The Role of the Family Network When Raising a Child with a Disability in Low- and Middle-Income Countries


Abstract
:1. Introduction
Aim of this Study
2. Methods
2.1. Dataset
Participants
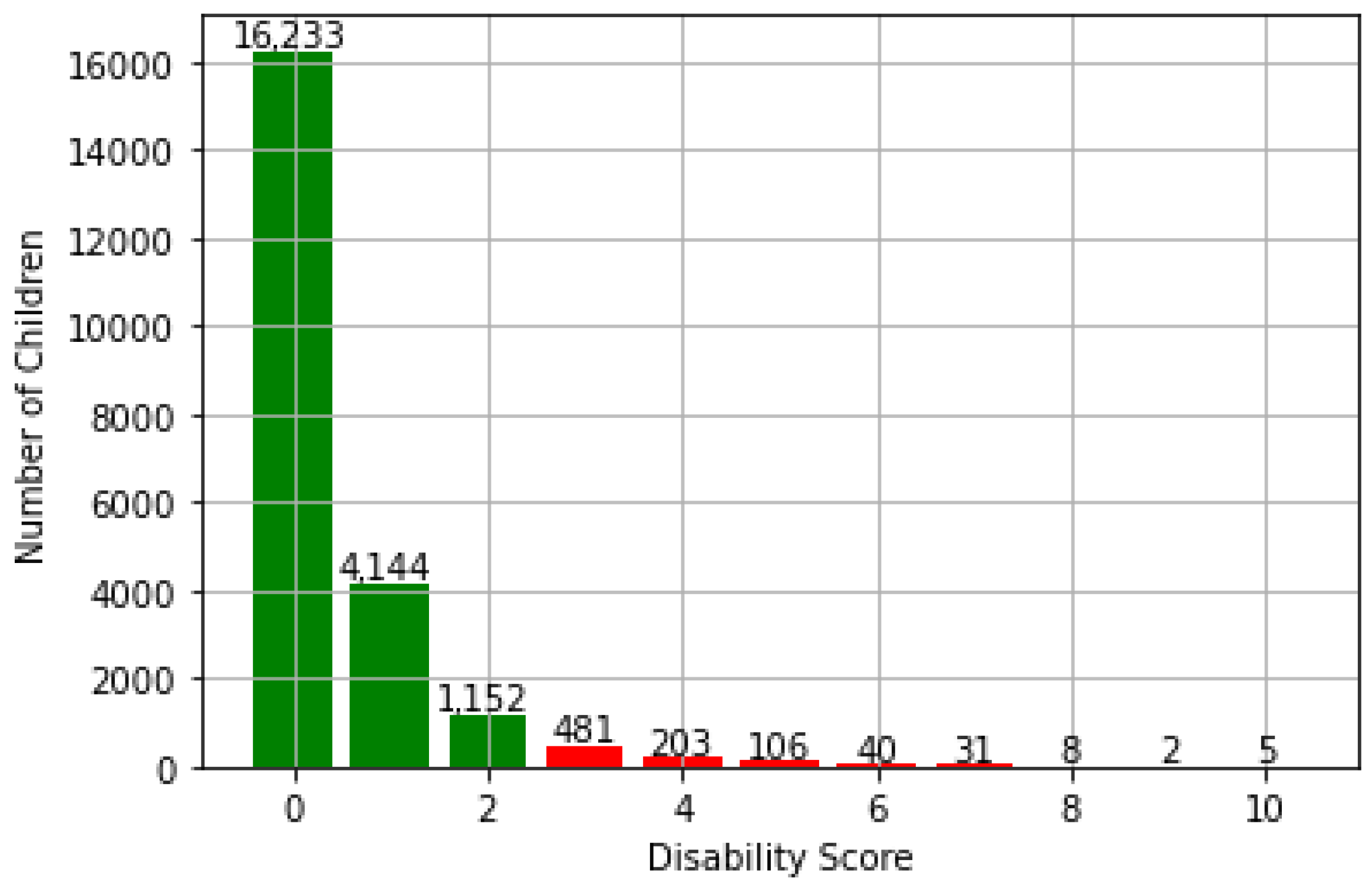
2.2. Child Developmental Disabilities
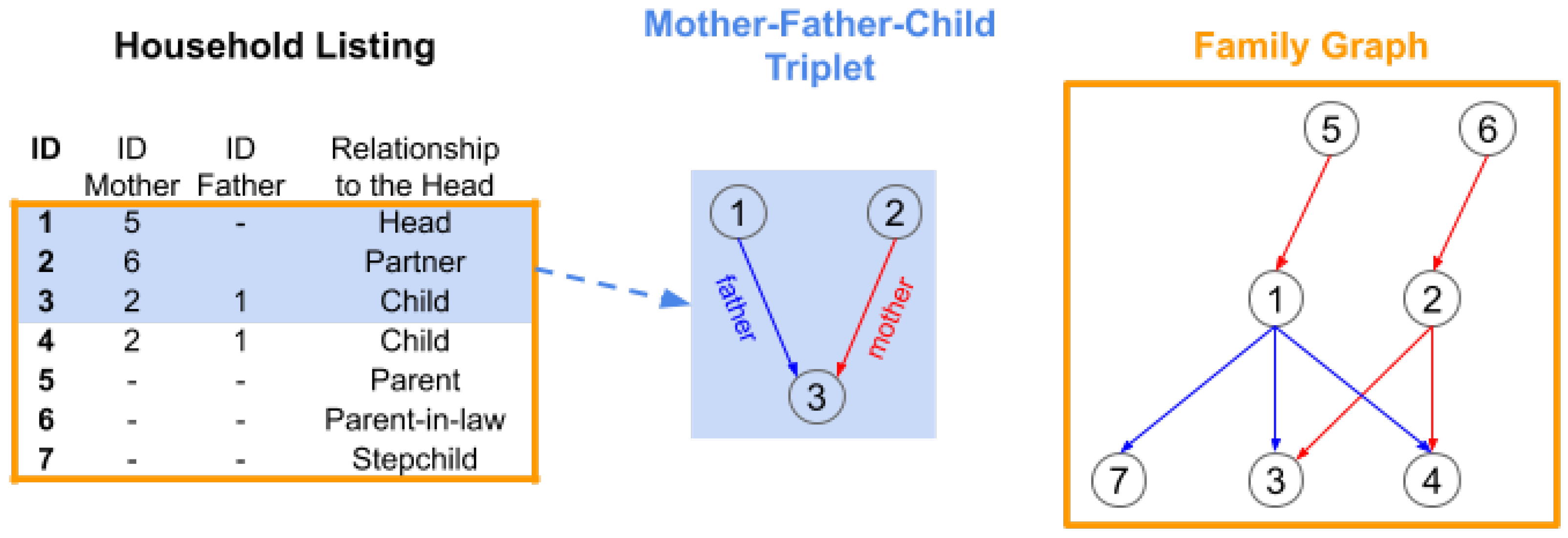
2.3. Household Listing
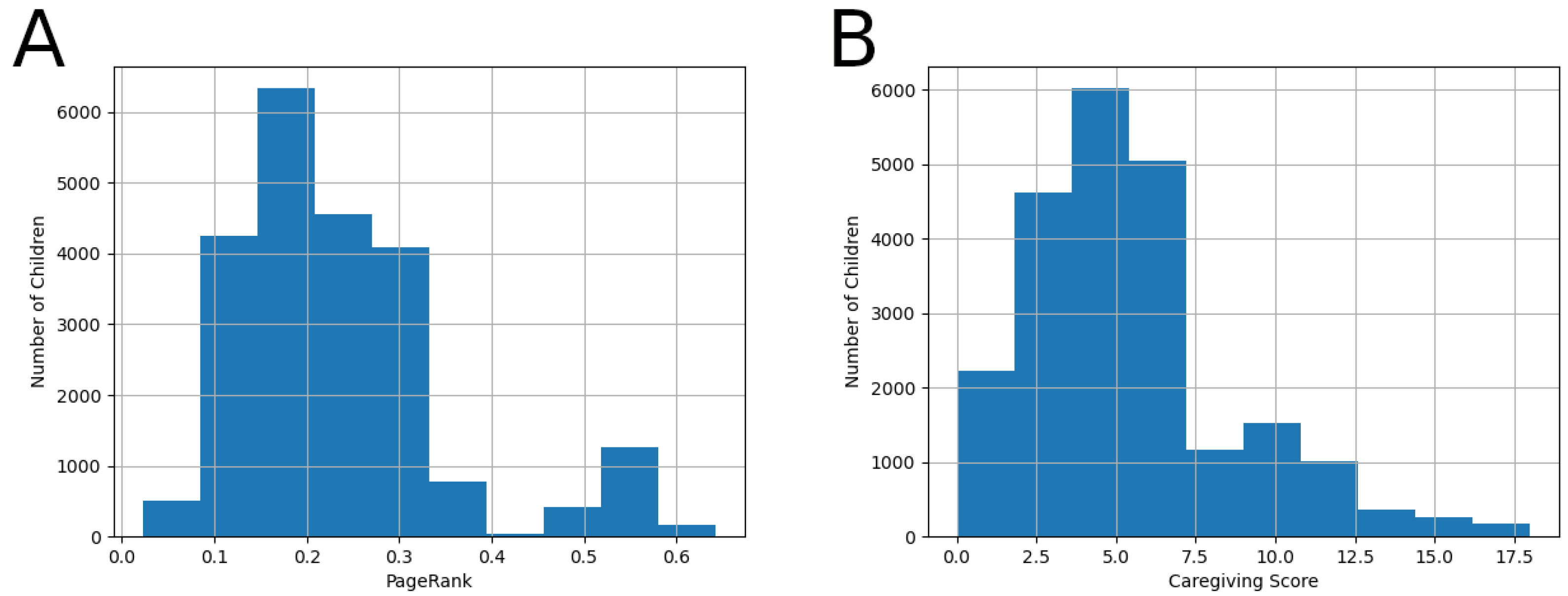
2.4. Caregiving
2.5. Parental Education
2.6. Data Analysis
3. Results
4. Discussion
4.1. Limitations
4.2. Implications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brooks, J.B. The Process of Parenting; ERIC: Washington, DC, USA, 1981.
- Anyanwu, J.I.; Onuigbo, L.N.; Obiyo, N.O.; Eze, U.N.; Akaneme, I.N.; Aye, E.N.; Enyi, C.; Oforka, T.O.; Chigbu, B.C.; Ezenwaji, I.O.; et