
Post-Mortem Quantitation of Amphetamine in Cadaveric Fluids in Saudi Arabia
by
 , ,
, ,
Ahmed I. Al-Asmari
1,* ,
,
Faiz D. Al-Solami
2 ,
,
Abdulnasser E. Al-Zahrani
2 and
Torki A. Zughaibi
3,4 1
Laboratory Department, Ministry of Health, King Abdul-Aziz Hospital, P.O. Box 6470, Jeddah 21442, Saudi Arabia
2
Poison Control and Forensic Medical Chemistry Center, Ministry of Health, P.O. Box 21543, Jeddah 21176, Saudi Arabia
3
Department of Medical Laboratory Sciences, Faculty of Applied Medical Sciences, King Abdulaziz University, P.O. Box 80216, Jeddah 21589, Saudi Arabia
4
King Fahd Medical Research Center, King Abdulaziz University, P.O. Box 80216, Jeddah 21589, Saudi Arabia
*
Author to whom correspondence should be addressed.
Forensic Sci. 2022, 2(1), 222-237; https://0-doi-org.brum.beds.ac.uk/10.3390/forensicsci2010017
Submission received: 15 January 2022
/
Revised: 8 February 2022
/
Accepted: 15 February 2022
/
Published: 1 March 2022
(This article belongs to the Special Issue Feature Papers in Forensic Sciences in 2022)
Abstract
:Amphetamine abuse is a known problem in Saudi Arabia; it is estimated that 40% of drug abusers misuse amphetamines. Here, our aim was to perform an up-to-date epidemiological study of amphetamine-related postmortem cases in Jeddah, Saudi Arabia, in which 235 postmortem cases were included. The largest number of cases was recorded for the groups aged between 31 and 40 years (86 cases) and the lowest number of cases was recorded for the group aged between 61 and 70 years old (5 cases). Amphetamine was co-ingested with other drug(s) in 55% of the total cases (blood with sodium fluoride (BN), median, 0.3 mg/L). Approximately 23% of all deaths were due to other co-ingested drugs (BN, median, 0.2 mg/L). Amphetamines alone were detected in 107 cases, (BN, median, 0.5 mg/L). Amphetamine was the sole cause of death in 16% of the studied cases (BN, median, 1.0 mg/L). The combination of amphetamine and a pre-existing disease were observed in 9.4% of all deaths (BN, median, 0.7 mg/L). The causes of death were determined to be accidental in the majority (47%) of cases, homicides in 26% of cases, suicides in 11% of cases, and unknown in 7% of cases. This is the first discussion of the amphetamine concentration in bile in amphetamine-related deaths, the relationship between amphetamine concentration in different bodily fluids, and the amphetamine concentration in putrefied corpses. This study concluded that amphetamine abuse in Jeddah, Saudi Arabia, increased over 400% between 2012 and 2018, and 41% of these cases involved violence. This result also suggests that preventive programs targeting youth and adolescent students are required to keep schools and universities free from drugs, especially amphetamines.
1. Introduction
Amphetamines are considered to be among the oldest stimulant drugs, first used in the early 1900s [1,2] and still consistently abused globally [3]. Amphetamines remain the recreational drug of choice in many countries, including Nordic and Middle Eastern countries. In Sweden, a 10-year study found that amphetamines were involved in 4% of postmortem cases related to road-traffic accidents [4]. Regular users of amphetamines are more likely to die from several causes [1].
Amphetamine abuse is a problem in Saudi Arabia, with 40% of drug abusers estimated to use amphetamines, particularly young individuals (12–22 years old) [5,6]. More than two-thirds of global amphetamine seizures are reported in Saudi Arabia [7,8]. It is not known when amphetamine use started in Saudi Arabia, but it has been banned since 1986 [9]. High rates of amphetamine abuse in this region can be explained by the general idea among users that amphetamine is a harmless and recreational drug that do not often result in fatality [10]. Amphetamine use increases during exam periods due to the belief by users that amphetamines can improve academic achievement. Some students believe that amphetamine use can help them overcome sleep deprivation and fatigue; however, amphetamines weaken cognition and can cause many serious complications [11].
The toxic effects of amphetamine use are observed when blood amphetamine concentrations are higher than 0.2 mg/L, and amphetamine fatalities are reported at blood amphetamine concentrations higher than 0.5 mg/L [12]. Decedents suffer nervousness, hyperthermia, convulsion, cardiac and respiratory failure prior to death [13]. Postmortem toxicology of amphetamine-related fatalities has rarely been reported, and most existing reports are dated in the 1970s [14,15,16,17], primarily reporting single-case investigations [15,18,19,20] or epidemiological studies involving large numbers of amphetamine-related fatalities [6,21]. It is common to detect amphetamines in postmortem specimens, but interpreting their contribution to fatalities is difficult. Although amphetamine-related fatalities have been reported, no link between death and amphetamine concentration has been demonstrated by autopsy. Death as a result of amphetamine ingestion is not rapid and often occurs several hours after the last dose, allowing for some of the drug to be metabolized and excreted [21,22]. This means that concentrations assessed after death do not reflect the concentration that led to death [23,24]. However, amphetamines are known to exhibit limited postmortem redistribution, which means that drug concentrations detected at the time of autopsy in a particular specimen are similar to those present at the time of death [6,13].
Most reported methods for extracting and detecting amphetamines are as a methamphetamine metabolite [25,26,27,28,29,30,31]. In fact, few reports are available for determining amphetamine in deaths solely attributable to amphetamine. Liquid–liquid extraction was the most common procedure for sample preparation [14,15,17,21,32,33,34], and three studies used solid-phase extraction (SPE; [10,18,35]). Techniques that have been applied to postmortem amphetamine detection include thin-layer chromatography [14,16], ultraviolet spectrometry [14,15,17], gas chromatography–mass spectrometry [18,20,32,33,36,37], liquid chromatography coupled with a photodiode array detector [22], and liquid chromatography–tandem mass spectrometry (LC-MS/MS) [10].
Although a well-known problem in Saudi Arabia, especially in the western region, no epidemiological studies concerning amphetamine-related postmortem cases have been conducted. Our aim here was to conduct an up-to-date epidemiological study of amphetamine-related postmortem cases in Jeddah, Saudi Arabia. In addition, we determined the demographic characteristics, circumstances, and pre-existing pathology of amphetamine-related postmortem deaths in Jeddah, Saudi Arabia (between 2012 and 2018). In this paper, we present new information regarding the distribution of amphetamines in amphetamine-related postmortem cases using an approach that considers multiple bodily fluids analysis (blood with sodium fluoride as a preservative (BN), urine, vitreous humor, bile, and stomach contents) and comparing these data with those obtained in previously reported studies.
2. Materials and Methods
2.1. Chemicals
HPLC-grade solvents and ammonium formate were obtained from Sigma Aldrich (Steinheim, Germany). Amphetamine and its internal standards (Amphetamine-D5) were purchased from Lipomed (Arlesheim, Switzerland). Solid-phase extraction (SPE) cartridges were obtained from United Chemical Technologies (part #CSDAU203) (Bristol, PA, USA).
2.2. Sample Preparation and Analysis
A recently published method for methamphetamine and amphetamine, in multiple bodily fluid specimens (blood, urine, vitreous humor, bile, and gastric contents) was adopted for the current investigation, using SPE as a sample pretreatment and triple quadrupole mass spectrometry and liquid chromatography–tandem mass spectrometry techniques (LC–MS/MS) [38].
2.3. Method Validation
The method was validated according to the ANSI/ASB standard [39]. Focus was placed on the validation and applicability of the described method for analysis of amphetamines using multiple postmortem bodily fluid specimens. Negative bodily fluid specimens obtained from postmortem cases were used as blank controls during validation.
2.4. Case Samples
All forensic autopsy cases of drug-related deaths submitted to the Jeddah Poison Control and Forensic Medical Chemistry Center (JPCC); Jeddah Health Affairs Ethical Approval Committee, research code: 00188) from 1 January 2012 to 31 July 2018 were included in this study. All autopsy samples were collected and analyzed using routine methods, as previously described [38]. In total, 3293 routine postmortem cases were investigated. Information about cases included in this study was collected by JPCC staff using the Forensic Toxicology Jeddah Database Service, including sex, history of drug abuse, postmortem interval time (PMI) details, circumstances of death, and place of death.
