
Multifactorial Effects of COVID-19: A Review of Published Autopsy Reports
by
 , , ,
, , ,
Karan Chawla
1,* ,
,
Stephen Hong
1,
Ryan Shields
1,
Alexandra Ford
1,
Gioia Pacella
2 and
Fedor Lurie
3,4 1
Department of Medical Microbiology and Immunology, University of Toledo College of Medicine and Life Sciences, Toledo, OH 43614, USA
2
Department of Biology, John Carroll University, University Heights, OH 44118, USA
3
Jobst Vascular Institute, Promedica Healthcare System, Toledo, OH 43606, USA
4
Division of Vascular Surgery, University of Michigan, Ann Arbor, MI 43606, USA
*
Author to whom correspondence should be addressed.
COVID 2022, 2(5), 553-568; https://0-doi-org.brum.beds.ac.uk/10.3390/covid2050041
Submission received: 20 March 2022
/
Revised: 19 April 2022
/
Accepted: 25 April 2022
/
Published: 27 April 2022
Abstract
:We systematically reviewed published data on autopsies of patients who died from COVID-19 to identify pathological changes that are consistently reported in autopsies and those that were reported anecdotally, and to compare consistent findings with autopsy findings in similar diseases. The MEDLINE, Google Scholar, and Embase databases were searched for full-text articles in the English language from December 2019 to March 2021 to include publications on autopsy findings in patients whose main cause of death was COVID-19 and COVID-19-related complications. This review included 124 published papers documenting COVID-19 patient autopsies for over 1100 patients. Most frequent and consistently reported pathological findings included diffuse alveolar damage in the lungs, cardiac inflammation, and hypertrophy, vascular microthrombi, shock kidney and acute tubular necrosis, congested liver and spleen, and shock-associated changes in other organs. These findings by themselves were not unique, and were similar to other severe viral infections and septic shock. However, the frequency of diffuse alveolar damage and the extent of microvascular thrombosis were much higher among the autopsies of patients who had died from COVID-19 compared with other severe viral infections. Autopsy data confirm clinical reports of high incidences of diffuse alveolar damage and microvascular thrombosis in the most severe cases of COVID-19 that caused death.
1. Introduction
As of 30 June 2020, an estimated 41% of U.S. adults reported that they delayed or avoided medical care during the pandemic due to concerns of contracting COVID-19, and 12% of these U.S. adults also reported avoiding urgent and emergency care [1]. This delay and/or decreased utilization of medical care could be the cause of increased negative patient outcomes in preventable and treatable conditions. As the coronavirus disease 2019 (COVID-19) pandemic reaches its third year, a multitude of preventative and treatment modalities have been developed that hope to control the spread of the disease. These include various COVID-19 vaccines and treatment strategies that range from new drugs like Paxlovid and simple hospital maneuvers like placing patients in prone position [2]. The pathogenesis of COVID-19 is complex with a multitude of factors leading to varying levels of injury to the lungs and numerous other organs. New data suggest that this disease causes other sequelae outside the traditional lung findings found in other viruses within the Coronaviridae family that can contribute to other serious morbidities. This review of 124 published papers documenting COVID-19 patient autopsies includes over 1100 patients and will act as a timestamp of COVID-19 patients who did not have new treatment technologies that exist today, giving a clearer picture of the first few variants (Figure 1).
2. Methods
A systematic review was performed using the PRISMA (preferred reporting items for systematic reviews and meta-analyses) guidelines. Search strategy: The MEDLINE, Google Scholar, and Embase databases were searched for full-text articles in the English language from December 2019 to March 2021without restriction. This review will not cover COVID-19 vaccine complications, as the endpoint of this study was March 2021.
2.1. Selection Criteria
This search was conducted using all available reports prior to March 2021. Any article providing autopsy reports of patients who had died from COVID-19 was included. Any data that ranged from specific organ systems or histological findings to full autopsy reports were included in the study. There was no restriction on the age, sex, or ethnicity of the patient as long as the main cause of death was from COVID-19 and COVID-19-related complications. Duplicated reports and findings found in separate articles were excluded (Figure 2). Study selection, data extraction, and risk of bias assessment were then performed by two independent reviewers (FL) and any conflicts were discussed in person.
2.2. Study Organization and Analysis
After all search engine results were screened, the articles that passed the initial selection criteria had their findings listed by organ system. The findings were placed in subcategories within each organ system. These subcategories were quantified by the number of patients found within each group. The prevalence of these findings was calculated using the number of patients in each subcategory divided by the number of patients that had data related to the organ system. All data extraction was performed by the four reviewers (KC, AF, SH, and RS) independently.
3. Results
3.1. Lung Findings
Of the 124 studies, 90 papers discussed lung findings in their autopsy reports. This represents 866 patients in this review (Table 1). The most common finding indicates that many of these patients had died with diffuse alveolar damage (DAD) (65.4%) [3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67] with type II pneumocyte hyperplasia (19.5%) [11,12,15,18,26,30,31,43,44,47,48,54,55,58,60,63,66,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84] and lymphocyte dominant inflammation (10.3%) [4,5,11,12,15,19,28,38,48,50,54,57,59,63,66,68,69,72,73,75,83,85,86,87]. This was to be expected as the most common initial and notable end-stage symptoms of COVID-19 are respiratory related. Under the umbrella of DAD, many of the reports indicated alveolar edema (29.1%) [10,14,15,16,19,25,29,30,31,38,43,44,46,47,48,49,53,54,55,58,59,60,61,62,63,67,70,74,75,80,81,82,83,87,88,89,90,91,92,93,94], and hyaline membrane (27.5%) [4,5,6,10,16,21,23,26,28,30,31,34,38,43,44,45,47,48,54,55,60,62,66,67,71,72,75,76,79,80,81,82,83,95,96,97] formation at the microscopic level. An interesting finding from these reports also showed a high number of patients with alveolar hemorrhage (19.2%) [10,12,15,16,19,23,24,30,38,55,57,61,63,66,68,70,71,72,73,74,83,84,86,88,89,95,96,98,99] and thrombus formation (9.8%) [12,21,30,33,46,60,66,67,74,84,89,100] within the parenchyma of the lungs.
3.2. Heart Findings
Of the 124 studies, 52 papers discussed cardiac findings; this represents 502 patients. The most common findings include cardiac inflammation (36.9%, 185/502) [3,12,13,19,25,26,31,35,44,51,58,68,71,79,83,85,88,94,95,101,102,103,104,105], hypertrophy (19.9%, 100/502) [13,14,21,26,31,42,55,56,59,73,85,96,97,104,105,106,107], fibrosis (26.3%, 132/502) [4,9,14,19,21,31,49,56,86,88,103,105], cardiomegaly (20.1%, 101/502) [7,14,29,36,47,55,58,60,62,72,85,86,96,97,98], and dilation (7.2%, 36/502) [34,36,42,47,70,73,92,95,98,107]. The various heart pathologies found in autopsy are interesting findings as pulmonary pathologies are the most common complication with COVID-19 infection.
3.3. Vascular Findings
Vascular clotting-associated pathologies are among the major complications observed in severe cases of COVID-19. Numerous studies have identified vascular microthrombi as a principal pathologic finding at autopsy in patients infected with SARS-CoV-2. In this review of 124 published papers documenting COVID-19 autopsies, which included over 1100 patients, we identified 771 patients with vascular pathology. Specifically, 57% (437/771) [4,8,9,10,12,14,15,17,18,19,20,21,22,24,26,27,28,29,31,35,40,41,42,43,45,46,47,49,53,56,57,58,62,63,68,76,85,86,90,97,98,100,103,105,106,108,109,110,111,112,113] of these patients were found to have vascular thrombi, while 15% (116/771) [26,36,41,53,68,92,104,106,114] were found to have inflammatory cell infiltrates of the vasculature. Our analysis was limited by the authors’ descriptions of the observed thrombi, with many authors not specifying the type of vasculature or the location of the thrombi. However, in the 528 cases where thrombosis was specifically categorized, microvascular thrombosis was overwhelmingly more common than macrovascular [9,12,14,18,20,21,26,28,29,31,35,41,42,45,46,47,57,58,68,97,107,109,111,112], being observed in 67% (356/528) [4,8,9,10,14,15,17,19,20,21,22,24,26,27,28,29,30,31,35,40,43,45,47,49,53,56,57,58,62,63,76,85,86,90,98,100,103,105,106,110,112,113] of cases (Figure 3).
3.4. Kidneys
Of the 124 studies, 38 papers talked about kidney findings, representing 427 patients, making it the most commonly noted problem; 112 patients (26%) [4,31,35,56,68,107] showed arteriosclerosis of the arteries feeding the kidneys [26], 81 (19%) [68,107] had shock kidney, and 80 (18%) [13,35,36,39,55,56,62,88,93,101,105,115] had acute tubular necrosis.
3.5. Spleen
3.6. Liver
Of the 124 studies, 41 papers elaborated about liver findings of COVID-19. This represents 407 (35%) patients in this review. Of the 407 patients with liver findings 102 had congestion (25%) [38,47,60,68,105,107], 107 had steatosis (26%) [4,6,14,29,31,32,34,35,38,51,56,58,60,62,71,100,101], and 84 had shock liver (20%) [13,68,107].
3.7. Remaining Affected Organ Systems
Prostate: 94 (8%); most common finding was thrombosis, 86 patients (91%) [68,107]. Bowel: 162 (14%); most common finding was shock changes, 80 patients (49%) [68]. Pharynx: 8 (1%); most common finding was lymphocytic pharyngitis (88%) [68]. Adrenal glands: 53 (5%); most common finding was lesions (23%) [90]. Testis: 33 (3%); most common finding was interstitial edema, 17 patients (52%) [78,116]. Brain: 109 (10%); most common finding was hypoxic-ischemic injury, 20 patients (18%) [76,81,117]. Cutaneous: 19 (2%); most common finding was thrombotic microangiopathy, 10 patients (53%) [56,91]. Pancreas: 13 (1%); most common finding was necrosis, 5 patients (38%) [59,101]. Lymph nodes: 18 (2%); most common findings were enlarged mediastinal (14 patients (78%)) [38,59] and hilar pulmonary lymph nodes (14 patients (78%)) [38,59], and loss of germinal centers, 11 patients (61%) [59]. Eyes: 3 (0.3%); most common findings were autolysis (3 patients (100%)) and cataracts (3 patients (100%)) [99]. Placenta: 1 (0.1%); most common findings were subchorial inflammation (1 patient (100%)), intervillous fibrin deposits (1 patient (100%)), and funisitis (1 patient (100%)) [82]. Olfactory bulbs: 2 (0.2%); most common findings were edema (2 patients (100%)), neuronal degeneration (2 patients (100%)), neuronal necrosis (2 patients (100%)), and inflammatory infiltrate (2 patients (100%)) [65]. Mouth: 7 (0.6%); most common finding was morphologic alteration in keratinocytes of junctional epithelium, 7 patients (100%) [66].
4. Discussion
While most patients infected with SARS-CoV-2 experience only mild illness, approximately 5% of patients develop severe lung injury or even multiorgan dysfunction, resulting in a 1–4% case fatality ratio [118]. Viral sepsis closely resembles the clinical manifestations of severe or critically ill COVID-19 patients; as such, a comparison between the two disease processes may provide a more accurate description of COVID-19′s pathologic effects.
