
Effectiveness of Bioactive Toothpastes against Dentin Hypersensitivity Using Evaporative and Tactile Analyses: A Randomized Clinical Trial

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Design
2.2. Ethical Considerations
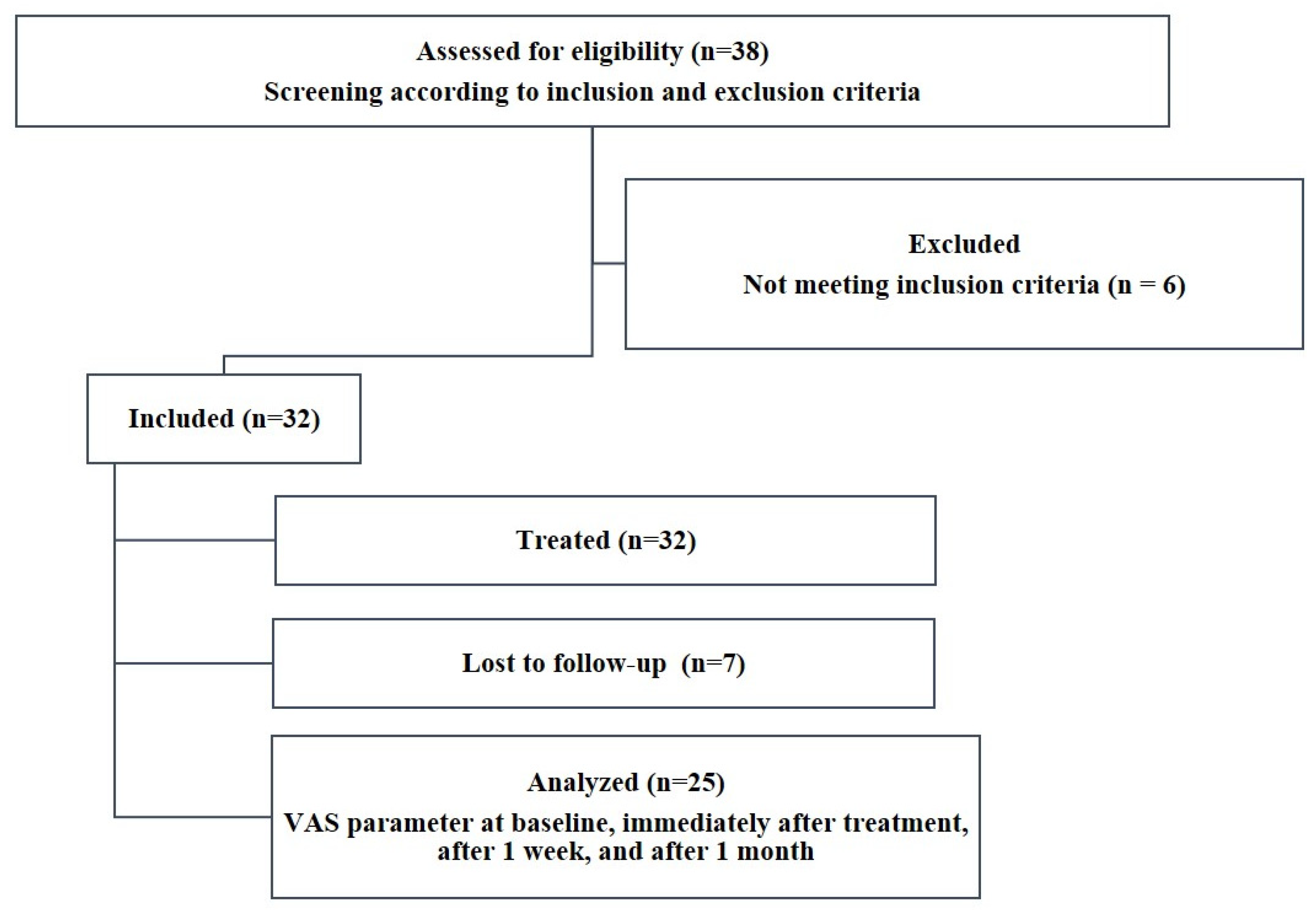
2.3. Patient Selection
2.4. Clinical Procedures
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Canadian Advisory Board on Dentin Hypersensitivity. Consensus-based recommendations for the diagnosis and management of dentin hypersensitivity. J. Can. Dent. Assoc. 2003, 69, 221–226. [Google Scholar]
- Maillard, M.; Bandiaky, O.N.; Maunoury, S.; Alliot, C.; Alliot-Licht, B.; Serisier, S.; Renard, E. The effectiveness of calcium phosphates in the treatment of dentinal hypersensitivity: A systematic review. Bioengineering 2023, 10, 447. [Google Scholar] [CrossRef] [PubMed]
- Favaro Zeola, L.; Soares, P.V.; Cunha-Cruz, J. Prevalence of dentin hypersensitivity: Systematic review and meta-analysis. J. Dent. 2019, 81, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.-X.; Tenenbaum, H.C.; Wilder, R.S.; Quock, R.; Hewlett, E.R.; Ren, Y.-F. Pathogenesis, diagnosis and management of dentin hypersensitivity: An evidence-based overview for dental practitioners. BMC Oral Health 2020, 20, 220. [Google Scholar] [CrossRef] [PubMed]
- Douglas-de-Oliveira, D.W.; Vitor, G.P.; Silveira, J.O.; Martins, C.C.; Costa, F.O.; Cota, L.O.M. Effect of dentin hypersensitivity treatment on oral health related quality of life—A systematic review and meta-analysis. J. Dent. 2018, 71, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Nardi, G.M.; Sabatini, S.; Acito, G.; Colavito, A.; Chiavistelli, L.; Campus, G. The decision tree for clinical management of dentin hypersensitivity. A consensus report. Oral Health Prev. Dent. 2022, 20, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Freitas, S.A.A.d.; Oliveira, N.M.A.d.; de Geus, J.L.; Souza, S.d.F.C.; Pereira, A.d.F.V.; Bauer, J. Bioactive toothpastes in dentin hypersensitivity treatment: A systematic review. Saudi Dent. J. 2021, 33, 395–403. [Google Scholar] [CrossRef]
- Vilhena, F.V.; de Oliveira, S.M.L.; Matochek, M.H.M.; Tomaz, P.L.S.; Oliveira, T.S.; D’Alpino, P.H.P. Biomimetic Mechanism of Action of Fluoridated Toothpaste Containing Proprietary REFIX Technology on the Remineralization and Repair of Demineralized Dental Tissues: An In Vitro Study. Eur. J. Dent. 2021, 15, 236–241. [Google Scholar] [CrossRef]
