
The Prognostic Factors and Required Degree Influencing the Activities of Daily Living and Gait in Brain Impairment Patients with Hemiplegia


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Assessment
2.2.1. Walking
2.2.2. Feeding
2.2.3. Personal Hygiene (Grooming)
2.2.4. Dressing
2.2.5. Toileting
2.2.6. Bathing
2.3. Statistics
3. Results
3.1. Chi-Squared or Independent T Test for ADL
3.2. Spearman’s Rho Test of Each ADL
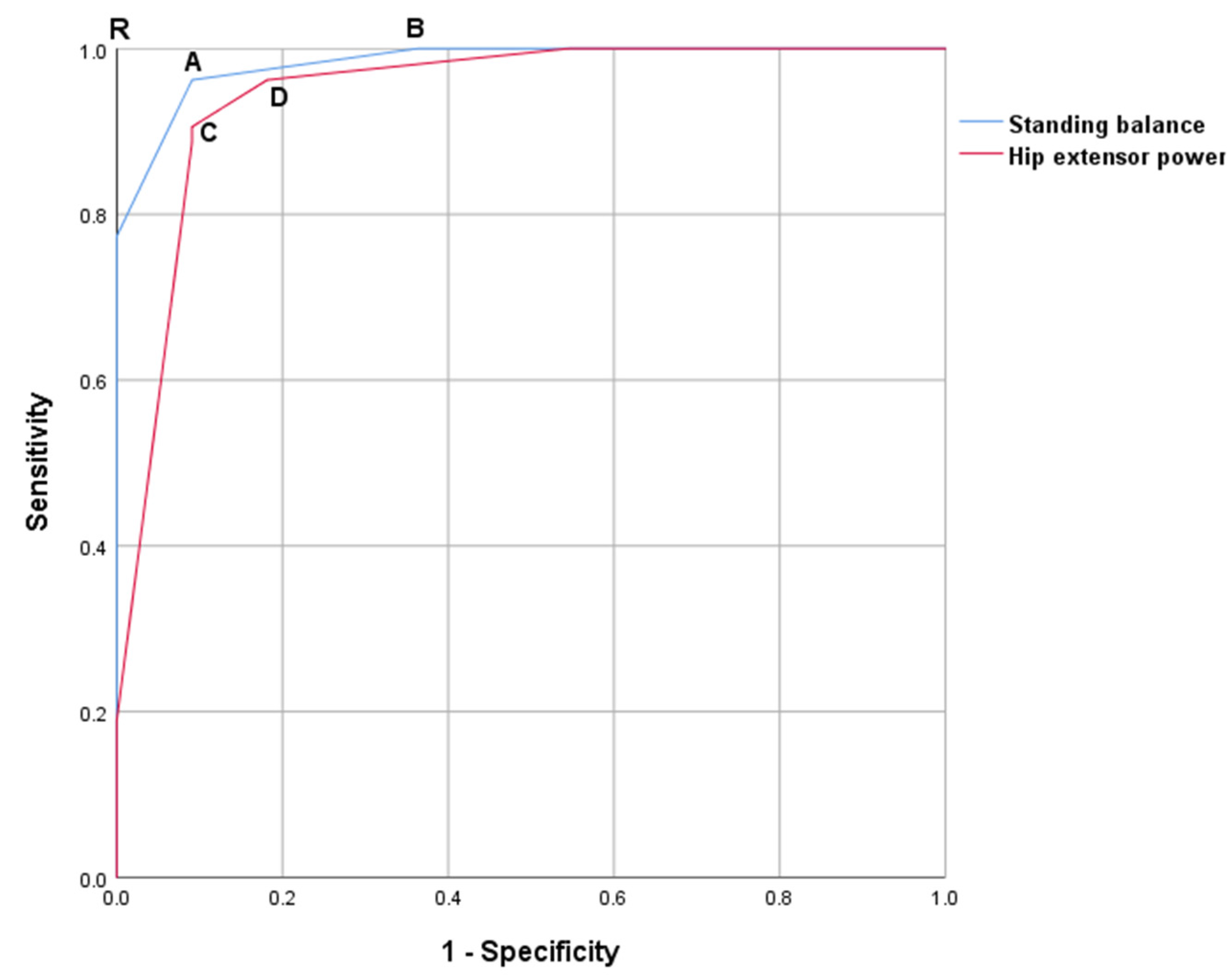
3.3. ROC Curve of Each ADL
4. Discussion
4.1. Walking
4.2. Feeding
4.3. Personal Hygiene (Grooming)
4.4. Dressing
4.5. Toileting
4.6. Bathing
4.7. Modified Balance Scale
4.8. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Anderson, C.S.; Linto, J.; Stewart-Wynne, E.G. A population-based assessment of the impact and burden of caregiving for long-term stroke survivors. Stroke 1995, 26, 843–849. [Google Scholar] [CrossRef]
- Kalra, L.; Langhorne, P. Facilitating recovery: Evidence for organized stroke care. J. Rehabil. Med. 2007, 39, 97–102. [Google Scholar] [CrossRef] [Green Version]
- Foulkes, M.A.; Wolf, P.A.; Price, T.R.; Mohr, J.P.; Hier, D.B. The Stroke Data Bank: Design, methods, and baseline characteristics. Stroke 1988, 19, 547–554. [Google Scholar] [CrossRef] [Green Version]
- Feigenson, J.S.; McDowell, F.H.; Meese, P.; McCarthy, M.L.; Greenberg, S.D. Factors influencing outcome and length of stay in a stroke rehabilitation unit. Stroke 1987, 18, 830–836. [Google Scholar]
- Brandstater, M.E.; de Bruin, H.; Gowland, C.; Clark, B.M. Hemiplegic gait: Analysis of temporal variables. Arch. Phys. Med. Rehabil. 1983, 64, 583–587. [Google Scholar]
- Bohannon, R.W. Gait performance of hemiparetic stroke patients: Selected variables. Arch. Phys. Med. Rehabil. 1987, 68, 777–781. [Google Scholar] [PubMed]
- Wade, D.T.; Hewer, R.L. Functional abilities after stroke: Measurement, natural history and prognosis. J. Neurol. Neurosurg. Psychiatry 1987, 50, 177–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shelton, F.D.; Volpe, B.T.; Reding, M. Motor impairment as a predictor of functional recovery and guide to rehabilitation treatment after stroke. Neurorehabil. Neural Repair 2001, 15, 229–237. [Google Scholar] [CrossRef]
- Hsu, A.L.; Tang, P.F.; Jan, M.H. Analysis of impairments influencing gait velocity and asymmetry of hemiplegic patients after mild to moderate stroke. Arch. Phys. Med. Rehabil. 2003, 84, 1185–1193. [Google Scholar] [CrossRef]
- Kollen, B.; van de Port, I.; Lindeman, E.; Twisk, J.; Kwakkel, G. Predicting improvement in gait after stroke: A longitudinal prospective study. Stroke 2005, 36, 2676–2680. [Google Scholar] [CrossRef]
