
HHV-6 in Cerebrospinal Fluid in Immunocompetent Children
by
 , ,
, ,
Mikhail A. Nikolskiy
1,* ,
,
Dmitriy A. Lioznov
2,3,*,
Evgeniy U. Gorelik
4 and
Tatyana V. Vishnevskaya
4 1
Department of Pediatrics, Pavlov First Saint Petersburg State Medical University, 197022 St. Petersburg, Russia
2
Department of Infectious Diseases, Pavlov First Saint Petersburg State Medical University, 197022 St. Petersburg, Russia
3
Smorodintsev Research Institute of Influenza, 197376 St. Petersburg, Russia
4
Infectious Diseases Department No. 7, N.F. Filatov Children’s City Clinical Hospital No. 5, 192289 St. Petersburg, Russia
*
Authors to whom correspondence should be addressed.
BioMed 2023, 3(3), 420-430; https://0-doi-org.brum.beds.ac.uk/10.3390/biomed3030034
Submission received: 31 July 2023
/
Revised: 13 September 2023
/
Accepted: 13 September 2023
/
Published: 20 September 2023
Abstract
:Background: Human herpes virus-6 (HHV-6) is a ubiquitous virus known as an etiological agent of exanthem subitum. HHV-6-encephalitis in immunocompetent children is a rare complication of the primary infection. There are a lack of data on the prevalence of HHV-6-encephalitis in Russia. The aim of our study was to analyze the prevalence of HHV-6 DNA in the cerebrospinal fluid (CSF) of immunocompetent children with suspected acute meningoencephalitis. Materials and Methods: A total of 712 CSF samples were tested using qualitative PCR over 12 years at N.F. Filatov Children’s City Clinical Hospital No.5, Saint-Petersburg, Russia. Results: HHV-6 DNA was detected in 20 (2.8%) of the samples. Retrospectively, we analyzed the medical records of 15 cases. There were seven boys and eight girls from 1 month to 7 years old; the mean age was 22.3 ± 5.6 months. Most HHV-6 DNA-positive cases were due to the primary form of HHV-6 infection. There were, in total, four cases of HHV-6-meningoencephalitis. All the children had a complete recovery, without neurological deficits or death. Conclusions: HHV-6 encephalitis is a very rare disease in immunocompetent children (four cases among 712 samples over 12 years). Additional studies are needed to develop accurate diagnostic criteria and therapeutic approaches.
1. Introduction
HHV-6 is a widespread herpes virus that was first discovered in 1986, and later, in 2012, divided into two separate biological species—HHV-6A and HHV-6B. Most clinical forms of this infection are associated with HHV-6B, whereas the role of HHV-6A in human pathology is still unclear. The transmission of HHV-6 occurs through saliva, which is the main reservoir of the pathogen. The virus causes different forms of the acute infection process, mainly in children from 6 to 18 months of age [1]. The incubation period is usually 7–10 days. Exanthem subitum (ES) (roseola infantum), known as the “sixth disease” since the beginning of the 20th century, has been studied in detail. ES is characterized by fever for three–four days, followed by the appearance of a blanching macular or maculopapular rash. Another form of the infection is fever without a rash. The characteristic symptoms of primary HHV-6 infection are fever, enlarged occipital lymph nodes, and a typical rash that appears after the normalization of body temperature. White blood cell counts often show leukopenia or a normal count, which is an important feature for diagnostic purposes in a febrile infant [2].
Although a primary HHV-6 infection is not life-threatening and does not require antiviral treatment, it causes frequent hospitalization in children under 2 years of age. About 10% of children with fever admitted to the hospital had a primary HHV-6 infection [3]. A certain seasonality of primary HHV-6 infection, with an increase in summer and fall, has been described [4].
HHV-6 has neurotrophic properties [5] with predominant damage to the limbic system. It may lead to severe irritability and/or apathy, that peaks on the last day of the fever before the appearance of a rash, even in patients with an uncomplicated primary infection. In addition, up to 20–30% of febrile seizures (FS) in children are caused by a primary HHV-6 infection [6]. FS usually occurs on the first or second day of fever and affects nearly 10–15% of children with a primary HHV-6 infection [2]. A series of convulsions that occur after the normalization of body temperature at the time of the appearance of the rash is called “HHV-6 encephalopathy with cluster of convulsions in eruptive stage” (HECCES) [7]. Afebrile seizures associated with HHV-6 have also been described in neonates [8]. Convulsions in HHV-6 infections are often complex and can lead to febrile epileptic status and subsequent epilepsy [9,10]. HHV-6 is thought to be associated with mesial temporal lobe epilepsy (MTLE) [11], one of the most common forms of focal epilepsy, caused by hippocampal sclerosis. The role of HHV-6 in the pathogenesis of multiple sclerosis and Alzheimer’s disease has also been considered [12].
