
Workloads of Emergency Call Types in Active-Duty Firefighters
by
 , ,
, ,
Rudi A. Marciniak
1,* ,
,
David J. Cornell
2,
Barbara B. Meyer
3,
Razia Azen
4,
Michael D. Laiosa
5 and
Kyle T. Ebersole
3 1
School of Kinesiology, College of Health, Ball State University, Muncie, IN 47306, USA
2
Department of Physical Therapy & Kinesiology, Zuckerberg College of Health Sciences, University of Massachusetts Lowell, Lowell, MA 01854, USA
3
School of Rehabilitation Sciences & Technology, College of Health Professions & Sciences, University of Wisconsin-Milwaukee, Milwaukee, WI 53211, USA
4
School of Education, College of Community Engagement & Professions, University of Wisconsin-Milwaukee, Milwaukee, WI 53203, USA
5
Joseph J. Zilber College of Public Health, University of Wisconsin-Milwaukee, Milwaukee, WI 53205, USA
*
Author to whom correspondence should be addressed.
Merits 2024, 4(1), 1-18; https://0-doi-org.brum.beds.ac.uk/10.3390/merits4010001
Submission received: 28 November 2023
/
Revised: 16 January 2024
/
Accepted: 25 January 2024
/
Published: 30 January 2024
(This article belongs to the Special Issue Current Research on Occupational Safety and Health)
Abstract
:Firefighting is an occupation with high injury risks, particularly when conducting fireground operations. The fire service generally quantifies the job demands of firefighting through tracking emergency call volume across 24 h shifts; however, volume alone does not account for the specific work completed in response to different call types. Utilization of external (i.e., objective work) and internal (i.e., intrinsic responses to work) training load measures have the potential to quantify the multifaceted workload demands of responses to medical and fire emergencies and inform injury prevention strategies. Therefore, the purpose of this study was to utilize training load measures to quantify the workloads across emergency call types. For medical emergencies and fire emergencies, the external load and the physiological, perceived, and cumulative internal loads were quantified. The results indicate that the magnitude of objective work required for fire emergency responses that include fire suppression and/or auto-extrication is approximately three times greater than that of medical and other fire emergency (i.e., no suppression or extrication) responses. Further, in response to the objective work for fire suppression and/or auto-extrication calls, the intrinsic workloads are six times more physiologically and perceptually demanding than—as well as double, cumulatively—those of medical and other fire emergency responses.
1. Introduction
Firefighting is a demanding occupation that requires the safe completion of various essential job demands which elicit responses from physiological and psychological systems [1]. The physiological demand of firefighting begins with a rapid increase in heart rate [2] in response to the sound of the alarm calling the crew to an emergency that is designated as medical or fire in nature. When responding to these emergencies, firefighters are required to work at potentially high intensities and subsequently return to lower intensity work around the fire station. Research suggests that the heart rate response to the sounding alarm is greater for fire than medical emergency calls [2]. Additionally, 6 h ambulance shifts with only medical call responses elicit lower average heart rate responses than 6 h fire rescue shifts [3], thus suggesting that both emergency types elicit physiological responses, yet fire emergencies elicit greater heart rate responses than medical emergencies. Firefighter heart rate responses during fire suppression are known to reach intensities of 95% maximal heart rate or greater [4]. Moreover, live fire emergencies often require multiple bouts of suppression where, after a short break period, the same firefighters return to the fire for additional work bouts, which subsequently increase heart rate responses with each repeated exposure [4]. Taken together, the physical demands of firefighting are extreme and unpredictable in nature, with a greater intensity elicited by fire over medical emergencies.
In addition to the physiological demands, research demonstrates that firefighting is also mentally strenuous. The presence of a live fire during a simulated ceiling overhaul elicited a heightened psychological response, as measured by task rating of perceived exertion [5]. However, across a 24 h shift with only medical emergency responses (i.e., no fire emergencies), urinary catecholamines are elevated, leading Lim and colleagues [6] to suggest that a baseline level of stress is present even in the absence of physically demanding fire calls. Further, non-fire suppression emergencies (e.g., motor vehicle accidents) are known to lead to anticipatory tension and post-call anxiety while on-duty [7]. Aside from the lack of sleep experienced on-duty as a result of emergencies occurring at any time of the day and circadian rhythm disruption [8], the on-scene trauma observed on-duty is also known to contribute to lingering hypervigilance and sleep disturbances [7]. Thus, to capture a holistic understanding of job demands in the fire service, a multi-system paradigm including physiological and psychological responses is necessary to quantify the unpredictable and cumulative demands placed on firefighters.
The fire service generally quantifies the job demands of firefighting through tracking emergency call volume across 24 h shifts at individual station locations within and across departments. Though minimal research examining call volume has been conducted, and there is not an established threshold that constitutes low, medium, and/or high call volumes, higher call volumes have been linked to greater compassion fatigue [9] and a greater likelihood for a work-related injury [10]. Despite these links to fatigue and injury, limitations to call volume as the single metric for job demands include a lack of quantification differences across single emergency calls and/or across shifts of equal call volumes. Thus, it is essential to investigate more specific and sensitive methods of work quantification at the individual call level beyond volume alone.
Among athlete populations, clinicians and practitioners utilize training, or the programmed “work” an athlete completes [11,12], to attain specific performance outcomes. The summation of work athletes complete (i.e., cumulative stress from training sessions, games, etc. over a period of time) [13] is most commonly referred to as training load. Training load has historically been utilized to monitor training adaptations in response to a training program, understand individual training responses, and identify fatigue and/or subsequent needs for recovery [14,15]. In general, loads are characterized and quantified independently as either external or internal. External training load measures are objective measures of the work completed by the participant [14,16] and, in a more general sense, can be considered the “stimulus” that the individual is performing to accomplish the parameters of the training program. Internal training loads reflect the intrinsic responses initiated by the external load stimuli [16] and include objective physiological measures (i.e., heart rate, etc.) or subjective perceptual measures (i.e., task rating of perceived exertion, etc.).
Researchers have utilized such load measures within the firefighting population to quantify firefighter workload or the quantified stimulus (i.e., external load) and response (i.e., internal load) to job demands. Specifically, workload has been examined utilizing traditional training load measures in only three known studies, including simulated settings examining the internal load of a computer-based fire scenario [17] and the influence of personal protective equipment on external and internal loads [18], as well as on-duty, to quantify the internal loads of 10 h shiftwork [19]. However, the examination of workloads across emergency response call types while on-duty remain uninvestigated. Targeting this gap may provide a unique perspective on the multifaceted demands of emergency responses to inform a more specific method for quantifying field work and injury prevention strategies. Therefore, the purpose of this study was to quantify the workload of emergency call responses, including external (i.e., objective work completed) and internal (i.e., intrinsic response to the work) loads, as well as to examine the differences in the workloads across call types.
2. Materials and Methods
2.1. Participants
After obtaining approval from the Institutional Review Board (IRB) at the University of Wisconsin-Milwaukee, study recruitment was conducted through the use of approved email correspondence, flyer distribution at individual firehouses, and speaking directly to individuals that expressed interest within a Midwest metropolitan fire department. Participants were considered eligible to participate if they were (a) at least 18 years of age; (b) a non-probationary active-duty firefighter; (c) cleared for full active-duty work; and (d) willing to give written informed consent. Participants were excluded from participating in the proposed study if they (a) reported a known cardiovascular or metabolic disease that was currently unmanaged; and/or (b) had been instructed by a physician or the Health Safety Officer to not participate in the study. Upon meeting the eligibility criteria and none of the exclusion criteria, participants that sought enrollment into the study were provided written documentation that outlined all components of the study. Researchers clearly communicated in both the written documentation and verbally that no collected data would be provided to their respective department in an individual format (i.e., non-aggregate format) and that participants could withdraw from the study at any time without consequences from the research team or their respective department.
2.2. Procedures
The study was broken into two phases for all participants (n = 38). Phase 1 of the study consisted of completing the informed consent process and determining the descriptive characteristics of the active-duty firefighters prior to continuing into Phase 2, where data were collected while on duty.
2.2.1. Phase 1
Phase 1 data collection was conducted within the Human Performance and Sport Physiology Laboratory at the University of Wisconsin-Milwaukee After completing a written informed consent, participants completed a survey for job characteristics (i.e., years of experience, rank) and self-reported their age in years (yrs) and biological sex. Following survey completion, participant height (cm) and body mass (kg) were measured to the nearest 0.01 using a medical grade balance-beam scale and stadiometer (Detecto, Webb City, MO, USA). To complete the session, participants were familiarized with the survey materials for Phase 2 and completed a practice survey.
2.2.2. Phase 2
All Phase 2 data were collected at department firehouses or in the field while participants responded to emergency calls throughout shifts that occurred between the months of April 2022 and February 2023. External load, or the objective work completed throughout each emergency call, was quantified as Impulse Load [20], and internal load, or the intrinsic (i.e., physiological and/or perceived) responses throughout each emergency call, were measured as Edwards’ Training Impulse [21], Foster’s Session Rating of Perceived Exertion [22], and the NASA-Task Load Index [23]. Accelerometer and heart rate data were collected continuously across all shifts and analyzed post hoc to quantify Impulse and Edward’s Training Impulse for all medical (MED) and fire (FIRE) calls, including those with (FIRE1) and without (FIRE0) fire suppression and/or auto-extrication tasks. Participants completed post-call surveys that were processed post hoc to quantify Foster’s Session Rating of Perceived Exertion and the NASA-Task Load Index for those calls. Due to the majority of emergencies throughout a shift being MED, participants completed surveys only after the first MED emergency of each shift in an attempt to avoid survey fatigue and to eliminate the potential impact of order of MED call (i.e., 1st MED vs. 10th MED). On the contrary, due to the unpredictable nature and lesser frequency of FIRE emergencies in particular, participants completed on-duty data collection for at least four shifts, and a maximum of six shifts, to maximize the chance of responding to at least one FIRE0 and FIRE1 call while also attempting to avoid fatigue of participation.
