
The Papanicolaou Society of Cytopathology System for Reporting Pancreaticobiliary Cytology: A Retrospective Review

Department of Pathology and Anatomical Sciences, University of Missouri, Columbia, MO 65211, USA
J. Mol. Pathol. 2021, 2(2), 101-108; https://0-doi-org.brum.beds.ac.uk/10.3390/jmp2020010
Submission received: 26 February 2021
/
Revised: 23 March 2021
/
Accepted: 26 March 2021
/
Published: 5 April 2021
(This article belongs to the Special Issue Selected Highlights of the 9th Molecular Cytopathology Meeting)
Abstract
:Since the introduction of the Papanicolaou Society of Cytopathology System for Reporting Pancreaticobiliary Cytology, much experience has been gained and published concerning the utility of the diagnostic categories, malignancy risk of the categories and reproducibility of the system. This new information has resulted in modifications to the system which will become part of the World Health Organization (WHO) System for Reporting Pancreatic Cytology. Herein we report our experience with the system and information from the published literature.
1. Introduction
In 2015, the Papanicolaou Society of Cytopathology (PSC) published its system for reporting pancreaticobiliary cytology [1,2]. This system was widely adopted and a number of publications reviewed experience with implementing the system, working with the system, risk stratification using the published categories and, finally, reproducibility among observers for various categories within this system. Reviews of the Papanicolaou proposal for standardized terminology and nomenclature, have shown utility for this system [3,4]
2. Papanicolaou Society of Cytopathology Categories and Nomenclature
The Papanicolaou Society of Cytopathology established a system composed of six categories, one of which is sub-divided into two sub-categories [1,2]. The categories scheme is shown in Table 1.
2.1. Category I
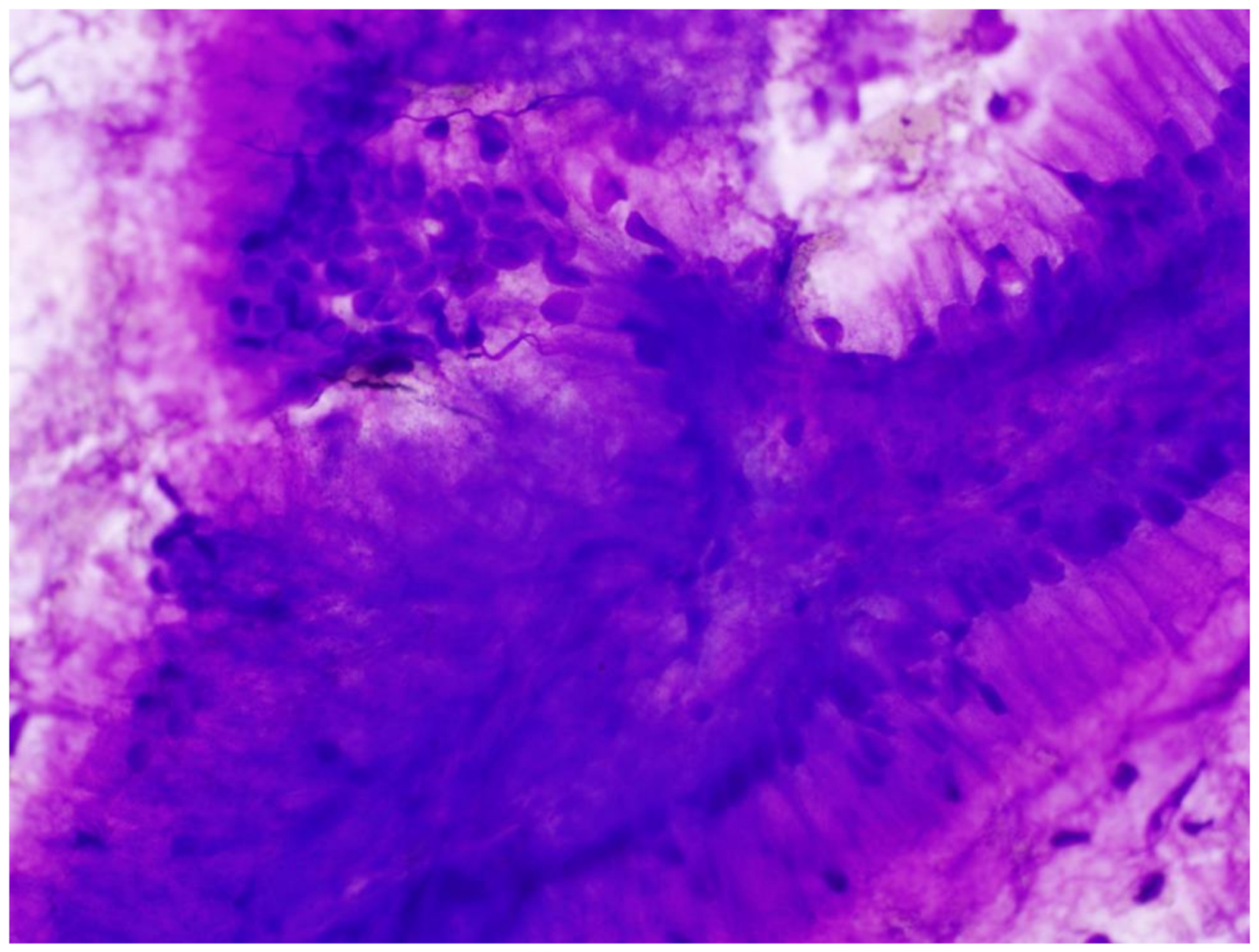
The first category, “non-diagnostic”, refers to cytology specimens that provide no useful diagnostic information about the lesion sampled. Any cellular atypia precludes a non-diagnostic report. Cytology samples included in this category are characterized by a preparation artifact that precludes evaluation of the cellular component. Obscuring artifacts such as hemorrhage or extensive necrosis also result in a non-diagnostic categorization when they obscure the cellular component (Figure 1). Specimens containing gastrointestinal epithelium only are considered non-diagnostic because such epithelium indicates that the lesions seen on imaging studies were not sampled. Similarly, normal