
Mental Health Literacy and Dementia

1
Research Department of Clinical, Educational and Health Psychology, University College London, London WC1E 6BT, UK
2
Norwegian Business School (BI), 0484 Oslo, Norway
*
Author to whom correspondence should be addressed.
Psychiatry Int. 2021, 2(2), 159-168; https://0-doi-org.brum.beds.ac.uk/10.3390/psychiatryint2020012
Submission received: 22 March 2021
/
Revised: 22 April 2021
/
Accepted: 24 April 2021
/
Published: 1 May 2021
Abstract
:This study aimed to investigate mental health literacy (MHL) with respect to dementia. Three forms of dementia were investigated. In all, 167 participants completed an online questionnaire which consisted of five vignettes that described the three dementia conditions, as well as depression and typical ageing. The vignette characters had no age specified, or they were described as 50-years-old or 70-years-old. Participants had to firstly decide if there was a disorder present and identify it by name, then answer questions relating to treatment and help-seeking. Results showed that participants could identify Alzheimer’s Disease significantly more so than they could vascular or frontotemporal dementia. All three dementias were significantly more recognised when the vignette was described as a 70-year-old. Frontotemporal dementia was significantly misdiagnosed as depression. Participant education and mental health experience did not influence the identification of dementia. Compared to some other well-known mental illnesses like schizophrenia, lay people are relatively good at recognising Alzheimer’s disease, but much less so at other forms of dementia. Implications and limitations of the study are discussed.
1. Introduction
This is a mental health literacy study concerning lay people’s ability to differentiate between different types of dementia, as well as clinical depression and normal aging. There is now emerging literature on dementia literacy [1,2] across many countries and continents [3,4,5] with many studies concentrating on the lay public’s attitudes to, and knowledge of, dementia [6,7].
This is an important issue for many reasons. Health educators are interested in how soon individuals correctly identify early signs of dementia in themselves and others. Next, there are questions about their misconceptions and general ignorance about dementia and related conditions. Third, there is the question about individual differences in dementia mental health literacy (MHL) which may help educators target those most in need to understand the condition.
From a theoretical point of view, MHL studies reveal lay understandings of mental and general physical health. They show how and where their understanding is different from professionals as well as how and why it differs from culture to culture [8]. It also gives an insight into what is called transitional psychiatry and the aging process [9,10,11].
Whilst there are a number of health literacy studies in this area [12], there have been far fewer mental health studies. Surprisingly, perhaps some studies have indicated that people have better physical than mental health literacy [13]. That is, they seem to recognise, label and understand some relatively common physical health conditions better than equally common mental health conditions. It is, however, recognised that the two are linked. That is, that some people are more generally health literate than others.
This is a MHL study concerning the identification of dementia. There are few others in this area; an exception being a study by Wijeratne and Harris [14], who administered a questionnaire based on clinical vignettes describing older people with depression, dementia and coronary heart disease. They found a high rate of recognition of all disorders amongst the sample of Australian GPs. They concluded that there is a need to improve the knowledge of GPs with regard to screening and investigating late life depression and managing dementia. However, one would expect medical doctors to be well informed about dementia compared to members of the general public
MHL is concerned with the general public’s understanding and beliefs of mental health [15]. In MHL studies, the typical methodology requires participants to read a vignette which describes a person possessing the well-known medical or psychological symptoms of a certain mental health disorder [16] and then make various judgements about the individual.
MHL has been successful in highlighting inaccuracy in the lay theories of a variety of mental health disorders, including borderline personality disorder (BPD) [17]. Recent studies have looked at conditions such as autism spectrum disorder [18]. Two factors that appear to have an impact are personal mental health experience and education. Better educated people (in general) and those who have personal experience of specific mental illnesses (particularly depression) have greater MHL.
Wickstead and Furnham [13] have argued that the differences in lay theories may be affected by prevalence rates. They showed that high prevalence disorders, such as depression, were identified much more (89.9%) than low prevalence disorders, such as obsessive–compulsive personality disorder (OCPD) (3.4%) [19].
1.1. Dementia
In the UK, there are around 850,000 people living with dementia [20]. With an ageing population, this number appears to be increasing. By 2025, it is expected to rise to over one million [21]. Furthermore, the Department of Health estimates that 59% of people with dementia in England have a formal diagnosis [22].
One of the most common forms of dementia is Alzheimer’s disease (AD). AD is characterized by an impairment in memory, confusion, disorientation and personality changes. It accounts for approximately 62% of cases of dementia in the UK. With a high prevalence rate, one would assume that it shall be often identified correctly. Bowers, Jorm, Henderson and Harris [23] found that GPs were better at identifying and diagnosing AD than depression. It was shown, however, that if a patient mentioned negative emotions, a misdiagnosis was often made of depression. Thus, if professionals can make this error in diagnosis, it may be even more common in the general public.