To begin a comparison, SARS-CoV-1 was examined first due to its relation to SARS-CoV-2 and to evaluate any evolution of their pathologies that may have occurred between these two viruses. Unchanged for SARS-CoV-2, SARS-CoV-1 binding domains specifically bind to angiotensin-converting enzyme 2 (ACE2) [119]. High viral loads were found in the epithelium of the respiratory, gastrointestinal, renal distal tubules, neurons of the brain, and macrophages across multiple organ systems. Two notable characteristics for SARS-CoV-1 are a major depletion of immune cells within immunogenic organs and lymph nodes and neuronal changes that included edema and scattered red degeneration [119]. Direct lymphocyte damage and not immune overreaction causing immune injury was a hallmark of the pathogenesis of SARS-CoV-1. In terms of vasculature, peripheral microthrombi formation and macroscopic pulmonary thromboemboli have also been noted in SARS-CoV-1 autopsies [120,121]. Systemic vasculitis with localized fibrinoid necrosis and infiltration of monocytes, lymphocytes, and plasma cells into vessel walls has been described in cardiac, pulmonary, hepatic, renal, and adrenal gland tissue as well [122].
MERS-CoV, the cause of the Middle East respiratory syndrome, is another member of the beta coronavirus genus, which includes SARS-CoV-1 and SARS-CoV-2 and was originally identified in Jordan in April 2012. Histopathological data for MERS-CoV infection are limited, as autopsies generally have not been performed either for religious or cultural reasons [123]. Similar to the other betacoronaviruses, the pathologic changes in the lungs of MERS-CoV patients are characterized by DAD with hyaline membrane formation indistinguishable from findings detected in severe pneumonia caused by other viral agents [124]. In cardiac tissue, diffuse myocyte hypertrophy has been observed [125]. Renal findings demonstrate signs of AKI, and glomeruli with ischemic and sclerotic changes [125,126]. Hepatic tissue congestion and steatosis has also been noted [125,126]. In contrast to the other betacoronaviruses, the functional receptor for MERS-CoV is dipeptidyl peptidase 4 (DPP4), which is widely distributed but predominantly expressed in the lower respiratory tract and kidneys [125,127]. This may partially explain the lack of findings in other organs affected by SARS-CoV-1 and SARS-CoV-2.
A review of autopsy findings in decedents infected with avian influenza A subtype H5N1 revealed several similarities to COVID-19. Pulmonary findings in these patients demonstrated that the primary target of viral infection was type II pneumocytes, resulting in extensive pneumocyte destruction. Autopsy also revealed DAD with interstitial lymphoplasmacytic infiltration and fibrosis following H5N1 infection [128]. DAD was in the acute exudative phase for patients dying in the first 2 weeks and the organizing phase for patients dying in the third week or later, while fibrosis appeared hyaline and paucicellular [128]. The H5N1 autopsied spleens showed atrophic white pulp and congested red pulp, livers demonstrated macrovesicular steatosis, and renal findings included acute tubular necrosis in nearly half of cases [128]. No significant pathology was noted in other organs. These findings were similar to the autopsy findings in COVID-19 decedents.
Patients who died secondary to infection with influenza A virus subtype H1N1—the strain associated with the 1918 and 2009 influenza pandemics—provide another source of comparison. In 411 autopsies from the 1918 pandemic, splenomegaly was noted in 37%, while cardiac hypertrophy was observed in 16.3% of decedents [122]. Peripheral lung pathology in both patients with COVID-19 and H1N1 shares the common feature of DAD and infiltrating perivascular lymphocytes. Similarly, H1N1 autopsies have demonstrated microthrombi in small pulmonary arteries and in alveolar capillaries. However, alveolar capillary microthrombi have been reported as significantly more prevalent in patients with COVID-19 than with influenza A [57]. In comparison, macroscopic thromboemboli were not observed at autopsy by Burkhard-Koren et al. in their review of 411 autopsies from 1918 and 12 autopsies from the 2009 pandemic. Macrothrombosis has been a frequently reported finding in COVID-19 autopsies.
As a last comparison, autopsy reports of patients infected by filoviruses were analyzed—this family of viruses were the cause of the 2013 West African Ebola virus epidemic. Autopsy reports showed macrophage-rich lymphoid tissues, the liver, and the adrenal glands were major targets for these viruses [129]. Although known to be a hemorrhagic disease process, there were no vascular lesions identified with decreased production of coagulation factors as the major cause of bleeding [129]. Lymphoid depletion of the spleen, thymus, and lymph node was characteristic of the disease as they were the primary sites of infection; however, there was little cellular inflammatory response noted in these diseased tissues [129]. The mechanism of this lymphocytic cell-death was theorized to be activated through TNF-related apoptosis-induced ligand (TRAIL) and Fas death receptor pathways, but was not confirmed [130]. A key pathogenesis of the late stage of this disease involves the adrenal cortex. Disruption of the adrenal cortex homeostatic function in blood pressure, causing hypovolemia and hypotension, was seen in almost every death caused by Ebola [129].
4.1. Unique COVID-19 Features
Pathological mechanisms leading to death in COVID-19 remain to be mainly hypothetical. These mechanisms include disordered immune response resulting in a hyperinflammatory state, [131] cytokine storm and activation of neutrophils and the release of neutrophil extracellular traps, [132] and virus-mediated injury of endothelial cells through angiotensin converting enzyme 2 (ACE2) receptors, [133] which explains elevated levels of von Willebrand factor (vWF) and Factor VIII seen in COVID-19 patients [134]. Hypoxia-related activation of coagulation factors like tissue factor may be another possible mechanism in triggering the disordered coagulation cascade, as well as immobility and ICU-related risk factors [132].
The pulmonary pathology of severe COVID-19 manifests as a severe acute respiratory distress syndrome (ARDS) with thrombotic microangiopathy. Our review of autopsy data suggests that these findings are associated with underlying DAD. COVID-19-induced DAD is characterized by damage to alveolar capillary endothelium and type II pneumocytes leading to alveolar septal edema and the formation of hyaline membranes, accumulation of numerous inflammatory cells, and precipitation of fibrin inside alveolar capillaries with a relatively mild accumulation of lymphocytes and macrophages within alveoli [135].
As previously described, similar features have been identified in DAD of other etiologies, including influenza A, MERS-CoV, and SARS-CoV-1. COVID-19 appears to lack pathognomonic characteristics in terms of morphology and extent of alveolar damage. There does not appear to be distinctive morphological features with which to differentiate COVID-19-related DAD from DAD due to other causes [52]. In fact, COVID-19 pulmonary disease is remarkably similar to the DAD described with SARS-CoV-1 infection, which has been reported as nearly indistinguishable from DAD caused by trauma, aspiration, oxygen toxicity, or infectious microorganisms [119].
While not universally present, COVID-19 pulmonary pathology is commonly accompanied by thrombosis [98]. Microthrombi in alveolar capillaries and small pulmonary arteries are likely related to the frequent development of a SARS-CoV-2-induced diffuse hypercoagulable state, which occasionally features macrothrombosis characterized by deep vein thromboses and large pulmonary thromboemboli [58,135]. Fox et al. hypothesize that a thrombotic microangiopathy, primarily involving the lungs, is an important mechanism underlying fatal COVID-19 disease [98].
However, as described previously, this is not necessarily a feature unique to COVID-19, as numerous viral infections have been associated with thrombotic coagulation disorders. Viral infections impact the coagulation cascade by directly interfering with various coagulation factors, contributing to either prothrombotic or hemorrhagic states [136]. Specifically, influenza A virus, SARS-CoV-1, and avian influenza A subtype H5N1 have been associated with pulmonary microthrombi and fibrin deposition [136,137,138,139]. In SARS-CoV-1 infection, the proposed thrombotic mechanism was an increased production of a novel pro-coagulant observed in infected cells due to increased hfg12 gene transcription induced by a viral nucleocapsid protein [97,140]. It is unclear why some viruses have a strong influence on coagulation and associated thrombotic complications while others do not. Inherited host factors, as well the mechanism by which a virus exerts its effect—direct target cell infection, virus-specific antibodies, or inflammatory mediators—likely plays a significant role [136]. Further, pulmonary microthrombi are not specific to viral infections but are instead features of acute lung injury and hypoxic respiratory failure, seen in bacterial infection, sepsis, trauma, aspiration, and toxic inhalation [122].
Myocardial inflammation is a common process that occurs with viral infections. Patients with viral infections can exhibit eosinophilic, lymphocytic, or granulomatous inflammation of the myocardial tissue which can lead to dilated cardiomyopathy [141]. Interestingly, one study characterized gross heart findings from a COVID-19-infected patient, showing right and left ventricular dilation with cardiomegaly. Microscopy of this myocardial tissue showed individual cell myocyte necrosis; however, there was no significant lymphocytic inflammatory infiltrate [98]. This is normally present in viral myocarditis, suggesting that COVID-19 attacks the heart in a novel process. One mechanism proposed that the pericytes could be infected with COVID-19, thus causing microvascular impairment, which can lead to cell necrosis [142].
Endothelial cell injury is a hallmark of vascular changes found in SARS-CoV-2 infections via endotheliitis in numerous organs as a direct result of viral infection mediated by the ACE2 receptor and subsequent inflammatory immune response [83]. This COVID-19-endotheliitis could explain the diffuse hypercoagulability and the clinical sequelae in patients with COVID-19, such as widespread vascular thrombosis with microangiopathy. Moreover, this endothelial damage likely predisposes patients with pre-existing endothelial dysfunction from comorbidities, such as old age, obesity, hypertension, and diabetes mellitus, to severe COVID-19 [122]. Additionally, Ackermann et al. reported a specific microangiopathy in the lungs of COVID-19 patients believed to be associated with SARS-CoV-2′s endothelial injury. They described new vessel growth primarily through a mechanism of intussusceptive angiogenesis that was significantly greater than that seen in patients with influenza A [57]. However, the clinical significance of this angiogenesis during COVID-19 remains incompletely understood. Of note, patients with pre-existing immune inflammatory disease being treated with anti-cytokine pharmacotherapy reveal incidence of hospitalization similar to the general population [143], therefore suggesting that the use of baseline biologics protects against worse COVID-19 outcomes.
4.2. COVID-19 Cardiovascular and CNS Theories
Patients with cardiovascular disease are at higher risk to develop severe complications of COVID-19 infection. While severe COVID-19 infection consistently damages the lungs, cases of myocardial injury have been reported. The proposed mechanisms of myocardial injury are direct damage to the cardiomyocytes, systemic inflammation, myocardial interstitial fibrosis, immune mediated response, coronary plaque destabilization, and hypoxia [94]. Specifically, myocarditis has been a topic of discussion in the media during the COVID-19 pandemic. The true prevalence of myocarditis among patients with COVID-19 is difficult to establish, as many early reports lacked specific diagnostic modalities to assess myocarditis [144]. Additionally, circulating biomarkers that correlate with myocardial injury may be a result of myocardial damage secondary to multiorgan failure, hypoxia, or hypoxemia [145] while studies in the early months of the pandemic suggested that myocardial injury may occur in 15–28% of severe COVID-19 cases [144]. More recent reviews purport that the true prevalence of myocarditis is likely much lower [146]. A review of 277 autopsied hearts across 22 separate publications of COVID-19 patients found the prevalence of myocarditis to be under 2%, while separate cardiac pathology like thrombi inflammation were reported in 48% of cases [146].