pancreatic tissue elements, in which imaging identifies a definitive solid or cystic mass, are considered non-diagnostic. Acellular specimens are designated non-diagnostic when a solid mass or pancreaticobiliary brushing specimen is obtained from a stricture. Similarly, acellular specimens obtained from a cyst that shows no evidence of a mucinous etiology are non-diagnostic. When acellular cyst aspirates are associated with thick colloid-like mucus, an elevated (above 192 ng/mL) carcinoembryonic carcinoembryonic Antigen (CEA) level or a KRAS or GNAS mutation, the material is considered diagnostic because a mucinous etiology was established. The risk of malignancy for the nondiagnostic category is approximately 20 to 25% [5,6].
2.2. Category II
“Negative for malignancy” includes a number of inflammatory and reactive lesions: acute pancreatitis, chronic pancreatitis, autoimmune pancreatitis, pseudocyst (Figure 2), lymphoepithelial cyst and splenule or accessory spleen. When imaging discloses no distinct solid or cystic lesion or stricture, benign pancreatic tissue is included in the negative category. When a distinct lesion is seen on imaging, such samples should be placed in “non-diagnostic”.
Specimens showing minor degrees of loss of cell or nuclear polarity are placed in the negative category. When the cytologist believes the changes are due to inflammation or repair, minor irregularities in the “honeycomb” pattern are insufficient for inclusion in the “atypical” category.
The risk of malignancy in the “benign” category is approximately 1% [6]. Management options depend on the nature of the abnormality. In general, surgical resection is not required for lesions in the “benign” category. For acute and chronic pancreatitis, treatment of the underlying etiology is appropriate. Autoimmune pancreatitis is currently treated with corticosteroids. Pseudocysts are drained.
2.3. Category III
“Atypical” is one of two indeterminate categories which, along with “suspicious for malignancy”, helps stratify the spectrum of morphologic changes between clearly benign and clearly malignant cytologic findings. This use of two indeterminate categories allows clinically useful stratification of the variable degrees of nuclear enlargement, nuclear hyperchromasia and anisonucleosis, in smears that are not clearly benign or clearly malignant. The “atypical” category contains specimens that have greater degrees of nuclear and architectural abnormalities than can be reasonably placed in the negative-for-malignancy category but insufficiently severe to be placed in the suspicious-for-malignancy category.