3. Results
3.1. Method Validation
This report employed a validated LC-MS/MS method to quantify amphetamine in bodily fluids from 235 postmortem cases that involved amphetamine. This method was found to be specific and sensitive in analyzing amphetamine in different biological fluids. A linear calibration curve was established between 0.001 and 1.0 mg/L for all bodily fluid specimens, with a good coefficient of determination (R2 = 0.99). The lower limit of quantification was 0.001 mg/L. Within-run precision was less than 7% and between-run precision was less than 5%. The accuracy values for the three tested precision controls (0.025 mg/L, 0.1 mg/L, and 0.750 mg/L) ranged between −2% and +4%. Matrix effects and recoveries were examined for the three tested precision control concentrations described above, and acceptable matrix effect and recovery values were obtained and ranged from 98% to 112% and 88% to 96% of the target concentration, respectively. Two dilution controls were investigated—0.1 and 7.5 mg/L—which were diluted 1:10 and 1:100 times, respectively; the target dilution concentrations of 0.010 and 0.075 mg/L were achieved within an acceptable range with a method accuracy of ±15%. In this work, interference from frequently detected drugs and their metabolites, blank bodily fluid postmortem specimens, or carryover effects from the last injection were examined and no effect on analyte detection was observed.
3.2. Demographic Profile
In this study, 235 postmortem cases were tested using the method described above. Positive amphetamine cases accounted for nearly 10% of all autopsy cases handled by JPCC between 2012 and 2018 (median, 5.3%; range 3–25%). The annual rate of positive amphetamine cases among JPCC postmortem cases ranged between 16 and 63 cases/year. Of the 235 cases included, the majority were men (99%), with a median age of 37 years. Multiple specimens were collected during autopsy, including BN, vitreous humor, bile, urine, and stomach contents. PMIs varied among cases, with a median of 24 h (range, 12–2664 h). The analyte concentrations and case details are listed in Table 1.
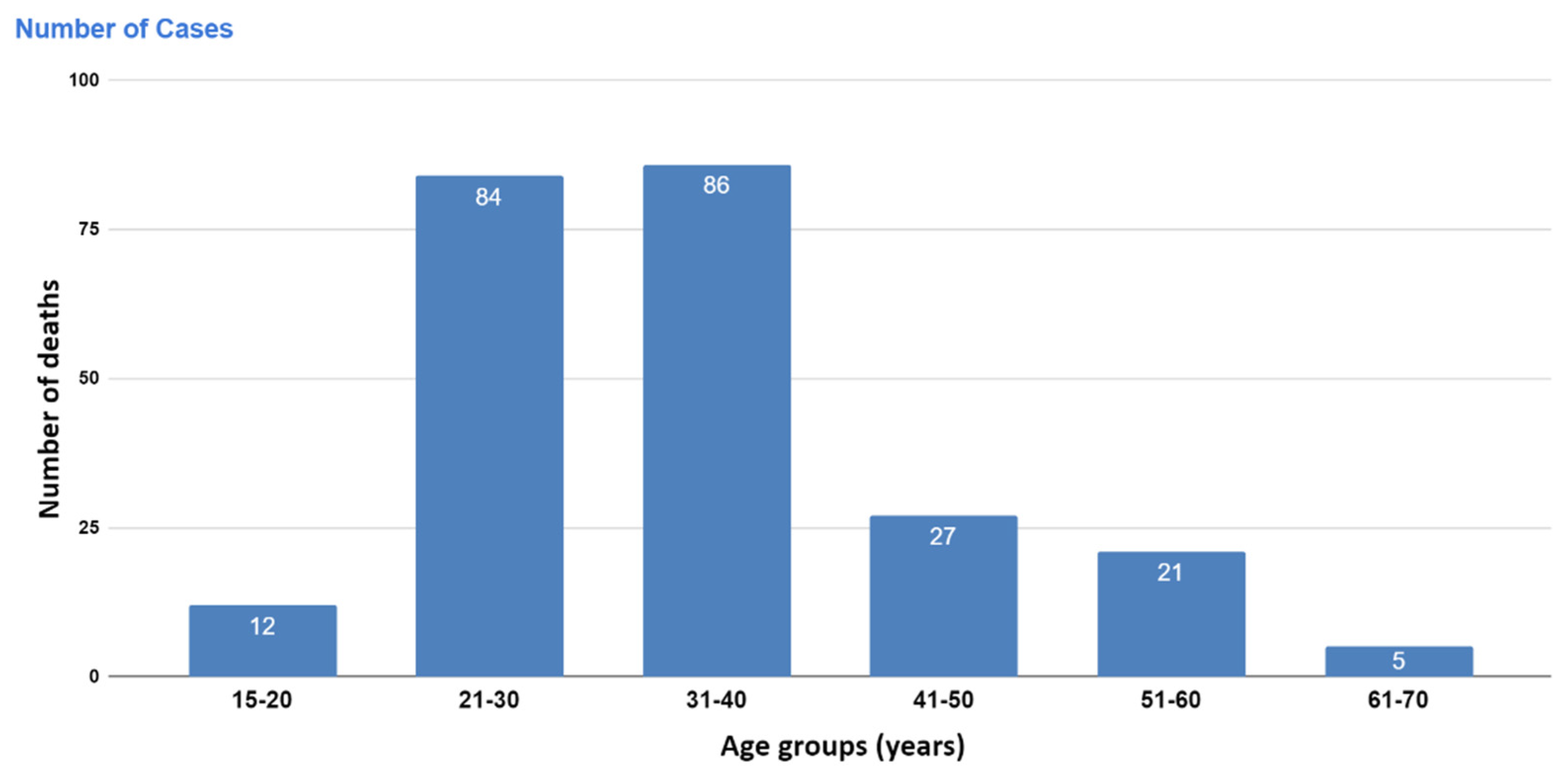
The highest number of cases was recorded for the group aged between 31 and 40 years (86 cases) and between 21 and 30 years (84 cases), whereas the lowest number of cases was recorded for the group aged between 61 and 70 years (5 cases) (Figure 1). An increase in the concentrations of amphetamines in BN and corresponding bodily fluids was observed with an increase in the age of the deceased, with a more than two-fold increase observed in the group of deceased patients older than 30 years compared with those younger than 30 years old. Table 2 displays the relationship between the amphetamine concentration in the amphetamine-related postmortem cases in different bodily fluid specimens and the age group.
3.3. Multiple Specimens
In this study, blood was collected from the subclavian artery (n = 187 cases, 80% of total cases). The second most tested specimen type was vitreous humor, which was available in 165 cases (70%); this was followed by urine samples, available in 152 cases (64%); stomach contents, available in 91 cases (38%); and bile samples, available in 88 cases (37%).
The relationship between amphetamine concentrations among multiple specimens has rarely been reported. In the current study, the Spearman correlation coefficient (Rs) was used to determine the relationship between amphetamine concentrations in different bodily fluids. Figure 2 clearly shows a positive relationship between the amphetamine levels in different bodily fluids (Rs, range = 0.553–0.867), and the p-values were always significant (p < 0.001). The highest Rs value was observed between the BN and vitreous humor samples, and the lowest Rs was observed between the BN samples and stomach contents (Figure 2, Table 3).
The median amphetamine concentration was 0.44 mg/L, 4.4 mg/L, 0.55 mg/L, 1.0 mg/L and 0.83 mg/L among the BN, urine, vitreous humor, stomach contents, and bile samples, respectively. The median urine/BN, vitreous humor/BN, stomach content/BN and bile/BN ratio of the detected amphetamine concentrations were 21:1, 1.1:1, 3.3:1, and 2.5:1, respectively.
