine its beneficial effects and evaluate its safety and efficacy for patients. Following the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses, we included 20 articles in the final review. Overall, most of the studies showed a significant effect of KD on weight loss (17/19 articles), BMI (7/7), glucose levels (9/13), insulin levels (7/9), HOMA-IR (4/5), HbA1c (7/7), total cholesterol (6/9), TG (13/15), AST (3/4), and ALT (3/5), and no major side effects. The results heterogeneity seems to be explained by a difference of diet composition and duration. In conclusion, KD is a safety diet which seems to be a promising approach for obesity and MetS treatment, even if the optimal carbohydrate proportion and diet duration must be explored to enhance the beneficial effects of KD.
1. Introduction
1.1. From Obesity to Metabolic Syndrome: Epidemiology and Physiopathology
Obesity is defined by the World Health Organization as “an abnormal or excessive fat accumulation that may impair health” [1]. Its development is intensified by the modern diet, also call Western Diet (WD), rich in carbohydrates, saturated fats, and additive food contents as added sugars, salt, or preservative agents [2]. The consumption of WD induces hyperglycemia and insulin secretion that promote the storage of excess substrates as fat accumulation in adipose tissue [3]. Chronic nutrient overload leads to adipocyte hypertrophy in the subcutaneous and visceral areas, leading to overweight development, then obesity [4]. When the adipose tissues reach their storage limit, lipids accumulate in extra-adipose tissues as skeletal muscles and liver [5]. In the liver, this ectopic lipid accumulation leads to non-alcoholic fatty liver disease (NAFLD) development. NAFLD is the most common liver disease and can progress to nonalcoholic steatohepatitis and cirrhosis [6]. The excessive expansion of visceral adipose tissue also alters endocrine functions. It secretes large amounts of hormones as leptin or adiponectin, proinflammatory cytokines as secretion of tumor necrosis factor-α (TNFα), interleukin-1 (IL-1) and interleukin-6 (IL-6), and releases free fatty acids (FFAs) which are altogether involved in obesity complications [7,8].
FFAs and proinflammatory cytokines activate enzymes of the protein kinase C (PKC) family. PKC can phosphorylate the insulin receptor substrates (IRS), a cytoplasmic protein involved in the insulin signaling pathway. Phosphorylation inactivates the IRS, leading to intracellular signaling chain reduction, attenuation of insulin effects on its targets, and ultimately to insulin resistance [9,10]. In addition to type 2 diabetes, cytokines alterations in signaling pathway impair the immune system, promote NAFLD pathogenesis, liver fibrosis, and increase cardiovascular risk (CVD) [11,12].
Natriuretic peptides, which are released from the heart, seem to play a role in obesity complications. Patients with obesity are associated with a decrease of natriuretic peptides secretion and activity [13,14]. Low levels of natriuretic peptides may lead to reduced lipolysis, fat oxidation, and excessive weight gain in obese patients, which may be one of the biological alterations that contribute to the development of obesity [15]. Lower natriuretic peptide levels were also associated with the development of insulin resistance (HOMA-IR), MetS, and hypertension [16,17,18].
Obesity is also associated with an increase in plasma triglycerides (TG) and low-density lipoprotein (LDL), and a decrease in high-density lipoprotein (HDL). These changes lead to dyslipidemia, a major risk factor of cardiovascular disease [19]. LDL and proinflammatory mediators are causal agents of atherogenesis and plaque vulnerability in atherosclerosis [20]. This pathology is characterized by a deposit of a plaque mostly composed of lipid as LDL particles, immune cells and endothelial cells [21]. The plaque rupture can lead to myocardial infarction and stroke [22]. The association of obesity and its complications as hypertension, insulin resistance or type 2 diabetes and dyslipidemia leads to the development of Metabolic syndrome (MetS) [23]. MetS is associated with an increased cardiovascular risk and type 2 diabetes [24]. Due to its important health issues, MetS had become, in the past few years, a major societal concern. Facts about obesity and MetS are alarming since nearly 40% of the current world’s adult population is overweight and 13% is obese. The worldwide obesity prevalence almost tripled between 1975 and 2016 and is still always increasing [1]. In France, the obesity prevalence among adults was 17% and in the United States, it was 42.4% in 2018, while 30% of American had a MetS in 2016 [25,26]. MetS has become an epidemic of major proportions around the world mainly due to lifestyle changes including physical inactivity and food habits [27,28,29]. Faced with the worsening of the MetS pandemic, it appears essential to find new therapeutic strategies, since, thus far, there is no miracle cure to treat obesity.
1.2. Lifestyle Recommendations for the Prevention and Management of Metabolic Syndrome
Weight loss through an energy-restricted diet together with an increase in energy spent through physical activity contribute to the prevention and treatment of MetS. A Mediterranean-type diet, with or without energy restriction, is an effective treatment component [30]. This dietary pattern should be built upon an increased intake of unsaturated fat, primarily from olive oil, and emphasize the consumption of legumes, cereals (whole grains), fruits, vegetables, nuts, fish, and low-fat dairy products, as well as moderate consumption of alcohol [31]. Other dietary patterns (dietary approaches to stop hypertension, new Nordic, and vegetarian diets) have also been proposed as alternatives for preventing obesity development [32]. Reducing intake of sugar-sweetened beverages and meat products are mandatory. Nevertheless, there are inconsistencies and gaps in the evidence, and additional research is needed to define the most appropriate therapies for MetS [33]. In conclusion, a healthy lifestyle is critical to prevent or delay the onset of MetS development in susceptible individuals and to prevent weight gain, cardiovascular disease and type 2 diabetes that occurs during MetS. Several recommendations should help patients and clinicians understand and implement the most effective approaches for lifestyle changes to prevent MetS and improve cardiometabolic health [34]. There are therefore many diets that can help reduce the appearance or the negative development of symptoms. The ketogenic diet (KD) is one of these promising diets and there is currently a large body of evidence that demonstrates the benefits of this approach to reduce or prevent symptoms of obesity and its comorbidities.
1.3. Ketogenic Diet: Definition, History and Principle
The KD, developed in the 1920s by Dr. Russell Wilder, is a diet which induces a nutritional ketosis [35]. The aim of this diet is to increase the fat proportion and restrain the carbohydrate proportions (around 5 or 10% of daily caloric supply) in order to imitate the metabolic effects of starvation, but in a lasting way [36]. This extreme changing in nutrient distribution leads to metabolic changes. The body, which is used to obtain energy mainly from carbohydrate metabolism, respond to glucose restriction by fatty acid oxidation and ketosis [37]. Glucose dependent organs, as brain, are not able to use lipids as energy. Fatty acids, coming from feeding, cross the blood brain barrier with difficulty, and the brain mitochondria have a low enzymatic capacity for fatty acid degradation [38]. To provide enough energy to the brain, a survival way is activated. Fatty acids are broken down into acetyl coenzyme A (acetyl-CoA) by hepatic mitochondria, leading to high level of acetyl-CoA. If a part of these molecules enters the tricarboxylic cycle (TCA) for ATP generation, the rest is used to synthetize compounds called ketone bodies [39]. Ketogenesis leads to the synthesis of three ketones bodies: acetoacetate (AcAc), 3-hydroxybutyrate (3HB), and acetone. AcAc are the central ketone bodies, and the two others are derived from it. Spontaneous decarboxylation of AcAc leads to the Acetone production, but this ketone body is evacuated by the lungs. The reduction of AcAc produces 3HB, which is more chemically stable than AcAc [40]. AcAc and 3HB can cross the blood brain barrier via monocarboxylate transporter, and then are used as fuel by the cerebral cells. In the brain mitochondria, they are once again transformed in acetyl-CoA which will enter in the TCA to produce ATP [41,42].
In the literature, different types of nutritional ketosis are described and commonly accepted. The high fat KD, also called KD, refers to the KD designed by Dr Wilder. KD is characterized by an ad libitum caloric intake diet, with a carbohydrate restriction between 20 and 50 g per day, an adequate or increase protein intake and an unrestricted intake of fat [35]. The very low calorie KD (VLCKD) is a KD with a carbohydrate restriction between 20 and 50 g per day is associated with an extreme caloric restriction (400–800 kcal/day) [43]. Other low-calorie diets are often classified as ketogenic diets, but these approaches have more to do with eating behavior than dietary concept since they do not necessary induce ketosis. Indeed, a caloric restriction which is not followed by an appropriate carbohydrate intake reduction is not enough to induce ketosis, that occurs when the intake of carbohydrate is equal or less than 50 g/day [44]. Finally, it is important to notice that KD is often qualified as a low carbohydrate (low carb) diet. Low carb diet is defined by a carbohydrate restriction of less than 130 g/day [45], so KD can be defined as a low carb diet, but all the low carb diets do not induce nutritional ketosis.
Initially, KD was used in the treatment of refractory epilepsy, but they became widely popular, and more and more authors are now interested by KD beneficial effects in obesity treatment [46,47]. Therefore, the aim of this study is to gather all the relevant studies using KD for metabolic disease treatment to determine its effects according to general recommendations of obesity management and evaluate its safety and efficacy for patients. As high fat KD is the most widespread KD type, this review will only focus on it.
2. Methods
A systematic review of the literature was performed, following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [48].
2.1. Eligibility Criteria
Clear inclusion and exclusion criteria were used to determinate the eligibility of studies. Studies included were full text English or French original articles, using KD for patients with obesity (BMI > 30). We defined “Ketogenic Diet” as a diet with a maximal carbohydrate intake of 50 g per day (corresponding to 10% of daily caloric supply) and no predetermined limit on the caloric intake amount. We used “Ketogenic Diet” and “Low carb diet” as keywords to avoid missing studies due to the utilization of different terms.
Studies not eligible for inclusion were animal studies, reviews, letters, editorials comments, short reports, book chapters, studies focusing on animals and studies focusing on other diseases. We excluded studies using other diets, caloric restriction or more than 50 g of carbohydrate per day, studies where KD were associated with exercise or studies of normal weight patients. Duplicated were also removed. In the case of studies using the same patient cohorts, we excluded studies that provided no new results, and we did not consider the results already published to avoid duplication.