- Philip, N. State of the art enamel remineralization systems: The next frontier in caries management. Caries Res. 2019, 53, 284–295. [Google Scholar] [CrossRef]
- Pandya, M.; Diekwisch, T.G.H. Enamel biomimetics-fiction or future of dentistry. Int. J. Oral Sci. 2019, 11, 8. [Google Scholar] [CrossRef]
- Meyer, F.; Amaechi, B.T.; Fabritius, H.O.; Enax, J. Overview of calcium phosphates used in biomimetic oral care. Open Dent. J. 2018, 12, 406–423. [Google Scholar] [CrossRef] [PubMed]
- Zangrando, M.S.R.; Silva, G.F.F.; Bigotto, M.L.B.; Cintra, F.M.R.N.; Damante, C.A.; Sant’Ana, A.C.P.; Vilhena, F.V. Blocking tubules technologies for dentin hypersensitivity in periodontal patients—Pilot study. Res. Soc. Dev. 2021, 10, e35101320398. [Google Scholar] [CrossRef]
- Seong, J.; Newcombe, R.G.; Matheson, J.R.; Weddell, L.; Edwards, M.; West, N.X. A randomised controlled trial investigating efficacy of a novel toothpaste containing calcium silicate and sodium phosphate in dentine hypersensitivity pain reduction compared to a fluoride control toothpaste. J. Dent. 2020, 98, 103320. [Google Scholar] [CrossRef]
- Joao-Souza, S.H.; Scaramucci, T.; Buhler Borges, A.; Lussi, A.; Saads Carvalho, T.; Correa Aranha, A.C. Influence of desensitizing and anti-erosive toothpastes on dentine permeability: An in vitro study. J. Dent. 2019, 89, 103176. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Magalhaes, A.C.; Francisconi-Dos-Rios, L.F.; Calabria, M.P.; Araujo, D.; Buzalaf, M.; Lauris, J.; Pereira, J.C. Treatment of Dentin Hypersensitivity Using Nano-Hydroxyapatite Pastes: A Randomized Three-Month Clinical Trial. Oper. Dent. 2016, 41, E93–E101. [Google Scholar] [CrossRef]
- Ritter, A.V.; de Dias, W.L.; Miguez, P.; Caplan, D.J.; Swift, E.J., Jr. Treating cervical dentin hypersensitivity with fluoride varnish: A randomized clinical study. J. Am. Dent. Assoc. 2006, 137, 1013–1020, quiz 1029. [Google Scholar] [CrossRef]
- Birang, R.; Poursamimi, J.; Gutknecht, N.; Lampert, F.; Mir, M. Comparative evaluation of the effects of Nd:YAG and Er:YAG laser in dentin hypersensitivity treatment. Lasers Med. Sci. 2007, 22, 21–24. [Google Scholar] [CrossRef]
- Sealed Envelope, Ltd. Power Calculator for Binary Outcome Non-Inferiority Trial. Available online: https://www.sealedenvelope.com/power/binary-noninferior/ (accessed on 17 October 2023).