In the current investigation, as indicated in Table 1, the highest median amphetamine concentration was found in urine samples, followed by stomach contents, bile, vitreous humor, and BN. This can be explained by the postmortem distribution of blood to other bodily fluids and tissue, accumulation in urine following multiple doses, and oral administration being the most common route of administration.
3.4. Causes of Death
Amphetamine is a recreational drug often detected in postmortem cases and rarely linked to the cause of death. Moreover, the combination of chronic amphetamine abuse and pre-existing disease has been reported [40]. In this investigation, amphetamines were the only detected drug in 107 cases (median BN concentration of 0.5 mg/L). Death was attributable to amphetamine intoxication (median BN concentration of 1.0 mg/L) in 37 cases (16% of all cases). In these cases, the median amphetamine concentrations were investigated in other bodily fluids and found to be ≥1.0 mg/L, as indicated in Table 1. In the current study, death was attributed to other co-ingested drugs in 53 (23%) cases, and the median amphetamine concentrations were often lower than 1.0 mg/L. Amphetamine concentration in the BN, vitreous humor, urine, stomach contents, and bile were 5-, 4-, 12-, 3-, and 3.3-fold higher, respectively, in cases of amphetamine-only-related death compared with cases in which death was attributed to co-ingested drugs.
In 22 cases, deaths were attributed to pre-existing diseases (9.4% of all cases), and the median amphetamine concentrations were higher in these cases than in those involving co-ingested-drug-related fatality cases but lower than amphetamine-only-related death cases, except for bile, for which amphetamine concentrations were similar to those of co-ingested-drug-related fatalities. In another 16 cases, the cause of death could not be determined due to a lack of information, as most were putrefied corpses and a few blood samples were available for testing, with a median concentration of 0.23 mg/L. In that group, high amphetamine concentrations were detected in urine, stomach contents, and bile specimens, with medians of 14.0, 1.7, and 4.3 mg/L, respectively. No vitreous humor samples were available in this group. Amphetamine concentrations in multiple bodily fluid specimens with the corresponding PMI, age, and cause of death are listed in Table 1.
3.5. Manner of Death
In the current investigation, cause of death can be divided into intentional (homicidal or suicidal), unintentional (accidental), and natural (deaths related to pre-existing diseases). In some cases, the manner of death could not be determined due to lack of information. Table 1 shows that the cause of death was accidental in 46% of cases. Homicide was the second most common manner of death in this investigation, accounting for 26% of total cases. Deaths were attributed to stabbing (20 cases), gunshot (15 cases), fighting (7 cases), vehicular assault (3 cases), fall from height (3 cases), and other causes (8 cases). Homicides were observed in both cases only involving amphetamines (39%) as well as polydrug cases (15%).
In the current study, the cause of death was suicide in 26 (11%) cases. Among the cases in which amphetamines were the only ingested drug (107 cases), suicides accounted for 17 cases (16%), while nine cases among polydrug cases (128 cases) were determined as suicide (7%). The most common method of suicide was hanging (18 cases, 69% of all suicides), followed by self-gunshot (11%), fall from height (8%), self-stabbing (8% cases), and self-immolation (reported in one case). In the current study, 9% of cases were due to natural causes, and cause of death was undetermined in 7% of cases. Interestingly, the median BN amphetamine concentration among cases of natural deaths was 0.70 mg/L, which is slightly lower than that of cases solely attributable to amphetamines (median: 1.0 mg/L). In 18 cases, the cause of death was unknown, as most putrefied cases in this study could not be assigned a definitive cause of death based on the available information. In addition, few BN or humor samples were available for testing. Instead, other biological fluids were investigated. The amphetamine concentrations, classed by cause of death, in multiple bodily fluid specimens, along with the corresponding PMI and age, are listed in Table 1.
3.6. Amphetamines and Polydrug Deaths
Among the 128 polydrug cases, the additional drugs detected included THC metabolites (45% of polydrug cases), methamphetamine (36%), heroin metabolites (24%), alcohol (17%), cocaine (3%), tramadol (1%), alprazolam (4%), diazepam (3%), olanzapine (2%), midazolam (2%), clonazepam (1%), carbon monoxide (6%), and sildenafil (6%). Table 1 shows the high BN amphetamine concentration in solely amphetamine-caused deaths, which could be interpreted in two different ways: it gives convincing evidence for chronic amphetamine abuse [34] and it confirms that the deceased had ingested large amounts of this stimulant [3]. In this study, the median BN amphetamine concentration was 1.0 mg/L and 0.2 mg/L in solely amphetamine and polydrug intoxication, respectively.
3.7. Route of Amphetamine Administration
In the current study, the most common route of administration was oral (174 cases, 74%), with a further 30 cases using intravenous injection (13%), whereas the route of administration was unavailable for 31 cases (13%). The route of amphetamine intake resulting in the highest BN (median concentration 0.52 mg/L) was oral. Amphetamine injection was determined as the route of injected in the fewest number of cases, with a median level of BN amphetamine concentration of 0.14 mg/L (Table 1).
Most of the cases with unknown routes of administration were putrefied cases. Of the cases with unknown routes of administration, 23% showed partial putrefaction and 71% were heavily decomposed. In these cases, amphetamine was detected in alternative specimens when no blood samples were available, with median levels of 0.32 mg/L in vitreous humor, 10.00 mg/L in urine, 1.24 mg/L in stomach contents, and 0.70 mg/L in bile.
3.8. Location of Deaths, Putrefaction, and Postmortem Intervals
In the current study, location of death was crucial to identification of the effects of environmental conditions (temperature and humidity) on amphetamine concentration in postmortem specimens. Outdoor locations of death were the most reported among cases in this investigation (58%). PMI was relatively low in non-putrefied cases (69%). In putrefied cases, 60% showed partial purification, with the remaining 40% in an advanced state of decomposition. Median BN amphetamine concentrations were higher in heavily decomposed cases than in partially decomposed cases (heavily decomposed: 0.44 mg/L, partially decomposed: 0.30 mg/L; Table 1).
Some outdoor cases had been transferred to a hospital, which increased the time between dose and death. Among outdoor deaths, the highest median amphetamine concentration was found in cases where the death occurred in the desert (1.30 mg/L); this was followed by hospitals (0.50 mg/L); open space, i.e., streets or gardens (0.40 mg/L); and car accidents (0.20 mg/L).
4. Discussion
4.1. Multiple Specimens
Few publications have reported amphetamine concentrations in different postmortem bodily fluids. In the current study, the advantage of analyzing different postmortem bodily fluids can be observed in the 48 putrefied cases for which no blood samples were available or deemed not suitable for analysis. The ratios of the median amphetamine concentrations among the different postmortem bodily fluids tested herein were always higher than 1:1. Blood is the most common postmortem sample studied for amphetamine. Previously reported amphetamine concentrations in blood ranged from 0.1 to 14.0 mg/L [14,15,16,22,33,34,41]. In three previous studies of amphetamine-related fatalities reported stomach content concentrations ranging between 2.1 and 22 mg/L total [16,41]. Stomach contents have been suggested to be valuable for distinguishing between oral routes of administration and other routes of administration, with higher concentrations in stomach contents than blood hypothesized to result from oral administration [19,29,31]. The ratio of the amphetamine concentration in stomach contents to blood has been previously reported to range 3–22 fold [16,41]. The ratios obtained in the current study were higher than previously reported, with a median of 3.3-fold (range: 0.3–60 fold). This can be explained by the high probability of oral administration compared to intravenous injections that occurred in most previous reports [34]. One of the strengths of the current study is the large number of stomach content specimens tested (91) compared to previous work.
Urine is a helpful matrix in this kind of analysis, especially in cases of delayed deaths (in which blood concentration drops sharply) and cases of bleeding or trauma. It allows confirmation of drug use over a much wider time window compared to blood. Urine samples have been examined for many amphetamine-related fatalities, with concentrations ranging from 0.4 to 775.0 mg/L, and the ratios of the amphetamine concentration in urine to blood ranging from 2 to 116 fold [13,14,16,17,33,41]. In the current study, the median ratio of amphetamine concentration in urine to BN was 21 fold (range: 1–247 fold), which is higher than previous reports.