2.2. Search and Study Selection
We searched in PubMed database with using a search strategy combining two groups of key words as “Ketogenic diet” OR “Low-carb” OR “Low-carb Diet” AND “Obesity” OR “Weight Loss” OR “Overweight” OR “Type 2 diabetes” OR “Metabolic Syndrome” OR “Non-alcoholic Fatty Liver Disease” OR “Nonalcoholic Steatohepatitis” OR “Cardiovascular Disease”. The relevance of studies was evaluated by collecting title and abstracts, between 30 September 2021 and the 30 November 2021. The full text of potentially eligible study was retrieved to apply the inclusion and exclusion criteria.
2.3. Data Extraction
Measures of interest extracted from each study included: study characteristics (primary author, year of publication, duration and nutritional composition of KD), baseline patient’s characteristics (sample size, age, sex, body mass index (BMI)), effect of KD on clinical measures (weight, BMI, systolic and diastolic blood pressure (BP)), results of KD effects on lipid profile (total cholesterol, HDL, LDL and TG), results of KD effects on glycemic profile (fasting glucose, fasting insulin, HOMA-IR, glycated hemoglobin (HbA1c)), results of KD effects on liver profile (liver enzyme levels as aspartate aminotransferase (AST) and alanine aminotransferase (ALT), volume of the left hepatic lobe, liver biopsy).
3. Results
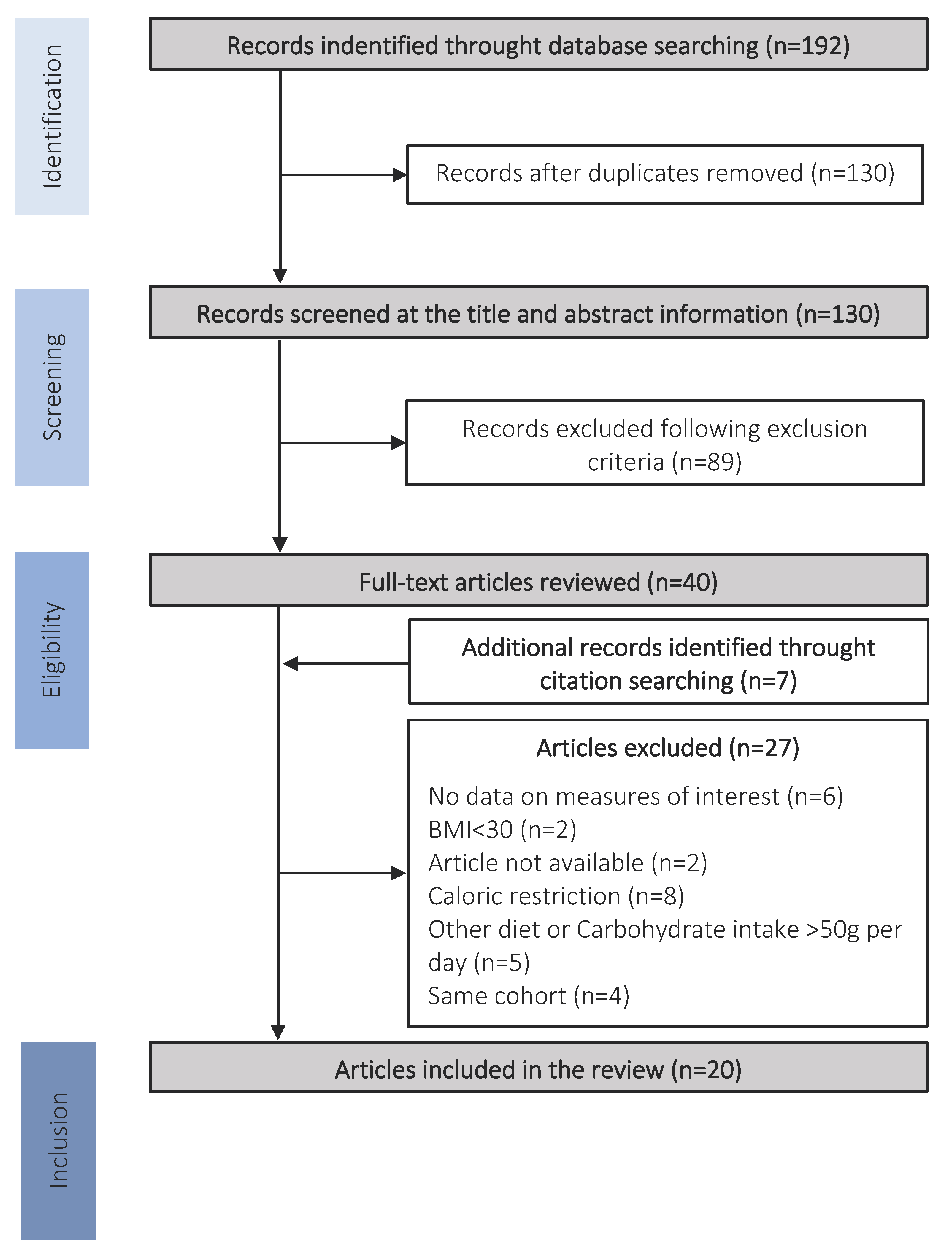
The studies research and identification process are presented in Figure 1.
The database searching from PubMed leads to 192 publications which 130 duplicates were removed. Among the 130 remaining publications, 89 were excluded based on the content of their abstract and titles. 41 articles were full-text reviewed, and additional articles were identified through citation searching and added to the full-text reviewed process.
A total of 25 publications were excluded, due to the following reasons: no data on measures of interest (n = 6), BMI < 30 (n = 1), article not available (n = 2), caloric restriction (n = 8), other diet or carbohydrate intake > 50 g per day (n = 5) and same cohort from another article (n = 4). Finally, the systematic research resulted in 20 studies that met the inclusion criteria [49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68]. Of these, 19 focused on weight loss, 8 on BMI, 8 on systolic and diastolic blood pressure, 14 on fasting glucose levels, 10 on fasting insulin levels, 5 on HOMA-IR, 7 on HbA1c level, 9 on total cholesterol, 15 on HDL and LDL levels, 16 on TG levels, 4 on AST levels, 5 on ALT levels, 1 on left hepatic lobe volume and 1 on liver biopsy histopathological characteristics (Table 1). The characteristics of the study designs are presented in Table 2.
3.1. Effects of KD on Obesity and Cardiovascular Risk
Weight loss is the main recommendation of health-care guidelines to reduce the risk of complication development [69,70] in the context of MetS. Interestingly, the majority of the studies have demonstrated a significant weight loss induced by KD [50,51,52,54,55,56,57,58,59,60,61,62,63,64,65,66,68]. In the eight studies which also investigated the effects of KD on the BMI, the significant weight loss was systematically associated with a significant decrease of the BMI [50,56,58,60,61,63,65]. Among the 19 papers, only 2 showed no significant effect of the KD on weight loss [49,53]. The lack of KD effects on weight loss could be explained by a too short diet duration, which was respectively of six weeks [49] and four days [53].
The cardiovascular risk can be evaluated by several parameters including obesity, high blood pressure, high cholesterol and high TG levels and lifestyle habits as smoking, alcohol consumption or physical inactivity [71]. The actual clinical recommendations support a decrease of blood pressure, LDL and TG levels to improve cardiovascular risk [72]. Eight studies are interested in KD effects on cardiac function, measuring especially systolic and diastolic pressure. Five of them showed a significant decrease in systolic BP [49,58,64,65,68] and four in diastolic BP [49,58,65,68]. Thirteen studies demonstrated that KD is significantly efficient to decrease TG blood levels (Table 3) [49,51,52,54,55,56,58,61,62,63,65,66,68] and only three showed no significant effects [57,59,60]. Concerning LDL and HDL blood levels, the effects of KD are moderated. Almost the half of the studies revealed a significant increase of HDL level [51,52,54,56,65,66,68] and one third showed a significant decrease of LDL levels [51,52,54,56,63] whereas no significant effects of KD were found in the remaining studies [49,51,52,54,55,56,57,58,60,61,62,63,65,66,68]. Finally, a significant decrease of total cholesterol were found in six studies and no significant effects were noticed in three (respectively, [51,52,56,58,63,66] and [57,60,68], Table 3).
The moderate KD effects on lipid parameters could be explained by a too short duration of the diet in several studies. Indeed, most of them had a diet duration of 10 weeks or less [49,55,57,58,59]. To explain the lack of KD effects despite longer diet duration, Partsalaki and al. suggested that KD might not be efficient when the lipidemic profiles are staying within the normal range [60,61,62]. These observations suggest that KD must have a sufficient duration to be effective. Furthermore, lower effects of KD on some parameters could be explained by a non-pathological basal level of the interest markers. It is also important to note that KD diet, are not designed in order to normalize the lipid profile, but to reduce weight and others type 2 diabetes risk factors.
3.2. Effects of KD on Type 2 Diabetes
Type 2 diabetes is associated with high fasting glucose levels (>1.26 mg/dL or 7.0 mmol/L), high HbA1c proportion (>6.5%) and alterations in insulin response [73]. The glycated hemoglobin, the reflect of the past three months mean blood glucose level, is a high-sensitive marker for diabetes diagnosis. A moderate hyperglycemia (between 1 and 1.25 mg/dL or 5.5 mmol/L and 6.8 mmol/L of fasting glucose levels or 6 to 6.4% of HbA1c) is also associated with an increased risk of diabetes development. The management of diabetes mainly consists in reducing hyperglycemia and improve insulin action [74]. Among the 14 studies, 10 showed that KD decrease fasting glucose levels [51,52,53,54,56,57,58,59,63,68], and 4 of them noticed no changes [49,55,60,64]. However, in these four studies patients had normal fasting glucose levels. KD significantly decrease Hb1Ac in all of the studies that measured this parameter [54,56,58,61,62,65,68] except for the study of Tendler and et al. [64]. The four studies that did not found significant effect of KD on fasting glucose did not measure HbA1c levels [49,55,60,67]. A decrease in insulin levels was found in seven studies [49,54,55,57,60,63,68], whereas three studies showed no effects of KD on insulin levels [59,61,64].