Werner [24] found that the laypersons’ knowledge of AD symptoms was fair, with over 60% of the participants correctly identifying a variety of warning signs: disorientation, problems with language and changes in mood or behaviour. They may be even poorer in those forms of dementia that have a lower prevalence rate than AD, such as frontotemporal dementia (2%) and vascular dementia (17%). One Australian telephone study using two interchangeable vignettes of people aged 75 years found 82% of the people could identify patients correctly as demented or AD. Around three quarters thought the risk of dementia could be reduced by exercise, diet and social contacts.
Age also appears to be a factor in the identification of dementia. Dementia can occur at an early onset (from 45-years-old) or at a late onset (from 65-years-old). In the UK, over 40,000 people under 65 have dementia [20]. Werner and Davidson [25] have shown, however, that when a vignette is presented with the omission of the age of the person, only one third of the sample could correctly identify AD. It appears that symptoms alone may not be enough for people to identify dementia, and contextual factors may be important in the decision-making process. Other forms which are characterized by an earlier onset, such as frontotemporal dementia, may be less likely to be identified due to the age factor as opposed to the symptoms present.
1.2. Current Study
The current study aimed to investigate the lay theories of three different forms of dementia; AD, frontotemporal and vascular dementia. These were chosen because they are some of the most common forms of dementia that appear in the DSM-5. It will also investigate whether emotional cues will influence the misdiagnosis of dementia to depression similar to that made by GP’s.
Five hypotheses were formulated for investigation based on the previous literature. H1: AD will be correctly identified significantly more than vascular or frontotemporal dementia. H2: The three forms of dementia will be correctly identified significantly more in a vignette of a 70-year-old than a 50-year-old or a person where age is omitted. H3: Those with mental health experience and a higher educational background will correctly identify the disorders significantly more than someone with no prior mental health or less education experience. H4: There will be significant misdiagnoses of AD and frontotemporal dementia as clinical depression. H5: The six knowledge-based questions will be answered more accurately in the AD rather than the vascular or frontotemporal dementia conditions.
2. Method
2.1. Participants
In total, 167 participants took part using Amazon Mechanical Turk (male (n = 69: 41.3%) and female (n = 98: 58.7%)). The age range was 18 to 69 years (M = 34, S.D = 12.63). The majority of participants were White British (83.2%, n = 139). The remaining participants were of Asian (9.0%, n = 15), Black African-Caribbean (3%, n = 5) or other British nationality (4.8%, n = 8). Majority of participants held an undergraduate degree (43.7%, n = 73). The lowest education level held was GCSE/10th grade (12.6%, n = 21) followed by A-Level/12th grade (21%, n = 35). The highest level of education held was a postgraduate degree (22.8%, n = 38). The majority of participants noted that they had not previously suffered from any mental health condition (73.1%, n = 122). Of the 45 participants who stated they had suffered from a mental health condition, the most common were depression (68.9%, n = 31) and anxiety (48.9%, n = 22). No participants mentioned being diagnosed with any form of dementia. The majority of participants, however, knew of another person who had suffered from a mental health condition (60%, n = 100), of which, 32% had known of someone who had suffered from a form of dementia and 43% had known of someone who had suffered from depression.
2.2. Vignettes
The questionnaire consisted of five vignettes (obtainable from the first author). These vignettes described frontotemporal dementia, vascular dementia, AD, depression and typical ageing. They were created using the diagnostic criteria within the DSM-5 [26]. The three critical vignettes (AD, frontotemporal and vascular dementia) were compared to typical ageing to highlight if participants could distinguish between a clinical condition and natural ageing. A vignette describing depression was included to test the external reliability that the lay person could identify depression well [13] and that it could be identified better with greater education and mental health experience [21]. The vignettes were standardized both in length and content, similar to the vignettes used in other MHL studies [18,19]. The vignette’s word length ranged from 85 to 93 words and were, on average, 90 words long. Each vignette stated that no medication had been taken by the character.
The person described had a non-gender specific name to try not to draw attention to gender as a potentially confounding factor. The age of the person in the vignette was varied to be either 50 or 70-years-old or no age was specified. These two ages were specifically chosen as they were five years older than the minimum age to be categorized as early onset (45-years-old) and late onset (65-years-old). Five years above the minimum age of onset was used as this removed the ambiguity as to whether it could be classified as early or late onset dementia. The five vignettes were show in a random order to each participant.
After each vignette, a series of six questions were included from Furnham et al. [19]. The questions were used to measure the layperson’s knowledge of the disorders presented. The first question was close-ended and asked participants “Do you believe x has a mental health condition?” Only a ‘yes’ or ‘no’ answer could be made to this question. If the answer ‘yes’ was selected, then participants were asked to complete the remaining five questions. Participants who believed there was a condition present were then asked what condition they believed the vignette character displayed. This was an open-ended question with a free-text response.
The remaining four questions provided a five-point Likert scale to respond on. For questions three and four, this scale ranged from 1 (extremely easy) to 5 (extremely difficult); for question five, 1 (definitely yes) to 5 (definitely not); and six, 1 (extremely unlikely) to 5 (extremely likely). A five-point scale was used as this was shown to be an optimum number of options without providing too little or too many options [27]. These questions related to ease of identifying, ease of treating and help-seeking behaviour.