al. Parenting stress in families of children with autism spectrum disorder: The roles of the extended family. Glob. J. Health Sci. 2019, 11, 51–60. [Google Scholar] [CrossRef]
- Tingvold, L.; Hauff, E.; Allen, J.; Middelthon, A.L. Seeking balance between the past and the present: Vietnamese refugee parenting practices and adolescent well-being. Int. J. Intercult. Relat. 2012, 36, 563–574. [Google Scholar] [CrossRef] [Green Version]
- Brandon, P. An analysis of kin-provided child care in the context of intrafamily exchanges: Linking components of family support for parents raising young children. Am. J. Econ. Sociol. 2000, 59, 191–216. [Google Scholar] [CrossRef]
- Zambrana, R.E.; Silva-Palacios, V.; Powell, D. Parenting concerns, family support systems, and life problems in Mexican-origin women: A comparison by nativity. J. Community Psychol. 1992, 20, 276–288. [Google Scholar] [CrossRef]
- Easen, P.; Kendall, P.; Shaw, J. Parents and educators: Dialogue and development through partnership. Child. Soc. 1992, 6, 282–296. [Google Scholar] [CrossRef]
- Johnson, C.P.; Kastner, T.A. Helping families raise children with special health care needs at home. Pediatrics 2005, 115, 507–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bronfenbrenner, U. The Ecology of Human Development; Harvard University Press: Cambridge, MA, USA, 1979. [Google Scholar]
- US Bureau of Labour Statistics. 2018. Available online: https://www.bls.gov/charts/american-time-use/activity-by-parent.htm (accessed on 15 May 2020).