The HOMA-IR is a simple index, based on an equation including fasting glucose levels and fasting insulin levels, developed to identify susceptible individuals to diabetes risk [75]. Five studies calculated the HOMA-IR: four out of five showed a significant reduction [49,54,57,60] on it and the last one noticed no effect on KD on it [61]. The amelioration of the HOMA-IR score is benefic for patients since it protects against insulin resistance development. All the results are summarized in Table 3.
3.3. Effects of KD on Nonalcoholic Steatohepatitis
Liver biopsy is the gold standard for non-alcoholic fatty liver disease diagnosis. However, as biopsy is invasive, it must be replaced, whenever it is possible, by noninvasive tests. For example, liver biochemistry or imaging can be performed. Non-alcoholic fatty liver disease is associated with an increase of AST and ALT levels, an accumulation of hepatic lipids, inflammation and fibrosis when steatohepatitis is established [76].
4. Discussion
4.1. Beneficial Effects of the Ketogenic Diet
One of the aims of this systematic review was to determine if KD could be an efficient strategy in obesity management. Overall, most of the studies showed a significant effect of KD on weight loss (17/19 articles), BMI (7/7), glucose levels (9/13), insulin levels (7/9), HOMA-IR (4/5), HbA1c (7/7), total cholesterol (6/9), TG (13/15), AST (3/4), and ALT (3/5) in human.
These beneficial effects are positive in the obesity treatment and agree with the general health-care recommendations. Indeed, guidelines recommend weight loss and glycemic control to reduce type 2 diabetes risk, blood pressure control and low serum lipid level to decrease risk of cardiovascular disease, and maintain of normal liver enzymes level to reduce the risk of steatohepatitis [77]. All of these objectives are essential to reduce the risk of metabolic complication development, as hyperglycemia, dyslipidemia steatohepatitis, and improve health [69,70]. Weight loss is central in obesity management, and, by reducing weight and BMI, KD is beneficial in obesity. Several studies showed that a weight loss, even moderate, is efficient to improve metabolic functions and reduce cardiometabolic diseases risk factors [78,79].
Positive effects of KD are found on the other parameters. The significant reduction in glucose and insulin levels, HOMA-IR and Hb1Ac are beneficial to improve glucose metabolism and the glycemic balance, and so reduce the risk of type 2 diabetes [80]. In diabetic patients, hyperglycemia reduction is associated with improvement of morbidity and mortality [81]. Furthermore, lower glucose and Hb1Ac levels reduces the risk of diabetes-relative complications development, as microvascular and macrovascular disease [82]. Indeed, insulin resistance and hyperglycemia are responsible for cardiovascular damages and endothelial dysfunction, and are involved in the development of cardiovascular complications [83,84]. Fasting glucose levels reduction is positive for diabetic patients since it is associated with a risk reduction in major cardiovascular events [85,86].
Dyslipidemia is also a major risk factor of cardiovascular disease. High Total cholesterol and LDL levels and low HDL levels are associated with atherosclerosis [87,88]. The effects of KD on lipid profile are mixed, and it is difficult to draw an unequivocal conclusion about the positive effects of KD on cardiovascular risk. The majority of studies showed a reduction on TG and total cholesterol levels that is known to lower the risk of vascular events [89,90]. About LDL and HDL levels, only less than one-half of the studies showed changes induced by KD, with a decrease of LDL levels and an increase of HDL levels. These modifications of lipoproteins levels are associated with cardiovascular risk reduction [91]. The reduction of systolic and diastolic blood pressure, associated in cardiovascular risk reduction, was induced by KD in half of the studies [92].
Finally, KD presented beneficial effects on liver in most studies. The decreases of AST and ALT levels showed improvement in liver health since an elevation in the level of these two enzymes is a liver injury indicator, and it is used as a biomarker of NAFLD prediction [93]. KD also seems to induce positive effect on liver anatomy, by a reduction of the left lobe volume, and a reduction of the histological markers of NASH, but only one study for each of these parameters had an anatomic and histological approach [63,64]. More studies focusing on liver enzyme levels, anatomy and histology will be necessary to conclude about the effects of KD on steatohepatitis.
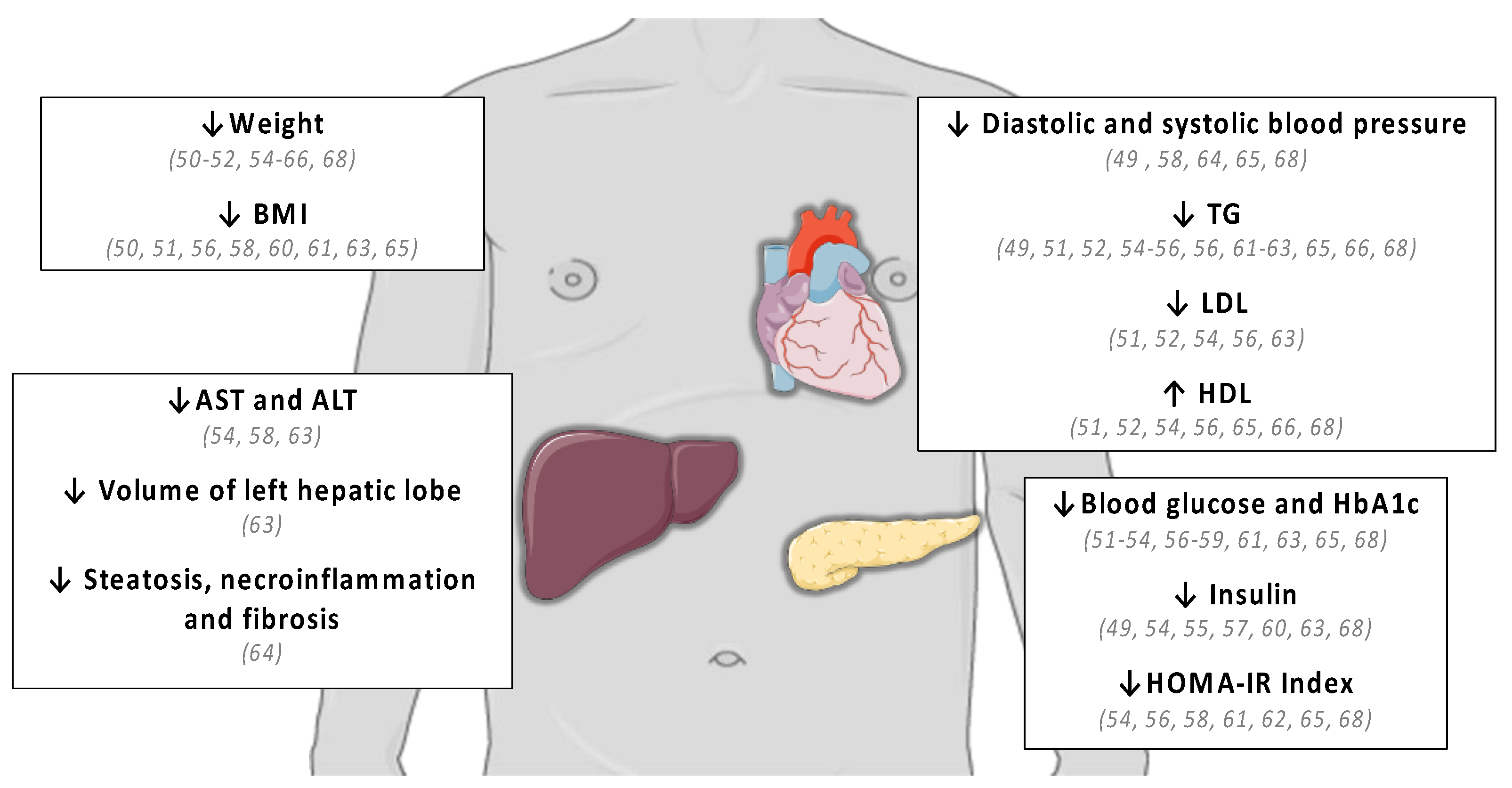
Thereby, KD seems to be efficient in obesity management by inducing weight loss, improving glucose metabolism, reducing cardiovascular disease risk factors and steatohepatitis. Even if KD was not effective in the same way for all parameters of interest, all studies found a beneficial effect on, at least, one of them (Figure 2).
4.2. Recommendations and Limitations of KD
The heterogeneity of the results can be explained by the difference within protocol design. First, the duration of the diet differs, and the length of the KD intake on all of the included studies range from 4 days [53,59] to 56 weeks [51,52]. The effective of patients are also different from each study and vary from 5 patients [64] to 261 [56]. Moreover, the duration of KD intake seems to be a major success criterion. All of the studies with mixed results on interest parameter was short-term KD (six month or less) whereas the most efficient protocols had a duration between 6 and 12 months. These observations suggest that KD should be perform at least for six months to present beneficial effect for the patients.
An important bias that also could explain the result difference is the diet itself. KD is defined by a carbohydrate restriction and an increase in lipid supply, and we limited the inclusion of studies with a carbohydrate restriction of <50 g per day, which is equivalent to 10% of the daily caloric supply [94]. Despite being all ketogenic, the diets were not based on consensus. The most restrictive study in terms of carbohydrates was the study of Johnstone et al. with a maximum consumption of 5.5 g per day [57], the majority of the studies allowed a maximal carbohydrate intake between 20 and 30 g and the least restrictive permit a maximum of 50 g per day [49,50,51,52,53,54,55,56,58,59,60,61,62,64,65,66,67,68]. The use of KD is mainly widespread in the treatment of refractory epilepsies since the early 20th century. Therefore, the studies carried out in this branch can be useful to understand the impact of the amount of restriction in carbohydrates on the effectiveness of KD. In the case of intractable epilepsy, KD shows greater antiepileptic efficiency when the carbohydrate intake is more restrictive [95]. Based on animal studies, the authors suggest that the correlation between a restrictive KD and protection from epileptic seizure seems to be the result of higher ketosis. The comparison of a classic KD (CKD, 4% of carbohydrate daily caloric supply) and modified Atkins diet (MAD, 10% of carbohydrate daily caloric supply) also demonstrated that the antiseizure effect was better with CKD than MAD [96,97].