Impulse Load. Impulse load (IMPULSE) is a triaxial accelerometry-based measure of external mechanical load that sums the forces (i.e., acceleration of motion) from the medio-lateral, anterior–posterior, and vertical planes of motion for a task and scales the total forces by gravity (N*s) [20,24]. IMPULSE was measured utilizing the ZephyrTM Bioharness and BioModule™ device (Medtronic, Annapolis, MD, USA). Prior to the start of a shift, each participant was fitted with a Zephyr™ Bioharness™ and BioModule™ device that continuously collected on-shift IMPULSE at a sampling rate of 100 Hz across the duration of each 24 h shift. Time-stamped (HH:MM:SS) department call logs were used to mark the IMPULSE data log for the initiation (i.e., alarm sounding) and completion times (i.e., time crew was available for next call) of all MED and FIRE emergencies, such that IMPULSE was summed across all MED (IMPULSEMED) and FIRE emergency calls with (IMPULSEFIRE1) and without (IMPULSEFIRE0) fire suppression and/or auto-extrication tasks.
The Zephyr™ system has established validity through very strong relationships between triaxial acceleration measures and oxygen uptake (r = 0.97) and mean step count (r = 0.99) during an incremental treadmill protocol and precision tilt table testing [25]. Additionally, using similar protocols, Johnstone et al. [26] demonstrated very strong (ICC ≥ 0.99) between subject, intra-device, and inter-device reliability for Zephyr™ Bioharness accelerometry measures. Further, upon examination of a discontinuous incremental walk-jog-run protocol, Zephyr™ Bioharness accelerometry-derived loads (e.g., IMPULSE) demonstrate excellent precision to oxygen uptake (r > 0.90) and very strong inter-device reliability (ICC = 0.93) [27]. Though this measure remains to be validated during firefighting tasks specifically, the objective job demands of firefighting typically involve discontinuous activities (i.e., combined non-steady state tasks) similar to the aforementioned validated works [26] and prior use within field-based military training [28]. Thus, it is likely that the external load of emergency call responses are adequately represented through IMPULSE measured via Zephyr™ Bioharness accelerometry.
Edwards’ Training Impulse. Edwards’ Training Impulse (eTRIMP) was calculated to quantify the physiological internal workload for all MED and FIRE emergency calls from all collected shifts based on the time spent in five predefined heart rate (HR) zones [29]. Specifically, the same Zephyr™ BioharnessTM and BioModule™ device that continuously collected IMPULSE also continuously collected HR at a sampling rate of 250 Hz across the duration of each 24 h shift. The HR data for the entire file were converted from bpm into a percentage of maximal heart rate (HRMAX), which was quantified as HRMAX = 208 − (0.7 × Age) [30]. Following, time-stamped department call logs were used to post hoc mark the HR data per second collected throughout each of the individual MED and FIRE calls into one of the five HR intensity zones, including 50–59%HRMAX (ZONE1), 60–69%HRMAX (ZONE2), 70–79%HRMAX (ZONE3), 80–89%HRMAX (ZONE4), and ≥90%HRMAX (ZONE5), and summed into total duration (HH:MM:SS) spent in each respective zone across the call duration (i.e., the time from alarm sounding until the availability for next call). The time spent in each HR zone was multiplied by the zone’s weighting factor (e.g., ZONE1 = 1, ZONE2 = 2, ZONE3 = 3, ZONE4 = 4, ZONE5 = 5) and summed to quantify eTRIMP for all MED (eTRIMPMED) and fire emergencies with (eTRIMPFIRE1) and without (eTRIMPFIRE0) suppression and/or extrication.
Foster’s Session Rating of Perceived Exertion. Foster’s Session Rating of Perceived Exertion (sRPE) was calculated to quantify the perceived internal load across individual emergency calls. Participant Rating of Perceived Exertion (RPE) from Borg’s CR-10 scale for each task multiplied by the time spent in each call response [29] was used to quantify sRPE in alignment with prior research [22,27]. At the Phase 1 laboratory session, participants were familiarized with a paper copy of the RPE scale, which included a verbal description of the scale and an explanation of the anchors, where “0” reflected no activity (i.e., work) at all—thus, the minimum possible exertion when called to an emergency was “0.3” (i.e., very weak)—and “11” reflected the greatest exertion possible. Following this, participants completed a practice survey using a Qualtrics Software administered via their smartphone during the laboratory visit for Phase 1. In the field, the RPE for the first MED and all FIRE calls of each shift were collected using the same Qualtrics Software administered via smartphone immediately upon the completion of each call by scanning a paper-copy of a QR code. Participants were instructed to place the QR code somewhere that maximized successful completion immediately post-call, which included on the rig itself and/or somewhere at their respective station, and this resulted in survey completion enroute back to the fire station or immediately upon station return. Via Qualtrics, the RPE scale was visually presented to the participants, including each value and the associated exertional descriptor (i.e., 0 = nothing at all, 1 = very weak, etc.), along with the written prompt: “Based on the Rating of Perceived Exertion (RPE) Scale below, please type the value that indicates the exertion you experienced across this emergency call”. Following this, time-stamped department call logs were used post hoc to identify the initiation (i.e., alarm sounding) and completion (i.e., marked available for next call) of each emergency call to quantify the exact duration (HH:MM:SS) of each MED and FIRE emergency. The duration of each emergency call was multiplied by the respective call RPE to quantify sRPE for MED (sRPEMED) and FIRE emergencies with (sRPEFIRE1) and without (sRPEFIRE0) suppression and/or extrication from all survey responses.
National Aeronautics and Space Administration-Task Load Index. The NASA-Task Load Index (NASA-TLX) was utilized to assess multiple facets of load across the individual calls, including subscales of mental demand, physical demand, temporal demand, performance, effort, and frustration level. The NASA-TLX has been demonstrated as a valid measure of the workload experienced when accomplishing a task, especially as it relates to flight simulation in air aviators [31], with additional use in various occupational populations like military soldiers and medical personnel [32]. Using the same Qualtrics survey administered via smartphone for sRPE, participants completed the NASA-TLX immediately upon completion of the first MED and all FIRE calls for each shift. By completing the NASA-TLX survey after each call, participants first rated the task(s) on each subscale, which included written descriptions (Table 1), within a 100-point range on a sliding scale. Following each call, the participants also responded to pairwise comparisons of each subscale (i.e., select the factor that represents the more important contributor to the workload of the call: mental demand or effort, mental demand, or frustration, etc.) until all subscales were compared, which resulted in 15 total pairwise comparisons per call. To determine the order of relevance for each subscale to the overall call load [31], the number of times each subscale was selected by the participant as the most relevant to the call load was summed and ranged from 0 (no relevance) to 5 (more important than all other factors) [31]. The summed relevancy for each scale was multiplied by the respective subscale score (up to 100-points) to weight each factor prior to summing for an overall load score for the MED (NASA-TLXMED) and FIRE emergencies with (NASA-TLXFIRE1) and without (NASA-TLXFIRE0) suppression and/or extrication.
2.2.3. Data Processing
Upon completion of HR and IMPULSE collection across each shift via Zephyr™ BioharnessTM and BioModule™, each file was visually inspected. Upon comparison to time-stamped department call logs, any calls that included errored measures (i.e., HR missing, etc.) during the time of a call response were entirely removed from the dataset to avoid inaccurately quantifying the subsequent eTRIMP measures.
All survey responses were also visually inspected prior to quantifying sRPE and NASA-TLX workloads to ensure data accuracy. Any RPE reported as “0” was considered inaccurate due to participants being instructed that a “0” reflects no work at all, thus the minimum possible exertion when called to an emergency was “0.3” (i.e., very weak). Accordingly, any RPE responses reported as “0” were subsequently replaced with a “0.3” to reflect the lowest possible exertion. Any responses with inaccurate NASA-TLX responses (i.e., all NASA-TLX subscales = 0) were removed from the dataset and not included in the analyses.
2.3. Statistical Analysis
The IMPULSE, eTRIMP, sRPE, and NASA-TLX measures for all collected MED, FIRE0, and FIRE1 calls were averaged to obtain a single average MED, FIRE0, and FIRE1 call observation per participant. The potential differences in external and internal load between MED, FIRE0, and FIRE1 calls were examined through separate one-way repeated-measures multivariate analyses of variance (RM MANOVA) for IMPULSE, eTRIMP, sRPE, and NASA-TLX. Before statistical analysis, the normality of data for each dependent variable (e.g., IMPULSE, eTRIMP, sRPE, NASA-TLX) was examined using visual inspections of univariate Q-Q plots for the data, and z tests were performed to identify extreme univariate skewness and kurtosis. No consistent outliers across the dependent variables were identified, and the normality assumption for the RM MANOVA and post hoc calculations was satisfied. All statistical analyses were conducted utilizing SAS 9.4 Analytics Software (SAS Institute Inc., Cary, NC, USA). A Bonferroni correction was applied to protect against Type I error, where an alpha of 0.05/4 = 0.0125 was utilized to determine statistical significance for all four omnibus RM MANOVA analyses. If groups differed significantly on any outcome, an additional Bonferroni correction was applied (using the alpha level of 0.0125/3 = 0.004) to compare each pair of groups using the three post hoc group contrasts. Partial eta squared (η2p) effect sizes were also examined for all RM MANOVA analyses, with η2p < 0.06, 0.06 ≤ η2p < 0.14, and 0.14 ≤ η2p indicating small, medium, and large effects, respectively [33].