Bile is used to identify chronic users [42]. There is no previous report of bile concentration in amphetamine-related deaths. However, it has been reported as a methamphetamine metabolite; in these reports, the ratios of amphetamine concentrations in bile to blood have ranged 1–5 fold [29,31,42]. In the current study, a higher ratio of amphetamine concentration in bile to BN was also observed (range: 1–46 fold) compared to previous reports, which may indicate that users in the current study were chronic amphetamine users.
Vitreous humor is known to eliminate drugs of abuse slower than other bodily fluids [43]; therefore, some of the detected concentration could include a previous dose. The amphetamine concentration in vitreous humor has only been previously reported in a single study (n = 5, median: 0.52 mg/L, range: 0.1–1.8 mg/L), while the median ratio of amphetamine concentration in vitreous humor to blood ranged 3–6 fold [41], which is in agreement with the results of this study (median: 1.1 fold, range: 3–6 fold).
4.2. Manners of Death
Most of the deaths for which amphetamine was detected occurred in those younger than 40 years old. Amphetamine abuse begins with no experience of drug-related complications and may be a trigger for abuse of other dangerous and harmful drugs, which may cause users to suffer poor health, eventually leading to death [43]. In agreement with current study, De Letter et al. reported a similar finding in their study, with 60% of deaths determined to be accidental, 26% determined as suicides, 6% determined as homicides, and 3% determined as undermined [41]. Verschraagen et al. found that almost 46% of their amphetamine-related fatalities were accidental, whereas 54% of their cases were violent homicides, i.e., gunshot, stabbing, or strangulation [22]. A similar study in Sweden found that amphetamines were most often detected incidentally and that most deaths were related to drug combinations [6]. In a Spanish study, accidental death was the most common cause of death (82%), followed by suicide (14%) and homicide (4%) [35]. Others found that 2–54% of amphetamine-related deaths involved homicide [22,33,44,45]. Similarly to the current study, amphetamine-related suicides in previous studies accounted for 11–26% of all amphetamine-related violent deaths [33,35,41]. Furthermore, 33–86% of amphetamine-related suicides used violent means [46]. In prior studies, the most common volent means of death was hanging (33–57%) [33,35,41], followed by gunshot (50%) [33], traffic accidents (29%), and stabbing (14%) [41].
In prior work, natural and undetermined causes of death have been reported in cases in which testing revealed the presence of amphetamines. In one study, somatic disease accounted for 14% of deaths, and 2% of the cases had undetermined causes of death [44]. Åhman et al. found that natural disease was the major cause of death in almost 40% of their postmortem cases. The authors attributed such a high rate of natural death to their long study period, which made it easy to distinguish deaths caused by natural diseases that developed with increasing age from those caused by amphetamine use [40]. This study had a similar percentage of undetermined cases as was reported by Ericsson et al. (8%) [44], but a higher percentage than that reported by De Letter et al. (3%) [41].
Several postmortem toxicology studies have tried to address the relationship between amphetamine concentration and violent behavior. The connection between crime and amphetamine use is obvious from the current study. Out of 235 cases, 97 (41%) had violent-behavior causes of death. Of these violent deaths, 66% resulted from the violent action of another, and 34% were considered violence against themselves. The median BN concentrations were slightly higher in those who harmed themselves: 0.45 mg/L versus 0.41 mg/L in those harmed by others. This trend held true in urine, vitreous humor, stomach contents, and bile. Even though these accidents and violent deaths were not directly caused by the drug, it is believed that because they occurred under the influence of amphetamines that they contributed to these deaths [26,34].
In this study, death due to somatic disease was associated with older age (median age, 45 years), which is in agreement with a previous report by Lee et al. [47]. In contrast, suicides were more common in younger individuals, with a median age of 30 years, also in agreement with previous reports [47,48]. In the current study, polydrug use that included amphetamines accounted for 35% of suicides, 31% of homicides, and 48% of accidents. Almost 44% of those who died as a result of car accidents in the current study were polydrug users, which is similar to data previously reported [3,49].
4.3. Amphetamines and Polydrug Deaths
Jones et al. presented a total of 419 postmortem cases, among which only 36 were amphetamine-related deaths (9%). Of these 36 cases, 50% were amphetamine-related intoxication, 8% were suicide by overdose, while amphetamines were detected in combination with disease in 11% [49]. In a Holmgren and Lindquist study, 40% of amphetamine-related fatalities were related to the combined toxicity of amphetamines and additional drugs and 9% had pre-existing cardiac diseases that contributed to the deaths [33]. These published conclusions are in agreement with the details of the current investigation.
In published reports, the median blood amphetamine concentration was 0.7–1.5 mg/L when only amphetamine was detected and 0.4–0.5 mg/L when at least one other drug was detected [3,6,34]. As reported by Jones et al. [34], there appeared to be a dose effect with the blood amphetamine concentration decreasing more with higher numbers of detected drugs. For example, a median concentration of 1.2 mg/L was reported when amphetamine was detected alongside one extra drug. This concentration further decreased to 0.2 mg/L when the number of other drugs in the blood increased to 10 [34]. In the current study, the median amphetamine concentrations also decreased when a greater number of drugs were involved. The median BN amphetamine concentration was 0.4 mg/L when only one extra drug was detected, 0.25 mg/L when two additional drugs were detected, and 0.12 mg/L when more than four drugs were detected.
In previous reports, THC co-occurred in 26–33% of amphetamine-related postmortem cases [3,6,41], alcohol co-occurred in 13–48% [3,6,21,41], cocaine co-occurred in 19–21% [35,41], and benzodiazepines co-occurred in 37–43% [3,6,41]. Cannabinoids were found in 58 of the 235 cases in this study (25% of total cases), followed by methamphetamines. Amphetamines are known to be active methamphetamine metabolites [50,51]. In several studies, the percentage of amphetamine concentration compared with its parent drug was estimated to be within 5–10% of the methamphetamine concentration in BN samples [26,52]. In prior reports, the postmortem percentage of amphetamine to methamphetamine varied based on the route of administration, time of administration, and purity of amphetamines used, ranging from 1 to 15% [33,41,50,51]. In some amphetamine-related postmortem cases, a low methamphetamine concentration could be due to methamphetamine’s presence as an impurity of amphetamine synthesis, or methamphetamine could be formed by a minor metabolic pathway of amphetamine methylation due to its high concentration [53]. A methamphetamine percentage higher than 10% may indicate that both drugs were used. In a recent study from Saudi Arabia of cases known to be related to methamphetamine intoxication, the median amphetamine/methamphetamine percentage was higher than 50% among cases, in which the authors supposed that both drugs were administrated [38].
In current investigation, heroin co-ingestions in addition to amphetamines accounted for 13% of all cases (n = 31, median amphetamine BN concentration of 0.2 mg/L). In a previous report, 29% of amphetamine-related fatalities were in combination with morphine [35]. In one previous study, heroin contributed to the death in 3 of the 19 amphetamine-related fatalities (16%), and blood amphetamine concentrations ranged from 0.05 to 0.09 mg/L [54].
4.4. Route of Amphetamine Administration
Few reports have discussed the route of amphetamine administration in amphetamine-related fatalities. In those that did, the most reported route of amphetamine administration was reported to be injection [3,6,14,16,17]. Oral routes of amphetamine administration have only been investigated in two previous studies [15,19]. Our study increases our knowledge of cases of oral amphetamine administration, which has not been the main route of administration reported in previous investigations.
4.5. Location of Deaths
The influence of the location of death on drug concentrations, whether in indoor residences or in an outdoor setting, has rarely been discussed for amphetamine-related postmortem cases. In previous reports, the median BN amphetamine concentrations ranged from 0.12 to 0.38 mg/L in indoor cases and from 0.10 to 0.27 mg/L in outdoor cases [34,42]. In the current investigation, the median amphetamine concentrations in different bodily fluids were higher in outdoor cases than indoor cases (Table 1), which is consistent with other reports [33,41].
