

Utilizing the Glucose and Insulin Response Shape of an Oral Glucose Tolerance Test to Predict Dysglycemia in Children with Overweight and Obesity, Ages 8–18 Years
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Design
2.2. The Oral Glucose Tolerance Test
2.2.1. OGTT Administration and Laboratory Parameters
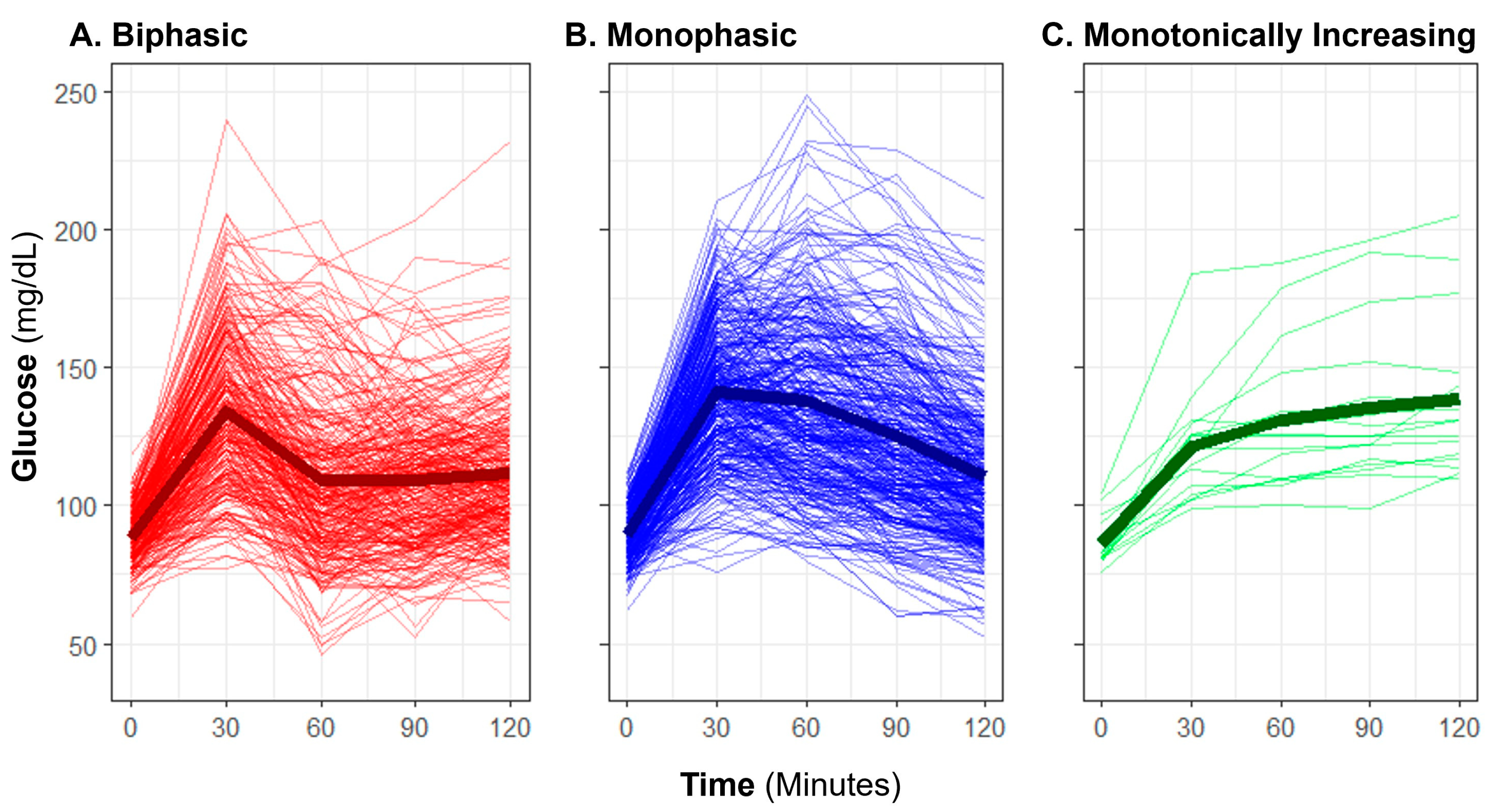
2.2.2. Manual OGTT Shape Classifications
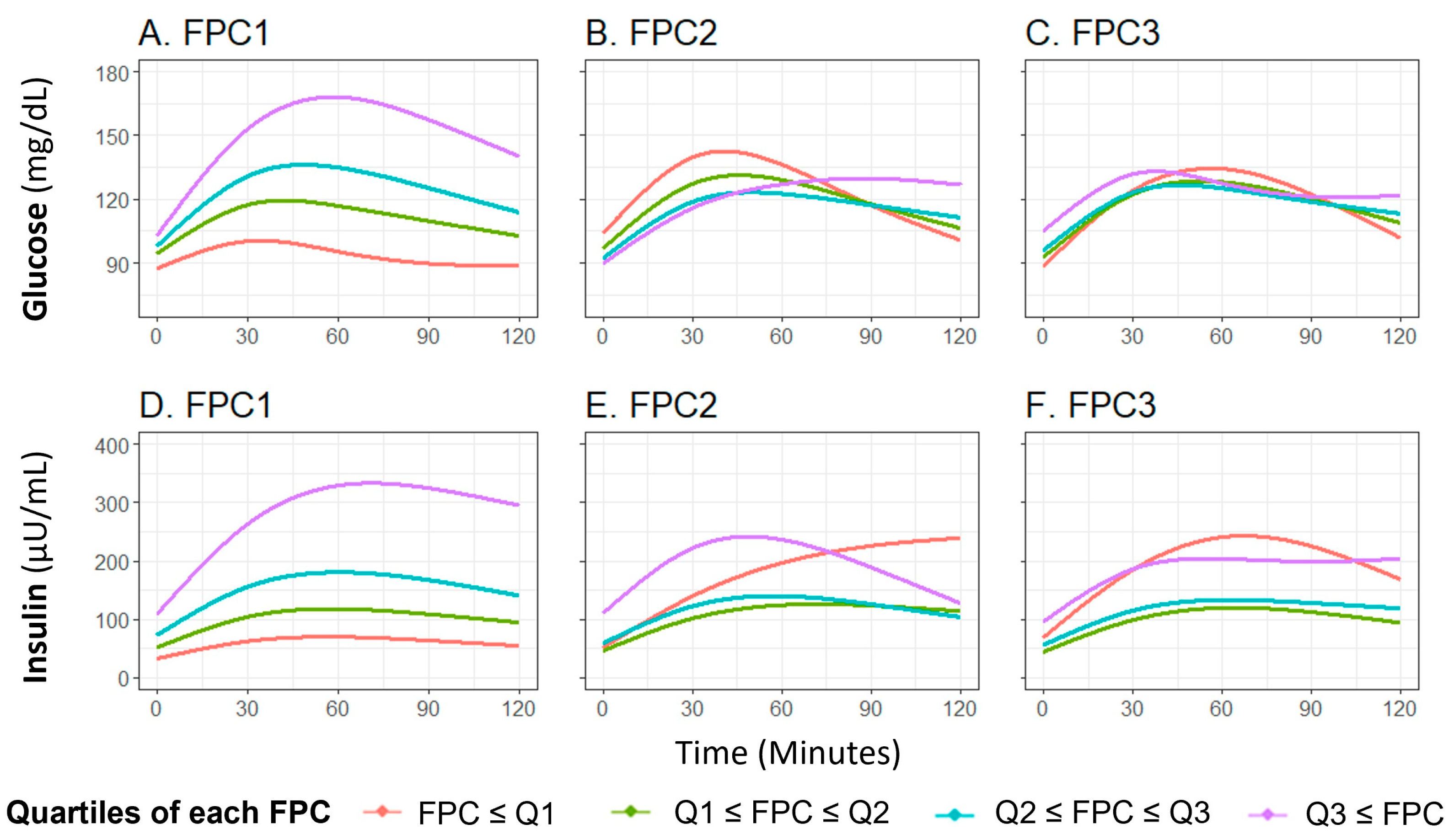
2.2.3. OGTT Shape Classifications Using Functional Data Analysis (FDA)
2.3. Statistical Analysis
2.3.1. Cross-Sectional Analysis
2.3.2. Longitudinal Analysis
3. Results
3.1. Sample Characteristics
3.2. Cross-Sectional Analysis
3.2.1. Glucose Profile Manual Shape Classifications
3.2.2. Glucose and Insulin FDA Shape Characteristics
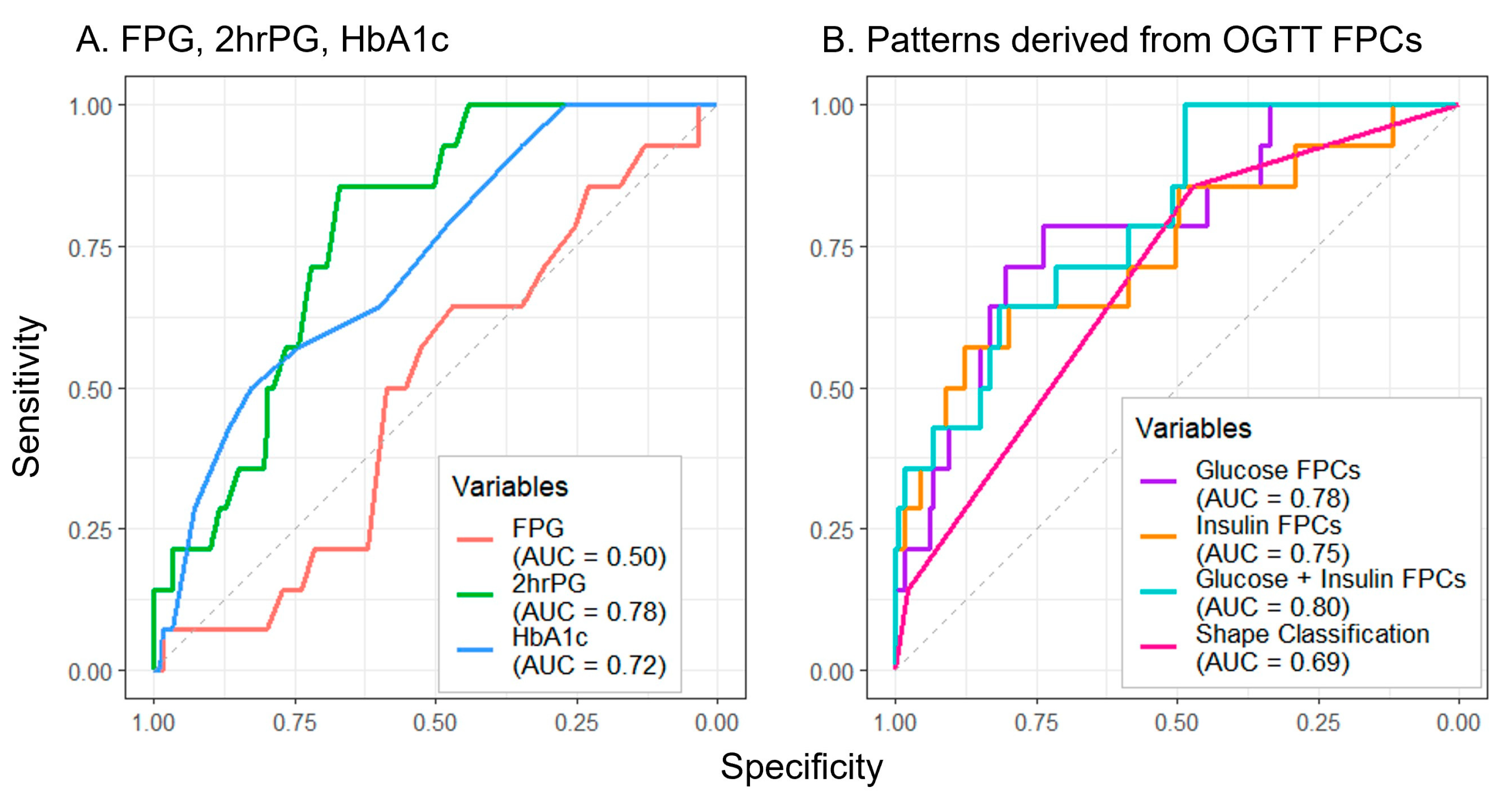
3.2.3. Cross-Sectional Associations with Metabolic Health Parameters
3.3. Longitudinal Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Divers, J.; Mayer-Davis, E.J.; Lawrence, J.M.; Isom, S.; Dabelea, D.; Dolan, L.; Imperatore, G.; Marcovina, S.; Pettitt, D.J.; Pihoker, C.; et al. Trends in Incidence of Type 1 and Type 2 Diabetes Among Youths—Selected Counties and Indian Reservations, United States, 2002–2015. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 161–165. [Google Scholar] [CrossRef]
- Dabelea, D.; Mayer-Davis, E.J.; Saydah, S.; Imperatore, G.; Linder, B.; Divers, J.; Bell, R.; Badaru, A.; Talton, J.W.; Crume, T.; et al. Prevalence of type 1 and type 2 diabetes among children and adolescents from 2001 to 2009. JAMA 2014, 311, 1778–1786. [Google Scholar] [CrossRef] [PubMed]
