
Molecular and Antifilarial IgG4 Detection Using the miniPCR-Duplex Lateral Flow Dipstick and BmSxp-ELISA in Myanmar Immigrant Communities


 ,
, 
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Antifilarial IgG4 Antibody Detection by ELISA Test
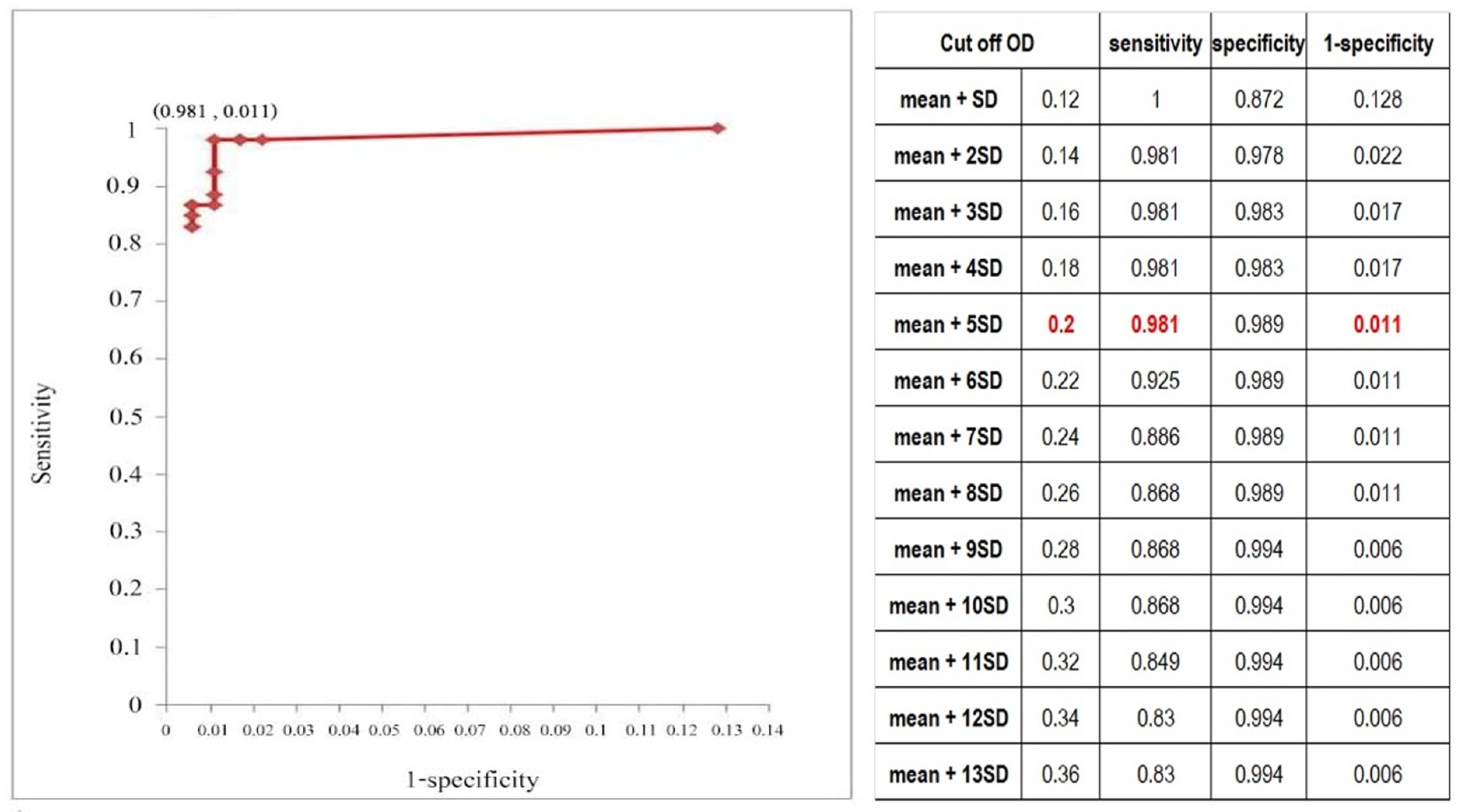
4.2.1. Cut-Off Determination
4.2.2. Sensitivity and Specificity of the Developed ELISA Test
4.2.3. Antifilarial IgG4 Detection in the Study Population
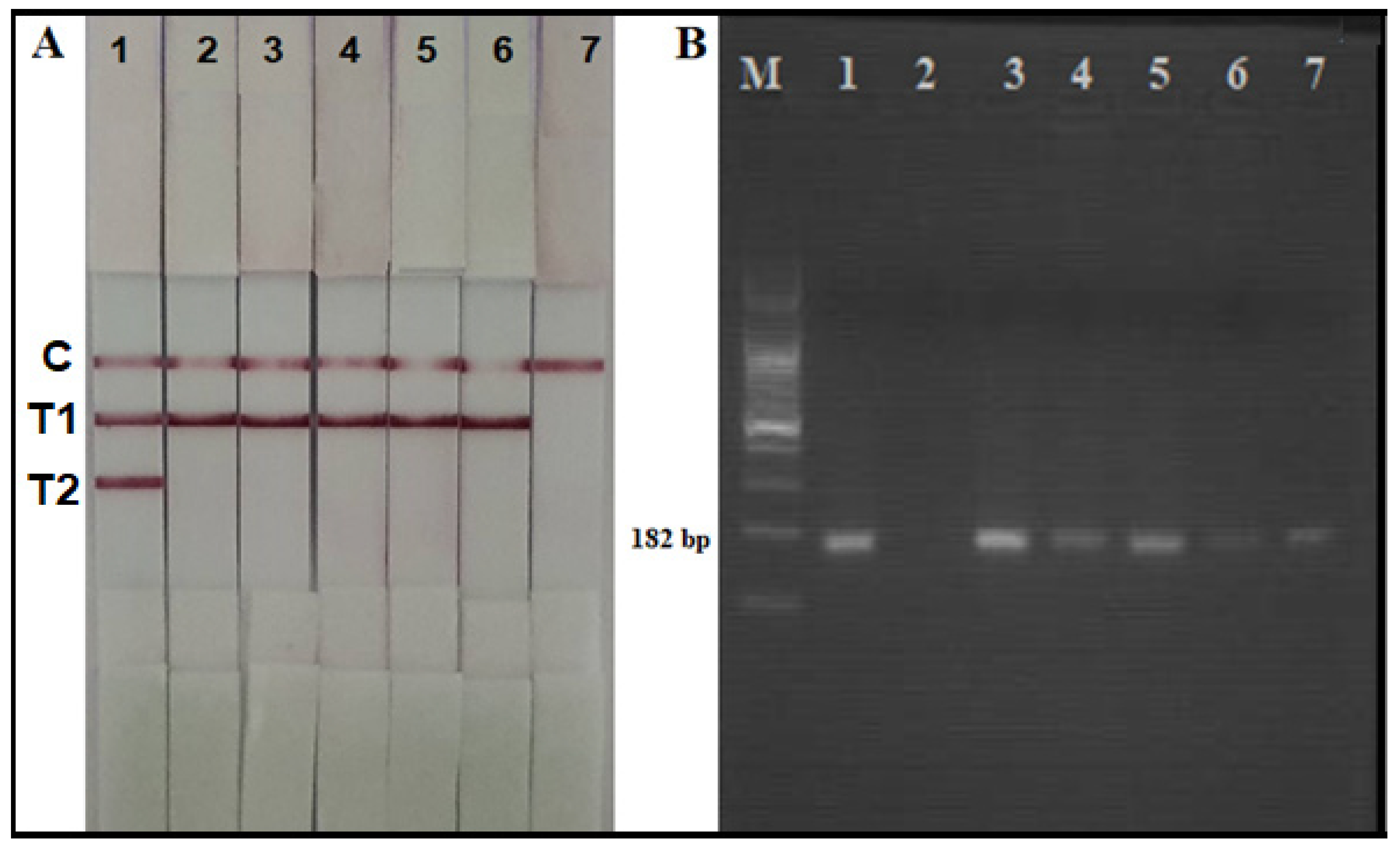
4.3. Detection of W. bancrofti DNA Using a miniPCR-DLFD
4.3.1. DNA Extraction from Study Blood Samples
4.3.2. Amplification of W. bancrofti DNA by Conventional PCR and by miniPCR
4.3.3. Detection of the Amplicon Using Agarose Gel Electrophoresis
4.3.4. Detection of the Amplicon Using the Duplex Lateral Flow Dipstick (DLFD)
4.4. Data Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Taylor, M.J.; Hoerauf, A.; Bockarie, M. Lymphatic filariasis and onchocerciasis. Lancet 2010, 376, 1175–1185. [Google Scholar] [CrossRef]
- Ottesen, E.A.; Duke, B.O.L.; Karam, M.; Behbehani, K. Strategies and tools for the control/elimination of lymphatic filariasis. Bull. World Health Org. 1997, 75, 491–503. [Google Scholar] [PubMed]
- WHO. Lymphatic filariasis: The disease and its control. In Fifth Report of the WHO Expert Committee on Filar Nnnias is World Health Organization Technical Report Series; WHO: Geneva, Switzerland, 1992; pp. 1–71. [Google Scholar]
- Wongkamchai, S.; Boitano, J. A move toward defeating lymphatic filariasis. Siriraj Med. J. 2010, 62, 93–97. [Google Scholar]
- Rojanapanus, S.; Toothong, T.; Boondej, P.; Thammapalo, B.; Khuanyoung, N.; Santabutr, W.; Prempree, P.; Gopinath, D.; Ramaiah, K.D. How Thailand eliminated lymphatic filariasis as a public health problem. Infect. Dis. Poverty 2019, 8, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Win, K.M.; Tripathy, J.P.; Maung, T.M.; Oo, T.; Aung Thi, K.N.; Lon, K.N.; Lin, Z. Rapid progress towards elimination of lymphatic filariasis in endemic regions of Myanmar as a result of 16 years of antifilarial activities (2001–2016). Trop. Med. Health 2018, 46, 14. [Google Scholar] [CrossRef]