- Åman-Back, S.; Björkqvist, K. Parents’ assessments of how much time they spend with their children at different ages. Psychol. Rep. 2004, 94, 1025–1030. [Google Scholar] [CrossRef] [PubMed]
- Rosen, K.S.; Rothbaum, F. Quality of parental caregiving and security of attachment. Dev. Psychol. 1993, 29, 358. [Google Scholar] [CrossRef]
- Rothbaum, F.; Weisz, J.R. Parental caregiving and child externalizing behavior in nonclinical samples: A meta-analysis. Psychol. Bull. 1994, 116, 55. [Google Scholar] [CrossRef]
- Armstrong, M.I.; Birnie-Lefcovitch, S.; Ungar, M.T. Pathways between social support, family well being, quality of parenting, and child resilience: What we know. J. Child Fam. Stud. 2005, 14, 269–281. [Google Scholar] [CrossRef]
- Kok, J.; Vandezande, M.; Mandemakers, K. Household structure, resource allocation and child well-being. A comparison across family systems. Tijdschr. Voor Soc. Econ. Geschied. 2011, 8, 76–101. [Google Scholar] [CrossRef] [Green Version]
- Corse, S.J.; Schmid, K.; Trickett, P.K. Social network characteristics of mothers in abusing and nonabusing families and their relationships to parenting beliefs. J. Community Psychol. 1990, 18, 44–59. [Google Scholar] [CrossRef]
- Leidy, M.S.; Guerra, N.G.; Toro, R.I. Positive parenting, family cohesion, and child social competence among immigrant Latino families. J. Fam. Psychol. 2010, 24, 252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention. 2019. Available online: https://www.cdc.gov/ncbddd/developmentaldisabilities/index.html (accessed on 15 May 2020).
- Tomanik, S.; Harris, G.E.; Hawkins, J. The relationship between behaviors exhibited by children with autism and maternal stress. J. Intellect. Dev. Disabil. 2004, 29, 16–26. [Google Scholar] [CrossRef]
- Hassall, R.; Rose, J.; McDonald, J. Parenting stress in mothers of children with an intellectual disability: The effects of parental cognitions in relation to child characteristics and family support. J. Intellect. Disabil. Res. 2005, 49, 405–418. [Google Scholar] [CrossRef] [PubMed]
- Oelofsen, N.; Richardson, P. Sense of coherence and parenting stress in mothers and fathers of preschool children with developmental disability. J. Intellect. Dev. Disabil. 2006, 31, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Pelchat, D.; Lefebvre, H.; Perreault, M. Differences and similarities between mothers’ and fathers’ experiences of parenting a child with a disability. J. Child Health Care 2003, 7, 231–247. [Google Scholar] [CrossRef] [Green Version]
- Anthony, L.G.; Anthony, B.J.; Glanville, D.N.; Naiman, D.Q.; Waanders, C.; Shaffer, S. The relationships between parenting stress, parenting behavior and preschoolers’ social competence and behavior problems in the classroom. Infant Child Dev. Int. J. Res. Pract. 2005, 14, 133–154. [Google Scholar] [CrossRef]
- Armstrong, M.I. An Empirical Study: A Model of the Pathways between Social Support, Family Well Being, Parenting Quality, and Child Resilience. Ph.D Thesis, Memorial University of Newfoundland, St. John’s, NL, Canada, 2003. [Google Scholar]
- Hammel, E.A.; Laslett, P. Comparing household structure over time and between cultures. Comp. Stud. Soc. Hist. 1974, 16, 73–109. [Google Scholar] [CrossRef]
- Laslett, P. Characteristics of the Western family considered over time. J. Fam. Hist. 1977, 2, 89–115. [Google Scholar] [CrossRef]
- Boyle, C.A.; Boulet, S.; Schieve, L.A.; Cohen, R.A.; Blumberg, S.J.; Yeargin-Allsopp, M.; Visser, S.; Kogan, M.D. Trends in the prevalence of developmental disabilities in US children, 1997–2008. Pediatrics 2011, 127, 1034–1042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leonard, H.; Petterson, B.; De Klerk, N.; Zubrick, S.R.; Glasson, E.; Sanders, R.; Bower, C. Association of sociodemographic characteristics of children with intellectual disability in Western Australia. Soc. Sci. Med. 2005, 60, 1499–1513. [Google Scholar] [CrossRef]
- Department of Health and Social Care (UK Government). Valuing People: A New Strategy for Learning Disability for the 21st Century; HM Stationery Office: London, UK, 2001.