2.3. Procedure
This study received approval from the appropriate ethics committee: CEHP/514/2017. The study took participants 15 min to complete on average, and they were paid £1.50 for their participation. They agreed to their unanimous results being analysed and published.
3. Results
Data was first inspected and cleaned. Our first question was concerned with the extent to which participants were accurate in identifying all the conditions described, as well as the individual differences correlated to those scores.
Pearson’s correlations were computed looking at the participant’s ability to identify the disorders in the five vignettes correctly and the demographics, which are included in Table 1. There was a positive relationship between age and the ability to correctly identify frontotemporal and vascular dementia. Typical ageing correlated negatively with vascular dementia and AD. There was a significant positive relationship between the ability to identify AD and depression.
3.1. Vignette Identification Task Analysis
All five vignettes were coded in a dichotomous fashion, either correct or incorrect. For the dementia vignettes, they could be deemed correct if the specific form of dementia or dementia in general were mentioned. If another form of dementia was chosen, this would be deemed as incorrect because different forms of dementia have varying symptoms. Furthermore, if only a symptom such as “memory loss” was provided, this would not be deemed correct as it can only be a symptom and not a disorder in itself. For the depression condition, only depression or its variations, such as bipolar or mania, would be accepted to be correct. Other answers, such as “sad” or “lack of interest”, were not accepted as they are not a classified disorder, but only symptoms of a variety of disorders. In the event of two or more answers being provided simultaneously for a single vignette, if the correct disorder was included, then this was deemed a correct response. A reliability analysis was conducted using a second-rater. They coded 10% of the questionnaires (n = 16) using the same coding framework as the lead researcher. These results were highly reliable, indicating high inter-rater reliability (Kappa = 0.875).
Regardless of if the correct condition was identified, 71.9% believed there to be something wrong with the AD vignette, 65.3% of participants believed there to be something wrong in the frontotemporal vignette, and 58.1% believed there was something wrong in the vascular dementia vignette.
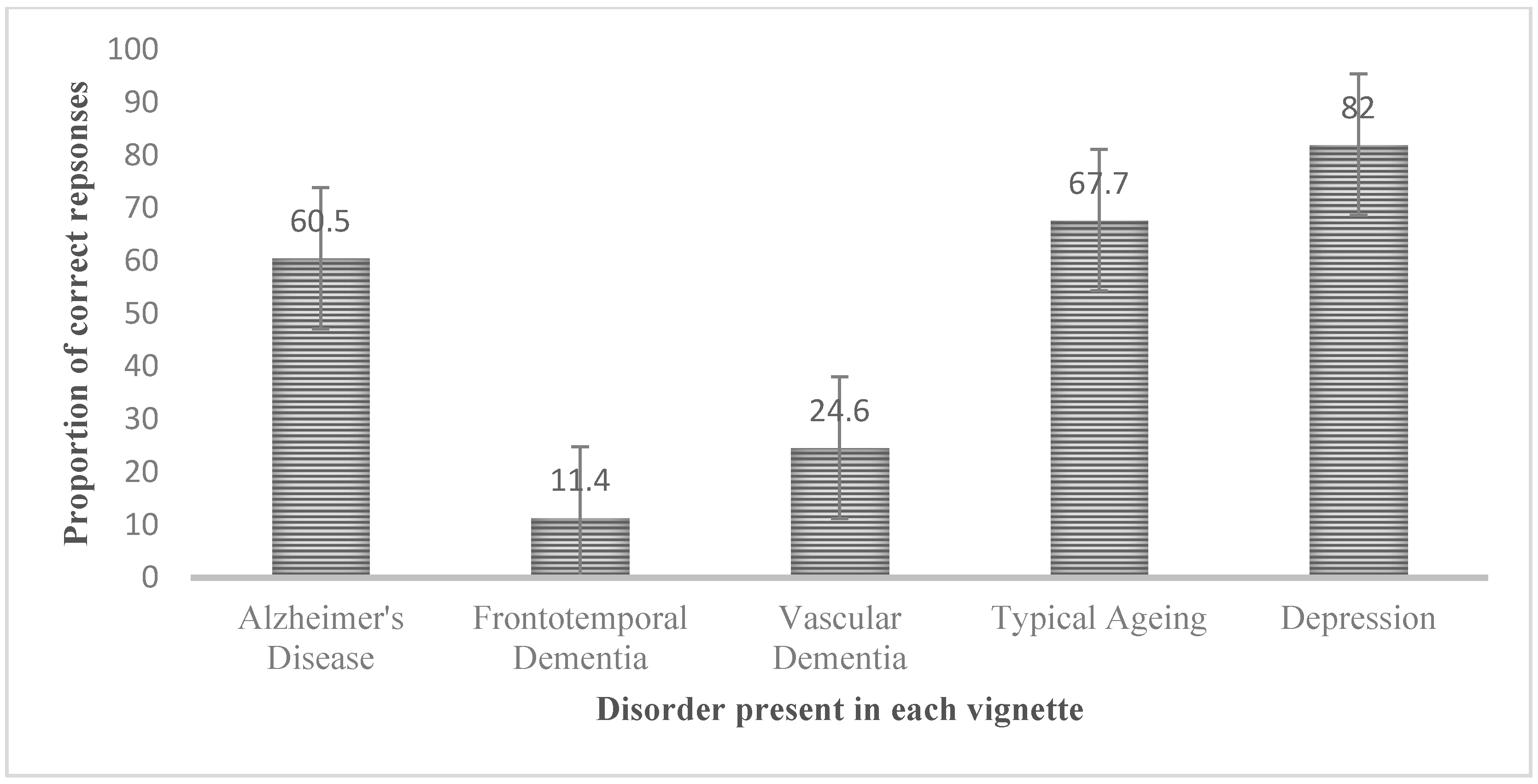
When only looking at the correct identifications, 82.2% of participants correctly identified a vignette’s disorder. AD was correctly identified by 60.5% of participants, frontotemporal by 11.4%, vascular by 24.6% of participants, depression by 82% and typical ageing by 67.7%. The proportion of correct responses for each condition can be seen in Figure 1.