3. Results
3.1. Participant Description
Thirty-eight active-duty members of a metropolitan fire department in the Midwest volunteered to participate in this study (34 males, 4 females; 36.45 ± 8.86 yrs; 180.21 ± 6.70 cm; 92.04 ± 13.85 kg). The sample was representative of different ranks within the department and years of experience in the fire service, including Captains (n = 7; 16.57 ± 4.85 yrs), Lieutenants (n = 11; 12.63 ± 4.88 yrs), and Firefighters (n = 20; 8.30 ± 7.92 yrs). Additionally, this sample of firefighters included 10% females, and this relatively low proportion reflects the fact that roughly 5% of career firefighters are female [34].
Each participant completed data collection for 4 to 6 shifts, which resulted in an original dataset of 201 shifts. A single participant did not respond to a FIRE0 call that was captured on the Zephyr Bioharness and Biomodule across their Phase 2 collection period. Sixteen participants did not complete survey responses for FIRE0 calls, and an additional participant did not complete a survey response for a FIRE1 call, across their Phase 2 collection period. These data (i.e., Zephyr and survey) were considered missing completely at random and listwise deleted from this analysis (Table 2) [35]. Despite strong adherence by participants donning the physiological monitoring strap throughout their shift, 19 collected shifts (approximately 10% of the total) were eliminated from the dataset due to poor signal quality and/or equipment malfunction (i.e., Zephyr Bioharness) during emergency call responses.
Accordingly, 182 shifts, which represented individual responses for 1082 medical and 371 fire emergencies (FIRE0 = 228, FIRE1 = 143), as well as 289 completed call surveys, were included in the analyses. The MED call responses within this study included patients needing fall assistance, experiencing trouble breathing, requiring emergency wound care, and/or without a pulse and not breathing. The FIRE1 calls included responses to fire alarms for automobile fires and/or extrication, garage fires, appliance fires, and structure fires. All other responses to fire alarms were included as FIRE0 calls, such as elevator rescues, alarms sounding in commercial buildings, and investigations for smoke. Of the total individual call responses examined (i.e., 1082 + 371 = 1453 calls), approximately 75% were medical, which is representative of the partnering department yet slightly above average (67.2%) for fire departments in the Midwest in 2020 [36]. Additionally, approximately 9.8% of calls in this sample were FIRE1 calls, which nearly double the average fire call responses in the Midwest (4.1%) [36] despite being a typical representation of the partnering department. However, it is unclear whether auto-extrications are included in the regional average reported by the United States Fire Administration (USFA) like the FIRE1 calls reported in this study, which may be inflating the response rate in the current sample. Descriptive data for the components that inform the load calculations (i.e., call duration, etc.) are provided in Table 3.
3.2. External Load
Impulse Load
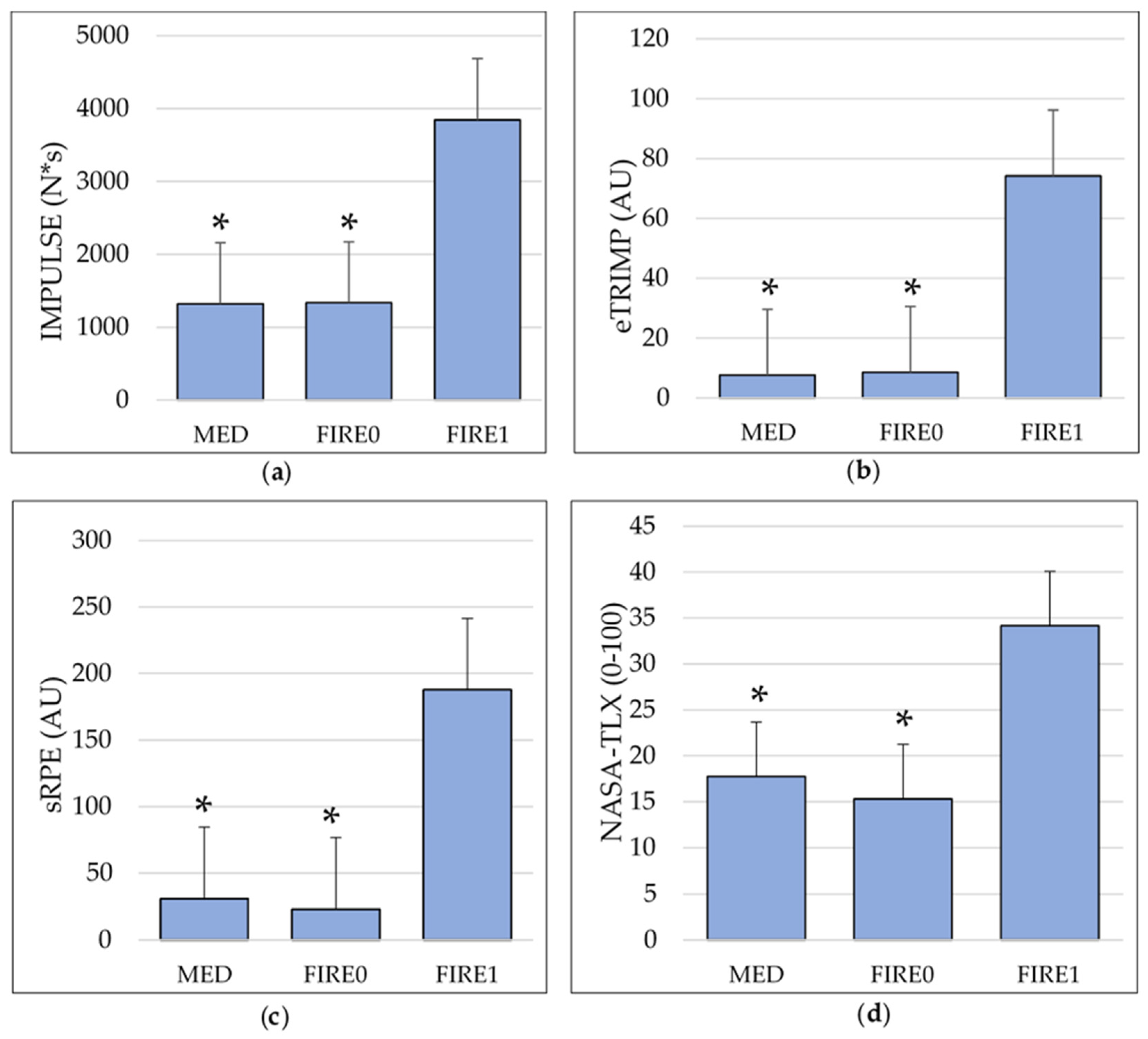
The one-way RM MANOVA identified a large significant effect of call type (F2,35 = 21.17, p < 0.001, η2p = 0.525) such that IMPULSEMED (1320.81 ± 221.05 N*s) and IMPULSEFIRE0 (1330.42 ± 375.76 N*s) were not significantly different (F1,36 = 0.02, p = 0.887), yet IMPULSEFIRE1 (3857.54 ± 2442.62 N*s) was significantly greater than both IMPULSEMED (F1,36 = 42.15, p < 0.001) and IMPULSEFIRE0 (F1,36 = 38.60, p < 0.001; Figure 1a). A summary of these results can be found in Table 4.
These results indicate that the objective work (i.e., external load) of FIRE calls that require fire suppression or the labor of auto-extrication required nearly three times the objective work demands required by MED calls or FIRE calls without suppression. Furthermore, the objective work for FIRE calls without suppression appears to be similar in magnitude to MED calls.
3.3. Internal Load
3.3.1. Edwards’ Training Impulse
The one-way RM MANOVA identified a large significant effect of call type (F2,35 = 31.84, p < 0.001, η2p = 0.569) such that eTRIMPMED (7.66 ± 6.31 AU) and eTRIMPFIRE0 (8.48 ± 7.28 AU) were not significantly different (F1,36 = 0.09, p = 0.349), yet eTRIMPFIRE1 (74.33 ± 59.84 AU) was significantly greater than both eTRIMPMED (F1,36 = 50.16, p < 0.001) and eTRIMPFIRE0 (F1,36 = 45.38, p < 0.001; Figure 1b).
These results indicate that the physiological response elicited when completing the work (i.e., external load) of FIRE calls that include fire suppression is approximately six times greater than it was for MED calls or FIRE calls that do not require suppression. However, the objective work for FIRE calls without suppression was similar to that for MED calls.