- Magnus, P. Correlations between socioeconomic status, level of IQ and aetiology in mental retardation: A populationbased study of Norwegian children. Soc. Psychiatry Psychiatr. Epidemiol. 2000, 35, 12–18. [Google Scholar]
- Drews, C.D.; Yeargin-Allsopp, M.; Decoufle, P.; Murphy, C.C. Variation in the influence of selected sociodemographic risk factors for mental retardation. Am. J. Public Health 1995, 85, 329–334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noel, M.; Peterson, C.; Jesso, B. The relationship of parenting stress and child temperament to language development among economically disadvantaged preschoolers. J. Child Lang. 2008, 35, 823–843. [Google Scholar] [CrossRef] [Green Version]
- Gaad, E. Cross-cultural perspectives on the effect of cultural attitudes towards inclusion for children with intellectual disabilities. Int. J. Incl. Educ. 2004, 8, 311–328. [Google Scholar] [CrossRef]
- Wong, S.Y.; Wong, T.K.; Martinson, I.; Lai, A.C.; Chen, W.; He, Y. Needs of Chinese parents of children with developmental disability. J. Learn. Disabil. 2004, 8, 141–158. [Google Scholar] [CrossRef]
- Fatimilehin, I.A.; Nadirshaw, Z. A cross-cultural study of parental attitudes and beliefs about learning disability (mental handicap). Ment. Handicap. Res. 1994, 7, 202–227. [Google Scholar] [CrossRef]
- Bornstein, M.H. Handbook of Cultural Developmental Science; Psychology Press: London, UK, 2014. [Google Scholar]
- Engle, P.L.; Black, M.M.; Behrman, J.R.; De Mello, M.C.; Gertler, P.J.; Kapiriri, L.; Martorell, R.; Young, M.E.; International Child Development Steering Group. Strategies to avoid the loss of developmental potential in more than 200 million children in the developing world. Lancet 2007, 269, 229–242. [Google Scholar] [CrossRef] [Green Version]
- Pan, K.M. Children and the Millennium Development Goals: Progress Towards a World Fit for Children; UNICEF: New York, NY, USA, 2007. [Google Scholar]
- Bizzego, A.; Lim, M.; Schiavon, G.; Setoh, P.; Gabrieli, G.; Dimitriou, D.; Esposito, G. Child disability and caregiving in low and middle income countries: Big data approach on open data. Res. Dev. Disabil. 2020, 107, 103795. [Google Scholar] [CrossRef]
- Bizzego, A.; Lim, M.; Schiavon, G.; Esposito, G. Children with developmental disabilities in low-and middle-income countries: More neglected and physically punished. Int. J. Environ. Res. Public Health 2020, 17, 7009. [Google Scholar] [CrossRef]
- UNICEF. Multiple Indicator Cluster Survey Manual 2005; UNICEF: New York, NY, USA, 2006. [Google Scholar]
- Bornstein, M.H.; Putnick, D.L.; Bradley, R.H.; Deater-Deckard, K.; Lansford, J.E. Gender in low- and middle-income countries. In Monographs of the Society for Research in Child Development; Blackwell Publishing: Hoboken, NJ, USA, 2016; Volume 81. [Google Scholar]
- Zaman, S.S.; Khan, N.Z.; Islam, S.; Banu, S.; Dixit, S.; Shrout, P.; Durkin, M. Validity of the ‘Ten Questions’ for screening serious childhood disability: Results from urban Bangladesh. Int. J. Epidemiol. 1990, 19, 613–620. [Google Scholar] [CrossRef] [PubMed]
- Hendricks, C.; Lansford, J.E.; Deater-Deckard, K.; Bornstein, M.H. Associations between child disabilities and caregiver discipline and violence in low-and middle-income countries. Child Dev. 2014, 85, 513–531. [Google Scholar] [CrossRef]