Various McNemar tests with Bonferroni corrections were then carried out to see which of the three dementia vignettes were significantly different from one another. The only significant difference was between the vascular dementia and AD vignette; (1, N = 167) = 7.224, p = 0.007, showing that AD was identified with something wrong significantly more so than vascular dementia.
When regarding only the correct responses, there were significant differences between the ability to correctly identify the specific types of dementia and typical ageing; Q (3) = 137.909, p < 0.001. When comparing only the three dementia conditions, there were significant differences in the correct identification of the three types; Q (2) = 99.156, p < 0.001. Post-hoc pairwise analyses were conducted using a Bonferroni correction. AD was identified significantly more so than frontotemporal ( (1, N = 167) = 69.798, p < 0.001) and vascular dementia ( (1, N = 167) = 41.440, p < 0.001). Vascular dementia was also identified significantly more so than frontotemporal dementia; (1, N = 167) = 11.025, p = 0.001.
The three forms of dementia were then compared to investigate the proportion of correct identifications in each age condition (see Table 3). Dementia was correctly identified and labelled by 44.1% of participants in the 70-year-old condition, 34.2% in the 50-year-old and 21.7% when there was no age present. It was shown that this was a significant difference; (2, N = 167) = 14.402, p = 0.001. This was then investigated for each form of dementia separately using a Bonferroni correction. Frontotemporal dementia was identified significantly more so in a 70-year-old (22.4%) than in a 50-year-old (10%) or when no age was present (1.9%); (2, N = 167) = 12.151, p = 0.002. There was no significant difference in the identification of AD and of vascular dementia at the different age conditions.
3.2. Misdiagnosis Analysis
From Table 3, it can be seen that frontotemporal dementia was misdiagnosed as depression in 33% of cases, AD in 4% on cases and vascular in 2% of cases. Using a Cochran’s Q test statistic, this was shown to be significantly different; Q (2) = 83.733, p < 0.001. From further analysis, it was shown that frontotemporal dementia was misdiagnosed significantly more so than AD ( (1, N = 167) = 48.167, p < 0.001) and vascular dementia ( (1, N = 167) = 39.446, p < 0.001).
3.3. Knowledge Analysis
The results for questions two and three can be seen in Table 4. Depression was rated easiest for identification and treatment. With regards to dementia, the ratings were significantly different; ease of identification—F (1.887, 313.183) = 18.653, p < 0.001 and ease of treatment—F (1.93, 320.435) = 12.445, p < 0.001. As Mauchley’s test of sphericity was significant for both ease of identification (W (2) = 0.940, (2) = 10.224, p = 0.006) and ease of treatment (W = 0.964, (2) = 6.065, p = 0.048).
To determine which of the three dementia conditions were significantly different from one another for the above conditions, pairwise comparisons were conducted with a Bonferroni correction. AD was considered significantly easier to identify from vascular (t (166) = 6.066, p < 0.001) and frontotemporal dementia (t (166) = 3.244, p = 0.001). Frontotemporal dementia was also considered significantly easier to identify from vascular dementia (t (166) = −2.829, p = 0.005). Frontotemporal dementia was also considered significantly easier to treat than AD (t (166) = −3.969, p < 0.001) and vascular dementia (t (166) = −4.262, p < 0.001).
There was a significant difference in the participants consideration for help-seeking (question five) for the three dementia conditions; F (2332) = 4.702, p = 0.010. To determine which of the dementia conditions were significantly different from another, pairwise comparisons with Bonferroni correction were conducted. AD was considered to require help significantly more than vascular dementia (t (166) = 3.002, p = 0.003).