Because there is a spectrum of change among benign, atypical, suspicious for malignancy and malignant, definitive criteria for these indeterminate categories are difficult to define. Both qualitative and quantitative abnormalities are evaluated but definitive cut points have not been established. Characteristically, specimens from the atypical category demonstrate loss of architectural polarity with mild alterations and loss of the benign “honeycomb” pattern (Figure 3). Nuclear crowding is seen along with minor degrees of nuclear overlapping. This results in the “drunken honeycomb” pattern. Characteristically, features of marked dysmorphology such as cell balls, marked nuclear overlapping, true nuclear molding and markedly irregular nuclear membranes are not seen. Additionally, variability in nuclear size and shape (anisonucleosis) is present to a modest degree and not as marked as in cases designated as “suspicious for malignancy” or “malignant”. In cases designated as “atypical”, the nuclear/cytoplasmic ratio remains near normal. Other features of malignancy are not seen. While nucleoli may be enlarged, true macronucleoli are not observed. The smear background is clean or contains red blood cells. Necrosis is characteristically absent and mitotic figures are not seen. The estimated risk of malignancy for the “atypical” category is between 44 and 62% [5,6]
2.4. Category IV
The “neoplastic category” is divided into 2 sub-categories, “benign” and “other”. “Benign” contains relatively few neoplasms that are sampled by FNA, the most common of which is serous cystadenoma, but rare examples of neuroendocrine microadenoma and lymphangioma have been sampled. In the study by Hoda et al., [6] the risk of malignancy for the “neoplasm benign” category was estimated to be zero, but this was based only on four cases. Management recommendations are dependent on neoplasm type but in general, surgical resection for serous cystadenomas is recommended for symptomatic patients or for surgically fit patients with large cystadenomas. Non-functioning neuroendocrine microadenomas should be followed by observation up to a size of 5 mm, while functioning microadenomas should be removed for relief of symptoms.
The sub-category “other” contains a variety of cystic and solid neoplasms with variable biological behavior. As originally defined in the PSC system, this category contained pancreatic neuroendocrine tumors, solid pseudo-papillary neoplasms, intraductal papillary mucinous neoplasms and mucinous cystic neoplasms. Hoda et al. [6] estimated that the malignancy risk for the overall category to be approximately 30% [6]. However, neoplastic mucinous cysts are associated with variable behavior depending on the degree of nuclear atypia present. Neoplastic mucinous cysts with low-grade atypia (Figure 4) have a malignancy risk of approximately 4%, while those with high-grade atypia have a malignancy risk of approximately 90% [6]. The diagnosis of solid pseudo-papillary neoplasm and pancreatic neuroendocrine tumor predominately relies on cytomorphologic features of smeared material but ancillary testing including immunohistochemistry for neuroendocrine markers, Ki-67 and beta-catenin can play an important role in the specific diagnosis and grading of these neoplasms.
The workup of neoplastic mucinous cysts assigned to the category “neoplasm, other” includes the combination of imaging findings, gross appearance of the cyst fluid, clinical laboratory studies, CEA levels and cytomorphology. Importantly, even when acellular material is aspirated from a neoplastic mucinous cyst, the sample can be appropriately assigned to the “neoplasm, other” category based on gross appearance of thick mucin coupled with a CEA level of at least 192 ng/mL or the presence of KRAS/GNAS mutations [7,8,9,10].
Solid pseudo-papillary neoplasms are resected while the management of pancreatic neuroendocrine neoplasms is somewhat more variable. Small pancreatic neuroendocrine tumors may be followed in elderly patients and those in poor health while neoplasms occurring in younger fit patients are usually resected. Recently, the World Health Organization (WHO) has reclassified pancreatic neuroendocrine tumors as malignancies and this reclassification may significantly affect management decisions.
Mucinous cystic neoplasms are resected regardless of cytologic grade. The management of intraductal papillary mucinous neoplasms is more complex and depends on cytologic grade as well as location in the pancreas. Main duct and combined type intraductal papillary mucinous neoplasms (IPMNs) are resected because of the associated significant risk for malignancy. On the other hand, branch–duct intraductal papillary mucinous neoplasms when of low-grade and occurring in elderly or infirm patients may be clinically followed. High-grade IPMNs undergo resection if the patients’ medical condition allows.