- Bornstein, M.H.; Hendricks, C. Screening for developmental disabilities in developing countries. Soc. Sci. Med. 2013, 97, 307–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gottlieb, C.A.; Maenner, M.J.; Cappa, C.; Durkin, M.S. Child disability screening, nutrition, and early learning in 18 countries with low and middle incomes: Data from the third round of UNICEF’s Multiple Indicator Cluster Survey (2005–06). Lancet 2009, 374, 1831–1839. [Google Scholar] [CrossRef]
- Mung’ala-Odera, V.; Meehan, R.; Njuguna, P.; Mturi, N.; Alcock, K.; Carter, J.; Newton, C. Validity and reliability of the ‘Ten Questions’ questionnaire for detecting moderate to severe neurological impairment in children aged 6–9 years in rural Kenya. Neuroepidemiology 2004, 23, 67–72. [Google Scholar] [CrossRef] [Green Version]
- Christianson, A.; Zwane, M.; Manga, P.; Rosen, E.; Venter, A.; Downs, D.; Kromberg, J. Children with intellectual disability in rural South Africa: Prevalence and associated disability. J. Intellect. Disabil. Res. 2002, 46, 179–186. [Google Scholar] [CrossRef]
- Fletcher, J.M.; Wennekers, T. From structure to activity: Using centrality measures to predict neuronal activity. Int. J. Neural Syst. 2018, 28, 1750013. [Google Scholar] [CrossRef] [Green Version]
- Bánky, D.; Iván, G.; Grolmusz, V. Equal opportunity for low-degree network nodes: A PageRank-based method for protein target identification in metabolic graphs. PLoS ONE 2013, 8, e54204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iván, G.; Grolmusz, V. When the Web meets the cell: Using personalized PageRank for analyzing protein interaction networks. Bioinformatics 2011, 27, 405–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hagberg, A.A.; Schult, D.A.; Swart, P.J. Exploring Network Structure, Dynamics, and Function using NetworkX. In Proceedings of the 7th Python in Science Conference, Pasadena, CA, USA, 19–24 August 2008; pp. 11–15. [Google Scholar]
- Bornstein, M.H.; Putnick, D.L.; Oburu, P.; Lansford, J.E.; Deater-Deckard, K.; Bradley, R.H.; Moriguchi, R.; Britto, P.R. Parenting, environment, and early child development in sub-Saharan Africa. In Handbook of Applied Developmental Science in Sub-Saharan Africa; Springer: Berlin/Heidelberg, Germany, 2017; pp. 15–53. [Google Scholar]
- Cuartas, J.; Jeong, J.; Rey-Guerra, C.; McCoy, D.C.; Yoshikawa, H. Maternal, paternal, and other caregivers’ stimulation in low-and-middle-income countries. PLoS ONE 2020, 15, e0236107. [Google Scholar] [CrossRef]
- Jeong, J.; McCoy, D.C.; Fink, G. Pathways between paternal and maternal education, caregivers’ support for learning, and early child development in 44 low-and middle-income countries. Early Child. Res. Q. 2017, 41, 136–148. [Google Scholar] [CrossRef]
- Bornstein, M.H.; Putnick, D.L.; Bradley, R.H.; Lansford, J.E.; Deater-Deckard, K. Pathways among caregiver education, household resources, and infant growth in 39 low-and middle-income countries. Infancy 2015, 20, 353–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindert, P.H. Fertility and Scarcity in America; Princeton University Press: Princeton, NJ, USA, 2015. [Google Scholar]
- Downey, D.B. When bigger is not better: Family size, parental resources, and children’s educational performance. Am. Sociol. Rev. 1995, 60, 746–761. [Google Scholar] [CrossRef]