In this review, we observed that studies with the higher carbohydrate amount all seem to be less effective [49,53,59,61,62] whereas the most effective studies had a carbohydrate restriction between 20–30 g per day [51,52,54,56] with a minimal duration of 10 weeks, suggesting that a restriction with a maximum of 20 to 30 g of carbohydrate intake each day is sufficient, but necessary. These observations are in line with the studies carried out in the field of refractory epilepsy and reinforce the importance to implement a sufficient carbohydrate restriction in order to obtain KD positive effects.
In obesity, the greater KD efficiency when the carbohydrate intake is low could also be explain by a better ketosis effect. A high carbohydrate restriction induces a decrease of insulin secretion, favor fat oxidation and so ketone bodies production. Ketone bodies present interesting properties, since they seem to decrease appetite and increase satiety [98]. The effect of ketone bodies also seems to be link with the activation of the AMP-dependent kinase (AMPK), since the increase of ketone body levels, particularly 3HB, lead to AMPK activation [99]. AMPK is an enzyme that plays a role of energy sensor and when it is activated, it is implicated in insulin pathway regulation and the increase of fatty acid oxidation [100,101]. Once again, these observations came from animal studies, and must be confirm in human.
One of the most challenge of KD is the compliance of the diet, which refers to the capacity to adhere to the diet and respect the carbohydrate restriction without breaking it. The restrictive nature of KD creates challenges to diet compliance related to psychosocial variables. A strict dietary restriction could interfere with social and family life, ask more food preparation time and be too restrictive and so, could be hard to follow [102]. KD can also cause some side effects. The most common being fatigue, headache, gastrointestinal pain, vomiting, nausea, and diarrhea. These frequent but minor symptoms, also called “keto flu”, appear at the early stages of the diet and generally disappear after few days [103]. A long-term KD, where the duration is longer than a year, can be associated with severe side effects, as kidney stones, acidosis or vitamin and mineral deficiencies. These adverse effects are occasional and have been mostly observed in epileptic patients, where the KD is pursued for a year or more. They can be avoided with a regular monitoring of the patients and nutritional supplements.
In the included studies of this review, only eight reported incidences of adverse reaction link to KD. Side effects was minor including constipation, headache, muscle cramps, halitosis, rash, diarrhea, and no serious adverse effects was reported, showing the safe profile of KD [50,51,52,54,58,63,66,68]. However, more studies are needed in order to determine an optimal protocol in terms of duration and carbohydrate restriction to reach the better risk and benefit ratio profile of KD.
We can notice the lack of information about major systemic parameters which seem to play a role in obesity. Indeed, the studies presented in this review did not measure inflammatory cytokines or cardiac natriuretic peptides while these parameters can easily be dosed in blood. It could be relevant for future studies to measure not only the classic medical measures (as described in this review as clinical measures, glycemic, lipid and liver profiles) but also patients’ compliance to the diet, as well as its effects on inflammation and natriuretic peptide levels. Moreover, molecular, and cellular pathway that are involved in KD beneficial effects remain unclear. If some clues on KD mechanism were provided in animal studies, there is currently no study allowing to describe the molecular pathway involved in the beneficial effects of KD in patients with Mets.
5. Conclusions
KD is a safety diet which seems to be a promising approach to reduce the risk of obesity and its complications as well as the MetS. The consumption of a KD improves weight loss, glucose metabolism, dyslipidemia, and steatohepatitis. However, more studies should be performed to assess if the KD could be used as a routine treatment in metabolic disease. Indeed, the effectiveness of KD seems directly link to the duration of the diet and above all the degree of carbohydrate restriction. One hand, KD efficiency is better with a high carbohydrate restriction and a duration of six months to one year. On the other hand, patients had a better tolerance and compliance to the diet when the carbohydrate intake is higher, and a long-term KD could be associated with side effects [95,104]. The restriction in sugar must be sufficient without being too restrictive otherwise it could reduce its adhesion. According to the data extracted in this review and the studies with the better KD effects, we could hypothesize that the optimal KD protocol could aim a carbohydrate restriction of 20 to 30 g and a duration of at least six months, with a regular medical monitoring to be sure of the patient compliance to the diet. We can also imagine beginning a KD with a high carbohydrate restriction (20 to 30 g) for six months, and then be more permissive (carbohydrate intake of 50 g). It could help to keep a good long-term compliance to the diet, while remaining enough efficient. Furthers investigations should be conducted to determine the optimal duration for the diet, the better carbohydrate proportion to have the higher beneficial effects of ketosis with a good tolerance and compliance. They should also consider starting a highly carbohydrate-restrictive KD, which may become more flexible once the beneficial effects are established.
Author Contributions
A.C. conducted the review and wrote the manuscript. J.Z. assisted in manuscript writing and supervised the whole project. All authors have read and agreed to the published version of the manuscript.
Funding
Research of the J.Z. team is supported in part by funding from the STEPAN Company and the University of Strasbourg.
Acknowledgments
We are grateful to Maude Bouchard Marmen for her precious assistance in language editing.
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organisation. Obesity and Overweight. Available online: http://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 26 November 2018).
- Odermatt, A. The Western-style diet: A major risk factor for impaired kidney function and chronic kidney disease. Am. J. Physiol. Physiol. 2011, 301, F919–F931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foufelle, F.; Ferré, P. Mechanism of Storage and Synthesis of Fatty Acids and Triglycerides in White Adipocytes. In Physiology and Physiopathology of Adipose Tissue; Bastard, J.-P., Fève, B., Eds.; Springer: Paris, France, 2013; pp. 101–121. ISBN 978-2-8178-0342-5. [Google Scholar]
- Deng, T.; Lyon, C.J.; Bergin, S.; Caligiuri, M.A.; Hsueh, W.A. Obesity, Inflammation, and Cancer. Annu. Rev. Pathol. Mech. Dis. 2016, 11, 421–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polyzos, S.A.; Kountouras, J.; Mantzoros, C.S. Adipose Tissue, Obesity and Non-Alcoholic Fatty Liver Disease. Minerva Endocrinol. 2017, 42, 92–108. [Google Scholar] [CrossRef] [PubMed]
- Milić, S.; Lulić, D.; Štimac, D. Non-alcoholic fatty liver disease and obesity: Biochemical, metabolic and clinical presentations. World J. Gastroenterol. 2014, 20, 9330–9337. [Google Scholar] [CrossRef] [PubMed]
- Abdul-Ghani, M.A.; Muller, F.L.; Liu, Y.; Chavez, A.O.; Balas, B.; Zuo, P.; Chang, Z.; Tripathy, D.; Jani, R.; Molina-Carrion, M.; et al. Deleterious action of FA metabolites on ATP synthesis: Possible link between lipotoxicity, mitochondrial dysfunction, and insulin resistance. Am. J. Physiol. Metab. 2008, 295, E678–E685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Algoblan, A.; Alalfi, M.; Khan, M. Mechanism linking diabetes mellitus and obesity. Diabetes, Metab. Syndr. Obesity: Targets Ther. 2014, 7, 587–591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Luca, C.; Olefsky, J.M. Inflammation and insulin resistance. FEBS Lett. 2008, 582, 97–105. [Google Scholar] [CrossRef] [Green Version]
- Ferré, P. Signalisation insulinique et résistance à l’insuline. Therapies 2007, 62, 277–284. [Google Scholar] [CrossRef]