HHV-6 infection may be complicated by a central nervous system (CNS) infection. In immunocompromised patients after hematopoietic stem-cell transplantation (HCT) [13,14], there are well-documented cases of a unique form of HHV-6 meningoencephalitis, caused by primary infection or its reactivation—post-transplant acute limbic encephalitis (PALE). PALE develops in up to 34% of children at 2–8 weeks after HCT and is characterized by mood swings, impaired consciousness, seizures, automatism, and amnesia. The course of this disease is unfavorable and can lead to severe long-term consequences and death [15].
The frequency and manifestations of HHV-6 encephalitis in immunocompetent patients have not been sufficiently studied. The most frequent age of manifestation varies from 2 months to 3 years [16,17], which corresponds to the peak detection of primary infection. The development of HHV-6 encephalitis is possible with any form of primary HHV-6 infection (with or without rash).
A retrospective study in Italy [18] examined cerebrospinal fluid (CSF) samples from 304 children with suspected viral encephalitis. HHV-6 was detected in eight patients (4.8%); half of them were less than 1 year old. Another Italian study found four cases of HHV-6 encephalitis in primary infection over a 10-year period [13]. Similar data with 10 confirmed cases (8.8%) were obtained in Iran [15] from 114 children under 2 years of age with suspected encephalitis and without signs of exanthem subitum. In a national study of Japan [17], which covered the majority of hospitals in the country over a 2-year period (2003–2004), 86 cases of HHV-6 encephalitis associated with ES were identified. Neurological complications were noted in 47% of cases, and two deaths were even recorded. By extrapolation, the frequency of HHV-6 encephalitis was obtained as 61.9 cases of the disease per year or 5.5 episodes per 100,000 cases of exanthem subitum.
A certain seasonality of HHV-6 encephalitis registration was noted. According to [16], most cases of HHV-6 encephalitis were reported in the fall and winter.
There are a number of problems in diagnosing HHV-6 infection. Confirmation of an acute HHV-6 infection is based on the detection of HHV-6 DNA in plasma/serum, or seroconversion. The quantity of HHV-6 in the blood plasma in acute infection varies from 100 to 10,000 copies/mL. After a primary infection, the virus persists in the body indefinitely, remaining in peripheral blood mononuclear cells and saliva. Therefore, the detection of HHV-6 in white blood cells less than 100 copies/mL of whole blood, as well as the detection of the virus in saliva—regardless of its amount—is typical for the latent stage and does not indicate an active infection. In addition, the constant presence of HHV-6 in all body tissues is observed in a unique form of HHV-6 infection called chromosomally integrated HHV-6 (ciHHV-6), which is most often inherited. To exclude ciHHV-6, it is necessary to determine the presence of the virus in the blood at weekly intervals, or examine the nail plates and/or hair follicles, where the virus can be found only in ciHHV-6 patients. On the other hand, the absence of HHV-6 in the blood does not exclude an active localized infection, for example, in the brain. Thus, in patients with encephalitis, HHV-6 can be detected only in the CSF and may not be detected in the blood [19].
In HHV-6 encephalitis, the virus appears in the CSF 1–2 days after the onset of the first symptoms but persists there much longer than in the blood (up to 1 month vs. 1 week) [20]. The level of the HHV-6 viral load in acute infection in immunocompetent children varied from 15 to 7000 copies per ml and was generally lower than that in HHV-6 encephalitis in immunocompromised patients [21]. A high HHV-6 viral load in the CSF may be important for diagnosing and choosing a treatment strategy for HIV patients [22]. On the other hand, it is noted that the concentration of the virus in the blood and CSF may decrease to become undetectable, while the inflammation localized in the brain tissue is still active [23].
It should be noted that in primary infection, HHV-6 DNA can be detected in unchanged CSF [24]. HHV-6 was found in the CSF in 6% of children with FS [25]. In the chromosomally integrated form of HHV-6, the virus is constantly detected in the CSF at 100–1000 copies per ml [26]. In one study, it was shown that after a primary infection, HHV-6 can persist in small amounts in the brain tissue and might be reactivated in intercurrent diseases [27].
