
Dosimetric Parameters Predicting Tooth Loss after Carbon Ion Radiotherapy for Head and Neck Tumors

 , , , , , and
, , , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. CIRT
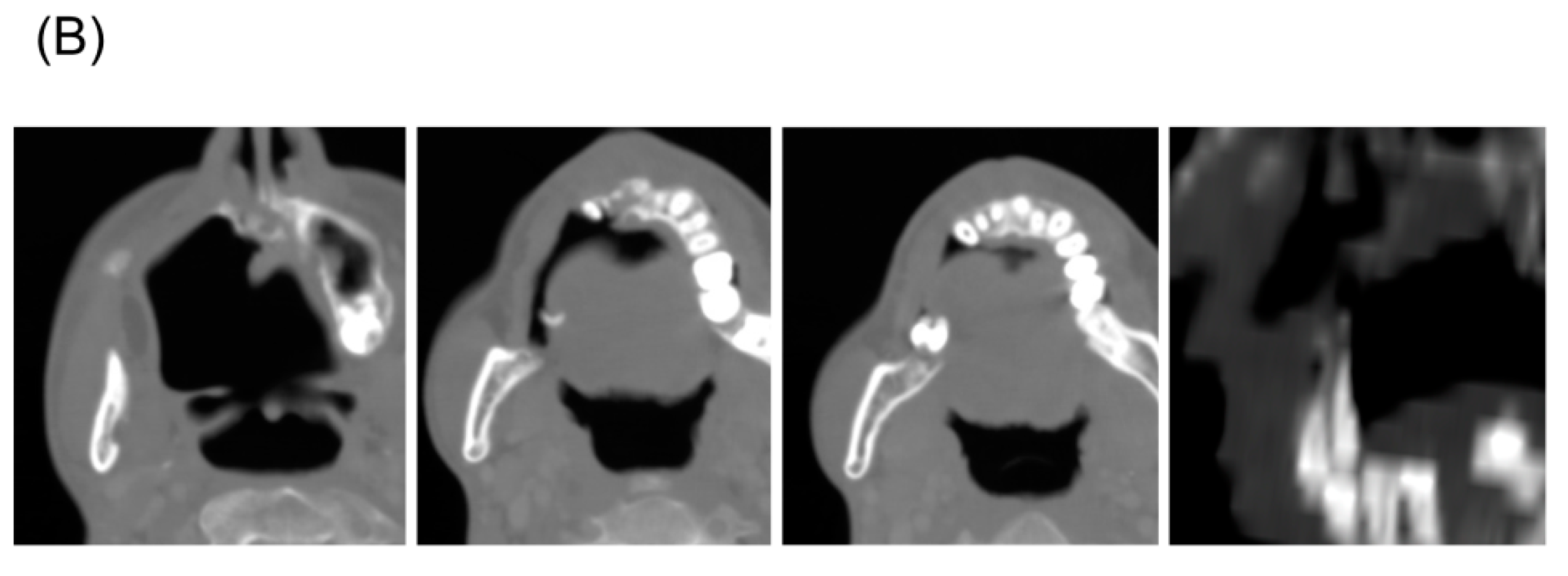
2.3. Assessment of Tooth Loss
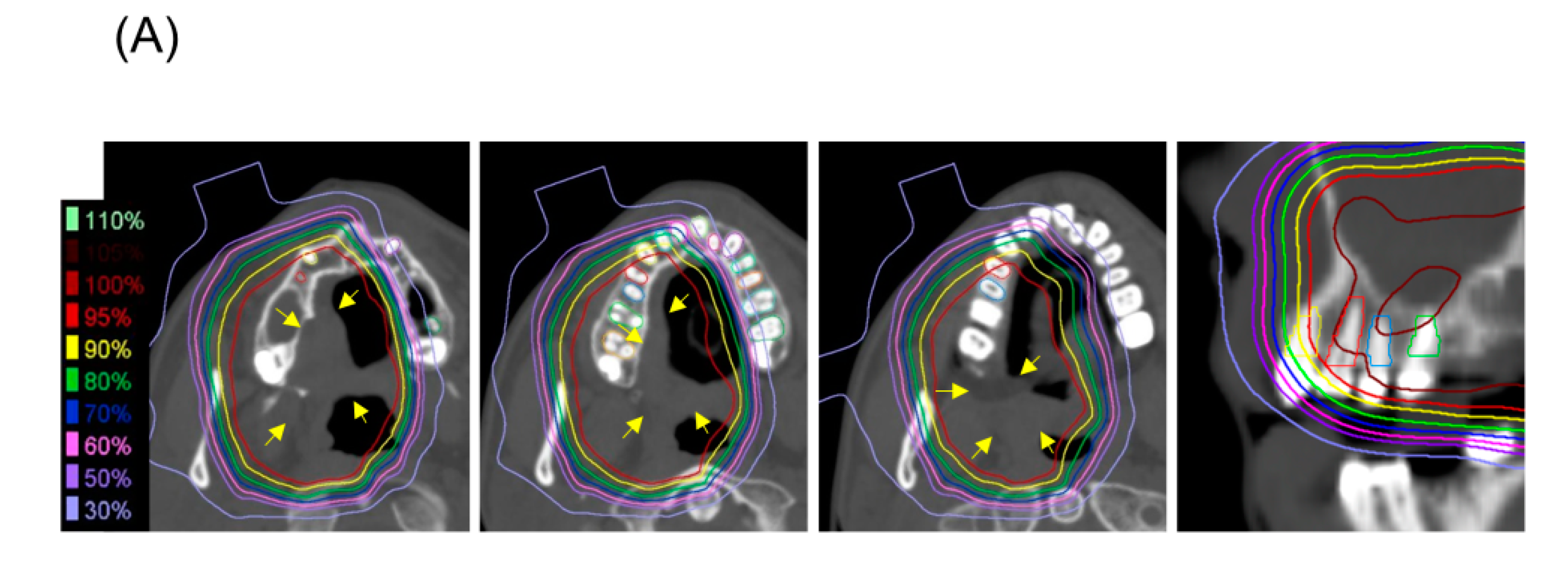
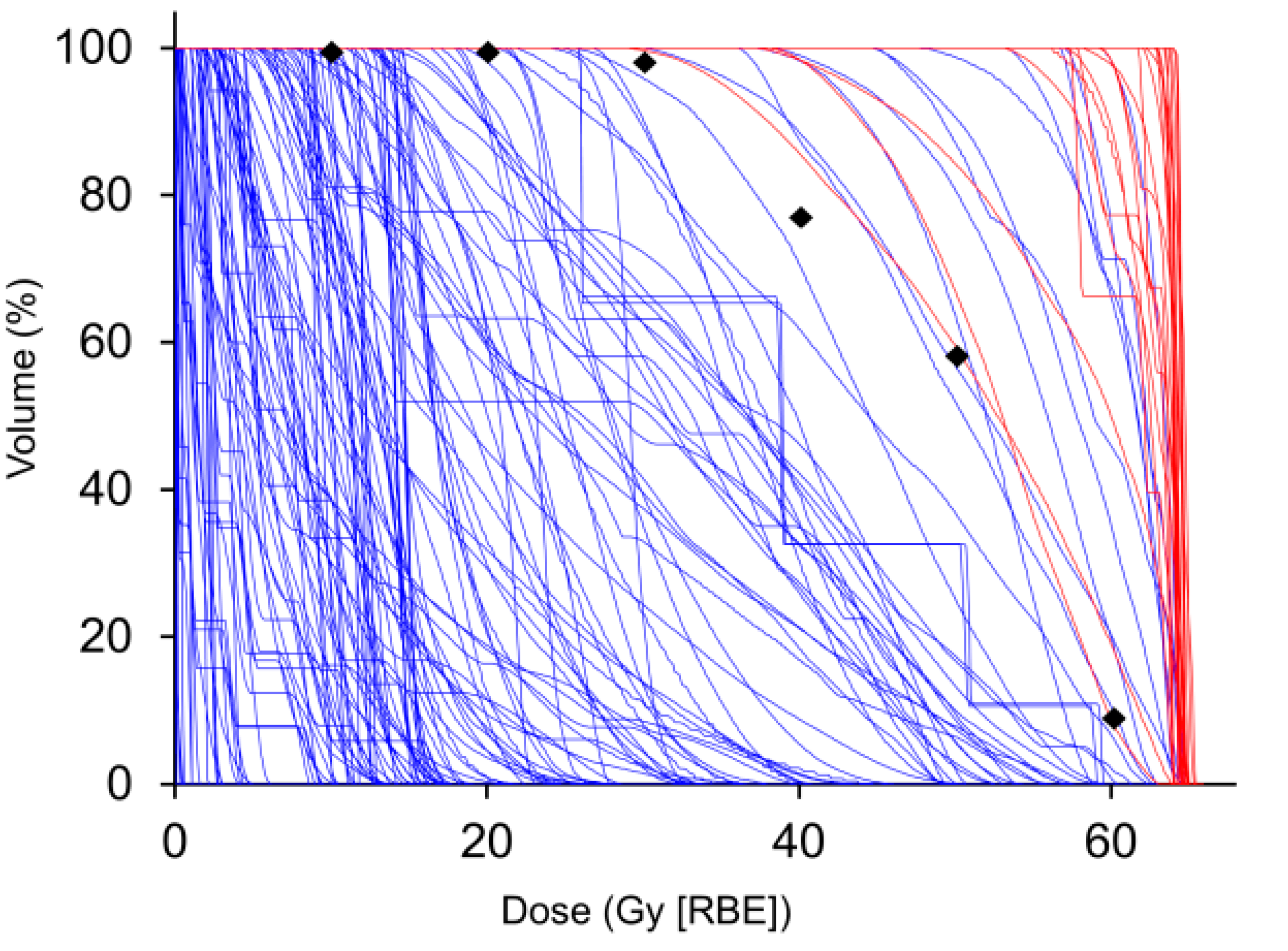
2.4. Dose–Volume Analysis of the Teeth
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
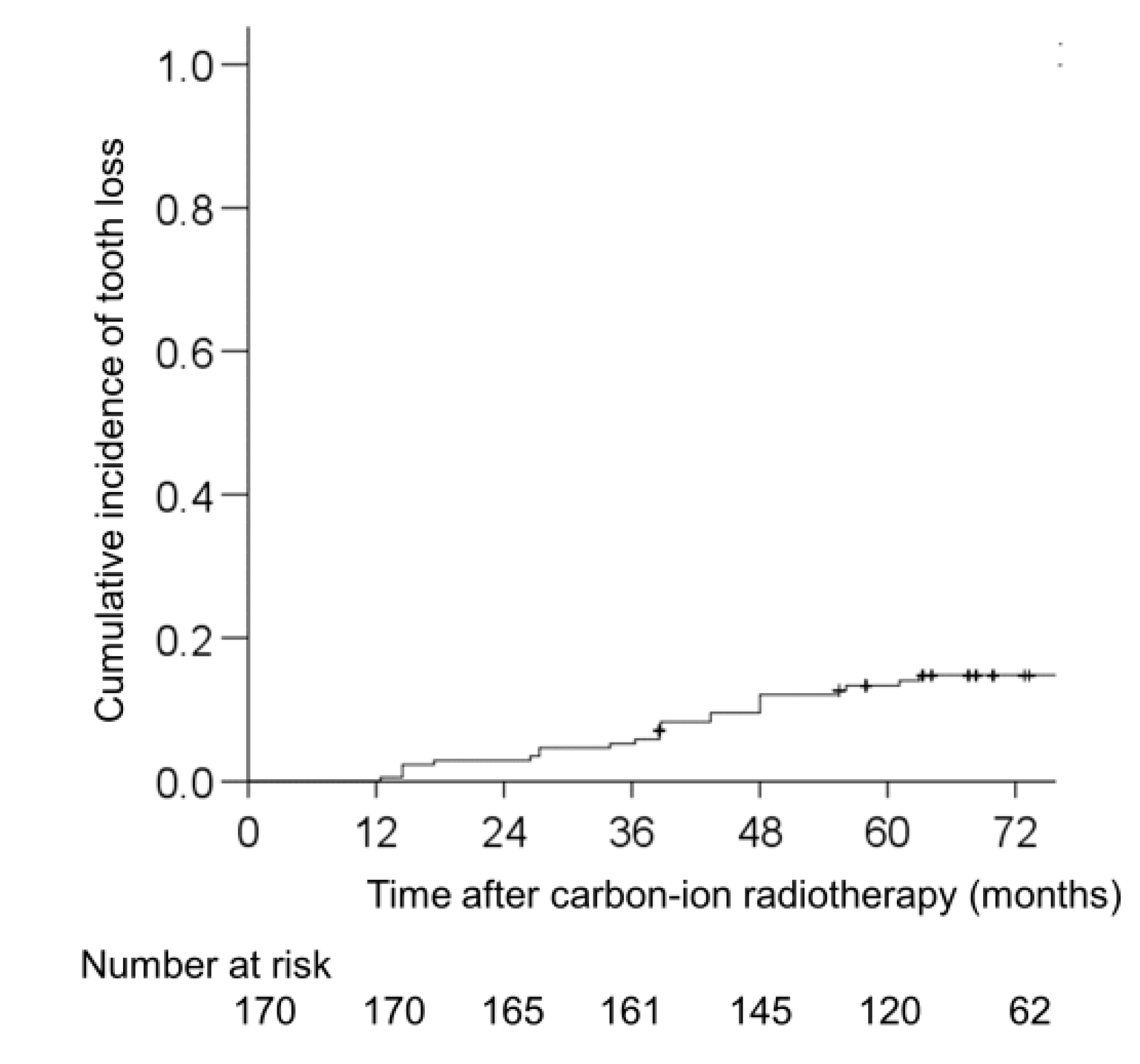
3.2. Incidence of Tooth Loss Post-CIRT
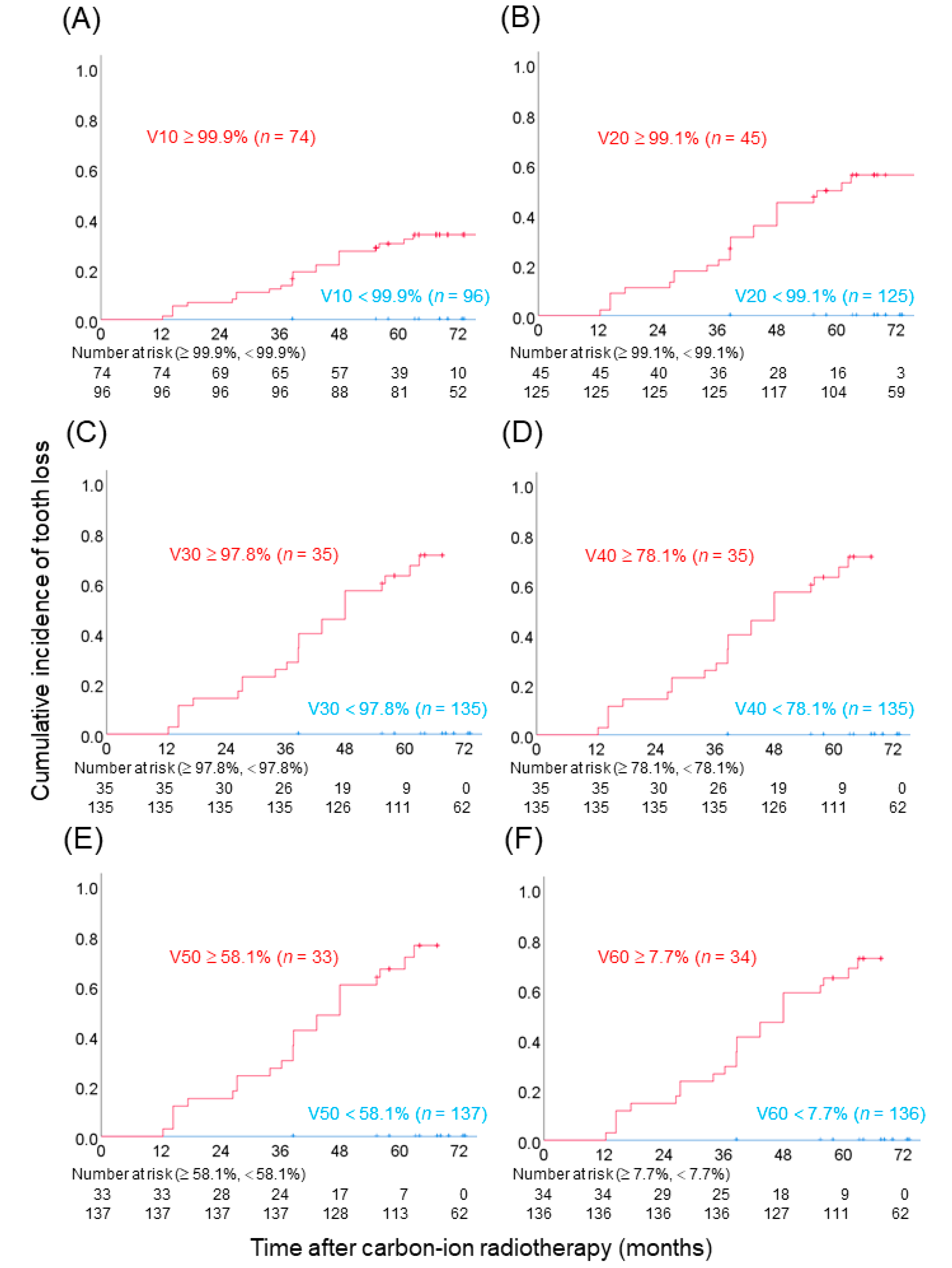
3.3. Dose–Volume Analysis of Tooth Loss Post-CIRT
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Delaney, G.; Jacob, S.; Featherstone, C.; Barton, M. The role of radiotherapy in cancer treatment: Estimating optimal utilization from a review of evidence-based clinical guidelines. Cancer 2005, 104, 1129–1137. [Google Scholar] [CrossRef] [PubMed]
- Strojan, P.; Hutcheson, K.A.; Eisbruch, A.; Beitler, J.J.; Langendijk, J.A.; Lee, A.W.M.; Corry, J.; Mendenhall, W.M.; Smee, R.; Rinaldo, A.; et al. Treatment of late sequelae after radiotherapy for head and neck cancer. Cancer Treat. Rev. 2017, 59, 79–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlaff, C.D.; Krauze, A.; Belard, A.; O’Connell, J.J.; Camphausen, K.A. Bringing the heavy: Carbon ion therapy in the radiobiological and clinical context. Radiat. Oncol. 