From Table 5, it can be seen that only two sources of help were rated as “likely to seek help from” with regards to the three forms of dementia were friend and GP. These were rated significantly different for the three dementia vignettes: friend—F (2332) = 3.197, p = 0.042 and GP—F (2332) = 4.568, p = 0.011. From pairwise comparisons with a Bonferroni correction, neither of the dementia vignettes were rated significantly different from one another with regards to seeking help from a friend. With regards to seeking help from a GP, the AD character was considered significantly more likely to seek help from a GP than the vascular dementia character (t (166) = −2.899, p = 0.004).
3.4. Demographics Analysis
Mental health experience was placed on an ordinal scale from one (no mental health experience) to four (own experience and experience of others). Education level was similarly placed on an ordinal scale from one (GCSE) to four (postgraduate). A Jonchkeere trend test was firstly used to investigate whether, similarly to the previous literature, higher levels of these two factors would be significant for greater identification of depression. Mental health experience had a significant impact on the identification of depression; TJT = 5249.50, z = 2.071, p = 0.038. That is, depression was identified more by those with greater experience. There was no significant difference in identifying depression from different education levels.
4. Discussions
It is evident that there is poor specific knowledge of dementia, more so in the case of frontotemporal and vascular dementia than that of AD. Frontotemporal and vascular dementia were identified substantially less (11.4% and 24.6% respectively) than AD (60.5%). This supports Werner [27], who found that over 60% of participants could identify AD. However, all three conditions were identified to have exhibited something wrong (even if they were unsure what it was) in more than half of participants. A positive correlation was also evident between the identification of frontotemporal and vascular dementia. This suggests that interventions to improve the former could show an increase in identification of the latter.
Confirming the second hypothesis, the dementia vignettes were identified significantly more in a vignette of a 70-year-old compared to a 50-year-old or a person where age was omitted. However, the only significant difference appeared to be in relation to frontotemporal dementia. Frontotemporal dementia is characterized by early onset. If the lay person is less likely to identify this form of dementia at an early onset compared to a late onset, this could have negative implications of seeking a diagnosis and medical help.
Participants generally had experience with the more common disorders, including depression and anxiety. None of the participants, however, had been personally diagnosed with dementia and only 32% had known someone else to have dementia. Experience may not have had an effect on the identification of dementia because the experience was not relevant to dementia. In the previous literature where experience was significant for identification, participants have often had experience with the disorder in the current study, such as depression,. For example, in a study where depression was identified by 97.2% of participants, it was also the most common mental health disorder one had experience with [18].
A fourth hypothesis predicted that frontotemporal dementia and AD would be misdiagnosed as depression. The results showed that all three forms of dementia were significantly different from one another. With vascular and AD being diagnosed by less than 5% of participants. The results show that only frontotemporal dementia appeared to be significantly misdiagnosed as depression in 32% of incidences. This does not replicate the findings of previous literature with regards to AD, which have shown that GP’s have previously misdiagnosed AD as depression when emotional symptoms were included. However, the current study did not include many emotional symptoms in the AD vignette and there were more obvious emotional symptoms in the frontotemporal vignette. Thus, the effect of emotional symptoms may still result in a poor distinction between depression and dementia.
A further reason for no significant differences in AD misdiagnosis may be due to the timing. The previous literature was conducted on GPs almost twenty years ago. The lay person may now have a better understanding of the symptoms of AD and depression and how they differ in the current study because there is more information readily available than there was when the previous study was conducted. The lay theories of frontotemporal dementia, on the other hand, may not have improved or be as great as that for AD and this is why there was a significant misdiagnosis of depression for this form of dementia. Therefore, the null hypothesis cannot be rejected with regards to AD but can be rejected with regards to frontotemporal dementia.
It was assumed that greater knowledge would be seen for AD as opposed to frontotemporal or vascular dementia (including knowledge of identifying, treating and help-seeking behaviour). The results showed that the AD vignette was easier to identify compared to the other two dementia vignettes. This average, however, was still low. Thus, all three forms of dementia may require information to be made available about their symptoms.
Similarly, ease of treating suggested that participants believed there was difficulty in treating the three forms of dementia. Surprisingly, AD was not rated the easiest to treat out of the three forms. This suggests that participants have a poor understanding of the treatments for dementia, including AD.
With regards to the final hypothesis, help-seeking was greatest for AD, and this was significantly different from vascular dementia. However, all forms of dementia were rated highly for requiring help. A significant difference in the source of help was found for GPs and friends. However, from pairwise comparisons, the friend source did not vary between the three vignettes. GP, on the other hand, was rated as being required significantly more as a source of help for AD than vascular dementia. The GP source had the highest ratings for all three vignettes, with an average rating of three (neither likely nor unlikely). That is, participants believed this was the most likely source of the six, but this was still only rated mid-way on the scale. This is an issue, because dementia requires help first and foremost from a GP to be able to diagnose it and then provide appropriate treatments. The fact that participants acknowledged this for all three conditions most highly is promising, but the average score does not suggest that all would seek help from a GP.