- Fryar, C.D.; Carroll, M.D.; Ogden, C.L. Prevalence of Overweight, Obesity, and Severe Obesity among Children and Adolescents Aged 2–19 Years: United States, 1963–1965 through 2015–2016; National Center for Health Statistics (U.S.): Hyattsville, MD, USA, 2018.
- American Diabetes Association. Economic costs of diabetes in the US in 2017. Diabetes Care 2018, 41, 917–928. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. 12. Children and Adolescents: Standards of Medical Care in Diabetes-2018. Diabetes Care 2018, 41, S126–S136. [Google Scholar] [CrossRef] [PubMed]
- ElSayed, N.A.; Aleppo, G.; Aroda, V.R.; Bannuru, R.R.; Brown, F.M.; Bruemmer, D.; Collins, B.S.; Hilliard, M.E.; Isaacs, D.; Johnson, E.L.; et al. 2. Classification and Diagnosis of Diabetes: Standards of Care in Diabetes-2023. Diabetes Care 2023, 46, S19–S40. [Google Scholar] [CrossRef]
- Jagannathan, R.; Neves, J.S.; Dorcely, B.; Chung, S.T.; Tamura, K.; Rhee, M.; Bergman, M. The Oral Glucose Tolerance Test: 100 Years Later. Diabetes Metab. Syndr. Obes. Targets Ther. 2020, 13, 3787–3805. [Google Scholar] [CrossRef]
- Di Bonito, P.; Licenziati, M.R.; Corica, D.; Wasniewska, M.; Di Sessa, A.; Miraglia Del Giudice, E.; Morandi, A.; Maffeis, C.; Faienza, M.F.; Mozzillo, E.; et al. Which Is the Most Appropriate Cut-Off of HbA1c for Prediabetes Screening in Caucasian Youths with Overweight or Obesity? Int. J. Environ. Res. Public Health 2023, 20, 928. [Google Scholar] [CrossRef]
- La Valle, A.; d’Annunzio, G.; Campanello, C.; Tantari, G.; Pistorio, A.; Napoli, F.; Patti, G.; Crocco, M.; Bassi, M.; Minuto, N.; et al. Are glucose and insulin levels at all time points during OGTT a reliable marker of diabetes mellitus risk in pediatric obesity? J. Endocrinol. Investig. 2023, 46, 1685–1694. [Google Scholar] [CrossRef]