2014, 9, 88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanai, T.; Furusawa, Y.; Fukutsu, K.; Itsukaichi, H.; Eguchi-Kasai, K.; Ohara, H. Irradiation of Mixed Beam and Design of Spread-Out Bragg Peak for Heavy-Ion Radiotherapy. Radiat. Res. 1997, 147, 78. [Google Scholar] [CrossRef]
- Kamada, T.; Tsujii, H.; Blakely, E.A.; Debus, J.; De Neve, W.; Durante, M.; Jäkel, O.; Mayer, R.; Orecchia, R.; Pötter, R.; et al. Carbon ion radiotherapy in Japan: An assessment of 20 years of clinical experience. Lancet Oncol. 2015, 16, e93–e100. [Google Scholar] [CrossRef] [Green Version]
- Miyasaka, Y.; Komatsu, S.; Abe, T.; Kubo, N.; Okano, N.; Shibuya, K.; Shirai, K.; Kawamura, H.; Saitoh, J.-I.; Ebara, T.; et al. Comparison of Oncologic Outcomes between Carbon Ion Radiotherapy and Stereotactic Body Radiotherapy for Early-Stage Non-Small Cell Lung Cancer. Cancers 2021, 13, 176. [Google Scholar] [CrossRef]
- Imai, R.; Kamada, T.; Araki, N.; Abe, S.; Iwamoto, Y.; Ozaki, T.; Chuman, H.; Hiraga, H.; Hiruma, T.; Kamade, N.; et al. Carbon Ion Radiation Therapy for Unresectable Sacral Chordoma: An Analysis of 188 Cases. Int. J. Radiat. Oncol. 2016, 95, 322–327. [Google Scholar] [CrossRef]
- Kawamura, H.; Kubo, N.; Sato, H.; Mizukami, T.; Katoh, H.; Ishikawa, H.; Ohno, T.; Matsui, H.; Ito, K.; Suzuki, K.; et al. Moderately hypofractionated carbon ion radiotherapy for prostate cancer; a prospective observational study “GUNMA0702”. BMC Cancer 2020, 20, 75. [Google Scholar] [CrossRef] [Green Version]