- Duerr, H.P.; Dietz, K.; Eichner, M. Determinants of the eradicability of filarial infections: A conceptual approach. Trends Parasitol. 2005, 21, 88–96. [Google Scholar] [CrossRef]
- Gass, K.; Rochars, M.; Boakye, D.; Bradley, M.; Fischer, P.U.; Gyapong, J.; Itoh, M.; Ituaso-Conway, N.; Joseph, H.; Kyelem, D.; et al. A multicenter evaluation of diagnostic tools to define endpoints for programs to eliminate bancroftian filariasis. PLoS Negl. Trop. Dis. 2012, 6, e1479. [Google Scholar] [CrossRef]
- Ichimori, K.; King, J.D.; Engels, D.; Yajima, A.; Mikhailov, A.; Lammie, P.; Ottesen, E.A. Global Programme to Eliminate Lymphatic Filariasis: The Processes Underlying Programme Success. PLoS Negl. Trop. Dis. 2014, 8, e3328. [Google Scholar] [CrossRef]
- Ramaiah, K.D.; Ottesen, E.A. Progress and Impact of 13 Years of the Global Programme to Eliminate Lymphatic Filariasis on Reducing the Burden of Filarial Disease. PLoS Neglected. Trop. Dis. 2014, 8, e3319. [Google Scholar] [CrossRef]
- Pilotte, N.; Torres, M.; Tomaino, F.; Laney, S.; Williams, S. A TaqMan-based multiplex real-time PCR assay for the simultaneous detection of Wuchereria bancrofti and Brugia malayi. Mol. Biochem. Parasitol. 2013, 189, 33–37. [Google Scholar] [CrossRef]
- Fischer, P.; Supali, T.; Wibowo, H.; Bonow, I.; Williams, S. Detection of DNA of nocturnally periodic Brugia malayi in night and day blood samples by a polymerase chain reaction-ELISA-based method using an internal control DNA. Am. J. Trop. Med. Hyg. 2000, 62, 291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plichart, C.; Lemoine, A. Monitoring and evaluation of lymphatic filariasis interventions: An improved PCR-based pool screening method for high throughput Wuchereria bancrofti detection using dried blood spots. BioMed Central. 