- Schmid, A.A.; Puymbroeck, M.V.; Altenburger, P.A.; Miler, K.K.; Combs, S.A.; Page, S.J. Balance is associated with quality of life in chronic stroke. Top Stroke Rehabil. 2013, 20, 340–346. [Google Scholar] [CrossRef] [PubMed]
- Hirano, Y.; Hayashi, T.; Nitta, O.; Takahashi, H.; Nishio, D.; Minakawa, T.; Kigawa, H. Prediction of independent walking ability for severely hemiplegic stroke patients at discharge from a rehabilitation hospital. J. Stroke Cerebrovasc Dis. 2016, 25, 1878–1881. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, S.; Takemura, N.; Taira, K.; Hamakawa, M.; Nakachi, Y.; Goya, M.; Yamazato, T.; Shimose, R.; Miura, H.; Tsunoda, S.; et al. Gait speed and balance function strongly determine the ability to walk independently without using a wheelchair in a facility setting for stroke patients. Kitasato Med. J. 2018, 48, 16–25. [Google Scholar]
- Preston, E.; Ada, L.; Stanton, R.; Mahendran, N.; Dean, C.M. Prediction of independent walking in people who are nonambulatory early after stroke: A systematic review. Stroke 2021. [Google Scholar] [CrossRef]
- Medical Research Council. Aids to the Investigation of Peripheral Nerve Injuries: War Memorandum No. 7. Revised, 2nd ed.; Her Majesty’s Stationery Office: London, UK, 1943. [Google Scholar]
- Bohannon, R.W.; Smith, M.B. Interrater reliability of a modified Ashworth scale of muscle spasticity. Phys. Ther. 1987, 67, 206–207. [Google Scholar] [CrossRef]
- Shah, S.; Vanclay, F.; Cooper, B. Improving the sensitivity of the Barthel index for stroke rehabilitation. J. Clin. Epidemiol. 1989, 42, 703–709. [Google Scholar] [CrossRef]
- Jung, H.Y.; Park, B.K.; Shin, H.S.; Kang, Y.K.; Pyun, S.B.; Paik, N.J.; Han, T.R. Development of the Korean version of modified Barthel index: Multi-center study for subjects with stroke. J. Korean Acad. Rehab. Med. 2007, 31, 283–297. [Google Scholar]
- Kang, Y.W.; Na, D.L.; Hahn, S.H. A validity study on the Korean mini-mental state examination (K-MMSE) in dementia patients. J. Korean Neurol. Assoc. 1997, 15, 300–308. [Google Scholar]
- O’Sullivan, S.B.; Schmitz, T.J. Physical Rehabilitation: Assessment and Treatment, 5th ed.; Davis Company: Philadelphia, PA, USA, 2007; p. 254. [Google Scholar]
- Montometry, P.; Connolly, B. Motor Control and Physical Therapy; Waterloo Library Friends: Waterloo, ON, Canada, 1991; p. 75. [Google Scholar]
- Kanji, J.N.; Anglin, R.E.S.; Hunt, D.L.; Panju, A. Does this patient with diabetes have large-fiber peripheral neuropathy? JAMA 2010, 303, 1526–1532. [Google Scholar] [CrossRef]