- Karczewski, J.; Śledzińska, E.; Baturo, A.; Jończyk, I.; Maleszko, A.; Samborski, P.; Begier-Krasińska, B.; Dobrowolska, A. Obesity and inflammation. Eur. Cytokine Netw. 2018, 29, 83–94. [Google Scholar] [CrossRef]
- Charlot, A.; Boumiza, R.; Roux, M.; Zoll, J. Obésité, inflammation et COVID-19: Intérêt préventif de l’alimentation Cétogène? Biol. Aujourd’hui 2021, 215, 63–72. [Google Scholar] [CrossRef]
- Das, S.R.; Drazner, M.H.; Dries, D.L.; Vega, G.L.; Stanek, H.G.; Abdullah, S.M.; Canham, R.M.; Chung, A.K.; Leonard, D.; WiansJr, F.H.; et al. Impact of Body Mass and Body Composition on Circulating Levels of Natriuretic Peptides: Results from the Dallas Heart Study. Circulation 2005, 112, 2163–2168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, T.J.; Larson, M.; Levy, D.; Benjamin, E.; Leip, E.P.; Wilson, P.W.; Vasan, R.S. Impact of Obesity on Plasma Natriuretic Peptide Levels. Circulation 2004, 109, 594–600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jordan, J.; Birkenfeld, A.L.; Melander, O.; Moro, C. Natriuretic Peptides in Cardiovascular and Metabolic Crosstalk. Hypertension 2018, 72, 270–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, T.J.; Larson, M.; Keyes, M.J.; Levy, D.; Benjamin, E.; Vasan, R.S. Association of Plasma Natriuretic Peptide Levels With Metabolic Risk Factors in Ambulatory Individuals. Circulation 2007, 115, 1345–1353. [Google Scholar] [CrossRef] [Green Version]
- Sarzani, R.; Spannella, F.; Giulietti, F.; Balietti, P.; Cocci, G.; Bordicchia, M. Cardiac Natriuretic Peptides, Hypertension and Cardiovascular Risk. High Blood Press. Cardiovasc. Prev. 2017, 24, 115–126. [Google Scholar] [CrossRef] [Green Version]
- Schlueter, N.; de Sterke, A.; Willmes, D.M.; Spranger, J.; Jordan, J.; Birkenfeld, A.L. Metabolic actions of natriuretic peptides and therapeutic potential in the metabolic syndrome. Pharmacol. Ther. 2014, 144, 12–27. [Google Scholar] [CrossRef] [Green Version]
- Howard, B.V.; Ruotolo, G.; Robbins, D.C. Obesity and dyslipidemia. Endocrinol. Metab. Clin. N. Am. 2003, 32, 855–867. [Google Scholar] [CrossRef]
- Golia, E.; Limongelli, G.; Natale, F.; Fimiani, F.; Maddaloni, V.; Pariggiano, I.; Bianchi, R.; Crisci, M.; D’Acierno, L.; Giordano, R.; et al. Inflammation and Cardiovascular Disease: From Pathogenesis to Therapeutic Target. Curr. Atheroscler. Rep. 2014, 16, 435. [Google Scholar] [CrossRef]
- Libby, P.; Ridker, P.M.; Hansson, G.K. Progress and challenges in translating the biology of atherosclerosis. Nature 2011, 473, 317–325. [Google Scholar] [CrossRef]
- Soysal, P.; Arik, F.; Smith, L.; Jackson, S.E.; Isik, A.T. Inflammation, Frailty and Cardiovascular Disease. In Frailty and Cardiovascular Diseases; Veronese, N., Ed.; Springer International Publishing: Cham, Switzerland, 2020; Volume 1216, pp. 55–64. ISBN 978-3-030-33329-4. [Google Scholar]
- Lee, M.-K.; Han, K.; Kim, M.K.; Koh, E.S.; Kim, E.S.; Nam, G.E.; Kwon, H.-S. Changes in metabolic syndrome and its components and the risk of type 2 diabetes: A nationwide cohort study. Sci. Rep. 2020, 10, 2313. [Google Scholar] [CrossRef]
- Lemieux, I.; Després, J.-P. Metabolic Syndrome: Past, Present and Future. Nutrients 2020, 12, 3501. [Google Scholar] [CrossRef]
- Hales, C.M.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Prevalence of Obesity and Severe Obesity among Adults: United States, 2017–2018; U.S. Department of Health and Human Services, Centers for Disease Control and Prevention: Atlanta, GA, USA, 2020. [Google Scholar]
- Ligue contre l’obésité. Enquête Épidémiologique Nationale Sur Le Surpoids et l’obésité; ObÉpi-Roche: Paris, France, 2021. [Google Scholar]
- Chan, J.C.; Malik, V.; Jia, W.; Kadowaki, T.; Yajnik, C.S.; Yoon, K.-H.; Hu, F.B. Diabetes in Asia: Epidemiology, risk factors, and pathophysiology. JAMA 2009, 301, 2129–2140. [Google Scholar] [CrossRef] [PubMed]
- Weiss, R.; Dziura, J.; Burgert, T.S.; Tamborlane, W.V.; Taksali, S.E.; Yeckel, C.W.; Allen, K.; Lopes, M.; Savoye, M.; Morrison, J.; et al. Obesity and the Metabolic Syndrome in Children and Adolescents. N. Engl. J. Med. 2004, 350, 2362–2374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Diabetes Association Standards of Medical Care in Diabetes—2009. Diabetes Care 2009, 32, S13–S61. [CrossRef] [PubMed] [Green Version]
- Babio, N.; Bulló, M.; Salas-Salvadó, J. Mediterranean diet and metabolic syndrome: The evidence. Public Health Nutr. 2009, 12, 1607–1617. [Google Scholar] [CrossRef] [Green Version]
- Davis, C.; Bryan, J.; Hodgson, J.; Murphy, K. Definition of the Mediterranean Diet; A Literature Review. Nutrients 2015, 7, 9139–9153. [Google Scholar] [CrossRef]
- Poulsen, S.K.; Due, A.; Jordy, A.B.; Kiens, B.; Stark, K.D.; Stender, S.; Holst, C.; Astrup, A.; Larsen, T.M. Health effect of the New Nordic Diet in adults with increased waist circumference: A 6-mo randomized controlled trial. Am. J. Clin. Nutr. 2014, 99, 35–45. [Google Scholar] [CrossRef] [Green Version]
- Feldeisen, S.E.; Tucker, K.L. Nutritional strategies in the prevention and treatment of metabolic syndrome. Appl. Physiol. Nutr. Metab. 2007, 32, 46–60. [Google Scholar] [CrossRef] [Green Version]
- Pérez-Martínez, P.; Mikhailidis, D.P.; Athyros, V.G.; Bullo, M.; Couture, P.; Covas, M.I.; de Koning, L.; Delgado-Lista, J.; Díaz-López, A.; Drevon, C.A.; et al. Lifestyle recommendations for the prevention and management of metabolic syndrome: An international panel recommendation. Nutr. Rev. 2017, 75, 307–326. [Google Scholar] [CrossRef] [Green Version]
- Wilder, R.M.; Winter, M.D. The Threshold of Ketogenesis. J. Biol. Chem. 1922, 52, 393–401. [Google Scholar] [CrossRef]
- Sampaio, L.P.D.B. Ketogenic diet for epilepsy treatment. Arq. Neuro-Psiquiatr. 2016, 74, 842–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kerndt, P.R.; Naughton, J.L.; Driscoll, C.E.; Loxterkamp, D.A. Fasting: The history, pathophysiology and complications. West. J. Med. 1982, 137, 379–399. [Google Scholar] [PubMed]
- Schönfeld, P.; Reiser, G. Why does Brain Metabolism not Favor Burning of Fatty Acids to Provide Energy?—Reflections on Disadvantages of the Use of Free Fatty Acids as Fuel for Brain. J. Cereb. Blood Flow Metab. 2013, 33, 1493–1499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, N.J.; Wodschow, H.Z.; Nilsson, M.; Rungby, J. Effects of Ketone Bodies on Brain Metabolism and Function in Neurodegenerative Diseases. Int. J. Mol. Sci. 2020, 21, 8767. [Google Scholar] [CrossRef]
- Fukao, T.; Lopaschuk, G.D.; Mitchell, G.A. Pathways and control of ketone body metabolism: On the fringe of lipid biochemistry. Prostaglandins Leukot. Essent. Fat. Acids 2004, 70, 243–251. [Google Scholar] [CrossRef]
- Pierre, K.; Pellerin, L. Monocarboxylate transporters in the central nervous system: Distribution, regulation and function. J. Neurochem. 2005, 94, 1–14. [Google Scholar] [CrossRef]
- Meyer-Rogge, S.; Meyer-Rogge, K. Biochimie Métabolique: Ler Cycle, PACES; De Boeck: Bruxelles, Belgium, 2012; ISBN 978-2-8041-7147-6. [Google Scholar]
- Watanabe, M.; Tozzi, R.; Risi, R.; Tuccinardi, D.; Mariani, S.; Basciani, S.; Spera, G.; Lubrano, C.; Gnessi, L. Beneficial effects of the ketogenic diet on nonalcoholic fatty liver disease: A comprehensive review of the literature. Obes. Rev. 2020, 21, e13024. [Google Scholar] [CrossRef] [Green Version]
- Terzikhan, N.; Doets, E.; Noordegraaf-Schouten, M.V. Extensive literature search and review as preparatory work for the evaluation of the essential composition of total diet replacement products for weight control. EFSA Support. Publ. 2015, 12, 2–21. [Google Scholar] [CrossRef]
- Oh, R.; Gilani, B.; Uppaluri, K.R. Low Carbohydrate Diet. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Gershuni, V.M.; Yan, S.L.; Medici, V. Nutritional Ketosis for Weight Management and Reversal of Metabolic Syndrome. Curr. Nutr. Rep. 2018, 7, 97–106. [Google Scholar] [CrossRef]
- Kosinski, C.; Jornayvaz, F.R. Effects of Ketogenic Diets on Cardiovascular Risk Factors: Evidence from Animal and Human Studies. Nutrients 2017, 9, 517. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ballard, K.D.; Quann, E.E.; Kupchak, B.R.; Volk, B.M.; Kawiecki, D.M.; Fernandez, M.L.; Seip, R.L.; Maresh, C.M.; Kraemer, W.J.; Volek, J.S. Dietary carbohydrate restriction improves insulin sensitivity, blood pressure, microvascular function, and cellular adhesion markers in individuals taking statins. Nutr. Res. 2013, 33, 905–912. [Google Scholar] [CrossRef] [PubMed]