CSF analysis in HHV-6 encephalitis has limited diagnostic value. Pleocytosis and changes in protein and glucose levels are characteristic of meningoencephalitis and occur in a minority of cases [17]. There are conflicting data on the changes in leukocyte and neutrophil counts in peripheral blood in this disease. C-reactive protein (CRP) is usually not elevated. A number of studies have also reported a transient increase in hepatic transaminase activity, hyponatremia, thrombocytopenia, increased ferritin, coagulopathy, and disseminated intravascular coagulation [28,29,30].
According to current recommendations, magnetic resonance imaging (MRI) is indicated for all patients with suspected encephalitis. The majority of immunocompetent children with encephalitis show changes on MRI. In the early stage of the disease (the first days), subcortical restricted diffusion is detected, followed by hyperintensities of most brain regions. In the late stages of the disease, brain atrophy is registered [31]. In PALE the affected areas are located mainly in the medial temporal lobe of the brain, in the hippocampus, and in the amygdala [32].
Due to the high risk of seizures and epilepsy, electroencephalography (EEG) is recommended for all patients with encephalitis both during the disease and after recovery.
Methods of treatment of HHV-6 encephalitis in immunocompetent patients are not standardized. In most cases, etiotropic treatment is not used since the disease is self-limited. At the same time, given the high risk of long-term consequences after encephalitis and even after febrile seizures (epilepsy), the development of such recommendations seems relevant. The use of antiviral agents (ganciclovir, valganciclovir, foscarnet) has been described [14,23,33]. Corticosteroids are associated with a lower frequency of complications if used in the first days of encephalitis due to the suppression of the inflammatory process [33]. On the other hand, the use of steroids can lead to an increase in the viral load of HHV-6 [34].
Long-term sequelae of HHV-6 encephalitis occur in half of the patients and are manifested by motor disorders, ataxia, developmental disabilities, and memory impairment [19]. Rarer syndromes of severe CNS damage due to HHV-6 were also described. These include cases of fatal acute necrotizing encephalitis (ANE) [35], HSES (hemorrhagic shock and encephalopathy syndrome), and AESD (acute encephalopathy with biphasic seizure and late reduced diffusion) [36]. Isolated cases of autoimmune encephalitis [37] and Rasmussen’s encephalitis (a rare inflammatory disease affecting one hemisphere of the brain with seizures, progressive hemiparesis, and unilateral cerebral atrophy observed on MRI) have been reported [38].
Thus, there is no doubt of the importance of understanding of the prevalence, clinical and laboratory manifestations, and outcomes of encephalitis caused by HHV-6.
The aim of our work was to analyze the frequency and clinical significance of detecting HHV-6 in CSF in children with suspected meningoencephalitis.
2. Materials and Methods
The analysis included samples of cerebrospinal fluid from 712 patients sent to the laboratory of N.F. Filatov Children’s City Clinical Hospital No.5, Saint-Petersburg, Russia, in the period from 2007 to 2018. All the children admitted to the emergency department with suspected CNS infection were immunocompetent. The age of the patients ranged from 14 days to 17 years; the mean age was 34.2 ± 8.6 months.
CSF DNA analysis for HHV-6 was performed using qualitative PCR. PCR for HHV-7, HHV-6 genotyping, and exclusion of iciHHV-6 were not performed.
All reagents and devices were from the DNA-Technology company—“Proba NK”. To isolate HHV-6 DNA from blood and CSF, as well as amplify and detect the marker fragment of HHV-6 DNA, a mixture for amplification under paraffin, Taq-polymerase, mineral oil, as well as a set of reagents GenePak®® DNA PCR test (LLC “Laboratory Isogen”, Moscow, Russia) and amplifiers “Tertsik”, RTS-100 (MJ-Research Inc., Reno, NV, USA) were used. PCR detection of the HHV-6 product was performed at the end of amplification using a Jinn 1/4 fluorescent detector.