3.3.2. Foster’s Session Rating of Perceived Exertion
The one-way RM MANOVA identified a large significant effect of call type (F2,19 = 14.46, p < 0.001, η2p = 0.589) such that sRPEMED (31.02 ± 37.15 AU) and sRPEFIRE0 (23.10 ± 16.01 AU) were not significantly different (F1,20 = 1.17, p = 0.292), yet sRPEFIRE1 (187.80 ± 141.06 AU) was significantly greater than both sRPEMED (F1,20 = 28.92, p < 0.001) and sRPEFIRE0 (F1,20 = 30.43, p < 0.001; Figure 1c).
These results indicate that the perceived load response to the work (i.e., external load) of FIRE calls that require fire suppression or auto-extrication is more than six times greater than it is for MED calls or FIRE calls that do not involve fire suppression. Furthermore, though the difference was not statistically significant, it is noted that the perceived load for FIRE calls without suppression was lower than that for MED calls.
3.3.3. NASA-Task Load Index
The one-way RM MANOVA identified a large significant effect of call type (F2,19 = 24.70, p < 0.001, η2p = 0.536) such that NASA-TLXMED (17.77 ± 16.08 AU) and NASA-TLXFIRE0 (15.33 ± 10.42 AU) were not significantly different (F1,20 = 0.77, p = 0.389), yet NASA-TLXFIRE1 (34.17 ± 15.74 AU) was significantly greater than both NASA-TLXMED (F1,20 = 20.99, p < 0.001) and NASA-TLXFIRE0 (F1,20 = 51.99, p < 0.001; Figure 1d).
These results indicate that the overall internal load response to the work (i.e., external load) of FIRE calls that require fire suppression or auto-extrication is two times that of the internal load response for MED calls or FIRE calls that do not involve fire suppression. Additionally, the overall demands of FIRE calls without suppression were similar in magnitude compared to MED calls.
4. Discussion
This study is the first of its kind to specifically quantify and examine differences in workload across different types of emergency call responses utilizing both external and internal load metrics. The results indicate that the objective work and subsequent physiological, perceived, and overall internal load for FIRE calls that require fire suppression and/or auto-extrication, are significantly greater than those for MED calls or for FIRE calls that do not include suppression or extrication. Further, external and internal loads of FIRE calls that do not include suppression or extrication are not different from those of MED calls. Together, these results demonstrate that FIRE calls that include fire suppression and/or auto-extrication (i.e., FIRE1) require firefighters to complete approximately three times more work, which elicits heightened intrinsic responses above and beyond what is required for MED calls and non-suppression FIRE calls.
4.1. External Load
The results of this study are challenging to compare to the single study that has measured external load in the fire service during a simulated task [18] because the measures utilized are different. However, the external load measure utilized by Marcel-Millet et al. [18] to examine the influence of various PPE and SCBA equipment combinations on a simulated rescue task suggested that PPE without a SCBA and/or breathing tank air elicited significantly greater job demands. Marcel-Millet et al.’s [18] findings demonstrate contradictory trends from the present results where FIRE1 calls exhibited significantly greater job demands than the other call types despite being the only call category that required firefighters to fully don PPE and SCBA, as well as to breathe on air. Although this is of interest to note, the heightened load in FIRE1 calls with PPE and SCBA in the present study are likely due to the change in overall task demands rather than the addition of the SCBA and breathing on air. Specifically, Marcel-Millet et al.’s [18] simulated rescue may have required work (e.g., carrying hoses, stair climbing, victim rescue) similar to the physical labor of fire suppression calls; however, the duration of the simulation was shorter (~13 min) than FIRE1 in the present study (~42 min). These differences in duration may explain, in part, why FIRE1 in the present study elicited a greater external workload than the other call types despite PPE and SCBA donned similarly to the condition with the lowest external load in Marcel-Millet et al. [18]. However, it is also possible that if the durations were similar, the quantity of objective work in a simulated setting may still be less than that of a live emergency response. Future research should seek to quantify if such differences in objective work exist.
The majority of the literature that has utilized impulse load to quantify external load demands has been completed in traditional sport athlete populations. Specifically, the more substantial load demands of the fire suppression and/or auto-extrication calls (i.e., FIRE1) are similar to the external load of running-related movement (4534.12 ± 3552.79 N*s) during ROTC training sessions [28], as well as the positional demands of a collegiate defensive specialist (6122 ± 1972 N*s) during a volleyball match [37]. In contrast, the impulse load of the job demands for all call response types (i.e., MED, FIRE0, and FIRE1) are substantially less than the load of a women’s collegiate soccer match (~20,000 N*s) [20] and a period of U16 male soccer (~40,000 N*s) [24]. This suggests that a measure such as IMPULSE is capable of quantifying work demands in occupational populations, but that the physical work completed is less than running-based sport athletes. Given this understanding, it is critical to continue developing insight for occupational athlete workloads independent of sport athlete populations. Specifically, it is crucial to further investigate the use of external load metrics within the occupational work of firefighters as establishing a compendium of occupational athlete workload may lead to improved, targeted preparation of fire service members and mitigation of associated preventable overexertion-related injury risk.
The difference in external load demands across the emergency call types is likely the result of varying task-specific characteristics (e.g., task duration, equipment demands, physical labor). The duration of FIRE1 calls (42.75 ± 23.67 min) was greater than the duration of MED (21.15 ± 3.42 min) and FIRE0 (14.30 ± 5.86 min) calls, which allowed for greater time to accumulate work. Additionally, unlike the MED and FIRE0 calls, FIRE1 calls include the complete donning of PPE and SCBA that adds approximately 22.4 kg (~50 lbs) of mass the firefighter must maneuver [1]. Although prior research in a simulated setting suggests that the added SCBA reduced the external load demands [18], an on-duty setting is highly uncontrolled, and it is possible that the added gear influenced the external load demands differently from the simulated scenario. Additionally, MED and FIRE0 calls likely require firefighters to cover less distance (i.e., walking from rig to emergency location within a structure) compared to FIRE1 calls that often include sizeable scenes (i.e., an entire single-family dwelling, apartment complex, etc.). The added distance to traverse, in combination with the demanding physical actions completed on scene (e.g., crawling, use of heavy tools, raising ladders, overhead work, climbing) [1,38] and post-suppression clean-up (e.g., repacking hose, storing equipment back on rig) likely also contribute to the larger IMPULSE values. It may be useful for future researchers to examine whether a different accelerometer location, such as on the arm or wrist where many power-based movements elicit motion, might enhance the ability to measure IMPULSE in firefighters.
4.2. Internal Load
4.2.1. Edwards’ Training Impulse
The results of this study indicate that the physiological workload response elicited when completing the job demands (i.e., external load) of fire calls that include suppression and/or auto-extrication is six times greater than it is for other calls and indicate that job demands of suppression and/or extrication elicit substantially greater physiological workloads than non-suppressive fire calls and medical emergencies. Interestingly, the job demands of non-suppressive fire calls and medical emergencies elicited similar physiological loads.
A single study has previously examined on-duty physiological responses in firefighters, and it measured physiological load using Banister’s Training Impulse (bTRIMP) [19]. This measure utilizes an average heart rate response, whereas the present study accounts for time spent in various intensity zones (i.e., used eTRIMP). Bouzigon et al. demonstrated that the bTRIMP of different rescue tasks completed throughout a 10 h shift were similar [19]. Although a direct comparison between Bouzigon et al. [19] and the present study cannot be made due to differences in physiological load quantification (i.e., overall average heart rate response (bTRIMP) vs. time spent in five heart rate zones (eTRIMP)), the present results are inconsistent with those of Bouzigon et al. due to differences in eTRIMP being identified between FIRE1 and MED calls as well as between FIRE1 and FIRE0 call types. Marcel-Millet et al. demonstrated that the eTRIMP of a simulated rescue in PPE alone (584.3 ± 83.3 AU) elicited a significantly lower physiological load than conditions that included an SCBA without facemask (707 ± 131.6 AU) and an SCBA while on air (754.7 ± 121.1 AU) [18]. Although direct comparisons cannot be made with the present results as Marcel-Millet et al. [18] quantified eTRIMP using a different unit of time, the present study also demonstrates that FIRE1 calls, which utilize PPE and SCBA, similarly elicit the greatest physiological load.
Due to eTRIMP being primarily utilized in sport athlete populations to date, it is possible to compare the on-duty call responses of firefighters to the magnitude of physiological load elicited during athletic events. Likely as a result of the similar interval-like work experienced on the fireground, eTRIMPFIRE1 (74.17 ± 59.93 AU) appears to elicit physiological loads similar to high-intensity functional training (HIFT; 77.7 + 4.9 AU) that included five upper- and lower-body power-based exercises (i.e., push-press, sumo deadlift high-pull, etc.) to be completed in 5-min segments for three total circuits [39]. On the contrary, a different HIFT session that was shorter in duration (4 min) than MED and FIRE0 elicited a substantially greater physiological load (19.8 + 8.4 AU) than eTRIMPMED (7.66 ± 6.31 AU) and eTRIMPFIRE0 (8.58 ± 7.24 AU), thus demonstrating that load in a single MED or FIRE0 call appears to be less than a short bout of high-intensity exercise. Aside from HIFT, the physiological load of all call types examined in the present study are substantially lower than other sport athlete populations, including single training sessions for men’s semipro soccer (216.3 ± 72.6 AU) [40] and young men’s club soccer (approximately 200–400 AU) [41], as well as the average weekly load for men’s rugby training (360 ± 104 AU) [42].