5. Conclusions
We conclude that amphetamine-related postmortem cases in Jeddah, Saudi Arabia, increased more than 400% over the seven-year study period. This can be dangerous because of the high mortality associated with poly-drug intoxication. Poly-drug intoxication was involved in 23% of all cases in this study, and 41% of amphetamine-related postmortem cases involved violence. The high death rate among amphetamine users indicates that this is a serious problem in Saudi Arabia, which may continue to increase in the coming years. We found that amphetamine abusers died young and often began amphetamine abuse before the age of 20 years. The highest rate of death was reported for the group aged between 21 and 40 years, indicating a long period of amphetamine abuse, although the role of pre-existing disease cannot be excluded. This result also suggests that preventive programs targeting youth and adolescent students are required to keep schools and universities free from drugs, especially amphetamines.
Author Contributions
Conceptualization, A.I.A.-A.; methodology, A.I.A.-A. and A.E.A.-Z.; software, T.A.Z. and A.I.A.-A.; validation, A.I.A.-A., F.D.A.-S. and A.E.A.-Z.; formal analysis, F.D.A.-S. and A.E.A.-Z.; investigation, A.I.A.-A. and A.E.A.-Z.; resources, F.D.A.-S. and A.E.A.-Z.; data curation, A.I.A.-A., A.E.A.-Z. and T.A.Z.; writing—original draft preparation, A.I.A.-A.; writing—review and editing, A.I.A.-A. and T.A.Z.; visualization, A.I.A.-A. and T.A.Z.; supervision, A.I.A.-A.; project administration, A.I.A.-A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
All forensic autopsy cases of drug-related deaths submitted to the Jeddah Poison Control and Forensic Medical Chemistry Center were investigated as part of the investigation into medico-legal cases-Jeddah Health Affairs Ethical Approval Committee, research code: 00188 (6 June 2014).
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
The authors would like to thank all the staff at the Forensic Toxicology department-Jeddah Poison Control and Forensic Medical Chemistry Center for supporting this work.
Conflicts of Interest
The authors have no conflict of interest to declare.
References
- Stockings, E.; Tran, L.T.; Santo, T., Jr.; Peacock, A.; Larney, S.; Santomauro, D.; Farrell, M.; Degenhardt, L. Mortality among people with regular or problematic use of amphetamines: A systematic review and meta-analysis. Addiction 2019, 114, 1738–1750. [Google Scholar] [CrossRef]
- Singleton, J.; Degenhardt, L.; Hall, W.; Zabransky, T. Mortality among amphetamine users: A systematic review of cohort studies. Drug Alcohol Depend. 2009, 105, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.W.; Holmgren, A.; Ahlner, J. High prevalence of previous arrests for illicit drug use and/or impaired driving among drivers killed in motor vehicle crashes in Sweden with amphetamine in blood at autopsy. Int. J. Drug Policy 2015, 26, 790–793. [Google Scholar] [CrossRef] [PubMed]
- UNODC. World Drug Report. 2018. Available online: https://www.unodc.org/wdr2018/prelaunch/WDR18_Booklet_1_EXSUM.pdf (accessed on 9 October 2019).
- Katselou, M.; Papoutsis, I.; Nikolaou, P.; Qammaz, S.; Spiliopoulou, C.; Athanaselis, S. Fenethylline (Captagon) Abuse—Local Problems from an Old Drug Become Universal. Basic Clin. Pharmacol. Toxicol. 2016, 119, 133–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, A.W.; Holmgren, A. Amphetamine Abuse in Sweden Subject Demographics, Changes in Blood Concentrations over Time, and the Types of Coingested Substances. J. Clin. Psychopharmacol. 2013, 33, 248–252. [Google Scholar] [CrossRef]
- Aljohar, H.I.; Abuhaimed, S.N.; Maher, H.M.; Nafisan, B.A.; Alkhalaf, A.M. Gas chromatography tandem mass spectrometry for the screening of adulterants in seized captagon (TM) tablets. J. Liq. Chromatogr. Relat. Technol. 2019, 42, 358–366. [Google Scholar] [CrossRef]
- Alhelail, M.; Alsairafi, R.; Alsairafi, A.; Qadhi, R. Body stuffer case report and literature review. Indo Am. J. Pharm. Sci. 2019, 6, 4013–4019. [Google Scholar] [CrossRef]
- Alabdalla, M.A. Chemical characterization of counterfeit captagon tablets seized in Jordan. Forensic Sci. Int. 2005, 152, 185–188. [Google Scholar] [CrossRef]
- Al-Asmari, A.I. Method for the identification and quantification of sixty drugs and their metabolites in postmortem whole blood using liquid chromatography tandem mass spectrometry. Forensic Sci. Int. 2020, 309, 110193. [Google Scholar] [CrossRef]
- Dabbagh, R.; Rawson, R. Captagon Use in Saudi Arabia: What Do we Know? Int. Addict. Rev. 2019, 2, 22–30. [Google Scholar]
- Moffat, A.C. Clarke’s Analysis of Drugs and Poisons: In Pharmaceuticals, Body Fluids and Postmortem Material, 4th ed.; Moffat, A.C., Osselton, M.D., Widdop, B., Watts, J., Eds.; Pharmaceutical: London, UK, 2011. [Google Scholar]
- Baselt, R.C.; Cravey, R.H. Amphetamine. In Disposition of Toxic Drugs and Chemicals in Man, 8th ed.; Baselt, R.C., Ed.; Biomedical Publications: Foster City, CA, USA, 2008; pp. 83–86. [Google Scholar]
- Orrenius, S.; Maehly, A.C. Lethal amphetamine intoxication. A report of three cases. Z. Fur Rechtsmedizin. J. Leg. Med. 1970, 67, 184–189. [Google Scholar] [CrossRef]
- Richards, H.G.; Stephens, A. Sudden death associated with the taking of amphetamines by an asthmatic. Med. Sci. Law 1973, 13, 35–38. [Google Scholar] [CrossRef] [PubMed]
- van Hoof, F.; Heyndrickx, A.; Timperman, J. Report of a human fatality due to amphetamine. Arch. Toxicol. 1974, 32, 307–312. [Google Scholar] [CrossRef] [PubMed]
- Adjutantis, G.; Coutselinis, A.; Dimopoulous, G. Fatal intoxication with amphetamines (a case report). Med. Sci. Law 1975, 15, 62–63. [Google Scholar] [CrossRef] [Green Version]
- Meyer, E.; VanBocxlaer, J.F.; Dirinck, I.M.; Lambert, W.E.; Thienpont, L.; DeLeenheer, A.P. Tissue distribution of amphetamine isomers in a fatal overdose. J. Anal. Toxicol. 1997, 21, 236–239. [Google Scholar] [CrossRef] [Green Version]
- Heinemann, A.; Miyaishi, S.; Iwersen, S.; Schmoldt, A.; Puschel, K. Body-packing as cause of unexpected sudden death. Forensic Sci. Int. 1998, 92, 1–10. [Google Scholar] [CrossRef]
- Cox, D.E.; Williams, K.R. “ADAM’ or “EVE’?—A toxicological conundrum. Forensic Sci. Int. 1996, 77, 101–108. [Google Scholar] [CrossRef]
- Jones, A.W.; Holmgren, A. Abnormally high concentrations of amphetamine in blood of impaired drivers. J. Forensic Sci. 2005, 50, 1215–1220. [Google Scholar] [CrossRef]
- Verschraagen, M.; Maes, A.; Ruiter, B.; Bosman, I.J.; Smink, B.E.; Lusthof, K.J. Post-mortem cases involving amphetamine-based drugs in the Netherlands: Comparison with driving under the influence cases. Forensic Sci. Int. 2007, 170, 163–170. [Google Scholar] [CrossRef]
- Pilgrim, J.L.; Gerostamoulos, D.; Drummer, O.H.; Bollmann, M. Involvement of Amphetamines in Sudden and Unexpected Death. J. Forensic Sci. 2009, 54, 478–485. [Google Scholar] [CrossRef]