2.5. Category V
The category “suspicious for malignancy” is the second intermediate or indeterminant category aiding in malignancy risk stratification along the spectrum of cytomorphologic features running from clearly benign to clearly malignant. The malignancy risk for the “suspicious” category has been estimated to run from 86 to 100% [3,5,6]. Specimens placed in this category are characterized by the loss of cell polarity resulting in significant architectural disorder (Figure 5). Additionally important for inclusion in the suspicious category are significant nuclear enlargement, nuclear membrane irregularities, presence of a course chromatin pattern, distinct nucleoli, increased nuclear/cytoplasmic ratio (generally 0.6 or greater) and significant anisonucleosis characterized by a three- to four-fold variation in nuclear size within a single cell group. The criteria given in the original Papanicolaou Society of Cytopathology System for Reporting Pancreaticobiliary Cytology did not give quantitative information for the assessment of these criteria. Changes should be significant but fall below those necessary for a definitive diagnosis of malignancy.
Management of patients whose cytologic specimens have been assigned to the “suspicious for malignancy” category requires correlation of clinical, imaging and cytologic data before therapeutic decisions are made. Multidisciplinary patient management conferences are the optimal place for such correlations to be made. It is important to remember that a cytologic diagnosis of “suspicious for malignancy” should never by itself be used to initiate surgical resection. When combined with clinical and imaging findings consistent with a malignancy, a “suspicious” diagnosis can aid in the decision for surgical resection. Additionally, ancillary studies including SMAD4 levels by immunohistochemical staining can support operative intervention when lost.
2.6. Category VI
Assignment to the “positive for malignancy” category is appropriate when the cytologic findings are definitive for a diagnosis. The malignancy risk for this category has varied between 94 and 100% [3,5,6]. Assignment to this category requires substantial architectural and cellular dysmorphology. Pancreatic ductal adenocarcinoma is the most common malignancy within this group (Figure 6). Pancreatic ductal adenocarcinomas show variable degrees of differentiation. While a number of criteria have been proposed, these have generally been qualitative rather than quantitative. Well-differentiated pancreatic ductal adenocarcinomas are difficult to diagnose and many will be assigned to the “suspicious for malignancy” category. Moderately and poorly differentiated pancreatic ductal adenocarcinomas are more clearly malignant and are characterized by three-dimensional tissue fragments with marked loss of nuclear polarity, nuclear overlapping and nuclear molding. The nuclei demonstrate significant nuclear membrane irregularities, nuclear hyperchromasia and an elevated nuclear-to-cytoplasmic ratio of 0.6 or greater. Poorly differentiated adenocarcinomas are characterized by extreme nuclear pleomorphism and a total lack of glandular differentiation. Many single cells with malignant characteristics are seen in the background. The nuclear/cytoplasmic ratio is high (usually 0.7 or greater). The nuclei have a very dark, coarse chromatin pattern, and macronucleoli are common. Importantly, a component of the malignant cells will be bizarre nuclei with irregular shapes. Anaplastic multinucleated cells may be seen. Mitotic figures and background necrosis characterize poorly differentiated ductal adenocarcinomas. Other malignancies placed in category VI include acinic cell carcinomas, lymphomas and metastatic adenocarcinomas. Small-cell neuroendocrine carcinomas are appropriately placed in the malignant category. With the possible exception of lymphomas, surgical resection is the treatment of choice. When a metastatic malignancy is considered, an immunohistochemical workup that includes differential keratins and neuroendocrine markers is appropriate.
3. Summary
Subsequent to the publication of the Papanicolaou Society of Cytopathology System for Reporting Pancreaticobiliary Cytology, modifications have been incorporated in the proposed World Health Organization recommendations for categorization of pancreatic neoplasms. Well- and moderately differentiated neuroendocrine tumors have been reassigned to the malignant category and their grading is based on mitotic count and Ki-67 proliferation index. An update to the Papanicolaou System and future categorization schemes will probably place all neuroendocrine tumors into the malignant category. This will affect the malignancy risk in the “neoplasm, other” category, and undoubtedly management recommendations. Nonetheless, the “neoplasm, other” category remains an important classification for a number of neoplasms, including intraductal papillary mucinous neoplasm, mucinous cystic neoplasm and solid pseudo-papillary neoplasm. Recommendations for refinement of diagnostic criteria for the “atypical”, “suspicious for malignancy” and “malignant” categories will undoubtedly be proffered and may include more quantitative criteria than used in the current system.