- Ebru, Y.Y. Updates in ASIA examination: Sensory examination. Turk. J. Phys. Med. Rehab. 2015, 61, 56–59. [Google Scholar]
- Kim, E.J.; Kim, S.S.; Kim, W.H.; Lee, W.J.; Nam, K.Y.; Park, C.W.; Choi, S.W. The selection of exercise stress test in hemiplegic patients. Ann. Rehabil. Med. J. Korean Acad. Rehab. Med. 2008, 32, 26–31. [Google Scholar]
- Chan, Y.H. Biostatistics 104: Correlational analysis. Singapore Med. J. 2003, 44, 614–619. [Google Scholar] [PubMed]
- Habibzadeh, F.; Habibzadeh, P.; Yadollahie, M. On determining the most appropriate test cut-off value: The case of tests with continuous results. Biochem. Med. 2016, 26, 297–307. [Google Scholar] [CrossRef] [PubMed]
- Duncan, P.W.; Lai, S.M.; Keighley, J. Defining post-stroke recovery: Implications for design and interpretation of drug trials. Neuropharmacology 2000, 39, 835–841. [Google Scholar] [CrossRef]
- DeLisa, J.A. Physical Medicine and Rehabilitation: Principles and Practice, 5th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2010; p. 560. [Google Scholar]
- Acar, M.; Karatas, G.K. The effect of arm sling on balance in patients with hemiplegia. Gait Posture 2010, 32, 641–644. [Google Scholar] [CrossRef] [PubMed]
- Meyns, P.; Gestel, L.V.; Massaad, F.; Desloovere, K.; Molenaers, G.; Duysens, J. Arm swing during walking at different speeds in children with Cerebral Palsy and typically developing children. Res. Dev. Disabil. 2011, 32, 1957–1964. [Google Scholar] [CrossRef]
- Han, S.H.; Kim, T.K.; Jang, S.H.; Kim, M.J.; Park, S.B.; Yoon, S.I.; Choi, B.K.; Lee, M.Y.; Lee, K.H. The effect of an arm sling on energy consumption while walking in hemiplegic patients: A randomized comparison. Clin. Rehabil. 2011, 25, 36–42. [Google Scholar] [CrossRef] [Green Version]
- Jeong, Y.G.; Jeong, Y.J.; Koo, J.W. The effect of an arm sling used for shoulder support on gait efficiency in hemiplegic patients with stroke using walking aids. Eur. J. Phys. Rehabil. Med. 2017, 53, 410–415. [Google Scholar] [CrossRef]
- Karen, W.H.; Marjorie, E.J. Measures of adult general performance tests: The berg balance scale, dynamic gait index, gait velocity, physical performance test, timed chair stand test, timed up and go, and tinetti performance-oriented mobility assessment. Arthritis Rheum. 2003, 49, 28–42. [Google Scholar]


{kind=link}
| Condition | Number |
|---|---|
| Number of subjects | 64 |
| Gender (n) | Male 42, Female 22 |
| Age (years) | 60.02 ± 12.02 * |
| Right hemiplegia (n) | 35 |
| Left hemiplegia (n) | 29 |
| Body mass index | 24.24 ± 3.38 * |
| Shoulder abduction limited range of motion | 20.31 ± 41.36 * |