- Bekes, K.; Heinzelmann, K.; Lettner, S.; Schaller, H.G. Efficacy of desensitizing products containing 8% arginine and calcium carbonate for hypersensitivity relief in MIH-affected molars: An 8-week clinical study. Clin. Oral Investig. 2017, 21, 2311–2317. [Google Scholar] [CrossRef]
- Ayad, F.; Ayad, N.; Vazquez, J.; Zhang, Y.P.; Mateo, L.R.; Cummins, D. Use of a toothpaste containing 8% arginine and calcium carbonate for immediate and lasting relief of dentin hypersensitivity: A simple and effective in-office procedure. Am. J. Dent. 2018, 31, 135–140. [Google Scholar]
- Vilhena, F.V.; Polassi, M.R.; Paloco, E.A.C.; Alonso, R.C.; Guiraldo, R.D.; D’Alpino, P.H. Effectiveness of toothpaste containing REFIX technology against dentin hypersensitivity: A randomized clinical study. J. Contemp. Dent. Pract. 2020, 21, 609–614. [Google Scholar] [CrossRef]
- Schiff, T.; Delgado, E.; Zhang, Y.P.; Cummins, D.; DeVizio, W.; Mateo, L.R. Clinical evaluation of the efficacy of an in-office desensitizing paste containing 8% arginine and calcium carbonate in providing instant and lasting relief of dentin hypersensitivity. Am. J. Dent. 2009, 22, 8A–15A. [Google Scholar] [PubMed]
- Delgado, D.A.; Lambert, B.S.; Boutris, N.; McCulloch, P.C.; Robbins, A.B.; Moreno, M.R.; Harris, J.D. Validation of digital visual analog scale pain scoring with a traditional paper-based visual analog scale in adults. J. Am. Acad. Orthop. Surg. Glob. Res. Rev. 2018, 2, e088. [Google Scholar] [CrossRef] [PubMed]
- Madruga, M.d.M.; Silva, A.F.d.; Rosa, W.L.d.O.d.; Piva, E.; Lund, R.G. Evaluation of dentin hypersensitivity treatment with glass ionomer cements: A randomized clinical trial. Braz. Oral Res. 2017, 31, e3. [Google Scholar] [CrossRef]
- Shiau, H.J. Dentin hypersensitivity. J. Evid. Based Dent. Pract. 2012, 12, 220–228. [Google Scholar] [CrossRef] [PubMed]
- Cummins, D. Clinical evidence for the superior efficacy of a dentifrice containing 8.0% arginine and calcium carbonate in providing instant and lasting relief of dentin hypersensitivity. J. Clin. Dent. 2011, 22, 97–99. [Google Scholar] [PubMed]
- Hu, M.-L.; Zheng, G.; Lin, H.; Yang, M.; Zhang, Y.-D.; Han, J.-M. Network meta-analysis on the effect of desensitizing toothpastes on dentine hypersensitivity. J. Dent. 2019, 88, 103170. [Google Scholar] [CrossRef]
- Martins, C.C.; Firmino, R.T.; Riva, J.J.; Ge, L.; Carrasco-Labra, A.; Brignardello-Petersen, R.; Colunga-Lozano, L.E.; Granville-Garcia, A.F.; Costa, F.O.; Yepes-Nuñez, J.J.; et al. Desensitizing toothpastes for dentin hypersensitivity: A network meta-analysis. J. Dent. Res. 2020, 99, 514–522. [Google Scholar] [CrossRef]
- Joshi, S.; Gowda, A.S.; Joshi, C. Comparative evaluation of NovaMin desensitizer and Gluma desensitizer on dentinal tubule occlusion: A scanning electron microscopic study. J. Periodontal Implant. Sci. 2013, 43, 269–275. [Google Scholar] [CrossRef]
- Khijmatgar, S.; Reddy, U.; John, S.; Badavannavar, A.N.; Souza, T.D. Is there evidence for Novamin application in remineralization?: A Systematic review. J. Oral Biol. Craniofacial Res. 2020, 10, 87–92. [Google Scholar] [CrossRef]