Author Contributions
The author conceptualized and wrote the entire manuscript. He was the sole reviewer and editor. The author have read and agreed to the published version of the manuscript.
Funding
No funding was associated with this manuscript.
Institutional Review Board Statement
This manuscript is IRB exempt.
Informed Consent Statement
This a review and no new data is present.
Conflicts of Interest
The author declares no conflict of interest.
References
- Pitman, M.B.; Centeno, B.A.; Ali, S.Z.; Genevay, M.; Stelow, E.; Mino-Kenudson, M. Standardized terminology and nomenclature for pancreaticobiliary cytology The Papanicolaou Society of Cytopathology Guidelines. Diagn. Cytopathol. 2014, 42, 338–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pitman, M.B.; Layfield, L.J. The Papanicolaou Society of Cytopathology System for Reporting Pancreaticobiliary Cytology; Springer: Berlin/Heidelberg, Germany, 2015. [Google Scholar] [CrossRef]
- Sung, S.; Del Portillo, A.; Gonds, T.A.; Kluger, M.; Tiscornia-Wasserman, P.G. Update on risk stratification in the Papanicolaou Society of Cytopathology System for Reporting Pancreaticobiliary Cytology categories: 3-year, prospective, single-institution experience. Cancer Cytopathol. 2020, 128, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Wright, P.K.; Shelton, D.A.; Holbrook, M.R.; Thiryayi, S.A.; Narine, N.; Slater, D.; Rana, D.N. Outcomes of endoscopic ultrasound-guided pancreatic FNAC diagnosis for solid and cystic lesions at Manchester Royal Infirmary based upon the Papanicolaou Society of Cytopathology pancreaticobiliary terminology classification scheme. Cytopathology 2018, 29, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Layfield, L.J.; Dodd, L.; Factor, R.; Schmidt, R.L. Malignancy risk associated with diagnostic categories defined by the Papanicolaou Society of Cytopathology pancreaticobiliary guidelines. Cancer Cytopathol. 2014, 122, 420–427. [Google Scholar] [CrossRef] [PubMed]
- Hoda, R.S.; Finer, E.B.; Arpin, R.N., III; Rosenbaum, M.; Pitman, M.B. Risk of malignancy in the categories of the Papanicolaou Society of Cytopathology system for reporting pancreaticobiliary cytology. Jam Soc. Cytopathol. 2019, 8, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Brugge, W.R.; Lewandrowski, K.; Lee-Lewandrowski, E.; Centeno, B.A.; Szydlo, T.; Regan, S. Diagnosis of pancreatic cystic neoplasms: A report of the cooperative pancreatic cyst study. Gastroenterology 2004, 40, 1024–1028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cizginer, S.; Turner, B.; Bilge, A.B.; Karaca, C.; Pitman, M.B.; Brugge, W.R. Cyst fluid carcinoembryonic antigen is an accurate diagnostic marker of pancreatic mucinous cysts. Pancreas 2011, 40, 1024–1028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nikiforova, M.N.; Khalid, A.; Fasanella, K.; McGrath, K.M.; Brand, R.; Chennat, J.S.; Slivka, A.; Zeh, H.J.; Zureikat, A.H.; Krasinskas, A.M.; et al. Integration of KRAS testing in the diagnosis of pancreatic cystic lesions: A clinical experience of 618 pancreatic cysts. Mod. Pathol. 2013, 26, 1478–1487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, J.; Matthaei, H.; Maitra, A.; Dal Molin, M.; Wood, L.D.; Eshleman, J.R. Recurrent GNAS mutations define an unexpected pathway for pancreatic cyst development. Sci. Transl. Med. 2011, 3, 92ra66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Figure 1.
Smear preparation characterized by crush artifact and debris-obscuring cellular detail to a degree that no diagnosis can be made (Diff–Quik stain).
Figure 1.
Smear preparation characterized by crush artifact and debris-obscuring cellular detail to a degree that no diagnosis can be made (Diff–Quik stain).

Figure 2.
Smear specimen obtained from a pseudocyst. Smear is characterized by a dirty background, scattered chronic inflammatory cells and aggregates of golden-brown pigment. Epithelial cells are absent (Diff–Quik stain).