| Shoulder external rotation limited range of motion | 11.48 ± 24.16 * |
| Ankle dorsiflexion limited range of motion | 19.97 ± 16.83 * |
| Cane or walker (n) | 31 |
| Paid caregiver (n) | 28 |
| Grade | Description |
|---|---|
| 4 (Normal) | Maintaining balance without support and shifting weight in all directions without interruption or deceleration |
| 3 (Good) | Maintaining balance without support, and maintaining balance while picking object (in front of weaker foot) off floor (standing balance), and shifting weight (sitting balance) |
| 2 (Fair) | Maintaining balance without support |
| 1 (Poor) | Maintaining balance with handhold support without the help of others or other equipment or objects (backrest, wall, etc.) |
| 0 (Zero) | Requiring help of others or other equipment of objects (backrest, wall, etc.). No maintaining balance even with handhold support |
| ADL | The significant factors calculated from chi-squared test or independent t-test |
| Gait (p < 0.05) | Chi-squared test: Hip flexor/extensor/abductor/adductor, Knee flexor/extensor, Ankle dosriflexor/plantarflexor, Shoulder flexor/extensor/abductor/adductor, Elbow flexor/extensor, Wrist flexor/extensor, Hand flexor, Thumb flexor, Index flexor, Balance (sitting, standing), Position sense Independent t-test: Body mass index |
| 50 m Walking | Chi-squared test: Hip flexor/extensor/abductor/adductor, Knee flexor/extensor, Ankle dosriflexor/plantarflexor, Shoulder flexor/extensor/abductor/adductor, Elbow flexor/extensor, Wrist flexor/extensor, Thumb flexor/extensor, Index flexor/extensor, Hand flexor/extensor, Balance (sitting, standing) |
| Independent t-test: K-MMSE, Age (negative direction), Body mass index, Shoulder abduction LOM (negative direction) | |
| Feeding | Chi-squared test: Hip flexor/extensor/abductor/adductor, Knee flexor/extensor, Ankle plantarflexor, Shoulder extensor/abductor/adductor, Elbow flexor, Balance (sitting, standing), Position sense Independent t-test: Body mass index |
| Grooming | Chi-squared test: Hip flexor/extensor/abductor/adductor, Knee flexor/extensor, Ankle dorsiflexor/plantarflexor, Shoulder flexor/extensor/abductor/adductor, Elbow flexor/extensor, Wrist flexor/extensor, Hand flexor/extensor, Thumb flexor/extensor, Index flexor/extensor, Balance (sitting, standing) Independent t-test: Body mass index, Limited range of motion (negative direction: shoulder abduction/external rotation) |