- Kawashiro, S.; Yamada, S.; Okamoto, M.; Ohno, T.; Nakano, T.; Shinoto, M.; Shioyama, Y.; Nemoto, K.; Isozaki, Y.; Tsuji, H.; et al. Multi-institutional Study of Carbon-ion Radiotherapy for Locally Advanced Pancreatic Cancer: Japan Carbon-ion Radiation Oncology Study Group (J-CROS) Study 1403 Pancreas. Int. J. Radiat. Oncol. 2018, 101, 1212–1221. [Google Scholar] [CrossRef]
- Saitoh, J.-I.; Koto, M.; Demizu, Y.; Suefuji, H.; Ohno, T.; Tsuji, H.; Okimoto, T.; Shioyama, Y.; Nemoto, K.; Nakano, T.; et al. A Multicenter Study of Carbon-Ion Radiation Therapy for Head and Neck Adenocarcinoma. Int. J. Radiat. Oncol. 2017, 99, 442–449. [Google Scholar] [CrossRef]
- Sulaiman, N.S.; Demizu, Y.; Koto, M.; Saitoh, J.-I.; Suefuji, H.; Tsuji, H.; Ohno, T.; Shioyama, Y.; Okimoto, T.; Daimon, T.; et al. Multicenter Study of Carbon-Ion Radiation Therapy for Adenoid Cystic Carcinoma of the Head and Neck: Subanalysis of the Japan Carbon-Ion Radiation Oncology Study Group (J-CROS) Study (1402 HN). Int. J. Radiat. Oncol. 2018, 100, 639–646. [Google Scholar] [CrossRef] [PubMed]
- Suefuji, H.; Koto, M.; Demizu, Y.; Saitoh, J.-I.; Shioyama, Y.; Tsuji, H.; Okimoto, T.; Ohno, T.; Nemoto, K.; Nakano, T.; et al. A Retrospective Multicenter Study of Carbon Ion Radiotherapy for Locally Advanced Olfactory Neuroblastomas. Anticancer Res. 2018, 38, 1665–1670. [Google Scholar] [CrossRef] [Green Version]