- Carter, J.D.; Vasey, F.B.; Valeriano, J. The effect of a low-carbohydrate diet on bone turnover. Osteoporos. Int. 2006, 17, 1398–1403. [Google Scholar] [CrossRef] [PubMed]
- Dashti, H.M.; Al-Zaid, N.S.; Mathew, T.C.; Al-Mousawi, M.; Talib, H.; Asfar, S.K.; Behbahani, A.I. Long Term Effects of Ketogenic Diet in Obese Subjects with High Cholesterol Level. Mol. Cell. Biochem. 2006, 286, 1. [Google Scholar] [CrossRef] [PubMed]
- Dashti, H.M.; Mathew, T.C.; Khadada, M.; Al-Mousawi, M.; Talib, H.; Asfar, S.K.; Behbahani, A.I.; Al-Zaid, N.S. Beneficial effects of ketogenic diet in obese diabetic subjects. Mol. Cell. Biochem. 2007, 302, 249–256. [Google Scholar] [CrossRef]
- Francois, M.E.; Myette-Cote, E.; Bammert, T.D.; Durrer, C.; Neudorf, H.; DeSouza, C.A.; Little, J.P. Carbohydrate restriction with postmeal walking effectively mitigates postprandial hyperglycemia and improves endothelial function in type 2 diabetes. Am. J. Physiol. Heart Circ. Physiol. 2018, 314, H105–H113. [Google Scholar] [CrossRef]
- Hallberg, S.J.; McKenzie, A.L.; Williams, P.T.; Bhanpuri, N.H.; Peters, A.L.; Campbell, W.W.; Hazbun, T.L.; Volk, B.M.; McCarter, J.; Phinney, S.D.; et al. Effectiveness and Safety of a Novel Care Model for the Management of Type 2 Diabetes at 1 Year: An Open-Label, Non-Randomized, Controlled Study. Diabetes Ther. 2018, 9, 583–612. [Google Scholar] [CrossRef] [Green Version]
- Hernandez, T.L.; Sutherland, J.P.; Wolfe, P.; Allian-Sauer, M.; Capell, W.H.; Talley, N.D.; Wyatt, H.R.; Foster, G.D.; Hill, J.O.; Eckel, R.H. Lack of suppression of circulating free fatty acids and hypercholesterolemia during weight loss on a high-fat, low-carbohydrate diet. Am. J. Clin. Nutr. 2010, 91, 578–585. [Google Scholar] [CrossRef] [Green Version]
- Hussain, T.A.; Mathew, T.C.; Dashti, A.A.; Asfar, S.; Al-Zaid, N.; Dashti, H.M. Effect of low-calorie versus low-carbohydrate ketogenic diet in type 2 diabetes. Nutrition 2012, 28, 1016–1021. [Google Scholar] [CrossRef]
- Johnstone, A.M.; Horgan, G.W.; Murison, S.D.; Bremner, D.M.; Lobley, G.E. Effects of a high-protein ketogenic diet on hunger, appetite, and weight loss in obese men feeding ad libitum. Am. J. Clin. Nutr. 2008, 87, 44–55. [Google Scholar] [CrossRef] [Green Version]
- McKenzie, A.L.; Hallberg, S.J.; Creighton, B.C.; Volk, B.M.; Link, T.M.; Abner, M.K.; Glon, R.M.; McCarter, J.P.; Volek, J.S.; Phinney, S.D. A Novel Intervention Including Individualized Nutritional Recommendations Reduces Hemoglobin A1c Level, Medication Use, and Weight in Type 2 Diabetes. JMIR Diabetes 2017, 2, e5. [Google Scholar] [CrossRef]
- Myette-Côté, É.; Durrer, C.; Neudorf, H.; Bammert, T.D.; Botezelli, J.D.; Johnson, J.D.; DeSouza, C.A.; Little, J.P. The effect of a short-term low-carbohydrate, high-fat diet with or without postmeal walks on glycemic control and inflammation in type 2 diabetes: A randomized trial. Am. J. Physiol. Integr. Comp. Physiol. 2018, 315, R1210–R1219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Partsalaki, I.; Karvela, A.; Spiliotis, B.E. Metabolic impact of a ketogenic diet compared to a hypocaloric diet in obese children and adolescents. J. Pediatr. Endocrinol. Metab. 2012, 25, 697–704. [Google Scholar] [CrossRef] [PubMed]
- Saslow, L.R.; Daubenmier, J.J.; Moskowitz, J.T.; Kim, S.; Murphy, E.J.; Phinney, S.D.; Ploutz-Snyder, R.; Goldman, V.; Cox, R.M.; Mason, A.E.; et al. Twelve-month outcomes of a randomized trial of a moderate-carbohydrate versus very low-carbohydrate diet in overweight adults with type 2 diabetes mellitus or prediabetes. Nutr. Diabetes 2017, 7, 304. [Google Scholar] [CrossRef]
- Saslow, L.R.; Mason, A.E.; Kim, S.; Goldman, V.; Ploutz-Snyder, R.; Bayandorian, H.; Daubenmier, J.; Hecht, F.M.; Moskowitz, J.T. An Online Intervention Comparing a Very Low-Carbohydrate Ketogenic Diet and Lifestyle Recommendations Versus a Plate Method Diet in Overweight Individuals with Type 2 Diabetes: A Randomized Controlled Trial. J. Med. Internet Res. 2017, 19, e36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schiavo, L.; Pilone, V.; Rossetti, G.; Barbarisi, A.; Cesaretti, M.; Iannelli, A. A 4-Week Preoperative Ketogenic Micronutrient-Enriched Diet Is Effective in Reducing Body Weight, Left Hepatic Lobe Volume, and Micronutrient Deficiencies in Patients Undergoing Bariatric Surgery: A Prospective Pilot Study. Obes. Surg. 2018, 28, 2215–2224. [Google Scholar] [CrossRef] [PubMed]
- Tendler, D.; Lin, S.; Yancy, W.S., Jr.; Mavropoulos, J.; Sylvestre, P.; Rockey, D.C.; Westman, E.C. The Effect of a Low-Carbohydrate, Ketogenic Diet on Nonalcoholic Fatty Liver Disease: A Pilot Study. Dig. Dis. Sci. 2007, 52, 589–593. [Google Scholar] [CrossRef]
- Walton, C.M.; Perry, K.; Hart, R.H.; Berry, S.L.; Bikman, B.T. Improvement in Glycemic and Lipid Profiles in Type 2 Diabetics with a 90-Day Ketogenic Diet. J. Diabetes Res. 2019, 2019, 8681959. [Google Scholar] [CrossRef] [Green Version]
- Yancy, W.S., Jr.; Olsen, M.K.; Guyton, J.R.; Bakst, R.P.; Westman, E.C. A Low-Carbohydrate, Ketogenic Diet versus a Low-Fat Diet to Treat Obesity and Hyperlipidemia: A randomized, controlled trial. Ann. Intern. Med. 2004, 140, 769–777. [Google Scholar] [CrossRef]
- Yancy, W.S.; Olsen, M.K.; Dudley, T.; Westman, E.C. Acid-base analysis of individuals following two weight loss diets. Eur. J. Clin. Nutr. 2007, 61, 1416–1422. [Google Scholar] [CrossRef] [Green Version]
- Yancy, W.S.; Westman, E.C.; McDuffie, J.R.; Grambow, S.; Jeffreys, A.S.; Bolton, J.; Chalecki, A.; Oddone, E.Z. A Randomized Trial of a Low-Carbohydrate Diet vs Orlistat Plus a Low-Fat Diet for Weight Loss. Arch. Intern. Med. 2010, 170, 136–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fruh, S.M. Obesity: Risk Factors, Complications, and Strategies for Sustainable Long-Term Weight Management. J. Am. Assoc. Nurse Pract. 2017, 29, S3–S14. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.D.; Ryan, D.H.; Apovian, C.M.; Ard, J.D.; Comuzzie, A.G.; Donato, K.A.; Hu, F.B.; Hubbard, V.S.; Jakicic, J.M.; Kushner, R.F.; et al. 2013 AHA/ACC/TOS Guideline for the Management of Overweight and Obesity in Adults: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. Circulation 2014, 129 (Suppl. S2), S102–S138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, J. Risk Assessment for Cardiovascular Disease with Nontraditional Risk Factors. JAMA J. Am. Med. Assoc. 2018, 320, 316. [Google Scholar] [CrossRef] [PubMed]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the primary prevention of cardiovascular disease: A report of the american college of cardiology/American heart association task force on clinical practice guidelines. Circulation 2019, 140, e596–e646. [Google Scholar] [CrossRef]
- Kerner, W.; Brückel, J.; German Diabetes Association. Definition, Classification and Diagnosis of Diabetes Mellitus. Exp. Clin. Endocrinol. Diabetes 2014, 122, 384–386. [Google Scholar] [CrossRef] [Green Version]
- Indonesian Diabetes Association. Guidelines on the Management and Prevention of Prediabetes. Acta Med. Indones. 2014, 46, 348–359. [Google Scholar]
- Tang, Q.; Li, X.; Song, P.; Xu, L. Optimal cut-off values for the homeostasis model assessment of insulin resistance (HOMA-IR) and pre-diabetes screening: Developments in research and prospects for the future. Drug Discov. Ther. 2015, 9, 380–385. [Google Scholar] [CrossRef] [Green Version]
- Leoni, S.; Tovoli, F.; Napoli, L.; Serio, I.; Ferri, S.; Bolondi, L. Current guidelines for the management of non-alcoholic fatty liver disease: A systematic review with comparative analysis. World J. Gastroenterol. 2018, 24, 3361–3373. [Google Scholar] [CrossRef]
- Yumuk, V.; Tsigos, C.; Fried, M.; Schindler, K.; Busetto, L.; Micic, D.; Toplak, H. European Guidelines for Obesity Management in Adults. Obes. Facts 2015, 8, 402–424. [Google Scholar] [CrossRef]