Numerous respiratory viruses have demonstrated the ability to penetrate the CNS [147], and coronaviruses in particular have shown neuroinvasive properties in various hosts, including humans, rats, pigs, rodents, and fowls [148]. However, based upon knowledge from other coronaviruses that have caused severe infection, like severe acute respiratory syndrome and Middle East respiratory syndrome [149], cases of severe neurologic disease caused by SARS-CoV-2 are likely rare [150]. A wide array of neurological manifestations of SARS-CoV-2 have been observed, with anosmia and ageusia being particularly common [150]. Of particular curiosity is SARS-CoV-2-associated encephalitis, which is an inflammatory condition of the brain that has been described as a severe neurological complication of COVID-19. While encephalitis related to COVID-19 infection has not been fully characterized and systematic reviews are limited, SARS-CoV-2 has been detected in the CSF of some patients [151]. One systematic review of SARS-CoV-2-associated encephalitis, including 23 studies reporting findings of 138 COVID-19 patients with encephalitis, revealed that the incidence of hospitalized COVID-19 patients with encephalitis was low at 0.215%; however, the mortality rate of these patients was high at 13.4%, and severely ill COVID-19 patients were more likely to suffer from encephalitis as a complication [151]. The pathophysiology of SARS-CoV-2-associated encephalitis has been speculated to be a result direct invasion of the nervous system, molecular mimicry, or systemic inflammation causing injury and edema, and subsequent alterations in consciousness [151]. If SARS-CoV-2-associated encephalitis does indeed exist, diagnosis may prove difficult as SARS-CoV-2 dissemination is transient and CSF titer may be extremely low [152].
4.3. Significance to the COVID-19 Pandemic
These findings help elucidate the broad effects of how COVID-19 infection can damage the human body. To effectively combat the spread of this pandemic researchers, clinicians, and all healthcare professionals can benefit from this information by understanding the terminal points of damage and can develop therapies to help reduce or eliminate these effects. These results are not only confined to this viral variant. There has already been an emergence of the Omicron variant and preliminary results have shown this virus to have enhanced transmissibility. Omicron has many spike mutations [153] and has been shown to be resistant to neutralization by serum from recovered COVID-19 patients and individuals who have been vaccinated [154]. Therefore, understanding the pathological targets of COVID-19 will help not only inform current and developing medical therapies, but also chart a trajectory for the course of this pandemic.
5. Limitations
A major limitation of this study is the heterogeneity of the autopsies analyzed in this study. The authors of these reports had goals that ranged from solely microscopic analysis to full body autopsy analysis. This represents a challenge as the percentage of reported findings is dependent on the original article aiming to look for these findings. This indicates that the percentages found in this analysis is most likely underrepresented. Another limitation of this study is that pneumonia or other lung pathologies were not the only cause of death for some COVID-19 patients. Our analysis mostly focused on comparisons with pneumonia-related autopsy reports; therefore, we cannot determine if our sample is representative of all COVID-19 mortality.
6. Conclusions
Through review of the data, the most common pulmonary findings were DAD with the associated findings of alveolar edema and hyaline membrane disease. As noted earlier, these findings were to be expected as these are the most common initial and end-stage symptoms of COVID-19 infection. However, the most notable extrapulmonary findings included effects on cardiovascular, renal, splenic, and liver organ systems. This is significant as this indicates broad viral tropism in the human body. This diversity of targets exhibited by COVID-19 infection will need to be explored further in comprehensive and longitudinal studies, as this will help characterize short-term and long-term sequela of COVID-19 infection. This will help inform and direct future healthcare professionals in treatment of intra- and post-COVID-19 infected patients [155].
Author Contributions
K.C., S.H., R.S., A.F., G.P. and F.L. Conceptualization; K.C., S.H., R.S., A.F., G.P. and F.L. Data curation; F.L. Project administration; K.C., S.H., R.S., A.F. and F.L. Writing—original draft; K.C., S.H., R.S., A.F. and F.L. Writing—review and editing. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by The Conrad and Caroline Jobst Foundation.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Czeisler, M.É.; Marynak, K.; Clarke, K.E.; Salah, Z.; Shakya, I.; Thierry, J.M.; Ali, N.; McMillan, H.; Wiley, J.F.; Weaver, M.D.; et al. Delay or avoidance of medical care because of COVID-19–related concerns—United States, June 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 1250. [Google Scholar]
- Coppo, A.; Bellani, G.; Winterton, D.; Di Pierro, M.; Soria, A.; Faverio, P.; Cairo, M.; Mori, S.; Messinesi, G.; Contro, E.; et al. Feasibility and physiological effects of prone positioning in non-intubated patients with acute respiratory failure due to COVID-19 (PRON-COVID): A prospective cohort study. Lancet Respir. Med. 2020, 8, 765–774. [Google Scholar] [CrossRef]
- Schaller, T.; Hirschbühl, K.; Burkhardt, K.; Braun, G.; Trepel, M.; Märkl, B.; Claus, R. Postmortem Examination of Patients with COVID-19. JAMA 2020, 323, 2518–2520. [Google Scholar] [CrossRef] [PubMed]
- Barton, L.M.; Duval, E.J.; Stroberg, E.; Ghosh, S.; Mukhopadhyay, S. COVID-19 Autopsies, Oklahoma, USA. Am. J. Clin. Pathol. 2020, 153, 725–733. [Google Scholar] [CrossRef] [Green Version]
- Keresztesi, A.A.; Perde, F.; Ghita-Nanu, A.; Radu, C.C.; Negrea, M.; Keresztesi, G. Post-Mortem Diagnosis and Autopsy Findings in SARS-CoV-2 Infection: Forensic Case Series. Diagnostics 2020, 10, 1070. [Google Scholar] [CrossRef]
- Zhao, C.L.; Rapkiewicz, A.; Maghsoodi-Deerwester, M.; Gupta, M.; Cao, W.; Palaia, T.; Zhou, J.; Ram, B.; Vo, D.; Rafiee, B.; et al. Pathological findings in the postmortem liver of patients with coronavirus disease 2019 (COVID-19). Hum. Pathol. 2021, 109, 59–68. [Google Scholar] [CrossRef]
- Schwensen, H.F.; Borreschmidt, L.K.; Storgaard, M.; Redsted, S.; Christensen, S.; Madsen, L.B. Fatal pulmonary fibrosis: A post-COVID-19 autopsy case. J. Clin. Pathol. 2021, 74, 400–402. [Google Scholar] [CrossRef]
- Chmielik, E.; Jazowiecka-Rakus, J.; Dyduch, G.; Nasierowska-Guttmejer, A.; Michalowski, L.; Sochanik, A.; Ulatowska-Bialas, M. COVID-19 Autopsies: A Case Series from Poland. Pathobiology 2020, 88, 78–87. [Google Scholar] [CrossRef]
- Bussani, R.; Schneider, E.; Zentilin, L.; Collesi, C.; Ali, H.; Braga, L.; Volpe, M.C.; Colliva, A.; Zanconati, F.; Berlot, G.; et al. Persistence of viral RNA, pneumocyte syncytia and thrombosis are hallmarks of advanced COVID-19 pathology. EBioMedicine 2020, 61, 103104. [Google Scholar] [CrossRef]
- Seetulsingh, P.; Kannangara, C.I.; Richman, P. Undetectable SARS-CoV-2 in a nasopharyngeal swab but persistent viral RNA from deep lung swabs: Findings from an autopsy. BMJ Case Rep. CP 2020, 13, e237446. [Google Scholar] [CrossRef]
- Nienhold, R.; Ciani, Y.; Koelzer, V.H.; Tzankov, A.; Haslbauer, J.D.; Menter, T.; Schwab, N.; Henkel, M.; Frank, A.; Zsikla, V.; et al. Two distinct immunopathological profiles in autopsy lungs of COVID-19. Nat. Commun. 2020, 11, 5086. [Google Scholar] [CrossRef] [PubMed]
- Schurink, B.; Roos, E.; Radonic, T.; Barbe, E.; Bouman, C.S.C.; de Boer, H.H.; de Bree, G.J.; Bulle, E.B.; Aronica, E.M.; Florquin, S.; et al. Viral presence and immunopathology in patients with lethal COVID-19: A prospective autopsy cohort study. Lancet Microbe 2020, 1, e290–e299. [Google Scholar] [CrossRef]
- Jacobs, W.; Lammens, M.; Kerckhofs, A.; Voets, E.; Van San, E.; Van Coillie, S.; Peleman, C.; Mergeay, M.; Sirimsi, S.; Matheeussen, V.; et al. Fatal lymphocytic cardiac damage in coronavirus disease 2019 (COVID-19): Autopsy reveals a ferroptosis signature. ESC Heart Fail. 2020, 7, 3772–3781. [Google Scholar] [CrossRef] [PubMed]