- Mizoguchi, N.; Tsuji, H.; Toyama, S.; Kamada, T.; Tsujii, H.; Nakayama, Y.; Mizota, A.; Ohnishi, Y. Carbon-ion radiotherapy for locally advanced primary or postoperative recurrent epithelial carcinoma of the lacrimal gland. Radiother. Oncol. 2015, 114, 373–377. [Google Scholar] [CrossRef] [PubMed]
- Laura, Q.M.; Chow, M.D. Head and Neck Cancer. N. Engl. J. Med. 2020, 382, 60–72. [Google Scholar] [CrossRef]
- Forastiere, A.A.; Koch, W.M.; Trotti, A.; Sidransky, D. Head and Neck Cancer. N. Engl. J. Med. 2001, 345, 1890–1900. [Google Scholar] [CrossRef]
- Shirai, K.; Saitoh, J.-I.; Musha, A.; Abe, T.; Kobayashi, D.; Takahashi, T.; Tamaki, T.; Kawamura, H.; Takayasu, Y.; Shino, M.; et al. Prospective observational study of carbon-ion radiotherapy for non-squamous cell carcinoma of the head and neck. Cancer Sci. 2017, 108. [Google Scholar] [CrossRef] [Green Version]
- Sasahara, G.; Koto, M.; Ikawa, H.; Hasegawa, A.; Takagi, R.; Okamoto, Y.; Kamada, T. Effects of the dose-volume relationship on and risk factors for maxillary osteoradionecrosis after carbon ion radiotherapy. Radiat. Oncol. 2014, 9, 92. [Google Scholar] [CrossRef] [Green Version]
- Hasegawa, A.; Mizoe, J.-E.; Mizota, A.; Tsujii, H. Outcomes of visual acuity in carbon ion radiotherapy: Analysis of dose–volume histograms and prognostic factors. Int. J. Radiat. Oncol. 2006, 64, 396–401. [Google Scholar] [CrossRef]