Figure 2.
Smear specimen obtained from a pseudocyst. Smear is characterized by a dirty background, scattered chronic inflammatory cells and aggregates of golden-brown pigment. Epithelial cells are absent (Diff–Quik stain).

Figure 3.
Sheet of ductal epithelial cells showing some loss of polarity and nuclear crowding consistent with an atypical designation (Diff Quik).
Figure 3.
Sheet of ductal epithelial cells showing some loss of polarity and nuclear crowding consistent with an atypical designation (Diff Quik).

Figure 4.
Papillary fragment of tissue composed of tall mucin-producing columnar cells containing bland nuclei polarized to the base of the cells. These features are characteristic of an intraductal papillary mucinous neoplasm (“Neoplasm, other”), (Diff–Quik stain).
Figure 4.
Papillary fragment of tissue composed of tall mucin-producing columnar cells containing bland nuclei polarized to the base of the cells. These features are characteristic of an intraductal papillary mucinous neoplasm (“Neoplasm, other”), (Diff–Quik stain).

Figure 5.
Cell group from a specimen categorized as suspicious for malignancy. Individual cells demonstrate nuclear enlargement with some nuclear crowding is not marked, the nuclear/cytoplasmic ratio remains below 0.6 and there is only moderate anisonucleosis. This material is best classified as suspicious for malignancy (Diff–Quik stain).
Figure 5.
Cell group from a specimen categorized as suspicious for malignancy. Individual cells demonstrate nuclear enlargement with some nuclear crowding is not marked, the nuclear/cytoplasmic ratio remains below 0.6 and there is only moderate anisonucleosis. This material is best classified as suspicious for malignancy (Diff–Quik stain).

Figure 6.
Smear specimen of a ductal adenocarcinoma. The cell group shows significant nuclear crowding, nuclear molding, and marked anisonucleosis. The nuclear/cytoplasmic ratio is greater than 0.7 in the majority of cells. A group of benign ductal cells is in the lower-right corner for comparison (Diff–Quik stain).
Figure 6.
Smear specimen of a ductal adenocarcinoma. The cell group shows significant nuclear crowding, nuclear molding, and marked anisonucleosis. The nuclear/cytoplasmic ratio is greater than 0.7 in the majority of cells. A group of benign ductal cells is in the lower-right corner for comparison (Diff–Quik stain).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Papanicolaou Society of Cytopathology Categories and Associated Malignancy Risks for Pulmonary Specimens.
Table 1.
Papanicolaou Society of Cytopathology Categories and Associated Malignancy Risks for Pulmonary Specimens.
| Category | Malignancy Risk | ||
|---|---|---|---|
| All Categories + | FNA | Sputum | |
| Non-Diagnostic | 50 to 64% | 0 to 40% | Up to 100% |
| Negative (Benign) | 40 to 45% | 6 to 25% | 40% |
| Atypical | 50 to 60% | 45 to 54% | 50% |
| Neoplasm | unknown * | unknown * | unknown * |
| Suspicious for Malignancy | 90% | 75 to 84% | 90% |
| Malignant | 90% | 86 to 100% | 90% |
* Insufficient data to calculate malignancy risk; + Includes average of malignancy risks for FNA, sputum, bronchial wash, and bronchial brush specimens.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Layfield, L.J. The Papanicolaou Society of Cytopathology System for Reporting Pancreaticobiliary Cytology: A Retrospective Review. J. Mol. Pathol. 2021, 2, 101-108. https://0-doi-org.brum.beds.ac.uk/10.3390/jmp2020010
AMA Style
Layfield LJ. The Papanicolaou Society of Cytopathology System for Reporting Pancreaticobiliary Cytology: A Retrospective Review. Journal of Molecular Pathology. 2021; 2(2):101-108. https://0-doi-org.brum.beds.ac.uk/10.3390/jmp2020010
Chicago/Turabian StyleLayfield, Lester J. 2021. "The Papanicolaou Society of Cytopathology System for Reporting Pancreaticobiliary Cytology: A Retrospective Review" Journal of Molecular Pathology 2, no. 2: 101-108. https://0-doi-org.brum.beds.ac.uk/10.3390/jmp2020010