- Brar, P.C.; Mehta, S.; Brar, A.; Pierce, K.A.; Albano, A.; Bergman, M. Value of 1-Hour Plasma Glucose During an Oral Glucose Tolerance Test in a Multiethnic Cohort of Obese Children and Adolescents. Clin. Med. Insights. Endocrinol. Diabetes 2023, 16, 11795514231177206. [Google Scholar] [CrossRef]
- Yin, C.; Zhang, H.; Xiao, Y.; Liu, W. Shape of glucose curve can be used as a predictor for screening prediabetes in obese children. Acta Paediatr. 2014, 103, e199–e205. [Google Scholar] [CrossRef]
- Tschritter, O.; Fritsche, A.; Shirkavand, F.; Machicao, F.; Haring, H.; Stumvoll, M. Assessing the shape of the glucose curve during an oral glucose tolerance test. Diabetes Care 2003, 26, 1026–1033. [Google Scholar] [CrossRef]
- Arslanian, S.; El Ghormli, L.; Young Kim, J.; Bacha, F.; Chan, C.; Ismail, H.M.; Levitt Katz, L.E.; Levitsky, L.; Tryggestad, J.B.; White, N.H.; et al. The Shape of the Glucose Response Curve During an Oral Glucose Tolerance Test: Forerunner of Heightened Glycemic Failure Rates and Accelerated Decline in beta-Cell Function in TODAY. Diabetes Care 2019, 42, 164–172. [Google Scholar] [CrossRef]
- de Andrade Mesquita, L.; Pavan Antoniolli, L.; Cittolin-Santos, G.F.; Gerchman, F. Distinct metabolic profile according to the shape of the oral glucose tolerance test curve is related to whole glucose excursion: A cross-sectional study. BMC Endocr. Disord. 2018, 18, 56. [Google Scholar] [CrossRef]