- Kubo, N.; Kubota, Y.; Kawamura, H.; Oike, T.; Sakai, M.; Kumazawa, T.; Miyasaka, Y.; Okazaki, S.; Kobayashi, D.; Sato, H.; et al. Dosimetric parameters predictive of nasolacrimal duct obstruction after carbon-ion radiotherapy for head and neck carcinoma. Radiother. Oncol. 2019, 141, 72–77. [Google Scholar] [CrossRef] [Green Version]
- Shirai, K.; Fukata, K.; Adachi, A.; Saitoh, J.-I.; Musha, A.; Abe, T.; Kanai, T.; Kobayashi, D.; Shigeta, Y.; Yokoo, S.; et al. Dose–volume histogram analysis of brainstem necrosis in head and neck tumors treated using carbon-ion radiotherapy. Radiother. Oncol. 2017, 125, 36–40. [Google Scholar] [CrossRef] [Green Version]
- Kanai, T.; Endo, M.; Minohara, S.; Miyahara, N.; Koyama-Ito, H.; Tomura, H.; Matsufuji, N.; Futami, Y.; Fukumura, A.; Hiraoka, T.; et al. Biophysical characteristics of HIMAC clinical irradiation system for heavy-ion radiation therapy. Int. J. Radiat. Oncol. 1999, 44, 201–210. [Google Scholar] [CrossRef]
- Vissink, A.; Jansma, J.; Spijkervet, F.K.L.; Burlage, F.R.; Coppes, R.P. Oral Sequelae of Head and Neck Radiotherapy. Crit. Rev. Oral Biol. Med. 2003, 14, 199–212. [Google Scholar] [CrossRef]
- Bhandari, S.; Soni, B.W.; Bahl, A.; Ghoshal, S. Radiotherapy-induced oral morbidities in head and neck cancer patients. Spec. Care Dent. 2020, 40, 238–250. [Google Scholar] [CrossRef] [PubMed]