2013, 6, 110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lammie, P.J. Research directly linked with GPELF activities (operational research). 2.1 Essential tools-diagnostics. Am. J. Trop. Med. Hyg. 2004, 71 (Suppl. S5), 3–6. [Google Scholar] [CrossRef] [Green Version]
- Lammie, P.J.; Reiss, M.D.; Dimock, K.A.; Streit, T.G.; Roberts, J.M.; Eberhard, M.L. Longitudinal analysis of the development of filarial infection and antifilarial immunity in a cohort of Haitian children. Am. J. Trop. Med. Hyg. 1998, 59, 217–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weil, G.J.; Ramzy, R.M.R.; El Setouhy, M.; Kandil, A.M.; Ahmed, E.S.; Faris, R. A longitudinal study of bancroftian filariasis in the Nile Delta of Egypt: Baseline Data and one-year follow-up. Am. J. Trop. Med. Hyg. 1999, 61, 53–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wongkamchai, S.; Rochjanawatsiriroj, C.; Monkong, N.; Nochot, H.; Loymek, S.; Jiraamornnimit, C.; Hunnangkul, S.; Choochote, W. Diagnostic value of IgG isotype responses against Brugia malayi antifilarial antibodies in the clinical spectrum of brugian filariasis. J. Helminthol. 2006, 80, 363–367. [Google Scholar] [CrossRef] [PubMed]
- Jiraamonnimit, C.; Wongkamchai, S.; Boitano, J.; Nochot, H.; Loymek, S.; Chujun, S.; Yodmek, S. A cohort study on anti-filarial IgG4 and its assessment in good and uncertain MDA-compliant subjects in brugian filariasis endemic areas in southern Thailand. J. Helminthol. 2009, 83, 351–360. [Google Scholar] [CrossRef]
- Chanteau, S.; Glaziou, P.; Plichart, C.; Luquiaud, P.; Moulia-Pelat, J.P.; N’Guyen, L.; Cartel, J.L. Wuchereria bancrofti filariasis in French Polynesia: Agespecific patterns of microfilaraemia, circulating antigen, and specific IgG and IgG4 responses according to transmission level. Int. J. Parasitol. 1995, 25, 81–85. [Google Scholar] [CrossRef]