As a result of the greater amount of work (i.e., external load) required during FIRE1 compared to MED or FIRE0 calls, the physiological demands placed on the body to meet such work demands is heightened and likely reflects changes in autonomic nervous system (ANS) activity. It is well-established that the ANS drives the physiological responses to firefighter work demands [2,43,44], such as increasing heart rate through withdrawal of the parasympathetic nervous system (PSNS) branch (i.e., rest and digest) and increasing control of the sympathetic nervous system (SNS) branch (i.e., fight or flight). The heightened SNS activity during each of the emergency call types is carried throughout the remainder of the job demands and to a greater extent for FIRE1. Of particular interest, despite the known heart rate response at the sound of the alarm for all fire emergencies, the heightened SNS activity throughout the remainder of the call seems to only occur in FIRE1, as evidenced by accumulated time in higher heart rate intensity zones compared to FIRE0 calls (Table 3). The prolonged elevation in SNS activity for FIRE1 may be informed by the initial job demands when arriving on-scene, which can include time-sensitive tasks (i.e., victim rescue) and other fast-paced demands that may drive SNS response to the higher-intensity zones (e.g., ZONE4-5). Following suppression and/or auto-extrication, the objective work demands for FIRE1 calls shift to other types of objective work where lower SNS demand is likely elicited, such as post-fire suppression clean up demands (e.g., repacking hose, returning equipment to rig), and accumulate external loads at lower-intensity zones similar to FIRE0 and MED. In addition to the job demands (i.e., external load) completed for FIRE1 as measured via IMPULSE, prior research demonstrates that the environmental temperature of fireground operations, and the duration of exposure to such operations, also supports greater SNS drive to elevate firefighter heart rate responses [4,43]. Therefore, it is possible that in addition to the greater objective work demands, the physiological load of FIRE1 calls may be related to the temperature of the emergency environment. Given these factors, there are likely several components that are increasing the SNS response of FIRE1 calls and contributing to the resultant eTRIMP.
The elevated SNS activity of fire calls with suppression and/or auto-extrication (i.e., FIRE1) prolonged the duration spent at lower-intensity heart rate zones compared to MED and FIRE0 calls, as well as uniquely elicited responses at the higher-intensity heart rate zones that accumulated into an eTRIMP roughly six times greater than other calls. Specifically, large portions of FIRE1 responses were spent in ZONE1 (8.51 ± 6.98 min), which was nearly twice that of MED and FIRE0 calls (4.63 ± 3.31 and 3.94 ± 2.75 min, respectively); despite the lowest-intensity zone (i.e., ZONE1) primarily contributing to the physiological load of MED and FIRE0, the totality of the duration in this low-intensity zone for both call types was nearly half that of FIRE1. A similar trend was exhibited for FIRE1 in ZONE2 (8.58 ± 7.31 min) and ZONE3 (6.23 ± 5.23 min) when compared to the shorter durations in the respective zones for MED (1.15 ± 1.25 and 0.21 ± 0.30 min) and FIRE0 (1.45 ± 1.53 and 0.46 ± 0.76 min). Thus, the lengthier durations of the FIRE1 calls in ZONE1–ZONE3 due to prolonged SNS activity contributed to the heightened physiological load over MED and FIRE0. Additionally, the SNS also evoked higher-intensity responses for FIRE1 in ZONE4 (4.38 ± 4.86 min) and ZONE5 (2.47 ± 4.43 min) compared to the minimal times spent in ZONE4 (0.03 ± 0.05 and 0.08 ± 0.16 min, respectively) and ZONE5 (0.01 ± 0.02 and 0.01 ± 0.03 min) for MED and FIRE0, respectively. As such, the accumulated times in ZONE4 and ZONE5, in tandem with the larger weighting factors that are applied to each when quantifying the physiological load (i.e., eTRIMP), supported the elevated SNS-driven physiological load for fire suppression and auto-extrication call responses (i.e., FIRE1) above and beyond medical emergencies (i.e., MED) and non-suppression fire calls (i.e., FIRE0).
The results of this study build on the foundational knowledge of previous research that has quantified peak cardiovascular demands (i.e., peak heart rate response) of fire suppression. Specifically, Horn et al. [4] demonstrated that during live-fire training operations (~15–30 min), firefighters achieved a peak cardiovascular response of at least 95% of their predicted maximal heart rate, which is similar to the maximal cardiovascular demands achieved in other training settings that included live-fire operations [45,46]. In an on-duty setting, fire suppression tasks (e.g., pike pole ventilation, victim rescue, ladder climbing) have elicited heart rate intensities up to 97% of maximal heart rate [47]. The results of the present study build on this foundational literature by demonstrating that in an on-duty fire suppression setting, maximal heart rate responses are elicited and sustained for an average accumulation of 2.47 ± 4.43 min (i.e., ZONE5). As such, it is evident that firefighters need to be capable of meeting and sustaining the maximal capacity of the cardiovascular system to meet the job demands of fire suppression and/or auto-extrication emergency responses (i.e., FIRE1). Given these findings, future researchers should consider reporting peak heart rate responses and the duration of responses in such zones to support the identification of the unique capacity needs required to sustain the maximal intensity workload of firefighting.
4.2.2. Foster’s Session Rating of Perceived Exertion
The results of the present study indicate that the perceived load response to complete the job demands (i.e., external load) of FIRE1 calls that require the complete donning of PPE and SCBA and fire suppression or auto-extrication is more than six times that of MED calls and FIRE0 calls that do not involve fire suppression. The perceived exertional load quantified by Bouzigon et al. [19] for an on-duty “person rescue” intervention (157.8 ± 117.2 AU) is similar in magnitude to the sRPE of a FIRE1 response in the present study (187.80 ± 141.06 AU) and similarly greater than the perceived exertional load of MED (31.02 ± 37.15 AU) and FIRE0 (23.10 ± 16.01 AU) calls. However, FIRE1 calls exhibited greater perceived loads when compared to a simulated rescue intervention while donning PPE alone (66.2 ± 17.0 AU), PPE and SCBA yet off air (89.5 ± 14.4 AU), and PPE and SCBA while on air (106.8 ± 21.5 AU) [18]. The duration of Marcel-Millet et al.’s [18] simulated intervention (~13 min) was longer than MED and FIRE0 calls in this study, yet much shorter than FIRE1 calls, which may explain why MED and FIRE0 exhibited lower perceived loads and FIRE1 exhibited higher perceived loads.
Similar to the physiological load of in an athletic population, FIRE1 calls exhibited perceived loads similar to those for a bout of HIFT (~160 AU) [39]. It is likely that the loads are similar due to a higher RPE during the HIFT (9.6 AU) than FIRE1 (3.5 AU), in combination with the lengthier duration of the average FIRE1 (42.75 min) than the HIFT (17 min) [39]; the load of FIRE1 is likely comparable to a bout of HIFT as a result of a longer duration rather than the tasks exhibiting similar perceived intensities. Unlike the physiological load, a shorter HIFT bout (4 min) examined by Tibana et al. [39] elicited a perceived load (~35 AU) that was similar to the average MED (31.02 ± 37.15 AU) and FIRE0 (23.10 ± 16.01 AU) calls. However, similar to FIRE1, it is likely that the loads are similar due to a higher RPE during the HIFT (8.7 AU) than MED and FIRE0 (1.06 and 1.38 AU, respectively; Table 3), combinedwith a longer duration for MED and FIRE0 calls than the HIFT bout (4 min) [39]; the similarities between HIFT and the MED and FIRE0 calls are likely comparable due to the longer duration of the emergency calls rather than the tasks exhibiting similar perceived intensities to the 4-min HIFT session. Aside from HIFT, the perceived load of FIRE1 is also similar to the perceived demands of a 75-min collegiate women’s soccer practice (143.30 ± 123.50 AU) [20] but substantially less than elite women’s (892.50 ± 358.50 AU) [20] and men’s (646.52 ± 192.88 AU) [48] soccer match play.
Prior research has demonstrated links between various mechanisms that may heighten the perceived load experienced during a task like that of the call responses in the present study. Gentles et al. [20] established that perceived load is strongly positively correlated to external load when measured as IMPULSE. As such, the perceived load of each of the emergency call types, including MED, FIRE0, and FIRE1, are likely directly informed by the job demands (i.e., external load) required of the respective emergency calls, which is supported in the mirrored magnitudes of the external and perceived load responses (Figure 1). It is also possible that, due to the established links between RPE and physiological measures like heart rate [49], the perceived exertional loads of each of the call types may similarly reflect varying physiological loads of the call responses. This is evidenced by the heightened SNS activation eliciting greater heart rate responses in FIRE1 calls and, in turn, a considerably larger physiological load (i.e., eTRIMP) that is mirrored by a similarly substantial perceived load (i.e., sRPE) response over MED and FIRE0 call types (Figure 1).
Beyond the job demands and physiological response to such demands, it is also possible that psychological factors contributed to the perceived loads of the call types examined. Specifically, as it relates to the distinct differences in perceived loads for FIRE1 compared to the other call types, the presence of a live fire is known to increase the RPE and cardiovascular response in firefighters conducting simulated fireground operations [50], and it is plausible that the live fires at scenes involving fire suppression for FIRE1 increased the RPE’s reported for those calls. Additionally, while objective work was completed in response to all emergency calls, it is also plausible that psychological stress in response to the emergency scenes and/or traumas may contribute to the perceived exertional loads [7]. The added critical-thinking and patient care required for MED emergencies may also explain why the perceived load for MED emergencies was slightly, though non-significantly, greater than it was for fire emergencies without suppression or extrication (i.e., FIRE0). These findings would suggest a potential need for future research to identify the psychological components that drive perceived demands across different emergency call responses.