- Elsoukkary, S.S.; Mostyka, M.; Dillard, A.; Berman, D.R.; Ma, L.X.; Chadburn, A.; Yantiss, R.K.; Jessurun, J.; Seshan, S.V.; Borczuk, A.C.; et al. Autopsy Findings in 32 Patients with COVID-19: A Single-Institution Experience. Pathobiology 2020, 88, 56–68. [Google Scholar] [CrossRef] [PubMed]
- Damiani, S.; Fiorentino, M.; De Palma, A.; Foschini, M.P.; Lazzarotto, T.; Gabrielli, L.; Viale, P.L.; Attard, L.; Riefolo, M.; D’Errico, A. Pathological post-mortem findings in lungs infected with SARS-CoV-2. J. Pathol. 2021, 253, 31–40. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Wu, J.; Wang, S.; Li, X.; Zhou, J.; Huang, B.; Luo, D.; Cao, Q.; Chen, Y.; Chen, S.; et al. Progression to fibrosing diffuse alveolar damage in a series of 30 minimally invasive autopsies with COVID-19 pneumonia in Wuhan, China. Histopathology 2021, 78, 542–555. [Google Scholar] [CrossRef]
- Veras, F.P.; Pontelli, M.C.; Silva, C.M.; Toller-Kawahisa, J.E.; de Lima, M.; Nascimento, D.C.; Schneider, A.H.; Caetité, D.; Tavares, L.A.; Paiva, I.M.; et al. SARS-CoV-2–triggered neutrophil extracellular traps mediate COVID-19 pathology. J. Exp. Med. 2020, 217, e20201129. [Google Scholar] [CrossRef] [PubMed]
- Valdivia-Mazeyra, M.F.; Salas, C.; Nieves-Alonso, J.M.; Martín-Fragueiro, L.; Bárcena, C.; Muñoz-Hernández, P.; Villar-Zarra, K.; Martín-López, J.; Ramasco-Rueda, F.; Fraga, J.; et al. Increased number of pulmonary megakaryocytes in COVID-19 patients with diffuse alveolar damage: An autopsy study with clinical correlation and review of the literature. Virchows Arch. 2021, 478, 487–496. [Google Scholar] [CrossRef] [PubMed]
- Falasca, L.; Nardacci, R.; Colombo, D.; Lalle, E.; Di Caro, A.; Nicastri, E.; Antinori, A.; Petrosillo, N.; Marchioni, L.; Biava, G.; et al. Postmortem Findings in Italian Patients with COVID-19: A Descriptive Full Autopsy Study of Cases with and without Comorbidities. J. Infect. Dis. 2020, 222, 1807–1815. [Google Scholar] [CrossRef] [PubMed]
- Borczuk, A.C.; Salvatore, S.P.; Seshan, S.V.; Patel, S.S.; Bussel, J.B.; Mostyka, M.; Elsoukkary, S.; He, B.; DEL Vecchio, C.; Fortarezza, F.; et al. COVID-19 pulmonary pathology: A multi-institutional autopsy cohort from Italy and New York City. Mod. Pathol. 2020, 33, 2156–2168. [Google Scholar] [CrossRef]
- De Michele, S.; Sun, Y.; Yilmaz, M.M.; Katsyv, I.; Salvatore, M.; Dzierba, A.L.; Marboe, C.C.; Brodie, D.; Patel, N.M.; Garcia, C.K.; et al. Forty postmortem examinations in COVID-19 patients. Am. J. Clin. Pathol. 2020, 154, 748–760. [Google Scholar] [CrossRef]
- Kommoss, F.K.; Schwab, C.; Tavernar, L.; Schreck, J.; Wagner, W.L.; Merle, U.; Jonigk, D.; Schirmacher, P.; Longerich, T. The Pathology of Severe COVID-19-Related Lung Damage. Dtsch. Ärzteblatt Int. 2020, 117, 500–506. [Google Scholar] [CrossRef] [PubMed]
- Roncati, L.; Ligabue, G.; Nasillo, V.; Lusenti, B.; Gennari, W.; Fabbiani, L.; Malagoli, C.; Gallo, G.; Giovanella, S.; Lupi, M.; et al. A proof of evidence supporting abnormal immunothrombosis in severe COVID-19: Naked megakaryocyte nuclei increase in the bone marrow and lungs of critically ill patients. Platelets 2020, 31, 1085–1089. [Google Scholar] [CrossRef] [PubMed]
- Wagner, W.L.; Hellbach, K.; Fiedler, M.O.; Salg, G.A.; Wehrse, E.; Ziener, C.H.; Merle, U.; Eckert, C.; Weber, T.F.; Stiller, W.; et al. Microvascular changes in COVID-19. Radiologe 2020, 60, 934–942. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.X.; Shao, C.; Huang, X.J.; Sun, L.; Meng, L.J.; Liu, H.; Zhang, S.J.; Li, H.J.; Lv, F.D. Histopathological features of multiorgan percutaneous tissue core biopsy in patients with COVID-19. J. Clin. Pathol. 2020, 74, 522–527. [Google Scholar] [CrossRef] [PubMed]
- Hanley, B.; Naresh, K.; Roufosse, C.; Nicholson, A.G.; Weir, J.; Cooke, G.S.; Thursz, M.; Manousou, P.; Corbett, R.; Goldin, R.; et al. Histopathological findings and viral tropism in UK patients with severe fatal COVID-19: A post-mortem study. Lancet Microbe 2020, 1, e245–e253. [Google Scholar] [CrossRef]
- Eckermann, M.; Frohn, J.; Reichardt, M.; Osterhoff, M.; Sprung, M.; Westermeier, F.; Tzankov, A.; Werlein, C.; Kühnel, M.; Jonigk, D.; et al. 3D virtual pathohistology of lung tissue from COVID-19 patients based on phase contrast X-ray tomography. eLife 2020, 9, e60408. [Google Scholar] [CrossRef]
- Skok, K.; Stelzl, E.; Trauner, M.; Kessler, H.H.; Lax, S.F. Post-mortem viral dynamics and tropism in COVID-19 patients in correlation with organ damage. Virchows Arch. 2021, 478, 343–353. [Google Scholar] [CrossRef]
- Remmelink, M.; De Mendonça, R.; D’Haene, N.; De Clercq, S.; Verocq, C.; Lebrun, L.; Lavis, P.; Racu, M.-L.; Trépant, A.-L.; Maris, C.; et al. Unspecific post-mortem findings despite multiorgan viral spread in COVID-19 patients. Crit. Care 2020, 24, 495. [Google Scholar] [CrossRef]
- Cipolloni, L.; Sessa, F.; Bertozzi, G.; Baldari, B.; Cantatore, S.; Testi, R.; D’Errico, S.; Di Mizio, G.; Asmundo, A.; Castorina, S.; et al. Preliminary Post-Mortem COVID-19 Evidence of Endothelial Injury and Factor VIII Hyperexpression. Diagnostics 2020, 10, 575. [Google Scholar] [CrossRef]
- Grosse, C.; Grosse, A.; Salzer, H.J.; Dünser, M.W.; Motz, R.; Langer, R. Analysis of cardiopulmonary findings in COVID-19 fatalities: High incidence of pulmonary artery thrombi and acute suppurative bronchopneumonia. Cardiovasc. Pathol. 2020, 49, 107263. [Google Scholar] [CrossRef] [PubMed]
- Beigee, F.S.; Toutkaboni, M.P.; Khalili, N.; Nadji, S.A.; Dorudinia, A.; Rezaei, M.; Askari, E.; Farzanegan, B.; Marjani, M.; Rafiezadeh, A. Diffuse alveolar damage and thrombotic microangiopathy are the main histopathological findings in lung tissue biopsy samples of COVID-19 patients. Pathol. Res. Pract. 2020, 216, 153228. [Google Scholar]
- Hellman, U.; Karlsson, M.G.; Engström-Laurent, A.; Cajander, S.; Dorofte, L.; Ahlm, C.; Laurent, C.; Blomberg, A. Presence of hyaluronan in lung alveoli in severe COVID-19: An opening for new treatment options? J. Biol. Chem. 2020, 295, 15418–15422. [Google Scholar] [CrossRef] [PubMed]
- Ducloyer, M.; Gaborit, B.; Toquet, C.; Castain, L.; Bal, A.; Arrigoni, P.P.; LeComte, R.; Clement, R.; Sagan, C. Complete post-mortem data in a fatal case of COVID-19: Clinical, radiological and pathological correlations. Int. J. Leg. Med. 2020, 134, 2209–2214. [Google Scholar] [CrossRef]
- Rapkiewicz, A.V.; Mai, X.; Carsons, S.E.; Pittaluga, S.; Kleiner, D.E.; Berger, J.S.; Thomas, S.; Adler, N.; Charytan, D.; Gasmi, B.; et al. Megakaryocytes and platelet-fibrin thrombi characterize multi-organ thrombosis at autopsy in COVID-19: A case series. EClinicalMedicine 2020, 24, 100434. [Google Scholar] [CrossRef]
- Cirstea, A.E.; Buzulică, R.L.; Pirici, D.; Ceauşu, M.C.; Iman, R.V.; Gheorghe, O.M.; Neamţu, S.D.; Stanca, L.; Ene, R.; Kumar-Singh, S.; et al. Histopathological findings in the advanced natural evolution of the SARS-CoV-2 infection. Rom. J. Morphol. Embryol. 2020, 61, 209–218. [Google Scholar] [CrossRef]
- Leth, P.M.; Rasmussen, C.H.; Pagh, M. Findings in post-mortem CT and autopsy in a 53-year-old-man with COVID-19. Ugeskr. Laeger 2020, 182. [Google Scholar]
- Prilutskiy, A.; Kritselis, M.; Shevtsov, A.; Yambayev, I.; Vadlamudi, C.; Zhao, Q.; Kataria, Y.; Sarosiek, S.R.; Lerner, A.; Sloan, J.M.; et al. SARS-CoV-2 Infection–Associated Hemophagocytic Lymphohistiocytosis. Am. J. Clin. Pathol. 2020, 154, 466–474. [Google Scholar] [CrossRef]
- Golmai, P.; Larsen, C.P.; DeVita, M.V.; Wahl, S.J.; Weins, A.; Rennke, H.G.; Bijol, V.; Rosenstock, J.L. Histopathologic and Ultrastructural Findings in Postmortem Kidney Biopsy Material in 12 Patients with AKI and COVID-19. J. Am. Soc. Nephrol. 2020, 31, 1944–1947. [Google Scholar] [CrossRef]
- Flikweert, A.W.; Grootenboers, M.J.; Yick, D.C.; du Mée, A.W.; van der Meer, N.J.; Rettig, T.C.; Kant, M.K. Late histopathologic characteristics of critically ill COVID-19 patients: Different phenotypes without evidence of invasive aspergillosis, a case series. J. Crit. Care 2020, 59, 149–155. [Google Scholar] [CrossRef]
- Aiolfi, A.; Bruni, B.; Biraghi, T.; Montisci, A.; Miceli, A.; Baronio, B.; Khor, D.; Cirri, S.; Donatelli, F.; Clemente, C.; et al. Late histological findings in symptomatic COVID-19 patients: A case report. Medicine 2020, 99, e21046. [Google Scholar] [CrossRef] [PubMed]