CSF was analyzed using the following parameters: CSF outflow pressure, color, turbidity, cytosis (the number of cell elements in 3 microL), glucose (mmol/L), and protein concentration (g/L). In all the cases, CSF culture, latex agglutination test (to quickly detect antigens of Neisseria meningitidis, Streptococcus pneumoniae, and Haemophilus influenzae serotype b (Hib)), and PCR testing for enterovirus, human herpesviruses types 1–2 (HSV), varicella-zoster virus (VZV), Epstein–Barr virus (EBV), and Cytomegalovirus (CMV) were performed. In children in the first months of life, PCR tests for Listeria monocytogenes and Streptococcus agalactiae were also performed. Additionally, during summer months, PCR for Tick-borne encephalitis virus and Borrelia burgdorferi was performed in children older than one year.
Signs of aseptic meningitis were considered in the case of cytosis above 30–90 cells in 3 microL (depending on the patient’s age) with a predominance of lymphocytes, decrease in glucose levels less than 2.8 mmol/L, and increase in protein more than 0.45 g/L. The cytosis of more than 1000 cells in 3 microL with a predominance of neutrophils was recorded as bacterial inflammation.
Most patients underwent additional examinations: EEG, ultrasound, and CT of the brain. MRI scan was not performed.
The study protocol was approved by the Ethics Committee of First Pavlov’s State Medical University, Saint-Petersburg, Russia. Informed consent was obtained from the parents at the time of the child’s hospitalization.
3. Results
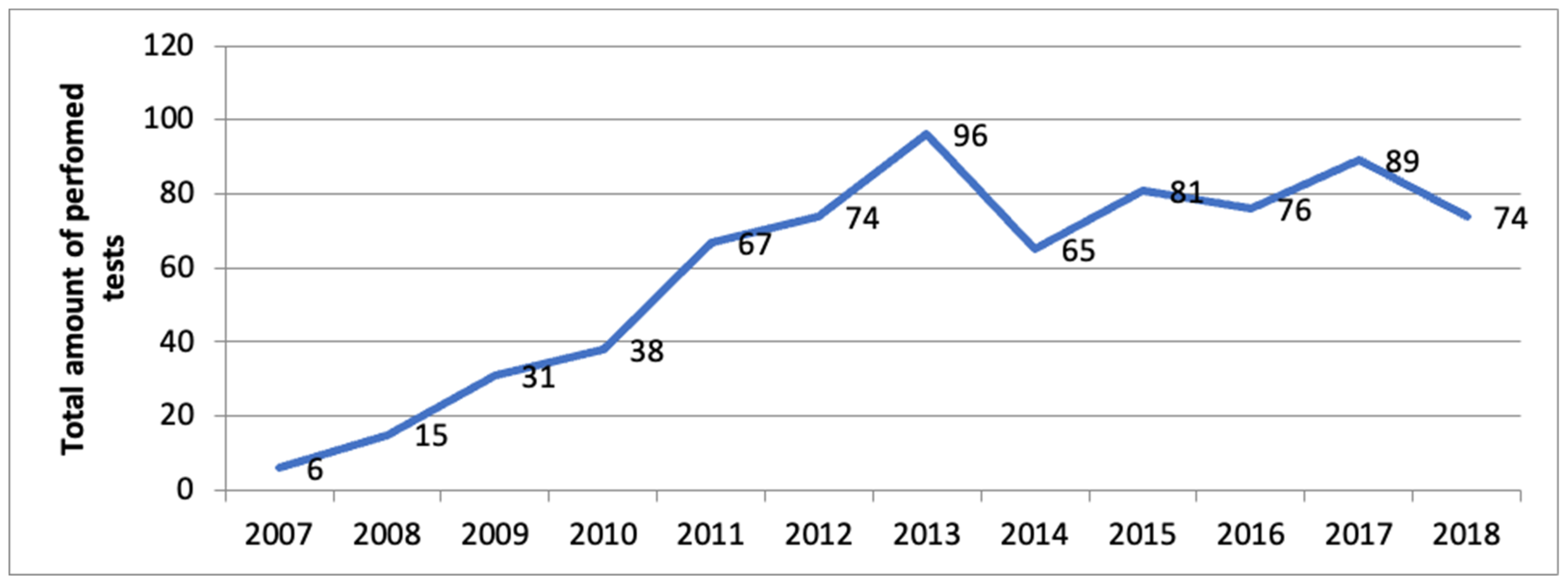
The annual number of CSF studies for HHV-6 from 2007 to 2018 increased by 10–15 times (Figure 1).