- Powell, B.; Steelman, L.C. Feeling the pinch: Child spacing and constraints on parental economic investments in children. Soc. Forces 1995, 73, 1465–1486. [Google Scholar] [CrossRef]
- Blake, J. Family size and Achievement; University of California Press: Berkeleym, CA, USA, 1989; Volume 3. [Google Scholar]
- Blake, J. Family size and the quality of children. Demography 1981, 18, 421–442. [Google Scholar] [CrossRef]
- Jensen, A.C.; Whiteman, S.D.; Bernard, J.M.; McHale, S.M. Family resource allocation after firstborns leave home: Implications for secondborns’ academic functioning. Fam. Process. 2017, 56, 766–780. [Google Scholar] [CrossRef] [Green Version]
- Dalton, M.; Hotz, J.; Thomas, D. Resources, Composition, and Family-Decision Making, Working Paper. 2014. Available online: http://public.econ.duke.edu/vjh3/working_papers/FamDecisionMaking.pdf (accessed on 18 March 2021).
- Leeb, R.T.; Bitsko, R.H.; Merrick, M.T.; Armour, B.S. Does childhood disability increase risk for child abuse and neglect? J. Ment. Health Res. Intellect. Disabil. 2012, 5, 4–31. [Google Scholar] [CrossRef]
- Eshbaugh, E.M.; Peterson, C.A.; Wall, S.; Carta, J.J.; Luze, G.; Swanson, M.; Jeon, H.J. Low-income parents’ warmth and parent–child activities for children with disabilities, suspected delays and biological risks. Infant Child Dev. 2011, 20, 509–524. [Google Scholar] [CrossRef] [Green Version]
- Hibbard, R.A.; Desch, L.W.; Committee on Child Abuse and Neglect. Maltreatment of children with disabilities. Pediatrics 2007, 119, 1018–1025. [Google Scholar] [CrossRef] [Green Version]
- Embry, R. Examination of risk factors for maltreatment of deaf children: Findings from a national survey. In Proceedings of the 7th International Family Violence Research Conference, Portsmouth, NH, USA, 22–25 July 2001. [Google Scholar]
- Sullivan, P.M.; Knutson, J.F. Maltreatment and disabilities: A population-based epidemiological study. Child Abus. Negl. 2000, 24, 1257–1273. [Google Scholar] [CrossRef]
- Li, X.; Lam, C.B.; Chung, K.K.H.; Leung, C. Linking parents’ self-stigma to the adjustment of children with disabilities. Am. J. Orthopsychiatry 2019, 89, 212. [Google Scholar] [CrossRef]
- Hilbert, D. Perceptions of parents of young children with and without disabilities attending inclusive preschool programs. J. Educ. Learn. 2014, 3, 49–59. [Google Scholar] [CrossRef]
- Dyson, L.L. Children with learning disabilities within the family context: A comparison with siblings in global self–concept, academic self–perception, and social competence. Learn. Disabil. Res. Pract. 2003, 18, 1–9. [Google Scholar] [CrossRef]
- Scanzoni, J. Household diversity. In Handbook of Contemporary Families: Considering the Past, Contemplating the Future; Sage: Los Angeles, CA, USA, 2004; p. 1. [Google Scholar]
- Bien, W.; Marbach, J.; Neyer, F. Using egocentered networks in survey research. A methodological preview on an application of social network analysis in the area of family research. Soc. Netw. 1991, 13, 75–90. [Google Scholar] [CrossRef]
- Wilson, P.; Pahl, R. The changing sociological construct of the family. Sociol. Rev. 1988, 36, 233–266. [Google Scholar] [CrossRef]
- Furstenberg, F.F. The new extended family: The experience of parents and children after remarriage. In Remarriage and Stepparenting: Current Research and Theory; The Guilford Press: New York, NY, USA, 1987. [Google Scholar]