A limitation of the current study and of all MHL studies is the use of the vignette identification task. The vignettes are of fictitious characters, which may have less ecological validity to the identification one may make of a real person exhibiting the same symptoms. The newest research in this area uses video-recordings which are much more realistic. Secondly, it was desirable to have a larger and more diverse population to ensure the reliability of the results. The size of the sample in this was such that this may be described as a pilot study, and replication is important. Thirdly, we were very strict in our classification of correct and incorrect diagnoses which may be less appropriate in areas where technical medical terms are very little known.
5. Conclusions
There are both clinical implications of this research and also suggestions for future studies. With the growing longevity of people, particularly in western countries, it may be expected that there will be a significant rise in the number of people with various types of dementia. Like all conditions, the sooner this is correctly identified the better and there are, in many countries, organisations and societies that help collect research funds and disseminate information about these conditions which helps dementia MHL. This study showed that people might not recognise those with dementia below the age of 70 and confuse symptoms with those of depression. Hence, the need for the education of the public in dementia and related illness remains important.
In many countries, there are voluntary and state-supported organisations which attempt to improve the mental and physical health literacy of the public through various media outlets. They offer simple ways to diagnose acute and chronic medical conditions and give advice about seeking help. What this study showed was that people seem reasonably well informed about and were familiar with the term “Alzheimer’s Disease”, which they believe to be an affliction of old age. Whilst it is much less important for people to always know and use the “correct” medical terminology and subtle differences between disorders with similar manifestations, it is important they recognise symptoms that require expert evaluation and assistance. Thus, like so many MHL studies, this suggests the importance of the education of the general public about the three major disorders examined in this study.
Author Contributions
Conceptualization, H.C. and A.F.; formal analysis, H.C.; data curation, H.C.; writing—original draft preparation, H.C.; writing—review and editing, A.F.; visualization, A.F.; supervision, A.F.; project administration, A.. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethics Permission Code: CEHP/514/2017.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
An SPSS file of the data is available on request from the first author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Loi, S.; Lautenschlager, N. Dementia literacy in older adults. Asia Pac. Psychiatry 2015, 7, 292–297. [Google Scholar] [CrossRef]
- Low, L.; Anstey, K. Dementia literacy: Recognition and beliefs on dementia of the Australian public. Alzheimer’s Dement. 2009, 5, 43–49. [Google Scholar] [CrossRef]
- Leung, A.; Molassiotis, A.; Zhang, M.; Deng, R.; Liu, M.; Van, I.K.; Leong, C.S.U.; Leung, I.S.H.; Leung, D.Y.P.; Lin, X.; et al. Dementia Literacy in the Greater Bay Area, China: Identifying the At-Risk Population and the Preferred Types of Mass Media for Receiving Dementia Information. Int. J. Environ. Res. Public Health 2020, 17, 2511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, W.J.; Hong, S.I.; Luo, N.; Lo, T.J.; Yap, P. The lay public’s understanding and perception of dementia in a developed Asian Nation. Dement. Geriatr. Cogn. Disord. Extra 2012, 2, 433–444. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Loi, S.M.; Zhou, S.; Zhao, M.; Lv, X.; Wang, J.; Wang, X.; Lautenschlager, N.; Yun, X.; Wang, H. Dementia Literacy among Community-Dwelling Older Adults in Urban China. Front. Public Health 2017, 5, 124–130. [Google Scholar] [CrossRef] [Green Version]
- Cahill, S.; Pierce, M.; Werner, P.; Darley, A.; Bobersky, A. A systematic review of the public’s knowledge and understanding of Alzheimer’s disease and dementia. Alzheimer Dis. Assoc. Disord. 2015, 29, 255–275. [Google Scholar] [CrossRef] [PubMed]
- Schelp, A.O.; Nieri, A.B.; Filho, P.; Bales, A.M.; Mendes-Chiloff, S. Public awareness of dementia: A study in Botucatu, a medium-sized city in the State of São Paulo, Brazil. Dement. Neuropsychol. 2008, 2, 192–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furnham, A.; Hamid, A. Mental health literacy in non-western countries: A review. Ment. Health Rev. 2014, 19, 84–98. [Google Scholar] [CrossRef]
- De Berardis, D.; De Filippis, S.; Masi, G.; Vicari, S.; Zuddas, A. A Neurodevelopment Approach for a Transitional Model of Early Onset Schizophrenia. Brain Sci. 2021, 11, 275. [Google Scholar] [CrossRef]