4.2.3. NASA Task Load Index
The results of the present study indicate that the subjective cumulative load for fire emergency responses that involve fire suppression or auto-extrication is two times greater than fire emergency responses that do not include suppression or extrication and medical emergencies. The NASA-TLX was established for use within pilot populations and has bridged into load quantification in other athletic populations. In comparison to pilot populations, the cumulative loads of all the call types (i.e., MED, FIRE0, and FIRE1) in the present study are substantially less than the subjective cumulative load of takeoff (~58 AU) and landing (~62 AU) during a flight simulation [51]. However, the subjective cumulative loads for MED and FIRE0 calls (17.77 ± 16.08 and 15.33 ± 10.42 AU) and FIRE1 calls (34.17 ± 15.74 AU) are, respectively, similar to the cumulative loads of entire flight simulations in high- (14.93 ± 6.42 AU) and low- (39.04 ± 7.86 AU) performing Finnish Air Force pilots [52]. Aside from occupational populations, the subjective cumulative loads of all call types in this study are much lower than the subjective cumulative load of a 20-min maximal cycling bout (~70 AU) in recreational and competitive cyclists [53].
Unique to the NASA-TLX, in comparison to other load measures, is the quantification of subjective cumulative load without consideration for the task duration, thus allowing for an examination of contributions from each subscale across tasks of different durations, like the MED, FIRE0, and FIRE1 emergency responses in this study. For MED, the greatest contribution to the subjective cumulative load (Table 3) was from the mental demand (27.88%), or magnitude of perceptual activity (e.g., thinking, deciding). Additionally, upon considering the slight elevation in perceived load for medical emergencies (i.e., sRPE) compared to FIRE0 emergencies, the greater mental demand contributions to the cumulative load of medical emergencies supports the notion that psychological stress is likely a strong contributor to the workload of medical emergencies. On the contrary, the contribution of the mental demand to the cumulative subjective load of FIRE0 and FIRE1 calls are decreasingly impactful (22.92% and 20.55%, respectively). However, interestingly, the contribution of temporal demands (i.e., time pressure) increasingly contributes to FIRE0 calls without suppression and/or auto-extrication (20.58%) and FIRE1 calls with suppression and/or extrication (21.69%). Taken together, it appears that the cognitive stressors for medical calls are the result of more decision-making based demands, whereas fire calls in general are the result of more time-based demands. For contributions of performance (i.e., personal level of success in accomplishing task goals) to medical emergencies, participants attributed a greater contribution of cumulative load to performance (21.80%) compared to FIRE0 or FIRE1 calls (17.84% and 12.20%, respectively), thus suggesting that individual performance on-scene is perceived to be more influential during MED than all fire call tone emergencies. Finally, in alignment with the physiological load (i.e., eTRIMP) outcomes, the greatest contributor to the cumulative load of FIRE1 calls is the physical demand (23.57%), or the magnitude of physical activity requirements, when compared to MED (7.79%) and FIRE0 (13.20%). Future research could determine if the NASA-TLX accurately reflects cumulative workload in both simulated and on-duty settings, thus supporting the use of computer-based training scenarios to inform firefighter readiness for workload demands in the field.
4.3. Limitations and Future Research
It is important to consider these results within the confines of the study limitations. This study is representative of a sample of structural firefighters from a large, metropolitan fire department in the Midwest and therefore may not entirely represent the workload demands of emergency responses among other fire service subpopulations (e.g., volunteer firefighters, wildland firefighters). Specifically, for Midwestern department emergency responses, the reported sample distribution in medical call types reflects the average response profile; however, the fire call responses of this sample are approximately double the Midwest average according to the USFA [36]. Therefore, it is possible that these results represent expected workloads in the Midwest, especially in relation to MED call responses, but may not represent other areas of the United States. Further, future research should consider how such workloads may differ across rank, where despite completing call responses as a team, differing duties across rank (i.e., firefighter, lieutenant, and captain) may influence the workload responses of fire service members. Additionally, there are several workload quantification methods to consider. The quantification of eTRIMP in the present study relied upon an age-estimated maximum heart rate, and future research should examine how such methodology influences physiological workload metrics. It should also be noted that the surveys to quantify sRPE and NASA-TLX were administered to firefighters while returning, or once returned, to the station following a call. While this limitation is relatively unavoidable in trying to capture the workloads of calls while on-duty, an avenue of future research could be to examine if survey timing (i.e., on-scene vs. once returned to station) influences the subjective loads being measured as well as to examine if physiological, perceived, and/or cumulative load metrics are different at different times of a shift (i.e., day vs. night). Finally, due to the similarities in workload between individual calls and bouts of interval-based training quantified in the literature previously, particularly as it relates to fire calls with suppression, future research could investigate how exposure to such training may impact emergency call workloads.
5. Conclusions
This study provides an enhanced understanding of the external load, and various internal loads, across different emergency call types for structural firefighters. It is evident that the magnitude of objective work required for fire emergency responses that include fire suppression and/or auto-extrication is approximately three times greater than medical and other fire emergency (i.e., no suppression or extrication) responses. Further, the yielded intrinsic loads when accomplishing the objective job demands of a fire suppression and/or auto-extrication call are physiologically and perceptually six times greater, and double cumulatively, in comparison to the workloads of medical and other fire emergency responses (i.e., no suppression or extrication). Additionally, the workload demands of medical calls are seemingly influenced by the mental demands of the task as evidenced by the larger contributions of this subscale to the NASA-TLX and slight elevation in sRPE over non-suppression fire calls. In contrast, the workload of fire calls, particularly those that require suppression and/or extrication, appear to be driven to a greater extent by physical and temporal demands, as evidenced by the resultant physiological load (i.e., eTRIMP) and the contributions of these subscales to the NASA-TLX. Given these findings, the current use of call volume (i.e., counting total calls responded to) to indicate the work experienced on duty, particularly around fire calls, is likely flawed. Rather, consideration for the unique differences in workload across medical and fire emergency calls should be explored as it is likely that the workloads of individual firefighters are unique to the call types they respond to on-duty. Targeted preparation and recovery strategies that reflect the specific call responses of individual companies, as well as individual firefighters, should be considered for injury mitigation and personnel wellness strategies. Additionally, future research should examine the influence of different call types, particularly fire calls that require suppression and/or auto-extrication, on the workloads of 24 h shifts.
Author Contributions
Conceptualization, R.A.M., D.J.C., B.B.M., R.A., M.D.L. and K.T.E.; methodology, R.A.M., K.T.E. and R.A.; data curation, R.A.M.; writing—original draft preparation, R.A.M.; writing—review and editing, R.A.M., D.J.C., B.B.M., R.A., M.D.L. and K.T.E. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of the University of Wisconsin-Milwaukee (IRB#22.158, approved 10 February 2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author (R.A.M.). The data are not publicly available due to information that could compromise research participant confidentiality.
Acknowledgments
The authors would like to acknowledge the support of Matthew R. Ebersole for assistance with the development of programming code to analyze the call logs and the City of Milwaukee Fire Department, in particular Assistant Fire Chief Joshua Parish and the firefighter participants who made this study possible.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- National Fire Protection Association. NFPA 1582 Standard on Comprehensive Occupational Medical Program for Fire Departments. Available online: https://www.nfpa.org/codes-and-standards/all-codes-and-standards/list-of-codes-and-standards/detail?code=1582 (accessed on 28 November 2023).