- Conde, P.N.; Monraval, P.A.; Medina, C.M.; Sánchez, A.J.; Teruel, J.C.A.; Marco, J.F.; Santos, V.P.; Aranda, E.M. Autopsy findings from the first known death from Severe Acute Respiratory Syndrome SARS-CoV-2 in Spain. Rev. Española Patol. 2020, 53, 188–192. [Google Scholar] [CrossRef] [PubMed]
- The COVID-19 Autopsy. The first COVID-19 autopsy in Spain performed during the early stages of the pandemic. Rev. Española Patol. 2020, 53, 182–187. [Google Scholar] [CrossRef] [PubMed]
- Stone, J.R.; Tran, K.M.; Conklin, J.; Mino-Kenudson, M. Case 23-2020: A 76-year-old woman who died from COVID-19. N. Engl. J. Med. 2020, 383, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Sauter, J.L.; Baine, M.K.; Butnor, K.J.; Buonocore, D.J.; Chang, J.C.; Jungbluth, A.A.; Szabolcs, M.J.; Morjaria, S.; Mount, S.L.; Rekhtman, N.; et al. Insights into pathogenesis of fatal COVID-19 pneumonia from histopathology with immunohistochemical and viral RNA studies. Histopathology 2020, 77, 915–925. [Google Scholar] [CrossRef]
- Tombolini, A.; Scendoni, R. SARS-CoV-2-related deaths in routine forensic autopsy practice: Histopathological patterns. Int. J. Leg. Med. 2020, 134, 2205–2208. [Google Scholar] [CrossRef]
- Bösmüller, H.; Traxler, S.; Bitzer, M.; Häberle, H.; Raiser, W.; Nann, D.; Frauenfeld, L.; Vogelsberg, A.; Klingel, K.; Fend, F. The evolution of pulmonary pathology in fatal COVID-19 disease: An autopsy study with clinical correlation. Virchows Arch. 2020, 477, 349–357. [Google Scholar] [CrossRef]
- Fang, Y.; Liu, H.; Huang, H.; Li, H.; Saqi, A.; Qiang, L.; Que, J. Distinct stem/progenitor cells proliferate to regenerate the trachea, intrapulmonary airways and alveoli in COVID-19 patients. Cell Res. 2020, 30, 705–707. [Google Scholar] [CrossRef]
- Wang, C.; Xie, J.; Zhao, L.; Fei, X.; Zhang, H.; Tan, Y.; Nie, X.; Zhou, L.; Liu, Z.; Ren, Y.; et al. Alveolar macrophage dysfunction and cytokine storm in the pathogenesis of two severe COVID-19 patients. EBioMedicine 2020, 57, 102833. [Google Scholar] [CrossRef]
- Schaefer, I.M.; Padera, R.F.; Solomon, I.H.; Kanjilal, S.; Hammer, M.M.; Hornick, J.L.; Sholl, L.M. In situ detection of SARS-CoV-2 in lungs and airways of patients with COVID-19. Mod. Pathol. 2020, 33, 2104–2114. [Google Scholar] [CrossRef]
- Suess, C.; Hausmann, R. Gross and histopathological pulmonary findings in a COVID-19 associated death during self-isolation. Int. J. Leg. Med. 2020, 134, 1285–1290. [Google Scholar] [CrossRef] [PubMed]
- Konopka, K.E.; Nguyen, T.; Jentzen, J.M.; Rayes, O.; Schmidt, C.J.; Wilson, A.M.; Farver, C.F.; Myers, J.L. Diffuse alveolar damage (DAD) resulting from coronavirus disease 2019 Infection is Morphologically Indistinguishable from Other Causes of DAD. Histopathology 2020, 77, 570–578. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.H.; Li, X.; Huang, B.; Su, H.; Li, Y.; Luo, D.J.; Chen, S.; Ma, L.; Wang, S.H.; Nie, X.; et al. Pathological changes of fatal coronavirus disease 2019 (COVID-19) in the lungs: Report of 10 cases by postmortem needle autopsy. Zhonghua Bing Li Xue Za Zhi 2020, 49, 568–575. [Google Scholar] [PubMed]
- Aguiar, D.; Lobrinus, J.A.; Schibler, M.; Fracasso, T.; Lardi, C. Inside the lungs of COVID-19 disease. Int. J. Leg. Med. 2020, 134, 1271–1274. [Google Scholar] [CrossRef] [PubMed]
- Sekulic, M.; Harper, H.; Nezami, B.G.; Shen, D.L.; Sekulic, S.P.; Koeth, A.T.; Harding, C.V.; Gilmore, H.; Sadri, N. Molecular detection of SARS-CoV-2 infection in FFPE samples and histopathologic findings in fatal SARS-CoV-2 cases. Am. J. Clin. Pathol. 2020, 154, 190–200. [Google Scholar] [CrossRef]
- Duarte-Neto, A.N.; Monteiro, R.; Da Silva, L.F.F.; Malheiros, D.M.A.C.; De Oliveira, E.P.; Theodoro-Filho, J.; Pinho, J.R.R.; Gomes-Gouvêa, M.S.; Salles, A.P.M.; De Oliveira, I.R.S.; et al. Pulmonary and systemic involvement in COVID-19 patients assessed with ultrasound-guided minimally invasive autopsy. Histopathology 2020, 77, 186–197. [Google Scholar] [CrossRef]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in COVID-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef]
- Buja, L.M.; Wolf, D.A.; Zhao, B.; Akkanti, B.; McDonald, M.; Lelenwa, L.; Reilly, N.; Ottaviani, G.; Elghetany, M.T.; Trujillo, D.O.; et al. The emerging spectrum of cardiopulmonary pathology of the coronavirus disease 2019 (COVID-19): Report of 3 autopsies from Houston, Texas, and review of autopsy findings from other United States cities. Cardiovasc. Pathol. 2020, 48, 107233. [Google Scholar] [CrossRef]
- Lax, S.F.; Skok, K.; Zechner, P.; Kessler, H.H.; Kaufmann, N.; Koelblinger, C.; Vander, K.; Bargfrieder, U.; Trauner, M. Pulmonary arterial thrombosis in COVID-19 with fatal outcome: Results from a prospective, single-center, clinicopathologic case series. Ann. Intern. Med. 2020, 173, 350–361. [Google Scholar] [CrossRef]
- Craver, R.; Huber, S.; Sandomirsky, M.; McKenna, D.; Schieffelin, J.; Finger, L. Fatal eosinophilic myocarditis in a healthy 17-year-old male with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2c). Fetal Pediatr. Pathol. 2020, 39, 263–268. [Google Scholar] [CrossRef]
- Farkash, E.A.; Wilson, A.M.; Jentzen, J.M. Ultrastructural Evidence for Direct Renal Infection with SARS-CoV-2. J. Am. Soc. Nephrol. 2020, 31, 1683–1687. [Google Scholar] [CrossRef] [PubMed]
- Menter, T.; Haslbauer, J.D.; Nienhold, R.; Savic, S.; Hopfer, H.; Deigendesch, N.; Frank, S.; Turek, D.; Willi, N.; Pargger, H.; et al. Post-mortem examination of COVID-19 patients reveals diffuse alveolar damage with severe capillary congestion and variegated findings of lungs and other organs suggesting vascular dysfunction. Histopathology 2020, 77, 198–209. [Google Scholar] [CrossRef]
- Konopka, K.E.; Wilson, A.; Myers, J.L. Postmortem Lung Findings in a Patient with Asthma and Coronavirus Disease 2019. Chest 2020, 158, e99–e101. [Google Scholar] [CrossRef] [PubMed]
- Tian, S.; Xiong, Y.; Liu, H.; Niu, L.; Guo, J.; Liao, M.; Xiao, S.Y. Pathological study of the 2019 novel coronavirus disease (COVID-19) through postmortem core biopsies. Mod. Pathol. 2020, 33, 1007–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stoyanov, G.S.; Petkova, L.; Dzhenkov, D.L.; Sapundzhiev, N.R.; Todorov, I. Gross and Histopathology of COVID-19 with First Histology Report of Olfactory Bulb Changes. Cureus 2020, 12, e11912. [Google Scholar] [CrossRef] [PubMed]
- Fernandes Matuck, B.; Dolhnikoff, M.; Maia, G.V.; Isaac Sendyk, D.; Zarpellon, A.; Costa Gomes, S.; Duarte-Neto, A.N.; Rebello Pinho, J.R.; Gomes-Gouvêa, M.S.; Sousa, S.C.; et al. Periodontal tissues are targets for SARS-Cov-2: A post-mortem study. J. Oral Microbiol. 2020, 13, 1848135. [Google Scholar] [CrossRef]
- Bruce-Brand, C.; Allwood, B.W.; Koegelenberg, C.F.N.; Lalla, U.; Louw, E.; Diacon, A.H.; Schubert, P.T. Postmortem lung biopsies from four patients with COVID-19 at a tertiary hospital in Cape Town, South Africa. S. Afr. Med J. 2020, 110, 1195–1200. [Google Scholar] [CrossRef]
- Edler, C.; Schröder, A.S.; Aepfelbacher, M.; Fitzek, A.; Heinemann, A.; Heinrich, F.; Klein, A.; Langenwalder, F.; Lütgehetmann, M.; Meißner, K.; et al. Dying with SARS-CoV-2 infection—An autopsy study of the first consecutive 80 cases in Hamburg, Germany. Int. J. Leg. Med. 2020, 134, 1275–1284. [Google Scholar] [CrossRef]
- Su, H.; Yang, M.; Wan, C.; Yi, L.-X.; Tang, F.; Zhu, H.-Y.; Yi, F.; Yang, H.-C.; Fogo, A.B.; Nie, X.; et al. Renal histopathological analysis of 26 postmortem findings of patients with COVID-19 in China. Kidney Int. 2020, 98, 219–227. [Google Scholar] [CrossRef]
- Adachi, T.; Chong, J.-M.; Nakajima, N.; Sano, M.; Yamazaki, J.; Miyamoto, I.; Nishioka, H.; Akita, H.; Sato, Y.; Kataoka, M.; et al. Clinicopathologic and Immunohistochemical Findings from Autopsy of Patient with COVID-19, Japan. Emerg. Infect. Dis. 2020, 26, 2157–2161. [Google Scholar] [CrossRef]
- Xu, Z.; Shi, L.; Wang, Y.; Zhang, J.; Huang, L.; Zhang, C.; Liu, S.; Zhao, P.; Liu, H.; Zhu, L.; et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir. Med. 2020, 8, 420–422. [Google Scholar] [CrossRef]
- Youd, E.; Moore, L. COVID-19 autopsy in people who died in community settings: The first series. J. Clin. Pathol. 2020, 73, 840–844. [Google Scholar] [CrossRef] [PubMed]
- Oprinca, G.C.; Muja, L.A. Postmortem examination of three SARS-CoV-2-positive autopsies including histopathologic and immunohistochemical analysis. Int. J. Leg. Med. 2021, 135, 329–339. [Google Scholar] [CrossRef] [PubMed]