- Shearer, K.; McAdam, J.; Parsons, M. Drug levels in fatal cases where death was not directly attributable to drug toxicity. Forensic Toxicol. 2020, 38, 536–541. [Google Scholar] [CrossRef]
- Kojima, T.; Une, I.; Yashiki, M.; Noda, J.; Sakai, K.; Yamamoto, K. A fatal methamphetamine poisoning associated with hyperpyrexia. Forensic Sci. Int. 1984, 24, 87–93. [Google Scholar] [CrossRef]
- Logan, B.K.; Fligner, C.L.; Haddix, T. Cause and manner of death in fatalities involving methamphetamine. J. Forensic Sci. 1998, 43, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Karch, S.B.; Stephens, B.G.; Ho, C.H. Methamphetamine-related deaths in San Francisco: Demographic, pathologic, and toxicologic profiles. J. Forensic Sci. 1999, 44, 359–368. [Google Scholar] [CrossRef]
- Moriya, F.; Hashimoto, Y. A case of fatal hemorrhage in the cerebral ventricles following intravenous use of methamphetamine. Forensic Sci. Int. 2002, 129, 104–109. [Google Scholar] [CrossRef]
- Kiely, E.; Lee, C.J.; Marinetti, L. A Fatality from an Oral Ingestion of Methamphetamine. J. Anal. Toxicol. 2009, 33, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Tominaga, M.; Michiue, T.; Oritani, S.; Ishikawa, T.; Maeda, H. Evaluation of Postmortem Drug Concentrations in Bile Compared with Blood and Urine in Forensic Autopsy Cases. J. Anal. Toxicol. 2016, 40, 367–373. [Google Scholar] [CrossRef] [Green Version]
- Wurita, A.; Hasegawa, K.; Minakata, K.; Gonmori, K.; Nozawa, H.; Yamagishi, I.; Suzuki, O.; Watanabe, K. Postmortem redistribution of methamphetamine and amphetamine in blood specimens from various blood vessels and in the specimens from pericardial fluid, bile, stomach contents and various solid tissues collected from a human cadaver. Forensic Toxicol. 2016, 34, 191–198. [Google Scholar] [CrossRef]
- Wiergowski, M.; Anand, J.S.; Krzyżanowski, M.; Jankowski, Z. Acute methoxetamine and amphetamine poisoning with fatal outcome: A case report. Int. J. Occup. Med. Environ. Health 2014, 27, 683–690. [Google Scholar] [CrossRef] [Green Version]
- Holmgren, P.; Lindquist, O. Lethal intoxications with centrally stimulating amines in Sweden 1966–1973. Z. Fur Rechtsmedizin. J. Leg. Med. 1975, 75, 265–273. [Google Scholar] [CrossRef]
- Jones, A.W.; Holmgren, A.; Ahlner, J. Quantitative analysis of amphetamine in femoral blood from drug-poisoning deaths compared with venous blood from impaired drivers. Bioanalysis 2011, 3, 2195–2204. [Google Scholar] [CrossRef] [PubMed]
- Lora-Tamayo, C.; Tena, T.; Rodríguez, A. Amphetamine derivative related deaths. Forensic Sci. Int. 1997, 85, 149–157. [Google Scholar] [CrossRef]
- Rohrig, T.P.; Hicks, C.A. Brain Tissue: A Viable Postmortem Toxicological Specimen. J. Anal. Toxicol. 2015, 39, 137–139. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.W.; Holmgren, A.; Ahlner, J. Post-mortem concentrations of drugs determined in femoral blood in single-drug fatalities compared with multi-drug poisoning deaths. Forensic Sci. Int. 2016, 267, 96–103. [Google Scholar] [CrossRef] [PubMed]
- Al-Asmari, A.I. Methamphetamine-related postmortem cases in Jeddah, Saudi Arabia. Forensic Sci. Int. 2021, 321, 110746. [Google Scholar] [CrossRef]
- American Academy of Forensic Sciences Standards Board 2019. ANSI/ASB Standard 036; Method Validation in Forensic Toxicology. American Academy of Forensic Sciences: Colorado Springs, CO, USA. Available online: https://www.aafs.org/sites/default/files/media/documents/036_Std_e1.pdf (accessed on 15 January 2022).
- Åhman, A.; Jerkeman, A.; Blomé, M.A.; Björkman, P.; Håkansson, A. Mortality and causes of death among people who inject amphetamine: A long-term follow-up cohort study from a needle exchange program in Sweden. Drug Alcohol Depend. 2018, 188, 274–280. [Google Scholar] [CrossRef]
- De Letter, E.A.; Piette, M.H.; Lambert, W.E.; Cordonnier, J.A. Amphetamines as potential inducers of fatalities: A review in the district of Ghent from 1976–2004. Med. Sci. Law 2006, 46, 37–65. [Google Scholar] [CrossRef]
- Kinoshita, H.; Takakura, A.; Kumihashi, M.; Jamal, M.; Tsutsui, K.; Kimura, S.; Ameno, K.; Matsubara, S.; Tanaka, N. Bile as a complementary matrix for methamphetamine testing, an autopsy case of methamphetamine poisoning. Rom. J. Leg. Med. 2019, 27, 379–381. [Google Scholar] [CrossRef]
- Thierauf, A.; Kempf, J.; Perdekamp, M.G.; Auwarter, V.; Gnann, H.; Wohlfarth, A.; Weinmann, W. Ethyl sulphate and ethyl glucuronide in vitreous humor as postmortem evidence marker for ethanol consumption prior to death. Forensic Sci. Int. 2011, 210, 63–68. [Google Scholar] [CrossRef]
- Ericsson, E.; Bradvik, L.; Hakansson, A. Mortality, Causes of Death and Risk Factors for Death among Primary Amphetamine Users in the Swedish Criminal Justice System. Subst. Use Misuse 2014, 49, 262–269. [Google Scholar] [CrossRef]
- Darke, S. The toxicology of homicide offenders and victims: A review. Drug Alcohol Rev. 2010, 29, 202–215. [Google Scholar] [CrossRef] [PubMed]
- Darke, S.; Kaye, S.; Duflou, J.; Lappin, J. Completed Suicide among Methamphetamine Users: A National Study. Suicide Life-Threat. Behav. 2019, 49, 328–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, D.Y.; Delcher, C.; Maldonado-Molina, M.M.; Thogmartin, J.R.; Goldberger, B.A. Manners of Death in Drug-Related Fatalities in Florida. J. Forensic Sci. 2016, 61, 735–742. [Google Scholar] [CrossRef]
- Stenbacka, M.; Leifman, A.; Romelsjö, A. Mortality and cause of death among 1705 illicit drug users: A 37 year follow up. Drug Alcohol Rev. 2010, 29, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Holmgren, A.; Holmgren, P.; Kugelberg, F.C.; Jones, A.W.; Ahlner, J. Predominance of illicit drugs and poly-drug use among drug-impaired drivers in Sweden. Traffic Inj. Prev. 2007, 8, 361–367. [Google Scholar] [CrossRef] [PubMed]
- Degenhardt, L.; Topp, L. ‘Crystal meth’ use among polydrug users in Sydney’s dance party subculture: Characteristics, use patterns and associated harms. Int. J. Drug Policy 2003, 14, 17–24. [Google Scholar] [CrossRef]
- Prakobsrikul, P.; Srisont, S.; Jinawath, A.; Boonkrem, M. Methamphetamine-related post-mortem cases in Bangkok, Thailand. Med. Sci. Law 2019, 59, 164–170. [Google Scholar] [CrossRef]
- Kojima, T.; Une, I.; Yashiki, M. CI-mass fragmentographic analysis of methamphetamine and amphetamine in human autopsy tissues after acute methamphetamine poisoning. Forensic Sci. Int. 1983, 21, 253–258. [Google Scholar] [CrossRef]
- Jemionek, J.F.; Addison, J.; Past, M.R. Low concentrations of methamphetamine detectable in urine in the presence of high concentrations of amphetamine. J. Anal. Toxicol. 2009, 33, 170–173. [Google Scholar] [CrossRef] [Green Version]
- Madea, B.; Wagner, R.; Markwerth, P.; Doberentz, E. Heat shock protein expression in cardiac tissue in amphetamine-related deaths. Rom. J. Leg. Med. 2017, 25, 8–13. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Distribution of the postmortem cases with positive amphetamine results, by age group.