- Nolfe, G.; Spreghini, M.R.; Sforza, R.W.; Morino, G.; Manco, M. Beyond the morphology of the glucose curve following an oral glucose tolerance test in obese youth. Eur. J. Endocrinol. 2012, 166, 107–114. [Google Scholar] [CrossRef]
- Kim, J.Y.; Michaliszyn, S.F.; Nasr, A.; Lee, S.; Tfayli, H.; Hannon, T.; Hughan, K.S.; Bacha, F.; Arslanian, S. The Shape of the Glucose Response Curve During an Oral Glucose Tolerance Test Heralds Biomarkers of Type 2 Diabetes Risk in Obese Youth. Diabetes Care 2016, 39, 1431–1439. [Google Scholar] [CrossRef] [PubMed]
- Manco, M.; Nolfe, G.; Pataky, Z.; Monti, L.; Porcellati, F.; Gabriel, R.; Mitrakou, A.; Mingrone, G. Shape of the OGTT glucose curve and risk of impaired glucose metabolism in the EGIR-RISC cohort. Metabolism 2017, 70, 42–50. [Google Scholar] [CrossRef] [PubMed]
- La Grasta Sabolic, L.; Pozgaj Sepec, M.; Cigrovski Berkovic, M.; Stipancic, G. Time to the Peak, Shape of the Curve and Combination of These Glucose Response Characteristics During Oral Glucose Tolerance Test as Indicators of Early Beta-cell Dysfunction in Obese Adolescents. J. Clin. Res. Pediatr. Endocrinol. 2021, 13, 160–169. [Google Scholar] [CrossRef] [PubMed]
- Cree-Green, M.; Xie, D.; Rahat, H.; Garcia-Reyes, Y.; Bergman, B.C.; Scherzinger, A.; Diniz Behn, C.; Chan, C.L.; Kelsey, M.M.; Pyle, L.; et al. Oral Glucose Tolerance Test Glucose Peak Time Is Most Predictive of Prediabetes and Hepatic Steatosis in Obese Girls. J. Endocr. Soc. 2018, 2, 547–562. [Google Scholar] [CrossRef]
- Frøslie, K.F.; Røislien, J.; Qvigstad, E.; Godang, K.; Bollerslev, J.; Voldner, N.; Henriksen, T.; Veierød, M.B. Shape information from glucose curves: Functional data analysis compared with traditional summary measures. BMC Med. Res. Methodol. 2013, 13, 6. [Google Scholar] [CrossRef] [PubMed]