- Magkos, F.; Fraterrigo, G.; Yoshino, J.; Luecking, C.; Kirbach, K.; Kelly, S.C.; De Las Fuentes, L.; He, S.; Okunade, A.L.; Patterson, B.W.; et al. Effects of Moderate and Subsequent Progressive Weight Loss on Metabolic Function and Adipose Tissue Biology in Humans with Obesity. Cell Metab. 2016, 23, 591–601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wing, R.R.; Lang, W.; Wadden, T.A.; Safford, M.; Knowler, W.C.; Bertoni, A.G.; Hill, J.O.; Brancati, F.L.; Peters, A.; Wagenknecht, L.; et al. Benefits of Modest Weight Loss in Improving Cardiovascular Risk Factors in Overweight and Obese Individuals with Type 2 Diabetes. Diabetes Care 2011, 34, 1481–1486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nathan, D.M.; Buse, J.B.; Davidson, M.B.; Ferrannini, E.; Holman, R.R.; Sherwin, R.; Zinman, B. Medical Management of Hyperglycemia in Type 2 Diabetes: A Consensus Algorithm for the Initiation and Adjustment of Therapy. Diabetes Care 2009, 32, 193–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurukulasuriya, L.R.; Sowers, J.R. Therapies for type 2 diabetes: Lowering HbA1c and associated cardiovascular risk factors. Cardiovasc. Diabetol. 2010, 9, 45. [Google Scholar] [CrossRef] [Green Version]
- Holman, R.R.; Paul, S.K.; Bethel, M.A.; Matthews, D.R.; Neil, H.A. 10-year follow-up of intensive glucose control in type 2 diabetes. N. Engl. J. Med. 2008, 359, 1577–1589. [Google Scholar] [CrossRef] [Green Version]
- Barr, E.L.; Zimmet, P.Z.; Welborn, T.A.; Jolley, D.; Magliano, D.J.; Dunstan, D.W.; Cameron, A.J.; Dwyer, T.; Taylor, H.R.; Tonkin, A.M.; et al. Risk of Cardiovascular and All-Cause Mortality in Individuals with Diabetes Mellitus, Impaired Fasting Glucose, and Impaired Glucose Tolerance: The Australian Diabetes, Obesity, and Lifestyle Study (AusDiab). Circulation 2007, 116, 151–157. [Google Scholar] [CrossRef] [Green Version]
- Huang, D.; Refaat, M.; Mohammedi, K.; Jayyousi, A.; Al Suwaidi, J.; Khalil, C.A. Macrovascular Complications in Patients with Diabetes and Prediabetes. BioMed Res. Int. 2017, 2017, 7839101. [Google Scholar] [CrossRef]
- Liao, H.-W.; Saver, J.; Yeh, H.-C.; Chen, C.-H.S.; Wu, Y.-L.; Lee, M.; Ovbiagele, B. Low fasting glucose and future risks of major adverse outcomes in people without baseline diabetes or cardiovascular disease: A systematic review and meta-analysis. BMJ Open 2019, 9, e026010. [Google Scholar] [CrossRef]
- Park, C.; Guallar, E.; Linton, J.A.; Lee, D.-C.; Jang, Y.; Son, D.K.; Han, E.-J.; Baek, S.J.; Yun, Y.D.; Jee, S.H.; et al. Fasting Glucose Level and the Risk of Incident Atherosclerotic Cardiovascular Diseases. Diabetes Care 2013, 36, 1988–1993. [Google Scholar] [CrossRef] [Green Version]
- Ference, B.A.; Ginsberg, H.N.; Graham, I.; Ray, K.K.; Packard, C.J.; Bruckert, E.; Hegele, R.A.; Krauss, R.M.; Raal, F.J.; Schunkert, H.; et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel. Eur. Heart J. 2017, 38, 2459–2472. [Google Scholar] [CrossRef] [Green Version]
- Yaghi, S.; Elkind, M.S. Lipids and Cerebrovascular Disease: Research and Practice. Stroke 2015, 46, 3322–3328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marston, N.A.; Giugliano, R.P.; Im, K.; Silverman, M.G.; O’Donoghue, M.L.; Wiviott, S.D.; Ference, B.A.; Sabatine, M.S. Association Between Triglyceride Lowering and Reduction of Cardiovascular Risk Across Multiple Lipid-Lowering Therapeutic Classes: A Systematic Review and Meta-Regression Analysis of Randomized Controlled Trials. Circulation 2019, 140, 1308–1317. [Google Scholar] [CrossRef] [PubMed]
- Jeong, S.; Choi, S.; Kim, K.; Kim, S.M.; Lee, G.; Park, S.Y.; Kim, Y.; Son, J.S.; Yun, J.; Park, S.M. Effect of Change in Total Cholesterol Levels on Cardiovascular Disease among Young Adults. J. Am. Hear. Assoc. 2018, 7, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ali, K.M.; Wonnerth, A.; Huber, K.; Wojta, J. Cardiovascular disease risk reduction by raising HDL cholesterol—current therapies and future opportunities. J. Cereb. Blood Flow Metab. 2012, 167, 1177–1194. [Google Scholar] [CrossRef] [Green Version]
- Antonakoudis, G.; Poulimenos, L.; Kifnidis, K.; Zouras, C.; Antonakoudis, H. Blood pressure control and cardiovascular risk reduction. Hippokratia 2007, 11, 114–119. [Google Scholar] [PubMed]
- Sanyal, A.J. AGA technical review on nonalcoholic fatty liver disease. Gastroenterology 2002, 123, 1705–1725. [Google Scholar] [CrossRef]
- Zilberter, T.; Zilberter, Y. Ketogenic Ratio Determines Metabolic Effects of Macronutrients and Prevents Interpretive Bias. Front. Nutr. 2018, 5, 75. [Google Scholar] [CrossRef]
- Seo, J.H.; Lee, Y.M.; Lee, J.S.; Kang, H.C.; Kim, H.D. Efficacy and Tolerability of the Ketogenic Diet According to Lipid:Nonlipid Ratios? Comparison of 3:1 with 4:1 Diet. Epilepsia 2007, 48, 801–805. [Google Scholar] [CrossRef]
- El-Rashidy, O.F.; Nassar, M.F.; Abdel-Hamid, I.A.; Shatla, R.H.; Abdel-Hamid, M.H.; Gabr, S.S.; Mohamed, S.G.; El-Sayed, W.S.; Shaaban, S.Y. Modified Atkins diet vs classic ketogenic formula in intractable epilepsy. Acta Neurol. Scand. 2013, 128, 402–408. [Google Scholar] [CrossRef]
- Ye, F.; Li, X.-J.; Jiang, W.-L.; Sun, H.-B.; Liu, J. Efficacy of and Patient Compliance with a Ketogenic Diet in Adults with Intractable Epilepsy: A Meta-Analysis. J. Clin. Neurol. 2015, 11, 26–31. [Google Scholar] [CrossRef] [Green Version]
- Paoli, A.; Bosco, G.; Camporesi, E.M.; Mangar, D. Ketosis, ketogenic diet and food intake control: A complex relationship. Front. Psychol. 2015, 6, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolb, H.; Kempf, K.; Röhling, M.; Lenzen-Schulte, M.; Schloot, N.C.; Martin, S. Ketone bodies: From enemy to friend and guardian angel. BMC Med. 2021, 19, 313. [Google Scholar] [CrossRef] [PubMed]
- Garcia, D.; Shaw, R.J. AMPK: Mechanisms of Cellular Energy Sensing and Restoration of Metabolic Balance. Mol. Cell 2017, 66, 789–800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Narbonne, P.; Roy, R. La protéine kinase activée par l’AMP (AMPK) protège les réserves énergétiques. Med. Sci. 2009, 25, 565–566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McNamara, N.; Carbone, L.A.; Shellhaas, R. Epilepsy Characteristics and Psychosocial Factors Associated with Ketogenic Diet Success. J. Child Neurol. 2013, 28, 1233–1237. [Google Scholar] [CrossRef] [PubMed]
- Masood, W.; Annamaraju, P.; Uppaluri, K.R. Ketogenic Diet. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Wirrell, E.C. Ketogenic ratio, calories, and fluids: Do they matter? Epilepsia 2008, 49, 17–19. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Flowchart of article selection for the systematic review.

Figure 2.
Beneficial effects of KD on metabolic markers.


{kind=link}
{kind=link}
Table 1.
Summary table presenting the parameters of interest found in the included studies. The cross “x” indicates the parameters measured in the study.
Table 1.
Summary table presenting the parameters of interest found in the included studies. The cross “x” indicates the parameters measured in the study.
| Clinical Measures | Glycemic Profile | Lipid Profile | Liver Profile | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Reference | Weight | BMI | Systolic BP | Diastolic BP | Fasting Glucose | Fasting Insulin | HOMA-IR | HbA1c | Total Cholesterol | HDL | LDL | TG | AST | ALT | Volume of Left Hepatic Lobe | Biopsy |
| [49] Ballard and et al., 2013 | x | x | x | x | x | x | x | x | x | |||||||
| [50] Carter and et al., 2006 | x | x | ||||||||||||||
| [51] Dashti and et al., 2006 | x | x | x | x | x | x | x | |||||||||
| [52] Dashti and et al., 2007 | x | x | x | x | x | x | ||||||||||
| [53] François and et al., 2018 | x | x | ||||||||||||||
| [54] Hallberg and et al., 2018 | x | x | x | x | x | x | x | x | x | x | ||||||
| [55] Hernandez and et al., 2010 | x | x | x | x | x | x | ||||||||||
| [56] Hussain and et al., 2012 | x | x | x | x | x | x | x | x | ||||||||
| [57] Johnstone et al., 2008 | x | x | x | x | x | x | x | x | ||||||||
| [58] McKenzie and et al., 2017 | x | x | x | x | x | x | x | x | x | x | x | x | ||||
| [59] Myette-Coté and et al., 2018 | x | x | x | x | ||||||||||||
| [60] Partsalaki and et al., 2012 | x | x | x | x | x | x | x | x | x | x | x | |||||
| [61] Saslow and et al., 2017 (1) | x | x | x | x | x | x | x | x | x | x | ||||||
| [62] Saslow and et al., 2017 (2) | x | x | x | x | x | |||||||||||
| [63] Schiavo and et al., 2018 | x | x | x | x | x | x | x | x | x | x | x | |||||
| [64] Tendler and et al., 2007 | x | x | x | x | x | x | ||||||||||
| [65] Walton and et al., 2019 | x | x | x | x | x | x | x | x | x | x | ||||||
| [66] Yancy and et al., 2004 | x | x | x | x | x | x | x | |||||||||
| [67] Yancy and et al., 2007 | x | |||||||||||||||
| [68] Yancy and et al., 2010 | x | x | x | x | x | x | x | x | x | x | ||||||
Table 2.