- Marchetti, D.; Musso, P.; Verrocchio, M.C.; Manna, G.; Kopala-Sibley, D.C.; De Berardis, D.; De Santis, S.; Falgares, G. Childhood maltreatment, personality vulnerability profiles, and borderline personality disorder symptoms in adolescents. Dev. Psychopathol. 2021, 26, 1–14. [Google Scholar] [CrossRef]
- Ullah, I.; Razzaq, A.; De Berardis, D.; Ori, D.; Adiukwu, F.; Shoib, S. Mental health problems in children & pandemic: Dangers lurking around the Corner and possible management. Int. J. Soc. Psychiatry 2021, 7, 20764021992816. [Google Scholar] [CrossRef]
- Rostamzadeh, A.; Stapels, J.; Genske, A.; Haidl, T.; Junger, S.; Seves, M.; Woopen, C.; Jessen, F. Health Literacy in individuals at risk for Alzheimer’s Dementia: A Systematic Review. J. Prev. Alzheimer’s Dis. 2020, 7, 47–55. [Google Scholar] [CrossRef]
- Wickstead, P.; Furnham, A. Comparing Mental Health Literacy and Physical Health Literacy: An Exploratory Study. J. Ment. Health 2017, 26, 449–456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wijeratne, C.; Harris, P. Late life depression and dementia: A mental health literacy survey of Australian general practitioners. Int. Psychogeriatr. 2009, 21, 330–337. [Google Scholar] [CrossRef] [PubMed]
- Jorm, A.F.; Korten, A.E.; Jacomb, P.A.; Christensen, H.; Rodgers, B.; Pollitt, P. Mental health literacy: A survey of the public’s ability to recognise mental disorders and their beliefs about the effectiveness of treatment. Med. J. Aust. 1997, 166, 182–186. [Google Scholar] [CrossRef] [PubMed]
- Sai, G.; Furnham, A. Identifying depression and schizophrenia using vignettes: A methodological note. Psychiatry Res. 2013, 210, 357–362. [Google Scholar] [CrossRef]
- Furnham, A.; Lee, V.; Kolzeev, V. Mental health literacy and borderline personality disorder (BPD): What do the public “make” of those with BPD? Soc. Psychiatry Psychiatr. Epidemiol. 2015, 50, 317–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Godfrey Born, C.; McClelland, A.; Furnham, A. Mental health literacy for autism spectrum disorder and depression. Psychiatry Res. 2019, 279, 272–277. [Google Scholar] [CrossRef]
- Furnham, A.; Swami, V. Mental health literacy: A review of what it is and why it matters. Int. Perspect. Psychol. 2018, 7, 240–257. [Google Scholar] [CrossRef]
- Alzheimer’s Society. Dementia 2014: Opportunity for Change; Alzheimer’s Society: London, UK, 2014. [Google Scholar]
- Lewis, F.; Karlsberg Schaffer, S.; Sussex, J.; O’Neill, P.; Cockcroft, L. The Trajectory of Dementia in the UK—Making a Difference; Office of Health Economics: London, UK, 2014. [Google Scholar]
- Prince, M.J.; Wimo, A.; Guerchet, M.M.; Ali, G.C.; Wu, Y.T.; Prina, M. World Alzheimer’s Report 2015—The Global Impact of Dementia; Alzheimer’s Disease International (ADI): London, UK, 2015. [Google Scholar]
- Bowers, J.; Jorm, A.F.; Henderson, S.; Harris, P. General practitioners’ detection of depression and dementia in elderly patients. Med. J. Aust. 1990, 153, 192–196. [Google Scholar] [CrossRef]
- Werner, P. Knowledge about symptoms of Alzheimer’s disease: Correlates and relationship to help-seeking behaviour. Int. J. Geriatr. Psychiatry 2003, 18, 1029–1036. [Google Scholar] [CrossRef] [PubMed]
- Werner, P.; Davidson, M. Emotional reactions of lay persons to someone with Alzheimer’s disease. Int. J. Geriatr. Psychiatry 2004, 19, 391–397. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; APA: Washington, DC, USA, 2015. [Google Scholar]
- Lozano, L.M.; García-Cueto, E.; Muñiz, J. Effect of the number of response categories on the reliability and validity of rating scales. Methodology 2008, 4, 73–79. [Google Scholar] [CrossRef]
Figure 1.
The percentage of correct responses to the five vignettes (error bars show standard error).
Figure 1.
The percentage of correct responses to the five vignettes (error bars show standard error).


{kind=link}
Table 1.
A correlation matrix of the identification of the five vignettes and demographics of the participants.
Table 1.
A correlation matrix of the identification of the five vignettes and demographics of the participants.
| Gender | Age | Education | Mental Health Experience | Fronto Temperal Dementia | Vascular Dementia | Alz Dis | Typical Ageing | Depression | |
|---|---|---|---|---|---|---|---|---|---|
| Gender | −0.052 | 0.033 | 0.027 | 0.043 | 0.151 | 0.319 ** | |||
| Age | −0.052 | 0.086 | 0.081 | 0.076 | −0.042 | 0.185 * | 0.059 | ||
| Education | −0.153 * | 0.009 | −0.051 | 0.047 | −0.122 | −0.020 | |||
| MH Exp | −0.007 | −0.028 | −0.087 | 0.059 | 0.141 | ||||
| FT Dement | 0.234 ** | 0.058 | −0.025 | 0.026 | |||||
| Vas Dem | 0.120 | −0.214 ** | 0.093 | ||||||
| Alzheimer | −0.185 * | 0.181 * | |||||||
| Typ Ageing | −0.013 |
* p < 0.05, ** p < 0.001, Positive correlations with gender indicate that female participants identified conditions more; positive correlations with experience indicates that those with previous experience with mental health identified conditions more; positive correlations with education indicates that those who have a higher level of education identified conditions more. We coded the answers to each vignette which is shown in Table 2.