- Szczesniak, R.D.; Li, D.; Duan, L.L.; Altaye, M.; Miodovnik, M.; Khoury, J.C. Longitudinal Patterns of Glycemic Control and Blood Pressure in Pregnant Women with Type 1 Diabetes Mellitus: Phenotypes from Functional Data Analysis. Am. J. Perinatol. 2016, 33, 1282–1290. [Google Scholar] [CrossRef] [PubMed]
- Gecili, E.; Huang, R.; Khoury, J.C.; King, E.; Altaye, M.; Bowers, K.; Szczesniak, R.D. Functional data analysis and prediction tools for continuous glucose-monitoring studies. J. Clin. Transl. Sci. 2020, 5, e51. [Google Scholar] [CrossRef]
- Lee, J.M.; Gebremariam, A.; Wu, E.L.; LaRose, J.; Gurney, J.G. Evaluation of nonfasting tests to screen for childhood and adolescent dysglycemia. Diabetes Care 2011, 34, 2597–2602. [Google Scholar] [CrossRef] [PubMed]
- Vajravelu, M.E.; Hirschfeld, E.; Gebremariam, A.; Burant, C.F.; Herman, W.H.; Peterson, K.E.; Meijer, J.L.; Lee, J.M. Prospective Test Performance of Nonfasting Biomarkers to Identify Dysglycemia in Children and Adolescents. Horm. Res. Paediatr. 2023, 96, 316–324. [Google Scholar] [CrossRef] [PubMed]
- LaBarre, J.L.; Hirschfeld, E.; Soni, T.; Kachman, M.; Wigginton, J.; Duren, W.; Fleischman, J.Y.; Karnovsky, A.; Burant, C.F.; Lee, J.M. Comparing the Fasting and Random-Fed Metabolome Response to an Oral Glucose Tolerance Test in Children and Adolescents: Implications of Sex, Obesity, and Insulin Resistance. Nutrients 2021, 13, 3365. [Google Scholar] [CrossRef] [PubMed]