| Dressing | Chi-squared test: Hip flexor/extensor/abductor/adductor, Knee flexor/extensor, Ankle dorsiflexor/plantarflexor, Shoulder flexor/extensor/abductor/adductor, Elbow flexor/extensor, Wrist flexor/extensor, Thumb flexor/extensor, Index flexor/extensor, Hand flexor/extensor, Balance (Sitting and standing), Paid caregiver Independent t-test: Age (negative direction), Body mass index, Limited range of motion (negative direction: shoulder external rotation, shoulder abduction) |
| Toileting | Chi-squared test: Hip flexor/extensor/abductor/adductor, Knee flexor/extensor Ankle dorsiflexor/plantarflexor, Shoulder flexor/extensor/abductor/adductor, Elbow flexor/extensor, Wrist flexor/extensor, Thumb flexor/extensor, Hand flexor/extensor, Index flexor/extensor, Balance (sitting and standing) Independent t-test: Age (negative direction), Body mass index, Limited range of motion (negative direction: shoulder external rotation, abduction) |
| Bathing | Chi-squared test: Hip flexor/extensor/abductor/adductor, Knee flexor/extensor, Ankle dorsiflexor/plantarflexor, Shoulder flexor/extensor/abductor/adductor, Elbow flexor/extensor, Wrist flexor/extensor, Thumb flexor/extensor, Index flexor/extensor, Hand flexor/extensor, Balance (sitting and standing), Cane, Paid caregiver, Modified Ashworth scale (ankle) Independent t-test: Age (negative direction), Body mass index, Limited range of motion (negative direction: shoulder abduction/external rotation) |
| Gait | ||||
| Sitting balance | Standing balance | Hip flexor | Hip extensor | Hip abductor |
| 0.798 ** | 0.738 ** | 0.653 ** | 0.656 ** | 0.641 ** |
| Hip adductor | Knee extensor | |||
| 0.650 ** | 0.648 ** | |||
| Feeding | ||||
| Sitting Balance | ||||
| 0.745 ** | ||||
| Grooming | ||||
| Standing balance | Sitting balance | Hip extensor | Hip abductor | Hip adductor |
| 0.653 ** | 0.616 ** | 0.625 ** | 0.644 ** | 0.649 ** |
| Hip flexor | Shoulder adductor | Knee extensor | ||
| 0.647 ** | 0.622 ** | 0.655 ** | ||
| Dressing | ||||
| Knee extensor | Standing balance | Hip abductor | Hip adductor | Shoulder extensor |
| 0.703 ** | 0.670 ** | 0.671 ** | 0.669 ** | 0.636 ** |
| Hip Flexor | Shoulder adductor | Shoulder abductor | Elbow flexor | Elbow extensor |
| 0.661 ** | 0.653 ** | 0.633 ** | 0.653 ** | 0.654 ** |
| Hip extensor | ||||
| 0.669 ** | ||||
| Toileting | ||||
| Standing balance | Hip abductor | Hip adductor | Knee extensor | Hip flexor |
| 0.648 ** | 0.607 ** | 0.610 ** | 0.634 ** | 0.608 ** |
| Hip extensor | ||||
| 0.598 ** | ||||
| Bathing | ||||
| Elbow flexor | Shoulder flexor | Shoulder extensor | Shoulder abductor | Shoulder adductor |
| 0.689 ** | 0.644 ** | 0.644 ** | 0.607 ** | 0.685 ** |