- Pasley, K.; Ihinger-Tallman, M. Family boundary ambiguity: Perception of adult remarried family members. In Remarriage and Step-Parenting: Current Research and Theory; The Guilford Press: New York, NY, USA, 1987; pp. 228–240. [Google Scholar]
- Widmer, E.D.; La Farga, L.A. Family networks: A sociometric method to study relationships in families. Field Methods 2000, 12, 108–128. [Google Scholar] [CrossRef]
- UNICEF. Monitoring Child Disability in Developing Countries; UNICEF: New York, NY, USA, 2008. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Country | N | Income Group | ||
|---|---|---|---|---|
| Albania | 666 | 647 | 19 | Upper-middle |
| Belize | 363 | 333 | 30 | Upper-middle |
| Cameroon | 2088 | 1984 | 104 | Lower-middle |
| Central African Republic | 3047 | 2748 | 299 | Low |
| Djibouti | 192 | 158 | 34 | Lower-middle |
| Georgia | 990 | 949 | 41 | Upper-middle |
| Ghana | 1051 | 1021 | 30 | Lower-middle |
| Lao PDR | 1697 | 1670 | 27 | Lower-middle |
| Mauritania | 1782 | 1696 | 86 | Lower-middle |
| Mongolia | 1801 | 1754 | 47 | Lower-middle |
| Mozambique | 4175 | 4134 | 41 | Low |
| Suriname | 973 | 926 | 47 | Upper-middle |
| Uzbekistan | 2433 | 2419 | 14 | Lower-middle |
| Yemen | 1147 | 1090 | 57 | Low |
| Question | Answer Indicating Disability | |
|---|---|---|
| Q1 | Any serious delay sitting, standing, or walking? | Yes |
| Q2 | Does she/he have difficulty seeing in the daytime or nighttime? | Yes |
| Q3 | Does she/he appear to have difficulty hearing? | Yes |
| Q4 | When you ask her/him to do something, does she/he seem to understand what you say? | No |
| Q5 | Does she/he have difficulty walking or moving? | Yes |
| Q6 | Does she/he have fits, become rigid, or lose consciousness | Yes |
| Q7 | Does she/he learn to do things like others? | No |
| Q8 | Can she/he say recognizable words? | No |
| Q9A | Can she/he name at least one object? (for 2 year old children) | No |
| Q9B | Is her/his speech in any way different from normal? (for children older than 2 years) | Yes |
| Q10 | Compared to other children, does she/he appear mentally backward, dull, or slow? | Yes |
| Coefficient | SE | z-Score | p-Value | |
|---|---|---|---|---|
| Intercept | 0.130 | 0.001 | 152.94 | <0.001 |
| CDI | −0.001 | 0.001 | −1.53 | 0.125 |
| PageRank | −0.015 | 0.003 | −4.70 | <0.001 |
| CDI*PageRank | −0.006 | 0.003 | 1.97 | 0.049 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bizzego, A.; Lim, M.; Dimitriou, D.; Esposito, G. The Role of the Family Network When Raising a Child with a Disability in Low- and Middle-Income Countries. Disabilities 2021, 1, 58-68. https://0-doi-org.brum.beds.ac.uk/10.3390/disabilities1010005
Bizzego A, Lim M, Dimitriou D, Esposito G. The Role of the Family Network When Raising a Child with a Disability in Low- and Middle-Income Countries. Disabilities. 2021; 1(1):58-68. https://0-doi-org.brum.beds.ac.uk/10.3390/disabilities1010005
Chicago/Turabian StyleBizzego, Andrea, Mengyu Lim, Dagmara Dimitriou, and Gianluca Esposito. 2021. "The Role of the Family Network When Raising a Child with a Disability in Low- and Middle-Income Countries" Disabilities 1, no. 1: 58-68. https://0-doi-org.brum.beds.ac.uk/10.3390/disabilities1010005