- Gallego-Suarez, C.; Bulan, A.; Hirschfeld, E.; Wachowiak, P.; Abrishami, S.; Griffin, C.; Sturza, J.; Tzau, A.; Hayes, T.; Woolford, S.J.; et al. Enhanced Myeloid Leukocytes in Obese Children and Adolescents at Risk for Metabolic Impairment. Front. Endocrinol. 2020, 11, 327. [Google Scholar] [CrossRef] [PubMed]
- CDC. Defining Childhood Weight Status. Available online: https://www.cdc.gov/obesity/childhood/defining.html (accessed on 3 March 2022).
- Kuczmarski, R.J.; Ogden, C.L.; Guo, S.S.; Grummer-Strawn, L.M.; Flegal, K.M.; Mei, Z.; Wei, R.; Curtin, L.R.; Roche, A.F.; Johnson, C.L. 2000 CDC Growth Charts for the United States: Methods and development. Vital Health Stat. 2002, 11, 1–190. [Google Scholar]
- Utzschneider, K.M.; Younes, N.; Rasouli, N.; Barzilay, J.I.; Banerji, M.A.; Cohen, R.M.; Gonzalez, E.V.; Ismail-Beigi, F.; Mather, K.J.; Raskin, P.; et al. Shape of the OGTT glucose response curve: Relationship with beta-cell function and differences by sex, race, and BMI in adults with early type 2 diabetes treated with metformin. BMJ Open Diabetes Res. Care 2021, 9, e002264. [Google Scholar] [CrossRef] [PubMed]
- Ramsay, J.; Hooker, G.; Graves, S. Package ‘fda’. Available online: https://cran.r-project.org/web/packages/fda/fda.pdf (accessed on 4 September 2023).
- Hollander, M.; Wolfe, D.A. Nonparametric Statistical Methods; John Wiley & Sons: New York, NY, USA, 1973. [Google Scholar]
- Agresti, A. Categorical Data Analysis; John Wiley & Sons: New York, NY, USA, 1990. [Google Scholar]
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.C.; Muller, M. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinform. 2011, 12, 77. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing. Available online: https://www.R-project.org/ (accessed on 3 March 2022).