| Knee flexor | Elbow extensor | Hand flexor | Wrist extensor | Wrist flexor |
| 0.601 ** | 0.654 ** | 0.638 ** | 0.657 ** | 0651 ** |
| Thumb flexor | Knee extensor | Standing balance | ||
| 0.638 ** | 0.584 ** | 0.570 ** | ||
| 50 m walking | ||||
| Standing balance | Hip flexor | Hip extensor | Hip abductor | Hip adductor |
| 0.747 ** | 0.678 ** | 0.665 ** | 0.638 ** | 0.641 ** |
| Knee extensor | Knee flexor | Shoulder flexor | Shoulder extensor | Shoulder abductor |
| 0.686 ** | 0.646 ** | 0.600 ** | 0.621 ** | 0.611 ** |
| Shoulder adductor | Elbow flexor | Sitting balance | ||
| 0.660 ** | 0.605 ** | 0.673 ** |
| Sensitivity | Specificity | Cut-Off Value | Area Under ROC | p | |
|---|---|---|---|---|---|
| Gait | |||||
| Standing balance | 0.962 | 0.909 | 1.50 | 0.983 | 0.000 |
| Sitting balance | 0.962 | 0.818 | 2.5 | 0.901 | 0.000 |
| Hip flexor | 1 0.887 | 0.818 0.909 | 1.5 (by Maximum Youden’s index) 2.5 (by Maximum Youden’s index) | 0.951 | 0.000 |
| Hip extensor | 0.906 | 0.909 | 2.5 | 0.945 | 0.000 |
| Hip abductor | 0.962 0.868 | 0.818 0.909 | 1.5 (by Maximum Youden’s index) 2.5 (by minimum distance from left-upper corner of unit square) | 0.943 | 0.000 |
| Hip adductor | 0.962 | 0.909 | 1.5 | 0.949 | 0.000 |
| Knee extensor | 0.981 | 0.909 | 1.5 | 0.944 | 0.000 |
| Feeding | |||||
| Sitting balance | 0.962 | 0.818 | 2.5 | 0.901 | 0.000 |
| Grooming | |||||
| Sitting balance | 0.978 | 0.526 | 2.5 | 0.756 | 0.001 |
| Standing balance | 0.822 | 0.789 | 2.5 | 0.853 | 0.000 |
| Hip flexor | 0.911 | 0.737 | 3.5 | 0.87 | 0.000 |
| Hip extensor | 0.933 | 0.684 | 3.5 | 0.85 | 0.000 |
| Hip abductor | 0.933 | 0.737 | 2.5 | 0.868 | 0.000 |
| Hip adductor | 0.911 | 0.737 | 3.5 | 0.871 | 0.000 |
| Knee extensor | 0.911 | 0.737 | 3.5 | 0.871 | 0.000 |
| Shoulder adductor | 0.733 | 0.895 | 2.5 | 0.884 | 0.000 |
| Dressing | |||||
| Knee extensor | 1 | 0.643 | 3.5 | 0.866 | 0.000 |
| Standing balance | 0.917 | 0.714 | 2.5 | 0.833 | 0.000 |
| Hip adductor | 0.972 | 0.607 | 3.5 | 0.852 | 0.000 |
| Hip abductor | 1 | 0.607 | 2.5 | 0.853 | 0.000 |
| Hip flexor | 0.972 | 0.607 | 3.5 | 0.848 | 0.000 |
| Hip extensor | 1 | 0.571 | 3.5 | 0.845 | 0.000 |
| Shoulder abductor | 0.944 | 0.643 | 1.5 | 0.860 | 0.000 |
| Shoulder adductor | 0.722 | 0.893 | 3.5 | 0.871 | 0.000 |
| Shoulder extensor | 0.861 | 0.786 | 2.5 | 0.861 | 0.000 |
| Elbow flexor | 0.917 | 0.679 | 1.5 | 0.870 | 0.000 |
| Elbow extensor | 0.944 | 0.607 | 0.5 | 0.869 | 0.000 |
| Toileting | |||||
| Standing balance | 0.857 | 0.773 | 2.5 | 0.837 | 0.000 |
| Hip flexor | 0.905 | 0.636 | 3.5 | 0.834 | 0.000 |