- Kielbassa, A.M.; Hinkelbein, W.; Hellwig, E.; Meyer-Lückel, H. Radiation-related damage to dentition. Lancet Oncol. 2006, 7, 326–335. [Google Scholar] [CrossRef]
- Beesley, R.; Rieger, J.; Compton, S.; Parliament, M.; Seikaly, H.; Wolfaardt, J. Comparison of tooth loss between intensity-modulated and conventional radiotherapy in head and neck cancer patients. J. Otolaryngol. Head Neck Surg. 2012, 41, 389–395. [Google Scholar] [CrossRef]
- Walker, M.P.; Wichman, B.; Cheng, A.-L.; Coster, J.; Williams, K.B. Impact of radiotherapy dose on dentition breakdown in head and neck cancer patients. Pract. Radiat. Oncol. 2011, 1, 142–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lieshout, H.F.J.; Bots, C.P. The effect of radiotherapy on dental hard tissue—A systematic review. Clin. Oral Investig. 2014, 18, 17–24. [Google Scholar] [CrossRef]
- Pinna, R.; Campus, G.; Cumbo, E.; Mura, I.; Milia, E. Xerostomia induced by radiotherapy: An overview of the physiopathology, clinical evidence, and management of the oral damage. Ther. Clin. Risk Manag. 2015, 11, 171–188. [Google Scholar] [CrossRef]
- Koga, D.H.; Salvajoli, J.V.; Alves, F.A. Dental extractions and radiotherapy in head and neck oncology: Review of the literature. Oral Dis. 2008, 14, 40–44. [Google Scholar] [CrossRef]