- Kelsey, M.M.; Zeitler, P.S. Insulin Resistance of Puberty. Curr. Diab. Rep. 2016, 16, 64. [Google Scholar] [CrossRef]
- Tobisch, B.; Blatniczky, L.; Barkai, L. Cardiometabolic risk factors and insulin resistance in obese children and adolescents: Relation to puberty. Pediatr. Obes. 2015, 10, 37–44. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall (N = 671) 1 | |
|---|---|
| Study Visits Completed | |
| Baseline and Follow-Up | 193 (28.8%) |
| Baseline Only | 478 (71.2%) |
| Age (Years) | 13.5 [11.5, 15.4] |
| Sex | |
| Female | 362 (53.9%) |
| Male | 309 (46.1%) |
| Race | |
| White | 386 (57.5%) |
| Black or African American | 212 (31.6%) |
| Other/Multiracial | 52 (7.8%) |
| Unknown/Not Reported | 21 (3.1%) |
| Ethnicity | |
| Non-Hispanic/Latino | 632 (94.2%) |
| Hispanic/Latino | 39 (5.8%) |
| BMI Percentile | 97.0 [94.1, 98.8] |
| OGTT Curve Shape Classification | |
| Monophasic | 367 (54.7%) |
| Biphasic | 282 (42.0%) |
| Monotonically Increasing | 17 (2.5%) |
| Inconclusive | 5 (0.7%) |
| Characteristic | At Baseline 1 | At Follow-Up 1 | p-Value 2 |
|---|---|---|---|
| Age (years) | 13.3 [11.5, 15.3] | 14.7 [12.9, 16.5] | |
| Δ Age (months) | 14.5 [12.6, 17.2] | ||
| Dysglycemia | 1.000 | ||
| No (%) | 179 (92.7%) | 179 (92.7%) | |
| Yes (%) | 14 (7.3%) | 14 (7.3%) | |
| FPG (mg/dL) | 83 [79, 90] | 87 [83, 91] | <0.001 |
| 2hrPG (mg/dL) | 99 [86, 114] | 102 [86, 114] | 0.438 |
| HbA1c (%) 3 | 5.2 [5.0, 5.4] | 5.2 [5.0, 5.4] | <0.001 |
| BMI Percentile | 96.2 [92.1, 98.6] | 96.3 [91.5, 98.8] | 0.567 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Renier, T.J.; Mai, H.J.; Zheng, Z.; Vajravelu, M.E.; Hirschfeld, E.; Gilbert-Diamond, D.; Lee, J.M.; Meijer, J.L. Utilizing the Glucose and Insulin Response Shape of an Oral Glucose Tolerance Test to Predict Dysglycemia in Children with Overweight and Obesity, Ages 8–18 Years. Diabetology 2024, 5, 96-109. https://0-doi-org.brum.beds.ac.uk/10.3390/diabetology5010008
Renier TJ, Mai HJ, Zheng Z, Vajravelu ME, Hirschfeld E, Gilbert-Diamond D, Lee JM, Meijer JL. Utilizing the Glucose and Insulin Response Shape of an Oral Glucose Tolerance Test to Predict Dysglycemia in Children with Overweight and Obesity, Ages 8–18 Years. Diabetology. 2024; 5(1):96-109. https://0-doi-org.brum.beds.ac.uk/10.3390/diabetology5010008
Chicago/Turabian StyleRenier, Timothy J., Htun Ja Mai, Zheshi Zheng, Mary Ellen Vajravelu, Emily Hirschfeld, Diane Gilbert-Diamond, Joyce M. Lee, and Jennifer L. Meijer. 2024. "Utilizing the Glucose and Insulin Response Shape of an Oral Glucose Tolerance Test to Predict Dysglycemia in Children with Overweight and Obesity, Ages 8–18 Years" Diabetology 5, no. 1: 96-109. https://0-doi-org.brum.beds.ac.uk/10.3390/diabetology5010008