| Hip abductor | 0.929 | 0.636 | 2.5 | 0.833 | 0.000 |
| Hip adductor | 0.952 | 0.591 | 2.5 | 0.835 | 0.000 |
| Hip extensor | 0.952 | 0.591 | 2.5 | 0.822 | 0.000 |
| Knee extensor | 0.929 | 0.682 | 3.5 | 0.845 | 0.000 |
| Bathing | |||||
| Knee flexor | 0.889 | 0.622 | 2.5 | 0.840 | 0.000 |
| Hip extensor | 1 | 0.432 | 3.5 | 0.797 | 0.000 |
| Hip adductor | 0.963 | 0.459 | 3.5 | 0.796 | 0.000 |
| Hip flexor | 0.963 | 0.459 | 3.5 | 0.792 | 0.000 |
| Shoulder adductor | 0.926 | 0.73 | 2.5 | 0.89 | 0.000 |
| Shoulder extensor | 0.963 | 0.703 | 2.5 | 0.867 | 0.000 |
| Elbow flexor | 0.815 | 0.838 | 3.5 | 0.892 | 0.000 |
| Shoulder flexor | 0.815 | 0.757 | 2.5 | 0.868 | 0.000 |
| Shoulder abductor | 1 | 0.541 | 1.5 | 0.847 | 0.000 |
| Elbow extensor | 0.889 | 0.703 | 2.5 | 0.87 | 0.000 |
| Wrist flexor | 0.630 | 0.919 | 3.5 | 0.865 | 0.000 |
| Wrist extensor | 0.630 | 0.919 | 3.5 | 0.868 | 0.000 |
| Hand flexor | 0.926 | 0.676 | 0.5 | 0.855 | 0.000 |
| Standing balance | 0.963 | 0.595 | 2.5 | 0.785 | 0.000 |
| Knee extensor | 1 | 0.486 | 3.5 | 0.806 | 0.000 |
| 50 m Walking | |||||
| Standing balance | 0.864 | 0.85 | 2.5 | 0.898 | 0.000 |
| Hip flexor | 0.932 | 0.75 | 3.5 | 0.881 | 0.000 |
| Hip extensor | 0.955 | 0.7 | 3.5 | 0.867 | 0.000 |
| Hip abductor | 0.932 | 0.7 | 2.5 | 0.859 | 0.000 |
| Hip adductor | 0.909 | 0.7 | 3.5 | 0.861 | 0.000 |
| Knee extensor | 0.932 | 0.75 | 3.5 | 0.882 | 0.000 |
| Knee flexor | 0.864 | 0.8 | 1.5 | 0.89 | 0.000 |
| Shoulder flexor | 0.795 | 0.8 | 1.5 | 0.865 | 0.000 |
| Shoulder extensor | 0.773 | 0.85 | 2.5 | 0.877 | 0.000 |
| Shoulder abductor | 0.886 | 0.75 | 1.5 | 0.872 | 0.000 |
| Shoulder adductor | 0.75 | 0.9 | 2.5 | 0.901 | 0.000 |
| Elbow flexor | 0.864 | 0.8 | 1.5 | 0.867 | 0.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.; Park, J.; Ko, Y.J. The Prognostic Factors and Required Degree Influencing the Activities of Daily Living and Gait in Brain Impairment Patients with Hemiplegia. Disabilities 2021, 1, 187-201. https://0-doi-org.brum.beds.ac.uk/10.3390/disabilities1030015
Kim S, Park J, Ko YJ. The Prognostic Factors and Required Degree Influencing the Activities of Daily Living and Gait in Brain Impairment Patients with Hemiplegia. Disabilities. 2021; 1(3):187-201. https://0-doi-org.brum.beds.ac.uk/10.3390/disabilities1030015
Chicago/Turabian StyleKim, Seungsu, Jihye Park, and Young Jin Ko. 2021. "The Prognostic Factors and Required Degree Influencing the Activities of Daily Living and Gait in Brain Impairment Patients with Hemiplegia" Disabilities 1, no. 3: 187-201. https://0-doi-org.brum.beds.ac.uk/10.3390/disabilities1030015