- Marciniak, R.A.; Tesch, C.J.; Ebersole, K.T. Heart rate response to alarm tones in firefighters. Int. Arch. Occup. Env. Health 2021, 94, 783–789. [Google Scholar] [CrossRef] [PubMed]
- Kaikkonen, P.; Lindholm, H.; Lusa, S. Physiological load and psychological stress during a 24-hour work shift among Finnish firefighters. J. Occup. Env. Med. 2017, 59, 41–46. [Google Scholar] [CrossRef]
- Horn, G.P.; Blevins, S.; Fernhall, B.; Smith, D.L. Core temperature and heart rate response to repeated bouts of firefighting activities. Ergonomics 2013, 56, 1465–1473. [Google Scholar] [CrossRef]
- Smith, D.L.; Petruzzello, S.J.; Kramer, J.M.; Misner, J.E. The effects of different thermal environments on the physiological and psychological responses of firefighters to a training drill. Ergonomics 1997, 40, 500–510. [Google Scholar] [CrossRef] [PubMed]
- Lim, C.S.; Ong, C.N.; Phoon, W.O. Work stress of firemen as measured by heart rate and catecholamine. J. Hum. Ergol. 1987, 16, 209–218. [Google Scholar] [CrossRef]
- Barnes, B.H. The experience of traumatic stress among urban firefighters. Aust. J. Emerg. Manag. 2000, 14, 59–60. [Google Scholar]
- Billings, J.; Focht, W. Firefighter shift schedules affect sleep quality. J. Occup. Env. Med. 2016, 58, 294–298. [Google Scholar] [CrossRef] [PubMed]
- Watkins, S.L.; Shannon, M.A.; Hurtado, D.A.; Shea, S.A.; Bowles, N.P. Interactions between home, work, and sleep among firefighters. Am. J. Ind. Med. 2021, 64, 137–148. [Google Scholar] [CrossRef]
- Blackwell, K.C.; Vaughn Becker, D.; Adams, G. Hot cognition: Exploring the relationship between excessive call volume and cognitive fatigue. FireFighter Health Saf. 2011, 7, 88–93. [Google Scholar]
- Gabbett, T.J.; Nassis, G.P.; Oetter, E.; Pretorius, J.; Johnston, N.; Medina, D.; Rodas, G.; Myslinski, T.; Howells, D.; Beard, A.; et al. The athlete monitoring cycle: A practical guide to interpreting and applying training monitoring data. Br. J. Sports Med. 2017, 51, 1451–1452. [Google Scholar] [CrossRef]
- Gabbett, T.J.; Ullah, S. Relationship between running loads and soft-tissue injury in elite team sport athletes. J. Strength Cond. Res. 2012, 26, 953–960. [Google Scholar] [CrossRef]
- Gabbett, T.J.; Whyte, D.G.; Hartwig, T.B.; Wescombe, H.; Naughton, G.A. The relationship between workloads, physical performance, injury and illness in adolescent male football players. Sports Med. 2014, 44, 989–1003. [Google Scholar] [CrossRef]
- Bourdon, P.C.; Cardinale, M.; Murray, A.; Gastin, P.; Kellmann, M.; Varley, M.C.; Gabbett, T.J.; Coutts, A.J.; Burgess, D.J.; Gregson, W.; et al. Monitoring athlete training loads: Consensus statement. Int. J. Sports Physiol. Perform 2017, 12, 161–170. [Google Scholar] [CrossRef] [PubMed]
- Jones, C.M.; Griffiths, P.C.; Mellalieu, S.D. Training Load and Fatigue Marker Associations with Injury and Illness: A Systematic Review of Longitudinal Studies. Sports Med. 2017, 47, 943–974. [Google Scholar] [CrossRef] [PubMed]
- Impellizzeri, F.M.; Marcora, S.M.; Coutts, A.J. Internal and external training load: 15 years on. Int. J. Sports Physiol. Perform. 2019, 14, 270–273. [Google Scholar] [CrossRef] [PubMed]
- Webb, H.E.; McMinn, D.R.; Garten, R.S.; Beckman, J.L.; Kamimori, G.H.; Acevedo, E.O. Cardiorespiratory responses of firefighters to a computerized fire strategies and tactics drill during physical activity. Appl. Erg. 2010, 41, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Marcel-Millet, P.; Ravier, G.; Groslambert, A. Effect of protective equipment on firefighters’ external and internal workloads during a simulated rescue intervention. J. Strength. Cond. Res. 2020, 36, 2291–2297. [Google Scholar] [CrossRef] [PubMed]
- Bouzigon, R.; Ravier, G.; Paulin, P.; Grappe, F. The use of two different methods of workload quantification in firefighters. Sci. Sports 2015, 30, 169–172. [Google Scholar] [CrossRef]
- Gentles, J.A.; Coniglio, C.L.; Besemer, M.M.; Morgan, J.M.; Mahnken, M.T. The demands of a women’s college soccer season. Sports 2018, 6, 16. [Google Scholar] [CrossRef] [PubMed]
- Edwards, S. The Heart Rate Monitor Book; Polar Electro Oy: New York, NY, USA, 1993; ISBN 0963463306. [Google Scholar]
- Foster, C. Monitoring training in athletes with reference to overtraining syndrome. Med. Sci. Sports Exerc. 1998, 30, 1164–1168. [Google Scholar] [CrossRef]
- Gawron, V.J. NASA Task Load Index. In Human Performance Measures Handbook; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 2000; pp. 130–135. ISBN 0-8058-3701-9. [Google Scholar]
- Gómez-Carmona, C.D.; Pino-Ortega, J.; Sánchez-Ureña, B.; Ibáñez, S.J.; Rojas-Valverde, D. Accelerometry-based external load indicators in sport: Too many options, same practical outcome? Int. J. Env. Res. Public Health 2019, 16, 5101. [Google Scholar] [CrossRef]
- Johnstone, J.A.; Ford, P.A.; Hughes, G.; Watson, T.; Garrett, A.T. BioharnessTM multivariable monitoring device. Part I: Validity. J. Sports Sci. Med. 2012, 11, 400–408. [Google Scholar]
- Johnstone, J.A.; Ford, P.A.; Hughes, G.; Watson, T.; Garrett, A.T. BioharnessTM multivariable monitoring device. Part II: Reliability. J. Sports Sci. Med. 2012, 11, 409–417. [Google Scholar] [PubMed]
- Johnstone, J.A.; Ford, P.A.; Hughes, G.; Watson, T.; Mitchell, A.C.S.; Garrett, A.T. Field based reliability and validity of the bioharnessTM multivariable monitoring device. J. Sports Sci. Med. 2012, 11, 643–652. [Google Scholar]
- Zadeh, A.; Taylor, D.; Bertsos, M.; Tillman, T.; Nosoudi, N.; Bruce, S. Predicting sports injuries with wearable technology and data analysis. Inf. Syst. Front. 2020, 23, 1023–1037. [Google Scholar] [CrossRef]
- Sanders, D.; Abt, G.; Hesselink, M.K.C.; Myers, T.; Akubat, I. Methods of monitoring training load and their relationships to changes in fitness and performance in competitive road cyclists. Int. J. Sports Physiol. Perform 2017, 12, 668–675. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Monahan, K.D.; Seals, D.R. Age-predicted maximal heart rate revisited. J. Am. Coll. Cardiol. 2001, 37, 153–156. [Google Scholar] [CrossRef] [PubMed]
- Hart, S.G.; Staveland, L.E. Development of NASA-TLX (Task load index): Results of empirical and theoretical research. In Human Mental Workload; Hancock, P.A., Meshkati, N., Eds.; Elsevier: Amsterdam, NL, USA, 1988; pp. 139–178. [Google Scholar]
- Hart, S.G. Nasa-task load index (NASA-TLX); 20 years later. Proc. Hum. Factors Ergon. Soc. 50th Annu. Meet. 2006, 50, 904–908. [Google Scholar] [CrossRef]
- Huck, S.W. Two-way analyses of variance. In Reading Statistics and Research, 6th ed.; Pearson: London, UK, 2012; pp. 276–311. ISBN 978-0132178631. [Google Scholar]
- Fahy, R.; Evarts, B.; Stein, G.P. U.S. Fire Department Profile. 2020. Available online: https://www.nfpa.org/education-and-research/research/nfpa-research/fire-statistical-reports/us-fire-department-profile?l=0 (accessed on 28 November 2023).
- Sainani, K.L. Dealing with missing data. PMR 2015, 7, 990–994. [Google Scholar] [CrossRef]
- United States Fire Administration. Fire Department Overall Run Profile as Reported to the National Fire Incident Reporting System (2020). Available online: https://www.usfa.fema.gov/downloads/pdf/statistics/v22i1-fire-department-run-profile.pdf (accessed on 28 November 2023).