Figure 2.
Correlation (Spearman-Rho) between the concentrations of amphetamine (mg/L) in amphetamine-related postmortem cases in the current investigation: (a) in blood with sodium fluoride preservative and urine; (b) in blood with sodium fluoride preservative and vitreous humor; (c) in blood with sodium fluoride preservative and stomach contents; and (d) in blood with sodium fluoride preservative and bile.
Figure 2.
Correlation (Spearman-Rho) between the concentrations of amphetamine (mg/L) in amphetamine-related postmortem cases in the current investigation: (a) in blood with sodium fluoride preservative and urine; (b) in blood with sodium fluoride preservative and vitreous humor; (c) in blood with sodium fluoride preservative and stomach contents; and (d) in blood with sodium fluoride preservative and bile.


{kind=link}
{kind=link}
Table 1.
Characteristics of the amphetamine-related postmortem cases in Jeddah, Saudi Arabia, 2012–2018, based on age and postmortem interval as well as the cause, manner, and location of death.
Table 1.
Characteristics of the amphetamine-related postmortem cases in Jeddah, Saudi Arabia, 2012–2018, based on age and postmortem interval as well as the cause, manner, and location of death.
| Circumstances of Death | Number of Cases | Age (Year) | Postmortem Interval (Hours) | Amphetamine Concentration (mg/L) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| BN § | Urine | Vitreous Humor | Stomach Contents | Bile | |||||||
| Amphetamine-related postmortem cases | All cases | All cases | 235 | Median | 35 | 24 | 0.4 | 4.4 | 0.55 | 1.00 | 0.83 |
| Range | 15–70 | 12–2664 | 0.05–11.00 | 0.10–475.4 | 0.05–7.90 | 0.06–26.60 | 0.05–44.50 | ||||
| Amphetamine only detected | All | 107 | Median | 35 | 48.0 | 0.54 | 9.70 | 0.67 | 0.96 | 1.31 | |
| Range | 15–70 | 15–1080 | 0.05–4.35 | 0.20–475.40 | 0.08–6.40 | 0.06–11.74 | 0.10–44.50 | ||||
| Other drugs plus Amphetamine | 128 | Median | 33 | 24 | 0.26 | 2.45 | 0.31 | 0.90 | 0.42 | ||
| Range | 16–66 | 12–2664 | 0.05–11.00 | 0.10–323.20 | 0.05–7.90 | 0.10–26.60 | 0.05–24.60 | ||||
| Cause of Deaths | Amphetamine-only | All cases | 37 | Median | 36 | 24 | 1.0 | 18.94 | 1.0 | 2.20 | 3.03 |
| Range | 20–57 | 24–2664 | 0.51–4.35 | 0.30–475.40 | 0.30–6.40 | 0.15–26.60 | 0.63–16.61 | ||||
| Polydrug intoxication | All cases | 53 | Median | 36 | 24 | 0.20 | 1.63 | 0.24 | 0.70 | 0.90 | |
| Range | 17–63 | 12–240 | 0.10–11.00 | 0.10–185.60 | 0.06–7.90 | 0.1–95.50 | 0.10–24.60 | ||||
| Natural diseases | All cases | 22 | Median | 45 | 24 | 0.67 | 4.05 | 0.60 | 0.85 | 0.84 | |
| Range | 23–66 | 24–768 | 0.10–2.94 | 0.30–128.54 | 0.10–2.56 | 0.80–2.60 | 0.80–0.90 | ||||
| Undetermined deaths | All cases | 16 | Median | 38 | 134 | 0.23 | 14.00 | n.a. | 1.70 | 4.30 | |
| Range | 20–55 | 24–1080 | 0.10–0.35 | 10.00–17.74 | 0.19 | 0.06–3.62 | 0.76–7.80 | ||||
| Manner of Deaths | Accidental | All cases | 110 | Median | 36 | 24 | 0.50 | 2.65 | 0.61 | 1.10 | 1.00 |
| Range | 17–63 | 12–2664 | 0.10–11.00 | 0.10–475.40 | 0.06–7.90 | 0.07–26.70 | 0.05–44.53 | ||||
| Drug poisoning | 90 | Median | 37 | 24 | 0.53 | 4.60 | 0.63 | 1.14 | 1.40 | ||
| Range | 17–63 | 12–2664 | 0.10–11.00 | 0.10–475.40 | 0.06–7.90 | 0.10–26.60 | 0.09–24.60 | ||||
| Traffic accidents | 9 | Median | 26 | 48 | 0.35 | 1.45 | 0.37 | 0.40 | 0.30 | ||
| Range | 17–40 | 18–96 | 0.05–2.44 | 0.13–18.04 | 0.13–1.31 | 0.07–3.10 | 0.10–2.14 | ||||
| Fall from height | 10 | Median | 35 | 24 | 0.30 | 1.80 | 0.48 | 0.60 | 0.50 | ||
| Range | 22–50 | 24–288 | 0.10–0.95 | 0.30–68.40 | 0.12–2.82 | 0.20–3.53 | 0.13–1.25 | ||||
| Drowning | 3 | Median | 24 | 48 | 1.85 | n.a * | 3.30 | n.s. # | n.s. | ||
| Range | 20–33 | 34–72 | 1.68–2.01 | 0.33–323.23 | 1.80–4.90 | n.s. | n.s. | ||||
| Suicidal | All cases | 26 | Median | 30 | 24 | 0.36 | 5.40 | 0.31 | 0.55 | 0.50 | |
| Range | 16–70 | 12–480 | 0.05–1.20 | 0.15–90.92 | 0.05–1.00 | 0.07–4.10 | 0.09–2.34 | ||||
| Violent means | Hanging | 18 | Median | 29 | 24 | 0.41 | 4.02 | 0.30 | 0.13 | 0.20 | |
| Range | 21–40 | 12–480 | 0.15–0.52 | 0.15–82.60 | 0.05–1.00 | 0.07–0.27 | 0.09–2.34 | ||||
| Gunshot | 3 | Median | 37 | 24 | 0.28 | 27.00 | 0.38 | 0.60 | n.a | ||
| Range | 29–40 | 24–120 | 0.28–1.15 | 18.60–90.82 | 0.34–0.42 | 0.55–0.64 | 0.14 | ||||
| Homicidal | All | 61 | Median | 30 | 24 | 0.43 | 5.00 | 0.55 | 0.90 | 0.67 | |
| Range | 15–63 | 18–192 | 0.06–3.85 | 0.12–167.80 | 0.06–2.35 | 0.21–8.06 | 0.10–44.53 | ||||
| Stabbing | 20 | Median | 29 | 24 | 0.50 | 4.40 | 0.45 | 0.55 | 0.60 | ||
| Range | 17–60 | 22–120 | 0.06–3.06 | 0.20–89.20 | 0.06–1.20 | 0.21–4.80 | 0.13–4.03 | ||||
| Gunshot | 15 | Median | 31 | 24 | 0.41 | 5.60 | 0.20 | 0.56 | 0.59 | ||
| Range | 25–63 | 18–72 | 0.07–3.64 | 0.31–16.80 | 0.08–2.30 | 0.45–8.06 | 0.10–1.34 | ||||
| Blunt force injury | 8 | Median | 37 | 36 | 0.73 | 5.40 | 0.88 | 1.80 | 9.83 | ||
| Range | 27–60 | 24–192 | 0.10–3.47 | 0.81–32.04 | 0.06–1.75 | 0.50–4.75 | 2.23–19.20 | ||||
| Fight | 7 | Median | 26 | 24 | 0.12 | 5.00 | 0.33 | 0.96 | 1.55 | ||
| Range | 18–42 | 24–48 | 0.06–0.40 | 0.12–22.60 | 0.08–1.61 | 0.29–5.54 | 0.200–19.43 | ||||