- Landa, N.A.; Oficialdegui, C.V.; Fernández, K.I.; Larrabe, I.G.; Onaindia, S.R.; Benguria, S.T. Ischemic-hemorrhagic stroke in patients with COVID-19. Rev. Española Anestesiol. Reanim. Engl. Ed. 2020, 67, 516–520. [Google Scholar]
- Wang, X.; Tu, Y.; Huang, B.; Li, Y.; Li, Y.; Zhang, S.; Lin, Y.; Huang, L.; Zhang, W.; Luo, H. Pulmonary vascular endothelial injury and acute pulmonary hypertension caused by COVID-19: The fundamental cause of refractory hypoxemia? Cardiovasc. Diagn. Ther. 2020, 10, 892–897. [Google Scholar] [CrossRef]
- Kantonen, J.; Mahzabin, S.; Mäyränpää, M.I.; Tynninen, O.; Paetau, A.; Andersson, N.; Sajantila, A.; Vapalahti, O.; Carpén, O.; Kekäläinen, E.; et al. Neuropathologic features of four autopsied COVID-19 patients. Brain Pathol. 2020, 30, 1012–1016. [Google Scholar] [CrossRef]
- Heinrich, F.; Sperhake, J.P.; Heinemann, A.; Mushumba, H.; Lennartz, M.; Nörz, D.; Glatzel, M.; Lütgehetmann, M.; Püschel, K. Germany’s first COVID-19 deceased: A 59-year-old man presenting with diffuse alveolar damage due to SARS-CoV-2 infection. Virchows Arch. 2020, 477, 335–339. [Google Scholar] [CrossRef]
- Yang, M.; Chen, S.; Huang, B.; Zhong, J.-M.; Su, H.; Chen, Y.-J.; Cao, Q.; Ma, L.; He, J.; Li, X.-F.; et al. Pathological Findings in the Testes of COVID-19 Patients: Clinical Implications. Eur. Urol. Focus 2020, 6, 1124–1129. [Google Scholar] [CrossRef]
- Stoyanov, G.S.; Lyutfi, E.; Dzhenkov, D.L.; Petkova, L. Acute Necrotizing Encephalitis in Viral Respiratory Tract Infection: An Autopsy Case Report. Cureus 2020, 12, e8070. [Google Scholar] [CrossRef]
- Iuga, A.C.; Marboe, C.C.; Yilmaz, M.M.; Lefkowitch, J.H.; Gauran, C.; Lagana, S.M. Adrenal Vascular Changes in COVID-19 Autopsies. Arch. Pathol. Lab. Med. 2020, 144, 1159–1160. [Google Scholar] [CrossRef]
- Reichard, R.R.; Kashani, K.B.; Boire, N.A.; Constantopoulos, E.; Guo, Y.; Lucchinetti, C.F. Neuropathology of COVID-19: A spectrum of vascular and acute disseminated encephalomyelitis (ADEM)-like pathology. Acta Neuropathol. 2020, 140, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Baud, D.; Greub, G.; Favre, G.; Gengler, C.; Jaton, K.; Dubruc, E.; Pomar, L. Second-trimester miscarriage in a pregnant woman with SARS-CoV-2 infection. JAMA 2020, 323, 2198–2200. [Google Scholar] [CrossRef] [PubMed]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Bulfamante, G.P.; Perrucci, G.L.; Falleni, M.; Sommariva, E.; Tosi, D.; Martinelli, C.; Songia, P.; Poggio, P.; Carugo, S.; Pompilio, G. Evidence of SARS-CoV-2 transcriptional activity in cardiomyocytes of COVID-19 patients without clinical signs of cardiac involvement. Biomedicines 2020, 8, 626. [Google Scholar] [CrossRef] [PubMed]
- Dettmeyer, R.; Lasczkowski, G.; Weber, A.; Wolter, T.; Kernbach-Wighton, G. Histopathological findings following SARS-CoV-2 infection with and without treatment-Report of three autopsies. Rechtsmedizin 2020, 1–8. [Google Scholar] [CrossRef]
- Fitzek, A.; Sperhake, J.; Edler, C.; Schröder, A.S.; Heinemann, A.; Heinrich, F.; Ron, A.; Mushumba, H.; Lütgehetmann, M.; Püschel, K. Evidence for systematic autopsies in COVID-19 positive deceased. Rechtsmedizin 2020, 30, 184–189. [Google Scholar] [CrossRef] [PubMed]
- Barnes, B.J.; Adrover, J.M.; Baxter-Stoltzfus, A.; Borczuk, A.; Cools-Lartigue, J.; Crawford, J.M.; Daßler-Plenker, J.; Guerci, P.; Huynh, C.; Knight, J.S.; et al. Targeting potential drivers of COVID-19: Neutrophil extracellular traps. J. Exp. Med. 2020, 217, e20200652. [Google Scholar] [CrossRef]
- Brook, O.R.; Piper, K.G.; Mercado, N.B.; Gebre, M.S.; Barouch, D.H.; Busman-Sahay, K.; Starke, C.E.; Estes, J.D.; Martinot, A.J.; Wrijil, L.; et al. Feasibility and safety of ultrasound-guided minimally invasive autopsy in COVID-19 patients. Abdom. Radiol. 2021, 46, 1263–1271. [Google Scholar] [CrossRef]
- McMullen, P.D.; Cho, J.H.; Miller, J.L.; Husain, A.N.; Pytel, P.; Krausz, T. A Descriptive and Quantitative Immunohistochemical Study Demonstrating a Spectrum of Platelet Recruitment Patterns Across Pulmonary Infections Including COVID-19. Am. J. Clin. Pathol. 2020, 155, 354–363. [Google Scholar] [CrossRef]
- Santana, M.F.; Borba, M.G.S.; Baía-da-Silva, D.C.; Val, F.; Alexandre, M.A.A.; Brito-Sousa, J.D.; Melo, G.C.; Queiroga, M.V.O.; Farias, M.E.L.; Camilo, C.C.; et al. Case report: Adrenal pathology findings in severe COVID-19: An autopsy study. Am. J. Trop. Med. Hyg. 2020, 103, 1604–1607. [Google Scholar] [CrossRef]
- Occidental, M.; Flaifel, A.; Lin, L.H.; Guzzetta, M.; Thomas, K.; Jour, G. Investigating the spectrum of dermatologic manifestations in COVID-19 infection in severely ill patients: A series of four cases. J. Cutan. Pathol. 2021, 48, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Fox, S.E.; Li, G.; Akmatbekov, A.; Harbert, J.L.; Lameira, F.S.; Brown, J.Q.; Heide, R.S.V. Unexpected Features of Cardiac Pathology in COVID-19 Infection. Circulation 2020, 142, 1123–1125. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Uppal, N.N.; Wanchoo, R.; Shah, H.H.; Yang, Y.; Parikh, R.; Khanin, Y.; Madireddy, V.; Larsen, C.P.; Jhaveri, K.D.; et al. COVID-19–Associated Kidney Injury: A Case Series of Kidney Biopsy Findings. J. Am. Soc. Nephrol. 2020, 31, 1948–1958. [Google Scholar] [CrossRef] [PubMed]
- Sasbou, L.; El Boussaadani, B.; Fellat, I.; Cherti, M. COVID-19 Myocarditis: Myth or Reality? J. Saudi Heart Assoc. 2020, 32, 421. [Google Scholar] [CrossRef] [PubMed]
- Del Nonno, F.; Frustaci, A.; Verardo, R.; Chimenti, C.; Nicastri, E.; Antinori, A.; Petrosillo, N.; Lalle, E.; Agrati, C.; Ippolito, G.; et al. Virus-negative myopericarditis in human coronavirus infection: Report from an autopsy series. Circ. Heart Fail. 2020, 13, e007636. [Google Scholar] [CrossRef]
- Attoh, S.A.; Hobenu, F.; Edusei, L.; Agyeman-Bediako, K.; Laryea, C.T.; Nyarko, E.O.; Amedi, M.K.; Asmah, R.H.; Asumanu, E.; McAddy, M.; et al. Postmortem diagnosis of COVID-19: Antemortem challenges of three cases at the 37 Military Hospital, Accra, Ghana. Afr. J. Lab. Med. 2020, 9, 1290. [Google Scholar] [CrossRef]
- Grimes, Z.; Bryce, C.; Sordillo, E.M.; Gordon, R.E.; Reidy, J.; Mondolfi, A.E.P.; Fowkes, M. Fatal pulmonary thromboembolism in SARS-CoV-2-infection. Cardiovasc. Pathol. 2020, 48, 107227. [Google Scholar] [CrossRef]
- Fox, S.E.; Akmatbekov, A.; Harbert, J.L.; Li, G.; Brown, J.Q.; Heide, R.S.V. Pulmonary and cardiac pathology in African American patients with COVID-19: An autopsy series from New Orleans. Lancet Respir. Med. 2020, 8, 681–686. [Google Scholar] [CrossRef]
- Löffler, K.U.; Reinhold, A.; Herwig-Carl, M.C.; Tzankov, A.; Holz, F.G.; Scholl, H.P.; Meyer, P. Ocular post-mortem findings in patients having died from COVID-19. Ophthalmol. Z. Dtsch. Ophthalmol. Ges. 2020, 117, 648–651. [Google Scholar]
- Khaba, M.C.; Ngale, T.C.; Madala, N. COVID-19 in an HIV-infected patient. Lessons learned from an autopsy case. Int. J. Infect. Dis. 2020, 101, 243–246. [Google Scholar] [CrossRef]
- Gauchotte, G.; Venard, V.; Segondy, M.; Cadoz, C.; Esposito-Fava, A.; Barraud, D.; Louis, G. SARS-Cov-2 fulminant myocarditis: An autopsy and histopathological case study. Int. J. Leg. Med. 2021, 135, 577–581. [Google Scholar] [CrossRef] [PubMed]
- Titi, L.; Magnanimi, E.; Mancone, M.; Infusino, F.; Coppola, G.; Del Nonno, F.; Colombo, D.; Nardacci, R.; Falasca, L.; D’Amati, G.; et al. Fatal Takotsubo syndrome in critical COVID-19 related pneumonia. Cardiovasc. Pathol. 2021, 51, 107314. [Google Scholar] [CrossRef] [PubMed]
- Basso, C.; Leone, O.; Rizzo, S.; De Gaspari, M.; Van Der Wal, A.C.; Aubry, M.-C.; Bois, M.C.; Lin, P.T.; Maleszewski, J.J.; Stone, J.R. Pathological features of COVID-19-associated myocardial injury: A multicentre cardiovascular pathology study. Eur. Heart J. 2020, 41, 3827–3835. [Google Scholar] [CrossRef] [PubMed]
- Yan, L.; Mir, M.; Sanchez, P.; Beg, M.; Peters, J.; Enriquez, O.; Gilbert, A. COVID-19 in a Hispanic Woman: Autopsy Report with Clinical Pathological Correlation. Arch. Pathol. Lab. Med. 2020, 144, 1041–1047. [Google Scholar] [CrossRef]
- Bradley, B.T.; Maioli, H.; Johnston, R.; Chaudhry, I.; Fink, S.L.; Xu, H.; Najafian, B.; Deutsch, G.; Lacy, J.M.; Williams, T.; et al. Histopathology and ultrastructural findings of fatal COVID-19 infections in Washington State: A case series. Lancet 2020, 396, 320–332. [Google Scholar] [CrossRef]