- Satimai, W.; Jiraamonnimit, C.; Thammapalo, S.; Choochote, W.; Luenee, P.; Boitano, J.J.; Wongkamchai, S. The impact of a national program to eliminate lymphatic filariasis in selected Myanmar immigrant communities in Bangkok and Ranong Province, Thailand. Southeast Asian J. Trop. Med. Public. Health 2011, 42, 1054–1064. [Google Scholar]
- Muck, A.E.; Pires, M.L.; Lammie, P.J. Influence of infection with non-filarial helminths on the specificity of serological assays for antifilarial immunoglobulin G4. Trans. Roy. Soc. Trop. Med. Hyg. 2003, 97, 88–90. [Google Scholar] [CrossRef] [Green Version]
- Lizotte, M.R.; Supali, T.; Partono, F.; Williams, S.A. A Polymerase Chain Reaction Assay for the Detection of Brugia Malayi in Blood. Am. J. Trop. Med. Hyg. 1994, 51, 314–321. [Google Scholar] [CrossRef] [PubMed]
- Phuakrod, A.; Sripumkhai, W.; Jeamsaksiri, W.; Pattamang, P.; Loymek, S.; Brindley, P.J.; Sarasombath, P.T.; Wongkamchai, S. A miniPCR-duplex lateral flow dipstick platform for rapid and visual diagnosis of lymphatic filariae infection. Diagnostics 2021, 11, 1855. [Google Scholar] [CrossRef]
- WHO. Towards Eliminating Lymphatic Filariasis: Progress in the South-East Region (2001–2011); World Health Organization Regional Office for South-East Asia: New Delhi, India, 2013. [Google Scholar]
- Collyer, B.S.; Irvine, M.A.; Hollingsworth, T.D.; Bradley, M.; Anderson, R.M. Defining a prevalence level to describe the elimination of Lymphatic Filariasis (LF) transmission and designing monitoring & evaluating (M&E) programmes post the cessation of mass drug administration (MDA). PLoS Negl. Trop. Dis. 2020, 14, e0008644. [Google Scholar] [CrossRef]
- Wikipedia. Available online: https://en.wikipedia.org/wiki/Mae_Sot_District (accessed on 10 August 2021).