- Alexandrino, L.D.; Alencar, C.d.M.; Silveira, A.D.S.d.; Alves, E.B.; Silva, C.M. Randomized clinical trial of the effect of NovaMin and CPP-ACPF in combination with dental bleaching. J. Appl. Oral Sci. 2017, 25, 335–340. [Google Scholar] [CrossRef]
- Du Min, Q.; Bian, Z.; Jiang, H.; Greenspan, D.C.; Burwell, A.K.; Zhong, J.; Tai, B.J. Clinical evaluation of a dentifrice containing calcium sodium phosphosilicate (novamin) for the treatment of dentin hypersensitivity. Am. J. Dent. 2008, 21, 210–214. [Google Scholar]
- Vilhena, F.V.; Lonni, A.A.S.G.; D’Alpino, P.H.P. Silicon-enriched hydroxyapatite formed induced by REFIX-based toothpaste on the enamel surface. Braz. Dent. Sci. 2021, 24, 1–7. [Google Scholar] [CrossRef]
- Fernandes, N.L.S.; Juliellen, L.D.C.; Andressa, F.B.O.; D’Alpino, H.P.P.; Sampaio, C.F. Resistance against erosive challenge of dental enamel treated with 1,450-PPM fluoride toothpastes containing different biomimetic compounds. Eur. J. Dent. 2021, 15, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, N.L.S.; Silva, J.; de Sousa, E.B.G.; D’Alpino, P.H.P.; de Oliveira, A.F.B.; de Jong, E.J.; Sampaio, F.C. Effectiveness of fluoride-containing toothpastes associated with different technologies to remineralize enamel after pH cycling: An in vitro study. BMC Oral Health 2022, 22, 489. [Google Scholar] [CrossRef] [PubMed]
- Vilhena, F.V.; Grecco, S.D.S.; Gonzalez, A.H.M.; D’Alpino, P.H.P. Regenerative and protective effects on dental tissues of a fluoride-silicon-rich toothpaste associated with a calcium booster: An in vitro study. Dent. J. 2023, 11, 153. [Google Scholar] [CrossRef]
- Parker, A.S.; Patel, A.N.; Al Botros, R.; Snowden, M.E.; McKelvey, K.; Unwin, P.R.; Ashcroft, A.T.; Carvell, M.; Joiner, A.; Peruffo, M. Measurement of the efficacy of calcium silicate for the protection and repair of dental enamel. J. Dent. 2014, 42, S21–S29. [Google Scholar] [CrossRef]
- Joiner, A.; Schäfer, F.; Naeeni, M.M.; Gupta, A.K.; Zero, D.T. Remineralisation effect of a dual-phase calcium silicate/phosphate gel combined with calcium silicate/phosphate toothpaste on acid-challenged enamel in situ. J. Dent. 2014, 42, S53–S59. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Treatment | UNIMES | UNIAN | Total | Dropouts |
|---|---|---|---|---|
| Colgate Sensitive Pro-Relief | 5 (49) | 1 (7) | 3 | |
| Sensodyne Repair & Protect | 3 (47) | 2 (16) | 5 (63) B | 3 |
| Regenerador Sensitive | 4 (44) | 2 (9) | 6 (53) A | 1 |
| Regenerador Sensitive + Calcium Booster | 4 (60) | 4 (15) | 8 (75) B | 0 |
| Dental Gel | Composition |
|---|---|
| Colgate Sensitive Pro-Relief a | Arginine 8%, Calcium Carbonate, Sodium, Monofluorophosphate 1.1% (1450 ppm fluoride), Water, Sorbitol, Sodium Lauryl Sulfate, Aroma, Cellulose, Gum, Potassium Acesulfame, Sodium Silicate, Xanthan Gum, Sucralose, Titanium Dioxide |
| Sensodyne Repair & Protect b | 1426 ppm sodium fluoride, Calcium Sodium Phosphosilicate 5% (NOVAMIN) Glycerin, PEG-8, hydrated silica, pentasodium triphosphate, sodium lauryl sulfate, flavor, titanium dioxide, polyacrylic acid, cocamidopropyl betaine, sodium saccharin |
| Regenerador Sentitive c | 1450 ppm sodium fluoride, glycerin, silica, sorbitol, sodium lauryl sulfate, aqua, aroma, PEF-12, cellulose gum, phosphoric acid, xylitol, tetrasodium pyrophosphate, sodium saccharin, triclosan, menthol, mica, sodium benzoate, REFIX Technology |