- Aida, J.; Ando, Y.; Akhter, R.; Aoyama, H.; Masui, M.; Morita, M. Reasons for Permanent Tooth Extractions in Japan. J. Epidemiol. 2006, 16, 214–219. [Google Scholar] [CrossRef]
- Hirotomi, T.; Yoshihara, A.; Ogawa, H.; Miyazaki, H. Tooth-related risk factors for tooth loss in community-dwelling elderly people. Community Dent. Oral Epidemiol. 2012, 40, 154–163. [Google Scholar] [CrossRef] [PubMed]
- Ravald, N.; Johansson, C.S. Tooth loss in periodontally treated patients. A long-term study of periodontal disease and root caries. J. Clin. Periodontol. 2012, 39, 73–79. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | All (n = 14) | ||
|---|---|---|---|
| Age | |||
| Median (range) | 59 (32–77) | ||
| Gender | |||
| Male | 5 | ||
| Female | 9 | ||
| Performance status | |||
| 0 | 6 | ||
| 1 | 8 | ||
| Histology | |||
| Adenoid cystic carcinoma | 10 | ||
| Mucoepidermoid carcinoma | 2 | ||
| Olfactory neuroblastoma | 1 | ||
| Basal cell adenocarcinoma | 1 | ||
| Primary tumor site | |||
| Nasal cavity | 7 | ||
| Maxillary sinus | 3 | ||
| Oral cavity | 2 | ||
| Pharynx | 1 | ||
| Parotid gland | 1 | ||
| Operability | |||
| Operable | 8 | ||
| Inoperable | 6 | ||
| Primary or recurrence | |||
| Primary tumor | 12 | ||
| Postoperative recurrence | 2 | ||
| T stage | |||
| T2 | 2 | ||
| T3 | 6 | ||
| T4 | 6 | ||
| N stage | |||
| N0 | 14 | ||
| Carbon-ion dose | |||
| 64.0 Gy (RBE)/16 fractions | 13 | ||