- Yao, X.H.; Li, T.Y.; He, Z.C.; Ping, Y.F.; Liu, H.W.; Yu, S.C.; Mou, H.M.; Wang, L.H.; Zhang, H.R.; Fu, W.J.; et al. A pathological report of three COVID-19 cases by minimally invasive autopsies. Zhonghua Bing Li Xue Za Zhi 2020, 49, E009. [Google Scholar]
- Wichmann, D. Autopsy Findings and Venous Thromboembolism in Patients with COVID-19. Ann. Intern. Med. 2020, 173, 1030. [Google Scholar]
- Wichmann, D.; Sperhake, J.P.; Lütgehetmann, M.; Steurer, S.; Edler, C.; Heinemann, A.; Heinrich, F.; Mushumba, H.; Kniep, I.; Schröder, A.S.; et al. Autopsy findings and venous thromboembolism in patients with COVID-19: A prospective cohort study. Ann. Intern. Med. 2020, 173, 268–277. [Google Scholar] [CrossRef]
- Okudela, K.; Hayashi, H.; Yoshimura, Y.; Sasaki, H.; Horiuchi, H.; Miyata, N.; Tachikawa, N.; Tsuchiya, Y.; Mitsui, H.; Ohashi, K. A Japanese case of COVID-19: An autopsy report. Pathol. Int. 2020, 70, 820–824. [Google Scholar] [CrossRef]
- Kirschenbaum, D.; Imbach, L.L.; Ulrich, S.; Rushing, E.J.; Keller, E.; Reimann, R.R.; Frauenknecht, K.; Lichtblau, M.; Witt, M.; Hummel, T.; et al. Inflammatory olfactory neuropathy in two patients with COVID-19. Lancet 2020, 396, 166. [Google Scholar] [CrossRef]
- Carsana, L.; Sonzogni, A.; Nasr, A.; Rossi, R.S.; Pellegrinelli, A.; Zerbi, P.; Rech, R.; Colombo, R.; Antinori, S.; Corbellino, M.; et al. Pulmonary post-mortem findings in a series of COVID-19 cases from northern Italy: A two-centre descriptive study. Lancet Infect. Dis. 2020, 20, 1135–1140. [Google Scholar] [CrossRef]
- Kirschenbaum, D.; Imbach, L.L.; Rushing, E.J.; Frauenknecht, K.B.M.; Gascho, D.; Ineichen, B.V.; Keller, E.; Kohler, S.; Lichtblau, M.; Reimann, R.R.; et al. Intracerebral endotheliitis and microbleeds are neuropathological features of COVID-19. Neuropathol. Appl. Neurobiol. 2020, 47, 454–459. [Google Scholar] [CrossRef] [PubMed]
- Magro, C.M.; Mulvey, J.; Kubiak, J.; Mikhail, S.; Suster, D.; Crowson, A.N.; Laurence, J.; Nuovo, G. Severe COVID-19: A multifaceted viral vasculopathy syndrome. Ann. Diagn. Pathol. 2021, 50, 151645. [Google Scholar] [CrossRef] [PubMed]
- Leppkes, M.; Knopf, J.; Naschberger, E.; Lindemann, A.; Singh, J.; Herrmann, I.; Stürzl, M.; Staats, L.; Mahajan, A.; Schauer, C.; et al. Vascular occlusion by neutrophil extracellular traps in COVID-19. EBioMedicine 2020, 58, 102925. [Google Scholar] [CrossRef]
- Diao, B.; Wang, C.; Wang, R.; Feng, Z.; Zhang, J.; Yang, H.; Tan, Y.; Wang, H.; Wang, C.; Liu, L.; et al. Human kidney is a target for novel severe acute respiratory syndrome coronavirus 2 infection. Nat. Commun. 2021, 12, 2506. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Xiao, X.; Zhang, J.; Zafar, M.I.; Wu, C.; Long, Y.; Lu, W.; Pan, F.; Meng, T.; Zhao, K.; et al. Impaired spermatogenesis in COVID-19 patients. EClinicalMedicine 2020, 28, 100604. [Google Scholar] [CrossRef] [PubMed]
- Solomon, I.H.; Normandin, E.; Bhattacharyya, S.; Mukerji, S.S.; Keller, K.; Ali, A.S.; Adams, G.; Hornick, J.L.; Padera, R.F., Jr.; Sabeti, P. Neuropathological Features of COVID-19. N. Engl. J. Med. 2020, 383, 989–992. [Google Scholar] [CrossRef]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Qu, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. China medical treatment expert group for COVID-19 2020. Clinical Characteristics of coronavirus disease in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Gu, J.; Korteweg, C. Pathology and Pathogenesis of Severe Acute Respiratory Syndrome. Am. J. Pathol. 2007, 170, 1136–1147. [Google Scholar] [CrossRef] [Green Version]
- Chong, P.Y.; Chui, P.; Ling, A.E.; Franks, T.J.; Tai, D.Y.; Leo, Y.S.; Kaw, G.J.; Wansaicheong, G.; Chan, K.P.; Ean Oon, L.L.; et al. Analysis of deaths during the severe acute respiratory syndrome (SARS) epidemic in Singapore: Challenges in determining a SARS diagnosis. Arch. Pathol. Lab. Med. 2004, 128, 195–204. [Google Scholar] [CrossRef]
- Nicholls, J.M.; Poon, L.; Lee, K.C.; Ng, W.F.; Lai, S.T.; Leung, C.Y.; Chu, C.M.; Hui, P.K.; Mak, K.L.; Lim, W.; et al. Lung pathology of fatal severe acute respiratory syndrome. Lancet 2003, 361, 1773–1778. [Google Scholar] [CrossRef] [Green Version]
- Burkhard-Koren, N.M.; Haberecker, M.; Maccio, U.; Ruschitzka, F.; Schuepbach, R.A.; Zinkernagel, A.S.; Hardmeier, T.; Varga, Z.; Moch, H. Higher prevalence of pulmonary macrothrombi in SARS-CoV-2 than in influenza A: Autopsy results from ‘Spanish flu’1918/1919 in Switzerland to Coronavirus disease 2019. J. Pathol. Clin. Res. 2021, 7, 135–143. [Google Scholar] [CrossRef]
- Memish, Z.A.; Perlman, S.; Van Kerkhove, M.D.; Zumla, A. Middle East respiratory syndrome. Lancet 2020, 395, 1063–1077. [Google Scholar] [CrossRef]
- Zhu, Z.; Lian, X.; Su, X.; Wu, W.; Marraro, G.A.; Zeng, Y. From SARS and MERS to COVID-19: A brief summary and comparison of severe acute respiratory infections caused by three highly pathogenic human coronaviruses. Respir. Res. 2020, 21, 224. [Google Scholar] [CrossRef] [PubMed]
- Ng, D.L.; Al Hosani, F.; Keating, M.K.; Gerber, S.I.; Jones, T.L.; Metcalfe, M.G.; Tong, S.; Tao, Y.; Alami, N.N.; Haynes, L.M.; et al. Clinicopathologic, Immunohistochemical, and Ultrastructural Findings of a Fatal Case of Middle East Respiratory Syndrome Coronavirus Infection in the United Arab Emirates, April 2014. Am. J. Pathol. 2016, 186, 652–658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alsaad, K.O.; Hajeer, A.H.; Al Balwi, M.; Al Moaiqel, M.; Al Oudah, N.; Al Ajlan, A.; AlJohani, S.; Alsolamy, S.; Gmati, G.E.; Balkhy, H.; et al. Histopathology of Middle East respiratory syndrome coronovirus (MERS-CoV) infection–clinicopathological and ultrastructural study. Histopathology 2018, 72, 516–524. [Google Scholar] [CrossRef]
- Raj, V.S.; Mou, H.; Smits, S.L.; Dekkers, D.H.; Müller, M.A.; Dijkman, R.; Muth, D.; Demmers, J.A.; Zaki, A.; Fouchier, R.A.; et al. Dipeptidyl peptidase 4 is a functional receptor for the emerging human coronavirus-EMC. Nature 2013, 495, 251–254. [Google Scholar] [CrossRef] [Green Version]
- Ng, W.-F.; To, K.-F.; Lam, W.W.; Ng, T.-K.; Lee, K.-C. The comparative pathology of severe acute respiratory syndrome and avian influenza A subtype H5N1—A review. Hum. Pathol. 2006, 37, 381–390. [Google Scholar] [CrossRef]
- Feldmann, H.; Geisbert, T.W. Ebola haemorrhagic fever. Lancet 2011, 377, 849–862. [Google Scholar] [CrossRef] [Green Version]
- Kim, B.; Figueroa-Romero, C.; Pacut, C.; Backus, C.; Feldman, E. Insulin Resistance Prevents AMPK-induced Tau Dephosphorylation through Akt-mediated Increase in AMPKSer-485 Phosphorylation. J. Biol. Chem. 2015, 290, 19146–19157. [Google Scholar] [CrossRef] [Green Version]
- Vasquez-Bonilla, W.O.; Orozco, R.; Argueta, V.; Sierra, M.; Zambrano, L.I.; Muñoz-Lara, F.; López-Molina, D.S.; Arteaga-Livias, K.; Grimes, Z.; Bryce, C.; et al. A review of the main histopathological findings in coronavirus disease 2019. Hum. Pathol. 2020, 105, 74–83. [Google Scholar] [CrossRef] [PubMed]
- Pujhari, S.; Paul, S.; Ahluwalia, J.; Rasgon, J.L. Clotting disorder in severe acute respiratory syndrome coronavirus 2. Rev. Med Virol. 2021, 31, e2177. [Google Scholar] [CrossRef] [PubMed]
- Deshmukh, V.; Motwani, R.; Kumar, A.; Kumari, C.; Raza, K. Histopathological observations in COVID-19: A systematic review. J. Clin. Pathol. 2021, 74, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Parry, A.H.; Wani, A.H.; Yaseen, M.; Dar, M.I. Demystifying pulmonary vascular complications in severe coronavirus disease-19 pneumonia (COVID-19) in the light of clinico-radiologic-pathologic correlation. Thromb. Res. 2020, 196, 559–560. [Google Scholar] [CrossRef]
- Barth, R.F.; Buja, L.M.; Parwani, A.V. The spectrum of pathological findings in coronavirus disease (COVID-19) and the pathogenesis of SARS-CoV-2. Diagn. Pathol. 2020, 15, 85. [Google Scholar] [CrossRef]
- Goeijenbier, M.; van Wissen, M.; van de Weg, C.; Jong, E.; Gerdes, V.; Meijers, J.; Brandjes, D.; van Gorp, E. Review: Viral infections and mechanisms of thrombosis and bleeding. J. Med. Virol. 2012, 84, 1680–1696. [Google Scholar] [CrossRef]
- Hwang, D.M.; Chamberlain, D.W.; Poutanen, S.; Low, D.E.; Asa, S.; Butany, J. Pulmonary pathology of severe acute respiratory syndrome in Toronto. Mod. Pathol. 2004, 18, 1–10. [Google Scholar] [CrossRef]