- Dickson, B.F.R.; Graves, P.M.; McBride, W.J. Lymphatic Filariasis in Mainland Southeast Asia: A Systematic Review and Meta-Analysis of Prevalence and Disease Burden. Trop. Med. Infect. Dis. 2017, 2, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Triteeraprapab, S.; Songtrus, J. High prevalence of Wuchereria bancrofti infection among Myanmar migrants in Thailand. Ann. Trop. Med. Parasitol. 2001, 95, 535–538. [Google Scholar] [CrossRef] [PubMed]
- Nuchprayoon, S.; Yentakam, S.; Sangprakarn, S.; Junpee, A. Endemic bancroftian filariasis in Thailand: Detection by Og4C3 antigen capture ELISA and the polymerase chain reaction. J. Med. Assoc. Thai. 2001, 84, 1300–1307. [Google Scholar]
- Chansiri, K.; Phantana, S. A polymerase chain reaction assay for the survey of bancroftian filariasis. Southeast Asian J. Trop. Med. Public Health 2002, 33, 504–508. [Google Scholar]
- Nuchprayoon, S.; Sanprasert, V.; Porksakorn, C.; Nuchprayoon, I. Prevalence of bancroftian filariasis on the Thai-Myanmar border. Asian Pac. J. Allergy Immunol. 2003, 21, 179–188. [Google Scholar]
- Aye, Z.; Lin, N.N.; Lon, K.N.; Linn, N.Y.Y.; Nwe, T.W.; Mon, K.M.; Ramaiah, K.; Betts, H.A. Kelly-Hope (2018) Mapping and modelling the impact of mass drug adminstration on filariasis prevalence in Myanmar. Inf. Dis. Poverty 2018, 7, 56. [Google Scholar] [CrossRef]
- Akobeng, A.K. Understanding diagnostic tests 1: Sensitivity, specificity and predictive values. Acta Paediatr. 2007, 96, 338–341. [Google Scholar] [CrossRef]
- Akobeng, A.K. Understanding diagnostic tests 3: Receiver operating characteristic curves. Acta Paediatr. 2007, 96, 644–647. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Age Range (Years) | Male | Female | ||||
|---|---|---|---|---|---|---|
| Number | Antifilarial IgG4 | W. bancrofti DNA | Number | Antifilarial IgG4 | W. bancrofti DNA | |
| 0–10 | 3 | 0 | 0 | 9 | 0 | 0 |
| 11–20 | 45 | 0 | 0 | 74 | 0 | 0 |
| 21–30 | 37 | 2 | 2 | 41 | 2 | 2 |
| 31–40 | 17 | 1 | 1 | 29 | 0 | 0 |
| 41–50 | 12 | 1 | 0 | 14 | 0 | 0 |
| 51–60 | 4 | 0 | 0 | 10 | 0 | 0 |
| >60 | 1 | 0 | 0 | 4 | 0 | 0 |
| Total | 119 | 4 | 3 | 181 | 2 | 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wongprompitak, P.; Kusuwan, N.; Khowawisetsut, L.; Phuakrod, A.; Pipatsatitpong, D.; Wongkamchai, S. Molecular and Antifilarial IgG4 Detection Using the miniPCR-Duplex Lateral Flow Dipstick and BmSxp-ELISA in Myanmar Immigrant Communities. Parasitologia 2022, 2, 27-36. https://0-doi-org.brum.beds.ac.uk/10.3390/parasitologia2010003
Wongprompitak P, Kusuwan N, Khowawisetsut L, Phuakrod A, Pipatsatitpong D, Wongkamchai S. Molecular and Antifilarial IgG4 Detection Using the miniPCR-Duplex Lateral Flow Dipstick and BmSxp-ELISA in Myanmar Immigrant Communities. Parasitologia. 2022; 2(1):27-36. https://0-doi-org.brum.beds.ac.uk/10.3390/parasitologia2010003
Chicago/Turabian StyleWongprompitak, Patimaporn, Navapon Kusuwan, Ladawan Khowawisetsut, Achinya Phuakrod, Duangnate Pipatsatitpong, and Sirichit Wongkamchai. 2022. "Molecular and Antifilarial IgG4 Detection Using the miniPCR-Duplex Lateral Flow Dipstick and BmSxp-ELISA in Myanmar Immigrant Communities" Parasitologia 2, no. 1: 27-36. https://0-doi-org.brum.beds.ac.uk/10.3390/parasitologia2010003