| Car related homicide | 3 | Median | 28 | 24 | 0.35 | 0.85 | 1.85 | n.s. | n.s. | ||
| Range | 15–32 | 24–72 | 0.35–3.85 | 0.23–24.13 | 1.36–2.35 | n.s. | n.s. | ||||
| Others | 8 | Median | 27 | 84 | 1.60 | n.a. | 0.85 | 3.14 | 0.28 | ||
| Range | 21–42 | 24–456 | 0.74–2.44 | 1.40 | 0.71–0.98 | 1.92–6.00 | 0.22–0.45 | ||||
| Unknown | All cases | 18 | Median | 36 | 96 | n.a | 11.5 | n.a | 1.2 | 4.3 | |
| Range | 25–55 | 24–1080 | n.a | 6.3–17.7 | n.a | 0.1–3.6 | 0.8–7.8 | ||||
| Route of administration | Oral | 174 | Median | 34 | 24 | 0.52 | 5.40 | 0.62 | 1.00 | 0.90 | |
| Range | 15–70 | 12–2664 | 0.10–11.00 | 0.12–475.40 | 0.05–6.40 | 0.13–26.60 | 0.05–24.62 | ||||
| Injection | 30 | Median | 36 | 24 | 0.14 | 2.04 | 0.17 | 0.70 | 0.47 | ||
| Range | 18–56 | 24–96 | 0.05–0.70 | 0.10–70.31 | 0.06–7.90 | 0.13–6.60 | 0.26–2.00 | ||||
| Unknown | 31 | Median | 38 | 96 | 0.16 | 10.00 | 0.32 | 1.24 | 0.70 | ||
| Range | 20–60 | 12–1080 | 0.09–0.53 | 1.100–18.74 | 0.20–0.39 | 0.06–3.63 | 0.13–44.50 | ||||
| Location of deaths | Home environment | 99 | Median | 36 | 24 | 0.34 | 4.00 | 0.30 | 0.70 | 0.60 | |
| Range | 16–66 | 12–480 | 0.05–4.05 | 0.12–175.74 | 0.06–6.40 | 0.03–11.74 | 0.09–19.43 | ||||
| Public location | 136 | Median | 35 | 24 | 0.40 | 5.80 | 0.63 | 1.25 | 0.94 | ||
| Range | 15–70 | 18–2664 | 0.05–11.00 | 0.10–475.40 | 0.06–7.90 | 0.07–26.60 | 0.07–44.50 | ||||
| Hospital | 21 | Median | 36 | 24 | 0.50 | 2.80 | 0.61 | 0.70 | 0.40 | ||
| Range | 25–57 | 18–120 | 0.13–4.33 | 0.30–475.40 | 0.13–5.50 | 0.35–9.60 | 0.10–4.35 | ||||
| Cars | 26 | Median | 29 | 48 | 0.35 | 1.50 | 0.45 | 0.90 | 0.36 | ||
| Range | 15–56 | 18–240 | 0.05–3.85 | 0.13–185.60 | 0.06–2.35 | 0.07–5.90 | 0.10–13.60 | ||||
| The desert | 22 | Median | 40 | 96 | 1.30 | 31.20 | 0.70 | 4.22 | 7.80 | ||
| Range | 21–60 | 24–2664 | 0.11–8.20 | 1.80–185.60 | 0.40–2.03 | 0.90–22.31 | 0.90–44.50 | ||||
| Street/open area | 69 | Median | 35 | 24 | 0.51 | 6.40 | 0.70 | 1.20 | 1.50 | ||
| Range | 15–63 | 18–432 | 0.05–3.85 | 0.10–323.23 | 0.06–7.90 | 0.13–26.60 | 0.13–14.80 | ||||
| Putrefaction | Putrefied cases | All | 73 | Median | 37 | 96 | 0.43 | 5.00 | 0.44 | 1.14 | 0.93 |
| Range | 19–70 | 24–2664 | 0.05–11.00 | 0.12–185.60 | 0.07–7.90 | 0.06–22.31 | 0.07–44.50 | ||||
| Some | 43 | Median | 35 | 72 | 0.31 | 1.70 | 0.51 | 0.70 | 1.00 | ||
| Range | 19–70 | 24–480 | 0.05–3.50 | 0.12–185.60 | 0.07–7.90 | 0.10–22.31 | 0.10–19.20 | ||||
| Heavy | 30 | Median | 40 | 168 | 0.44 | 22.20 | 0.37 | 1.24 | 0.76 | ||
| Range | 21–60 | 24–2664 | 0.20–8.20 | 10.00–36.40 | 0.12–0.50 | 0.06–3.63 | 0.07–44.50 | ||||
| Non-putrefied | All | 163 | Median | 33 | 24 | 0.44 | 4.40 | 0.60 | 0.91 | 0.80 | |
| Range | 15–66 | 12–384 | 0.05–4.35 | 0.10–475.40 | 0.05–6.40 | 0.13–26.60 | 0.09–19.43 | ||||
§ BN: blood with sodium fluoride; * n.a: not available; # n.s: no sample.
Table 2.
The relationship between the amphetamine concentration in amphetamine-related postmortem cases in the bodily fluid specimens and age group.
Table 2.
The relationship between the amphetamine concentration in amphetamine-related postmortem cases in the bodily fluid specimens and age group.
| Age Group | Number of Cases | Specimen’s Type | ||||
|---|---|---|---|---|---|---|
| BN * | Urine | VH Ҿ | ST # | Bile | ||
| (Years) | Median Amphetamine Concentration (mg/L) | |||||
| 15–20 | 12 | 0.12 | 1.5 | 0.31 | 2.72 | 0.41 |
| 21–30 | 84 | 0.15 | 5 | 0.44 | 0.9 | 0.95 |
| 31–40 | 86 | 0.33 | 6.3 | 0.7 | 1.2 | 0.8 |
| 41–50 | 27 | 0.20 | 3.4 | 0.45 | 0.83 | 0.4 |
| 51–60 | 21 | 0.44 | 1.6 | 0.63 | 1.3 | 1.1 |
| 61–70 | 5 | 0.35 | 5.9 | 0.4 | 0 | 0.8 |
* BN: blood with sodium fluoride; Ҿ VH: vitreous humor; # ST: stomach contents.
Table 3.
Correlation (Spearman-Rho) between the amphetamine concentration detected in 235 amphetamine-related postmortem cases.
Table 3.
Correlation (Spearman-Rho) between the amphetamine concentration detected in 235 amphetamine-related postmortem cases.
| Specimen’s Type | BN | Urine | VH Ҿ | ST # | Bile |
|---|---|---|---|---|---|
| BN * | 1 | ||||
| Urine | 0.722 | 1 | |||
| VH | 0.867 | 0.635 | 1 | ||
| ST | 0.800 | 0.562 | 0.703 | 1 | |
| Bile | 0.778 | 0.747 | 0.801 | 0.739 | 1 |
* BN: blood with sodium fluoride; Ҿ VH: vitreous humor; # ST: stomach contents.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Al-Asmari, A.I.; Al-Solami, F.D.; Al-Zahrani, A.E.; Zughaibi, T.A. Post-Mortem Quantitation of Amphetamine in Cadaveric Fluids in Saudi Arabia. Forensic Sci. 2022, 2, 222-237. https://0-doi-org.brum.beds.ac.uk/10.3390/forensicsci2010017
AMA Style
Al-Asmari AI, Al-Solami FD, Al-Zahrani AE, Zughaibi TA. Post-Mortem Quantitation of Amphetamine in Cadaveric Fluids in Saudi Arabia. Forensic Sciences. 2022; 2(1):222-237. https://0-doi-org.brum.beds.ac.uk/10.3390/forensicsci2010017
Chicago/Turabian StyleAl-Asmari, Ahmed I., Faiz D. Al-Solami, Abdulnasser E. Al-Zahrani, and Torki A. Zughaibi. 2022. "Post-Mortem Quantitation of Amphetamine in Cadaveric Fluids in Saudi Arabia" Forensic Sciences 2, no. 1: 222-237. https://0-doi-org.brum.beds.ac.uk/10.3390/forensicsci2010017