- Keller, T.T.; Van Der Sluijs, K.F.; de Kruif, M.; Gerdes, V.E.A.; Meijers, J.C.M.; Florquin, S.; Van Der Poll, T.; Van Gorp, E.C.M.; Brandjes, D.P.M.; Buller, H.R.; et al. Effects on Coagulation and Fibrinolysis Induced by Influenza in Mice with a Reduced Capacity to Generate Activated Protein C and a Deficiency in Plasminogen Activator Inhibitor Type 1. Circ. Res. 2006, 99, 1261–1269. [Google Scholar] [CrossRef]
- Muramoto, Y.; Ozaki, H.; Takada, A.; Park, C.-H.; Sunden, Y.; Umemura, T.; Kawaoka, Y.; Matsuda, H.; Kida, H. Highly Pathogenic H5N1 Influenza Virus Causes Coagulopathy in Chickens. Microbiol. Immunol. 2006, 50, 73–81. [Google Scholar] [CrossRef]
- Han, M.; Yan, W.; Huang, Y.; Yao, H.; Wang, Z.; Xi, D.; Li, W.; Zhou, Y.; Hou, J.; Luo, X.; et al. The nucleocapsid protein of SARS-CoV induces transcription of hfgl2 prothrombinase gene dependent on C/EBP alpha. J. Biochem. 2008, 144, 51–62. [Google Scholar] [CrossRef] [Green Version]
- Rose, N.R. Viral myocarditis. Curr. Opin. Rheumatol. 2016, 28, 383–389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, L.; Li, X.; Chen, M.; Feng, Y.; Xiong, C. The ACE2 expression in human heart indicates new potential mechanism of heart injury among patients infected with SARS-CoV-2. Cardiovasc. Res. 2020, 116, 1097–1100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costela-Ruiz, V.J.; Illescas-Montes, R.; Puerta-Puerta, J.M.; Ruiz, C.; Melguizo-Rodríguez, L. SARS-CoV-2 infection: The role of cytokines in COVID-19 disease. Cytokine Growth Factor Rev. 2020, 54, 62–75. [Google Scholar] [CrossRef] [PubMed]
- Chimenti, C.; Magnocavallo, M.; Ballatore, F.; Bernardini, F.; Alfarano, M.; Della Rocca, D.G.; Severino, P.; Lavalle, C.; Francesco, F.; Frustaci, A. Prevalence and Clinical Implications of COVID-19 Myocarditis. Card. Electrophysiol. Clin. 2021, 14, 53–62. [Google Scholar] [CrossRef]
- Siripanthong, B.; Nazarian, S.; Muser, D.; Deo, R.; Santangeli, P.; Khanji, M.Y.; Cooper, L.T.; Chahal, C.A.A. Recognizing COVID-19–related myocarditis: The possible pathophysiology and proposed guideline for diagnosis and management. Heart Rhythm 2020, 17, 1463–1471. [Google Scholar] [CrossRef]
- Halushka, M.K.; Heide, R.S.V. Myocarditis is rare in COVID-19 autopsies: Cardiovascular findings across 277 postmortem examinations. Cardiovasc. Pathol. 2021, 50, 107300. [Google Scholar] [CrossRef]
- Roy, D.; Ghosh, R.; Dubey, S.; Dubey, M.J.; Benito-León, J.; Ray, B.K. Neurological and Neuropsychiatric Impacts of COVID-19 Pandemic. Can. J. Neurol. Sci. 2021, 48, 9–24. [Google Scholar] [CrossRef]
- Talbot, P.J. Coronaviruses as Encephalitis—Inducing Infectious Agents; IntechOpen: London, UK, 2011. [Google Scholar]
- Desforges, M.; Le Coupanec, A.; Dubeau, P.; Bourgouin, A.; Lajoie, L.; Dube, M.; Talbot, P.J. Human Coronaviruses and Other Respiratory Viruses: Underestimated Opportunistic Pathogens of the Central Nervous System? Viruses 2019, 12, 14. [Google Scholar] [CrossRef] [Green Version]
- Ellul, M.A.; Benjamin, L.; Singh, B.; Lant, S.; Michael, B.D.; Easton, A.; Kneen, R.; Defres, S.; Sejvar, J.; Solomon, T. Neurological associations of COVID-19. Lancet Neurol. 2020, 19, 767–783. [Google Scholar] [CrossRef]
- Siow, I.; Lee, K.S.; Zhang, J.J.Y.; Saffari, S.E.; Ng, A. Encephalitis as a neurological complication of COVID-19: A systematic review and meta-analysis of incidence, outcomes, and predictors. Eur. J. Neurol. 2021, 28, 3491–3502. [Google Scholar] [CrossRef]
- Ye, M.; Ren, Y.; Lv, T. Encephalitis as a clinical manifestation of COVID-19. Brain Behav. Immun. 2020, 88, 945–946. [Google Scholar] [CrossRef] [PubMed]
- Scott, L.; Hsiao, N.-Y.; Moyo, S.; Singh, L.; Tegally, H.; Dor, G.; Maes, P.; Pybus, O.G.; Kraemer, M.U.G.; Semenova, E.; et al. Track Omicron’s spread with molecular data. Science 2021, 374, 1454–1455. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Iketani, S.; Guo, Y.; Chan, J.F.W.; Wang, M.; Liu, L.; Luo, Y.; Chu, H.; Huang, Y.; Nair, M.S.; et al. Striking antibody evasion manifested by the Omicron variant of SARS-CoV-2. Nature 2022, 602, 676–681. [Google Scholar] [CrossRef] [PubMed]
- Haberman, R.; Axelrad, J.; Chen, A.; Castillo, R.; Yan, D.; Izmirly, P.; Neimann, A.; Adhikari, S.; Hudesman, D.; Scher, J.U. COVID-19 in Immune-Mediated Inflammatory Diseases—Case Series from New York. N. Engl. J. Med. 2020, 383, 85–88. [Google Scholar] [CrossRef] [PubMed]
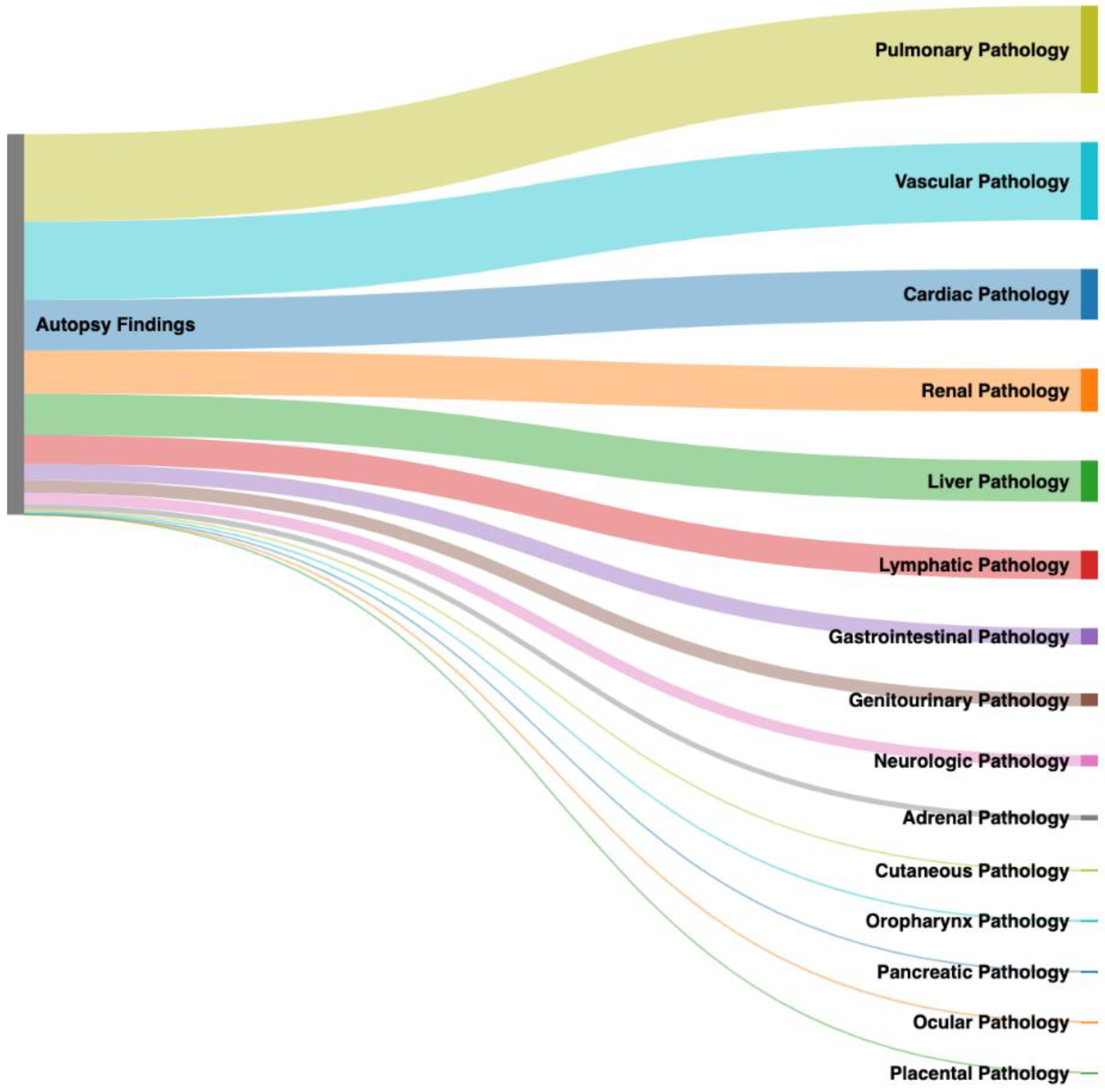
Figure 1.
Graphical representation of the distribution of post-mortem organ system pathology ranging from greatest prevalence to lowest prevalence in this review of 1142 COVID-19 patients.
Figure 1.
Graphical representation of the distribution of post-mortem organ system pathology ranging from greatest prevalence to lowest prevalence in this review of 1142 COVID-19 patients.

Figure 2.
Selection process used for selecting published autopsy reports of COVID-19 infections.

Figure 3.
Graphical representation of the prevalence of vascular pathology in this review of 1142 COVID-19 decedents, with visualization of the high frequency of thrombotic complications and further characterization of microvascular and macrovascular thrombi.
Figure 3.
Graphical representation of the prevalence of vascular pathology in this review of 1142 COVID-19 decedents, with visualization of the high frequency of thrombotic complications and further characterization of microvascular and macrovascular thrombi.


{kind=link}
{kind=link}
{kind=link}
Table 1.
Summary of the most common post-mortem findings in 1142 COVID-19 decedents organized by organ system. The total number of autopsies displaying organ system pathology and the corresponding prevalence of the specific findings are listed.
Table 1.
Summary of the most common post-mortem findings in 1142 COVID-19 decedents organized by organ system. The total number of autopsies displaying organ system pathology and the corresponding prevalence of the specific findings are listed.
| Organ Systems (# of Autopsies with Pathology) | Common Pathology (% of Autopsies with Pathology) |
|---|---|
| Pulmonary (n = 865) | DAD (65%), consolidations (32%), alveolar edema (29%), hyaline membranes (28%), type II pneumocyte hyperplasia (20%), alveolar hemorrhage (19%), thrombus (10%), lymphocyte dominate inflammation (10%), pleural effusion (5%), PE (3%) |
| Cardiac (n = 502) | Cardiac inflammation (37%), hypertrophy (20%), fibrosis (26%), cardiomegaly (20%), ventricular dilation (7%) |
| Vasculature (n = 771) | Thrombi (57%), inflammatory cell infiltrates (15%) |
| Renal (n = 427) | Arteriosclerosis (26%) of the renal arteries, shock kidney (19%), acute tubular necrosis (18%) |
| Liver (n = 407) | Steatosis (26%), congestion (25%), shock liver (20%) |
| Lymphatic (n = 284) | Spleen (n = 266): congestion (38%), white pulp depletion (14%), autolysis (12%); Lymph Nodes (n = 18): enlarged mediastinal (78%), hilar pulmonary lymph nodes (78%), loss of germinal centers 11 (61%) |
| Gastrointestinal (n = 162) | Shock changes (49%) |
| Genitourinary (n = 127) | Testis (n = 33): interstitial edema (52%); Prostate (n = 94): thrombosis (8%) |
| Neurologic (n = 111) | Brain (n = 109): hypoxic-ischemic injury (18%); Olfactory bulbs (n = 2): edema (100%), neuronal degeneration (100%), neuronal necrosis (100%) and inflammatory infiltrate (100%) |
| Adrenal (n = 53) | Macroscopic lesions (23%) |
| Cutaneous (n = 19) | Thrombotic microangiopathy (53%) |
| Oropharynx (n = 15) | Pharynx (n = 8): lymphocytic pharyngitis (88%); Oral cavity (n = 7): keratinocytes of junctional epithelium (100%) |
| Pancreas (n = 13) | Necrosis (38%) |
| Ocular (n = 3) | Autolysis (100%), cataracts (100%) |
| Placenta (n = 1) | Subchorial inflammation (100%), intervillous fibrin deposits (100%), funisitis (100%) |
| Total Number of Autopsies (n = 1142) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Chawla, K.; Hong, S.; Shields, R.; Ford, A.; Pacella, G.; Lurie, F. Multifactorial Effects of COVID-19: A Review of Published Autopsy Reports. COVID 2022, 2, 553-568. https://0-doi-org.brum.beds.ac.uk/10.3390/covid2050041
AMA Style
Chawla K, Hong S, Shields R, Ford A, Pacella G, Lurie F. Multifactorial Effects of COVID-19: A Review of Published Autopsy Reports. COVID. 2022; 2(5):553-568. https://0-doi-org.brum.beds.ac.uk/10.3390/covid2050041
Chicago/Turabian StyleChawla, Karan, Stephen Hong, Ryan Shields, Alexandra Ford, Gioia Pacella, and Fedor Lurie. 2022. "Multifactorial Effects of COVID-19: A Review of Published Autopsy Reports" COVID 2, no. 5: 553-568. https://0-doi-org.brum.beds.ac.uk/10.3390/covid2050041