Summary table presenting the characteristics of the study designs.
| Reference | Patients Characteristic | Maximum Carbohydrate Intake of | Duration | Sample Size |
|---|---|---|---|---|
| [49] Ballard and et al., 2013 |
Participants > 18 y.o BMI > 30 | 50 g per day | 6 weeks | n = 21 |
| [50] Carter and et al., 2006 |
Participants > 18 y.o BMI > 30 | 40 g per day | 3 months | n = 13 |
| [51] Dashti and et al., 2006 |
Normal cholesterol level and high cholesterol level adults (>18 y.o) BMI > 30 | 20 g per day | 56 weeks |
Normal cholesterol level adults: n = 23 High cholesterol level adults: n = 26 |
| [52] Dashti and et al., 2007 |
Diabetics and non-diabetics adults (>18 y.o) BMI > 30 | 20 g per day | 56 weeks | Diabetics: n = 31 Non-diabetics: n = 33 |
| [53] François and et al., 2018 |
48 to 72 y.o diabetics participants BMI > 30 | 50 g per day | 4 days | n = 11 |
| [54] Hallberg and et al., 2018 |
Diabetic participants (>18 y.o) BMI > 30 | 30 g per day | 1 year | n = 218 |
| [55] Hernandez and et al., 2010 | Obese participants > 18 y.o | 20 g per day | 6 weeks | n = 32 |
| [56] Hussain and et al., 2012 |
Diabetics and non-diabetics adults (>18 y.o) BMI > 30 | 30 g per day | 24 weeks | Diabetics: n = 102 Non-diabetics: n = 261 |
| [57] Johnstone et al., 2008 |
20 to 65 y.o men BMI > 30 | 5.5 g per day | 4 weeks | n = 17 |
| [58] McKenzie and et al., 2017 |
21 to 65 y.o diabetic participants BMI > 30 | 30 g per day | 10 weeks | n = 238 |
| [59] Myette-Coté and et al., 2018 | 48 to 72 y.o diabetic participants | 50 g per day | 4 days | n = 11 |
| [60] Partsalaki and et al., 2012 |
8 to 18 y.o children and adolescents BMI > 30 | 20 g per day | 6 months | n = 21 |
| [61] Saslow and et al., 2017 (1) |
Diabetic participants > 18 y.o BMI > 30 | 20 to 50 g per day | 6 months | n = 16 |
| [62] Saslow and et al., 2017 (2) | Diabetic obese participants > 18 y.o | 20 to 50 g per day | 32 weeks | n = 12 |
| [63] Schiavo and et al., 2018 |
Participants > 18 y.o BMI > 40 | 15 g per day | 4 weeks | n = 27 |
| [64] Tendler and et al., 2007 |
18 to 65 y.o participants with NAFLD BMI > 30 | 20 g per day | 6 months | n = 5 |
| [65] Walton and et al., 2019 |
18 to 45 y.o diabetic women BMI > 30 | 30 g per day | 90 days | n = 11 |
| [66] Yancy and et al., 2004 |
18 to 65 y.o participants BMI > 30 | 20 g per day | 24 weeks | n = 60 |
| [67] Yancy and et al., 2007 |
18 to 65 y.o participants BMI > 30 | 20 g per day | 24 weeks | n = 21 |
| [68] Yancy and et al., 2010 |
18 to 70 y.o participants BMI > 30 | 20 g per day | 48 weeks | n = 52 |
Table 3.
Summary table presenting the effect of KD on clinical measures, glycemic profile, lipide profile and liver profile. ↓ indicates a decrease and ↑ indicates an increase.
Table 3.
Summary table presenting the effect of KD on clinical measures, glycemic profile, lipide profile and liver profile. ↓ indicates a decrease and ↑ indicates an increase.
| Clinical Measures | Glycemic Profile | Lipid Profile | Liver Profile | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Reference | Weight | BMI | Systolic BP | Diastolic BP | Fasting Glucose | Fasting Insulin | HOMA-IR | HbA1c | Total Cholesterol | HDL | LDL | TG | AST | ALT | Volume of Left Hepatic Lobe | Biopsy |
| [49] Ballard and et al., 2013 | ns | ↓ | ↓ | ns | ↓ | ↓ | ns | ns | ↓ | |||||||
| p = 0.01 | p = 0.001 | p < 0.01 | p < 001 | p < 0.001 | ||||||||||||
| [50] Carter and et al., 2006 | ↓ | ↓ | ||||||||||||||
| p < 0.0008 | p < 0.0001 | |||||||||||||||
| [51] Dashti and et al., 2006 | ↓ | ↓ | ↓ | ↓ | ↑ | ↓ | ↓ | |||||||||
| p < 0.0001 | p < 0.0001 | p < 0.0001 | p < 0.0001 | p < 0.0001 | p < 0.0001 | p < 0.0001 | ||||||||||
| ↓ | ↓ | ↓ | ↓ | ↑ | ↓ | ↓ | ||||||||||
| p < 0.0001 | p < 0.0001 | p < 0.0001 | p < 0.0001 | p < 0.0001 | p < 0.0001 | p < 0.0001 | ||||||||||
| [52] Dashti and et al., 2007 | ↓ | ↓ | ↓ | ↑ | ↓ | ↓ | ||||||||||
| p < 0.0001 | p < 0.0001 | p < 0.0001 | p < 0.0001 | p < 0.0001 | p < 0.0001 | |||||||||||
| ↓ | ↓ | ↓ | ↑ | ↓ | ↓ | |||||||||||
| p < 0.0001 | p < 0.0069 | p < 0.002 | p < 0.0001 | p < 0.0001 | p < 0.0001 | |||||||||||
| [53] François and et al., 2018 | ns | ↓ | ||||||||||||||
| p < 0.05 | ||||||||||||||||
| [54] Hallberg and et al., 2018 | ↓ | ↓ | ↓ | ↓ | ↓ | ↑ | ↓ | ↓ | ↓ | ↓ | ||||||
| p < 0.0001 | p < 0.0001 | p < 0.0001 | p < 0.0001 | p < 0.0001 | p < 0.0001 | p < 0.0001 | p < 0.0001 | p < 0.0001 | p < 0.0001 | |||||||
| [55] Hernandez and et al., 2010 | ↓ | ns | ↓ | ns | ns | ↓ | ||||||||||
| p < 0.0001 | p = 0.03 | p = 0.01 | ||||||||||||||
| [56] Hussain and et al., 2012 | ↓ | ↓ | ↓ | ↓ | ↑ | ↓ | ↓ | |||||||||
| p < 0.0001 | p < 0.0001 | p < 0.0001 | p < 0.0001 | p < 0.0001 | p < 0.0001 | p < 0.0001 | ||||||||||
| ↓ | ↓ | ↓ | ↓ | ↓ | ↑ | ↓ | ↓ | |||||||||
| p < 0.0001 | p < 0.0001 | p < 0.0001 | p < 0.05 | p < 0.0001 | p < 0.0001 | p < 0.0001 | p < 0.0001 | |||||||||
| [57] Johnstone et al., 2008 | ↓ | ↓ | ↓ | ↓ | ns | ns | ns | ns | ||||||||
| p = 0.006 | p < 0.001 | p < 0.001 | p < 0.001 | |||||||||||||
| [58] McKenzie and et al., 2017 | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | ns | ns | ↓ | ↓ | ↓ | ||||
| p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | p = 0.009 | p < 0.001 | p < 0.001 | p < 0.001 | |||||||
| [59] Myette-Coté and et al., 2018 | ↓ | ↓ | ns | ns | ||||||||||||
| p < 0.001 | p < 0.001 | |||||||||||||||
| [60] Partsalaki and et al., 2012 | ↓ | ↓ | ns | ns | ns | ↓ | ↓ | ns | ns | ns | ns | |||||
| p < 0.001 | p < 0.001 | p = 0.017 | p = 0.014 | |||||||||||||
| [61] Saslow and et al., 2017 (1) | ↓ | ↓ | ns | ns | ns | ns | ↓ | ns | ns | ↓ | ||||||
| p < 0.001 | p < 0.001 | p = 0.007 | p = 0.022 | |||||||||||||
| [62] Saslow and et al., 2017 (2) | ↓ | ↓ | ns | ns | ↓ | |||||||||||
| p < 0.001 | p < 0.002 | p < 0.01 | ||||||||||||||
| [63] Schiavo and et al., 2018 | ↓ | ↓ | ↓ | ↓ | ns | ↓ | ↓ | ↓ | ↓ | ↓ | ||||||
| p < 0.001 | p < 0.001 | p = 0.0108 | p < 0.001 | p < 0.001 | p < 0.0001 | p < 0.001 | p < 0.001 | p < 0.001 | ||||||||
| [64] Tendler and et al., 2007 | ↓ | ↓ | ns | ns | ns | ↓ steatosis (p = 0.02) ↓ necro-inflammation (p = 0.02) ↓ fibrosis (p = 0.07) | ||||||||||
| p < 0.036 | p < 0.006 | |||||||||||||||
| [65] Walton and et al., 2019 | ↓ | ↓ | ↓ | ↓ | ↓ | ↑ | ns | ↓ | ns | ns | ||||||
| p < 0.001 | p < 0.0001 | p < 0.0001 | p < 0.005 | p < 0.0001 | p < 0.005 | p < 0.005 | ||||||||||
| [66] Yancy and et al., 2004 | ↓ | ns | ns | ↓ | ↑ | ns | ↓ | |||||||||
| p < 0.001 | p = 0.08 | p < 0.001 | p < 0.001 | |||||||||||||
| [67] Yancy and et al., 2007 | ns | |||||||||||||||
| [68] Yancy and et al., 2010 | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | ns | ↑ | ns | ↓ | ||||||
| p-val not available | p-val not available | p-val not available | p-val not available | p-val not available | p-val not available | p-val not available | p-val not available | |||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Charlot, A.; Zoll, J. Beneficial Effects of the Ketogenic Diet in Metabolic Syndrome: A Systematic Review. Diabetology 2022, 3, 292-309. https://0-doi-org.brum.beds.ac.uk/10.3390/diabetology3020020
AMA Style
Charlot A, Zoll J. Beneficial Effects of the Ketogenic Diet in Metabolic Syndrome: A Systematic Review. Diabetology. 2022; 3(2):292-309. https://0-doi-org.brum.beds.ac.uk/10.3390/diabetology3020020
Chicago/Turabian StyleCharlot, Anouk, and Joffrey Zoll. 2022. "Beneficial Effects of the Ketogenic Diet in Metabolic Syndrome: A Systematic Review" Diabetology 3, no. 2: 292-309. https://0-doi-org.brum.beds.ac.uk/10.3390/diabetology3020020