| 57.6 Gy (RBE)/16 fractions | 1 | ||
| Parameter | V10 | V20 | V30 | V40 | V50 | V60 |
|---|---|---|---|---|---|---|
| Cut-off value | 99.9% | 99.1% | 97.8% | 78.1% | 58.1% | 7.67% |
| Sensitivity | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Specificity | 0.66 | 0.86 | 0.92 | 0.92 | 0.94 | 0.93 |
| Accuracy | 0.71 | 0.88 | 0.94 | 0.94 | 0.95 | 0.94 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kubo, N.; Sakai, M.; Kawamura, H.; Oike, T.; Kubota, Y.; Anakura, M.; Adachi, A.; Sato, H.; Musha, A.; Okano, N.; et al. Dosimetric Parameters Predicting Tooth Loss after Carbon Ion Radiotherapy for Head and Neck Tumors. Radiation 2021, 1, 183-193. https://0-doi-org.brum.beds.ac.uk/10.3390/radiation1030017
Kubo N, Sakai M, Kawamura H, Oike T, Kubota Y, Anakura M, Adachi A, Sato H, Musha A, Okano N, et al. Dosimetric Parameters Predicting Tooth Loss after Carbon Ion Radiotherapy for Head and Neck Tumors. Radiation. 2021; 1(3):183-193. https://0-doi-org.brum.beds.ac.uk/10.3390/radiation1030017
Chicago/Turabian StyleKubo, Nobuteru, Makoto Sakai, Hidemasa Kawamura, Takahiro Oike, Yoshiki Kubota, Mai Anakura, Akiko Adachi, Hiro Sato, Atsushi Musha, Naoko Okano, and et al. 2021. "Dosimetric Parameters Predicting Tooth Loss after Carbon Ion Radiotherapy for Head and Neck Tumors" Radiation 1, no. 3: 183-193. https://0-doi-org.brum.beds.ac.uk/10.3390/radiation1030017