Table 2.
Responses to each vignette.
| Frontotemporal Dementia | Vascular Dementia | Alzheimer’s Disease | Depression | Typical Ageing | |
|---|---|---|---|---|---|
| Dementia (general term) | 19 | 40 | 60 | 2 | 27 |
| Frontotemporal Dementia | |||||
| Vascular Dementia | 1 | ||||
| Alzheimer’s Disease | 11 | 11 | 41 | 1 | 19 |
| Depression | 55 | 7 | 3 | 137 | 2 |
| Stress related (i.e., stress, anxiety and trauma) | 7 | 4 | 2 | 1 | 1 |
| Physical illness (i.e., cancer, stroke) | 2 | 3 | 1 | ||
| Mood deficit | 1 | ||||
| Attention deficit | 7 | ||||
| Autism | 1 | ||||
| Memory loss | 4 | 3 | |||
| Typical ageing | 113 | ||||
| Not sure | 16 | 21 | 9 | 2 | 3 |
Table 3.
Proportion of correct responses to the vignettes.
| Condition | No Age | 50-Year-Old | 70-Year-Old |
|---|---|---|---|
| Frontotemporal Dementia | 1 | 5 | 13 |
| Vascular Dementia | 7 | 14 | 20 |
| Alzheimer’s Disease | 27 | 36 | 38 |
| Depression | 50 | 42 | 45 |
| Typical Ageing | 37 | 31 | 45 |
Table 4.
Ratings from 1 to 5 given to questions on the ease of identifying and treating (Mean and SD).
Table 4.
Ratings from 1 to 5 given to questions on the ease of identifying and treating (Mean and SD).
| Condition | Ease of Identifying | Ease of Treatment |
|---|---|---|
| Frontotemporal dementia | 3.78 (1.23) | 4.05 (1.01) |
| Alzheimer’s Disease | 3.34 (1.41) | 4.38 (0.76) |
| Vascular dementia | 4.10 (1.15) | 4.43 (0.76) |
| Depression | 2.54 (1.37) | 3.29 (1.13) |
| Typical Ageing | 4.28 (1.17) | 4.59 (0.81) |
Ratings were averaged over the three age conditions for each disorder; mean in bold was lower than half of the rating scale (less than 3).
Table 5.
Rating of the six help-seeking platforms for the five conditions (mean and SD).
| Condition | Mean Likelihood of Suggesting Help | No One | Internet | Friend | Family | GP | Psychologist/Psychiatrist |
|---|---|---|---|---|---|---|---|
| Frontotemporal | 2.75 (1.74) | 1.36 (0.86) | 1.87 (1.18) | 2.62 (1.50) | 2.80 (1.61) | 3.34 (1.84) | 2.75 (1.65) |
| Vascular | 2.90 (1.86) | 1.22 (0.70) | 1.64 (1.03) | 2.38 (1.54) | 2.66 (1.63) | 3.20 (1.92) | 2.53 (1.63) |
| Alzheimer’s Disease | 2.37 (1.72) | 1.29 (0.80) | 1.18 (1.18) | 2.71 (1.56) | 3.01 (1.65) | 3.75 (1.77) | 2.87 (1.60) |
| Depression | 1.29 (0.55) | 1.35 (0.86) | 2.29 (1.28) | 3.35 (1.34) | 3.58 (1.41) | 4.12 (1.50) | 3.66 (1.50) |
| Typical Ageing | 1.28 (.618) | 1.28 (0.72) | 1.55 (1.06) | 1.81 (1.29) | 1.96 (1.44) | 2.29 (1.80) | 1.84 (1.35) |
Ratings were averaged over the three age conditions for each disorder; means in bold were greater than half of the rating scale (over 3).
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Carr, H.; Furnham, A. Mental Health Literacy and Dementia. Psychiatry Int. 2021, 2, 159-168. https://0-doi-org.brum.beds.ac.uk/10.3390/psychiatryint2020012
AMA Style
Carr H, Furnham A. Mental Health Literacy and Dementia. Psychiatry International. 2021; 2(2):159-168. https://0-doi-org.brum.beds.ac.uk/10.3390/psychiatryint2020012
Chicago/Turabian StyleCarr, Hannah, and Adrian Furnham. 2021. "Mental Health Literacy and Dementia" Psychiatry International 2, no. 2: 159-168. https://0-doi-org.brum.beds.ac.uk/10.3390/psychiatryint2020012