| Calcium Booster c | 5% calcium mix (calcium carbonate, tricalcium phosphate), silica, glycerin, CPC, saccharine, water) |
| Dental Gel | Initial | First Brushing | 1 Week | 1 Month |
|---|---|---|---|---|
| Colgate Sensitive Pro-Relief | 4.3 (2.9) B | 3.8 (3.2) B | 2.7 (2.7) A | 2.1 (2.4) A |
| Sensodyne Repair & Protect | 5.6 (3.0) C | 3.2 (2.5) B | 2.9 (2.2) B | 1.3 (1.9) A |
| Regenerador Sensitive | 5.9 (1.9) C | 4.0 (2.9) B | 2.6 (2.0) A | 2.1 (2.4) A |
| Regenerador Sensitive + Calcium Booster | 5.3 (2.3) D | 3.9 (2.7) C | 2.4 (2.1) B | 1.0 (2.1) A |
| Dental Gel | After First Brushing | After 1 Week | After 1 Month |
|---|---|---|---|
| Colgate Sensitive Pro-Relief | 15.5% (47.1) b | 43.4% (47.0) a | 36.7% (72.9) c |
| Sensodyne Repair & Protect | 30.2% (77.7) a | 33.5% (68.6) a | 79.2% (33.7) ab |
| Regenerador Sensitive | 27.4% (64.3) ab | 51.0% (41.1) a | 61.2% (53.1) bc |
| Regenerador Sensitive + Calcium Booster | 30.3% (36.5) ab | 47.7% (55.2) a | 78.9% (57.6) a |
| Dental Gel | Initial | First Brushing | 1 Week | 1 Month |
|---|---|---|---|---|
| Colgate Sensitive Pro-Relief | 4.5 (2.6) C | 2.9 (2.6) B | 1.4 (2.1) A | 0.9 (1.3) A |
| Sensodyne Repair & Protect | 3.8 (2.2) B | 1.3 (2.2) A | 0.7 (1.9) A | 0.4 (1.0) A |
| Regenerador Sensitive | 6.1 (2.3) B | 1.9 (2.4) A | 1.4 (2.3) A | 0.9 (1.6) A |
| Regenerador Sensitive + Calcium Booster | 4.0 (2.9) B | 1.3 (1.3) A | 0.8 (1.6) A | 0.6 (1.0) A |
| Dental Gel | After First Brushing | After 1 Week | After 1 Month |
|---|---|---|---|
| Colgate Sensitive Pro-Relief | 33.5% (53.2) a | 72.3% (43.4) a | 74.2% (43.5) a |
| Sensodyne Repair & Protect | 64.9% (57.2) b | 82.9% (46.5) a | 87.4% (32.7) a |
| Regenerador Sensitive | 66.7% (38.3) ab | 73.1% (39.1) a | 85.6% (52.0) a |
| Regenerador Sensitive + Calcium Booster | 58.0% (59.5) ab | 87.2% (28.4) a | 83.1% (30.4) a |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alonso, R.C.B.; Oliveira, L.d.; Silva, J.A.B.; Santos, W.B.B.d.; Ferreira, L.R.d.S.L.; Guiraldo, R.D.; Vilhena, F.V.; D’Alpino, P.H.P. Effectiveness of Bioactive Toothpastes against Dentin Hypersensitivity Using Evaporative and Tactile Analyses: A Randomized Clinical Trial. Oral 2024, 4, 36-49. https://0-doi-org.brum.beds.ac.uk/10.3390/oral4010004
Alonso RCB, Oliveira Ld, Silva JAB, Santos WBBd, Ferreira LRdSL, Guiraldo RD, Vilhena FV, D’Alpino PHP. Effectiveness of Bioactive Toothpastes against Dentin Hypersensitivity Using Evaporative and Tactile Analyses: A Randomized Clinical Trial. Oral. 2024; 4(1):36-49. https://0-doi-org.brum.beds.ac.uk/10.3390/oral4010004
Chicago/Turabian StyleAlonso, Roberta Caroline Bruschi, Letícia de Oliveira, Jaqueline Alves Batista Silva, Williane Bernadete Bezerra dos Santos, Lúria Ribeiro de Souza Laranja Ferreira, Ricardo Danil Guiraldo, Fabiano Vieira Vilhena, and Paulo Henrique Perlatti D’Alpino. 2024. "Effectiveness of Bioactive Toothpastes against Dentin Hypersensitivity Using Evaporative and Tactile Analyses: A Randomized Clinical Trial" Oral 4, no. 1: 36-49. https://0-doi-org.brum.beds.ac.uk/10.3390/oral4010004