- Coniglio, C.L.; Smith, A.; Bursais, A.; Kirkpatrick, J.; Justin, T. Training loads of a Division I conference volleyball tournament. In Proceedings of the East Tennessee State University College and Sport Science College Proceedings, Johnson City, TN, USA, 30 November–1 December 2018. [Google Scholar]
- Gledhill, N.; Jamnik, V.K. Characterization of the physical demands of firefighting. Can. J. Sport. Sci. 1992, 17, 207–213. [Google Scholar]
- Tibana, R.A.; de Sousa, N.M.F.; Cuhna, G.V.; Prestes, J.; Fett, C.; Gabbett, T.J.; Voltarelli, F.A. Validity of session rating perceived exertion method for quantifying internal training load during high-intensity functional training. Sports 2018, 6, 68. [Google Scholar] [CrossRef] [PubMed]
- Casamichana, D.; Castellano, J.; Calleja-Gonzalez, J.; Roman, J.S.; Castagna, C. Relationship between indicators of training load in soccer players. J. Strength. Cond. Res. 2013, 27, 369–374. [Google Scholar] [CrossRef]
- Impellizzeri, F.M.; Rampinini, E.; Coutts, A.J.; Sassi, A.; Marcora, S.M. Use of RPE-based training load in soccer. Med. Sci. Sports Exerc. 2004, 36, 1042–1047. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.J.; Sanders, D.; Myers, T.; Abt, G.; Taylor, C.A.; Akubat, I. The dose-response relationship between training load and aerobic fitness in academy rugby union players. Int. J. Sports Physiol. Perform 2018, 13, 163–169. [Google Scholar] [CrossRef]
- Smith, D.L.; DeBlois, J.P.; Kales, S.N.; Horn, G.P. Cardiovascular strain of firefighting and the risk of sudden cardiac events. Exerc. Sport. Sci. Rev. 2016, 44, 90–97. [Google Scholar] [CrossRef] [PubMed]
- Kesler, R.M.; Ensari, I.; Bollaert, R.E.; Motl, R.W.; Hsiao-Wecksler, E.T.; Rosengren, K.S.; Fernhall, B.; Smith, D.L.; Horn, G.P. Physiological response to firefighting activities of various work cycles using extended duration and prototype SCBA. Ergonomics 2018, 61, 390–403. [Google Scholar] [CrossRef]
- Colburn, D.; Suyama, J.; Reis, S.E.; Morley, J.L.; Goss, F.L.; Chen, Y.; Moore, C.G.; Hostler, D. A comparison of cooling techniques in firefighters after a live burn evolution. Prehosp Emerg. Care 2011, 15, 226–232. [Google Scholar] [CrossRef]
- Smith, D.L.; Petruzzello, S.J.; Chludzinski, M.A.; Reed, J.J.; Woods, J.A. Selected hormonal and immunological reponses to strenuous live-fire firefighting drills. Ergonomics 2005, 48, 55–65. [Google Scholar] [CrossRef]
- Sothmann, M.S.; Saupe, K.; Jasenof, D.; Blaney, J. Heart rate response of firefighters to actual emergencies. Implications for cardiorespiratory fitness. J. Occup. Med. 1992, 34, 797–800. [Google Scholar] [CrossRef]
- Enes, A.; Oneda, G.; Alves, D.L.; de Palumbo, P.D.; Cruz, R.; Moiano Junior, J.V.M.; Novack, L.F.; Osieki, R. Determinant factors of the match-based internal load in elite soccer players. Res. Q. Exerc. Sport 2021, 92, 63–70. [Google Scholar] [CrossRef]
- Borg, G.A.V. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.L.; Petruzzello, S.J.; Kramer, J.M.; Misner, J.E. Physiological, psychophysical, and psychological responses of firefighters to training drills. Aviat. Space Env. Med. 1996, 67, 1063–1068. [Google Scholar]
- Alaimo, A.; Esposito, A.; Orlando, C.; Simoncini, A. Aircraft pilots workload analysis: Heart rate variability objective measures and NASA-Task Load Index subjective evaluation. Aerospace 2020, 7, 137. [Google Scholar] [CrossRef]
- Mansikka, H.; Virtanen, K.; Harris, D. Comparison of NASA-TLX scale, modified Cooper–Harper scale and mean inter-beat interval as measures of pilot mental workload during simulated flight tasks. Ergonomics 2019, 62, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Kesisoglou, A.; Nicolò, A.; Passfield, L. Cycling performance and training load: Effects of intensity and duration. Int. J. Sports Physiol. Perform. 2021, 16, 535–543. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Differences in external and internal workloads across emergency call types: (a) Impulse; (b) Edward’s Training Impulse; (c) Foster’s Session Rating of Perceived Exertion; (d) NASA-Task Load Index. *, significantly different from FIRE1.
Figure 1.
Differences in external and internal workloads across emergency call types: (a) Impulse; (b) Edward’s Training Impulse; (c) Foster’s Session Rating of Perceived Exertion; (d) NASA-Task Load Index. *, significantly different from FIRE1.


{kind=link}
Table 1.
NASA-TLX subscale descriptions.
| Description | |
|---|---|
| Mental Demand | How much mental and perceptual activity was required (e.g., thinking, deciding, calculating, remembering, looking, searching, etc.)? Was the task easy or demanding, simple or complex, exacting or forgiving? |
| Physical Demand | How much physical activity was required (e.g., pushing, pulling, turning, controlling, activating, etc.)? Was the task easy or demanding, slow or brisk, slack or strenuous, restful or laborious? |
| Temporal Demand | How much time pressure did you feel due to the rate of pace at which the tasks or task elements occurred? Was the pace slow and leisurely or rapid and frantic? |
| Performance | How successful do you think you were in accomplishing the goals of the task? How satisfied were you with your performance in accomplishing these goals? |
| Effort | How hard did you have to work (mentally and physically) to accomplish your level of performance? |
| Frustration Level | How insecure, discouraged, irritated, stressed, and annoyed versus secure, gratified, content, relaxed, and complacent did you feel during the task? |
Table 2.
Participant sample sizes (N) per statistical analysis.
| MED | FIRE0 | FIRE1 | RM MANOVA Sample | |
|---|---|---|---|---|
| IMPULSE | 38 | 37 | 38 | 37 |
| eTRIMP | 38 | 37 | 38 | 37 |
| sRPE | 38 | 22 | 37 | 21 |
| NASA-TLX | 38 | 22 | 37 | 21 |
Table 3.
Descriptive statistics (Mean ± SD) of load components across emergency call types.
| Component | MED | FIRE0 | FIRE1 |
|---|---|---|---|
| Call Duration (min) | 21.15 ± 3.42 | 14.30 ± 5.86 | 42.75 ± 23.67 |
| RPE (AU) | 1.06 ± 0.84 | 1.38 ± 0.85 | 3.53 ± 1.22 |
| Heart Rate Zones (Total Time Per Call, min) | |||
| ZONE1 | 4.63 ± 3.31 | 3.94 ± 2.75 | 8.51 ± 6.98 |
| ZONE2 | 1.15 ± 1.25 | 1.45 ± 1.53 | 8.58 ± 7.31 |
| ZONE3 | 0.21 ± 0.30 | 0.46 ± 0.76 | 6.23 ± 5.23 |
| ZONE4 | 0.03 ± 0.05 | 0.08 ± 0.16 | 4.38 ± 4.86 |
| ZONE5 | 0.01 ± 0.02 | 0.01 ± 0.03 | 2.47 ± 4.43 |
| Heart Rate Zones (Percent of Call Duration, %) | |||
| ZONE1 | 21.89 ± 15.65 | 27.55 ± 19.23 | 19.91 ± 16.33 |
| ZONE2 | 5.44 ± 5.91 | 10.14 ± 10.70 | 20.07 ± 17.10 |
| ZONE3 | 0.99 ± 1.42 | 3.22 ± 5.31 | 14.57 ± 12.23 |
| ZONE4 | 0.14 ± 0.24 | 0.56 ± 1.12 | 10.25 ± 11.37 |
| ZONE5 | 0.00 ± 0.00 | 0.00 ± 0.21 | 5.78 ± 10.36 |
| NASA-TLX Raw Scores (0–100) | |||
| Mental Demand | 16.95 ± 15.97 | 12.89 ± 8.22 | 38.20 ± 23.71 |
| Physical Demand | 11.10 ± 12.21 | 12.18 ± 7.92 | 43.69 ± 23.31 |
| Temporal Demand | 14.57 ± 18.04 | 11.70 ± 8.37 | 39.28 ± 22.81 |
| Performance | 22.32 ± 31.14 | 20.46 ± 31.52 | 24.63 ± 29.14 |
| Effort | 13.86 ± 13.11 | 13.75 ± 9.55 | 40.72 ± 22.84 |
| Frustration | 12.84 ± 13.85 | 6.42 ± 5.26 | 16.02 ± 10.48 |
| NASA-TLX Weighted Contribution (%) | |||
| Mental Demand | 27.88 ± 17.40 | 22.92 ± 13.81 | 20.55 ± 14.16 |
| Physical Demand | 7.79 ± 10.26 | 13.20 ± 12.62 | 23.57 ± 13.44 |
| Temporal Demand | 14.88 ± 12.20 | 20.58 ± 12.80 | 21.69 ± 12.72 |
| Performance | 21.80 ± 22.56 | 17.84 ± 15.12 | 12.20 ± 13.53 |
| Effort | 14.30 ± 9.48 | 18.30 ± 9.99 | 18.99 ± 9.44 |
| Frustration | 13.35 ± 13.69 | 7.15 ± 8.92 | 3.00 ± 4.89 |
Table 4.
Results summary of omnibus test results and least significant differences.
| Omnibus Test Results | Call Type (Mean ± SD) | |||
|---|---|---|---|---|
| Wilks’ Lambda | ||||
| F Value | MED | FIRE0 | FIRE1 | |
| Impulse (N*s) | ||||
| 21.17 * | 1320.81 ± 221.05 | 1330.42 ± 375.76 | 3857.54 ± 2442.62 ab | |
| eTRIMP (AU) | ||||
| 31.84 * | 7.67 ± 6.31 | 8.48 ± 7.28 | 74.33 ± 59.84 ab | |
| sRPE (AU) | ||||
| 14.46 * | 31.02 ± 37.15 | 23.11 ± 16.01 | 187.80 ± 141.06 ab | |
| NASA-TLX (0–100) | ||||
| 24.70 * | 17.77 ± 16.08 | 15.33 ± 10.42 | 34.17 ± 15.74 ab | |
*, p < 0.001; a, significantly different from MED; b, significantly different from FIRE0.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Marciniak, R.A.; Cornell, D.J.; Meyer, B.B.; Azen, R.; Laiosa, M.D.; Ebersole, K.T. Workloads of Emergency Call Types in Active-Duty Firefighters. Merits 2024, 4, 1-18. https://0-doi-org.brum.beds.ac.uk/10.3390/merits4010001
AMA Style
Marciniak RA, Cornell DJ, Meyer BB, Azen R, Laiosa MD, Ebersole KT. Workloads of Emergency Call Types in Active-Duty Firefighters. Merits. 2024; 4(1):1-18. https://0-doi-org.brum.beds.ac.uk/10.3390/merits4010001
Chicago/Turabian StyleMarciniak, Rudi A., David J. Cornell, Barbara B. Meyer, Razia Azen, Michael D. Laiosa, and Kyle T. Ebersole. 2024. "Workloads of Emergency Call Types in Active-Duty Firefighters" Merits 4, no. 1: 1-18. https://0-doi-org.brum.beds.ac.uk/10.3390/merits4010001