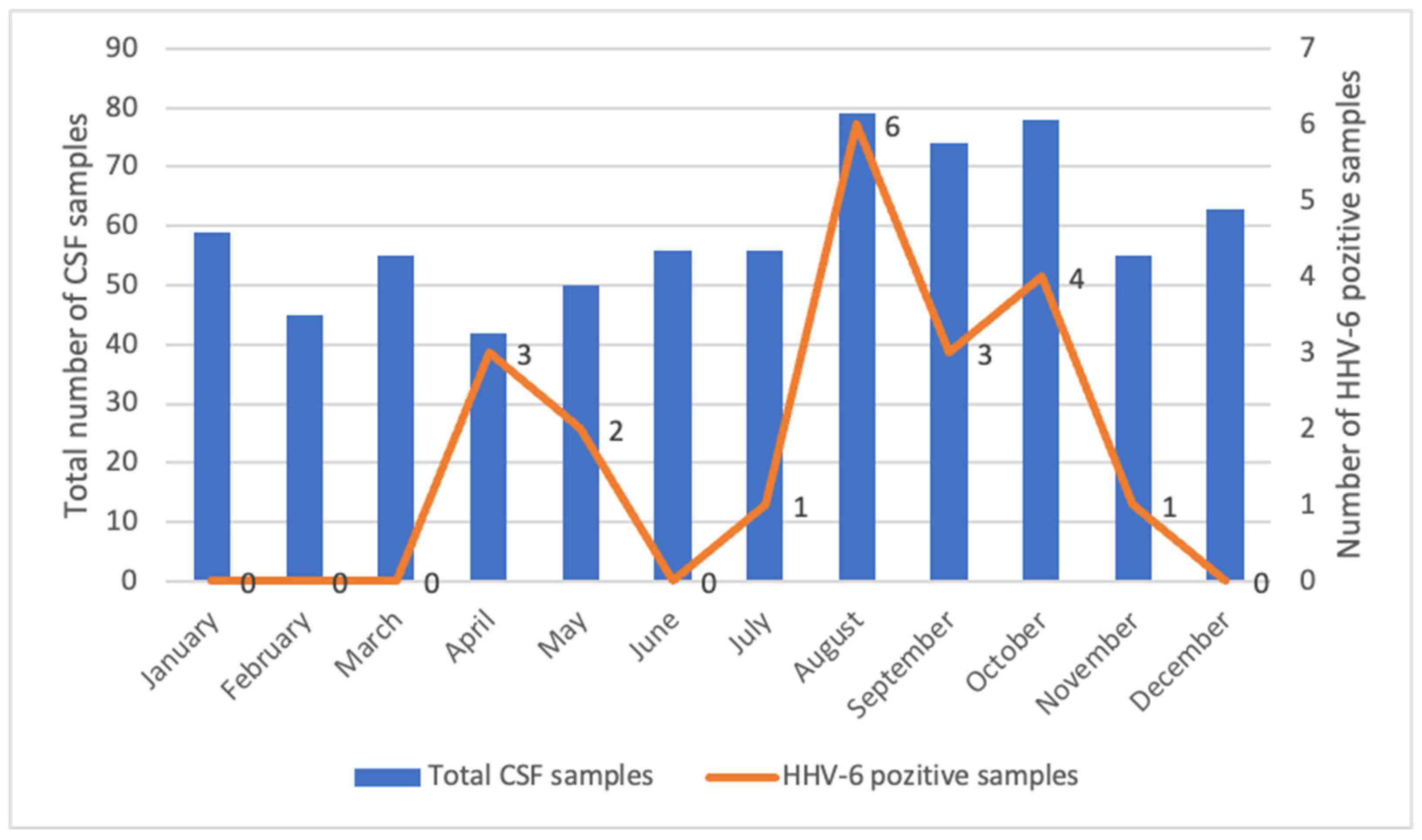
Taking into account a certain seasonality of primary HHV-6 infection, we estimated the frequency of samples sent for analysis. One-way ANOVA tests did not reveal significant differences in the number of CSF PCR tests for HHV-6 in different months and seasons of the year. Over 12 years, HHV-6 DNA was detected in 20 samples, which accounted for 2.8% of all 712 CSF specimens. The number of positive results was unequal over the duration of the study, and ranged from 0 to 4 cases per year. All positive cases of HHV-6 in the cerebrospinal fluid occurred from April to November (Figure 2).
Available for retrospective analysis were 15 medical records of patients with HHV-6 in the cerebrospinal fluid. A brief clinical and laboratory description of these cases is given in Table 1.
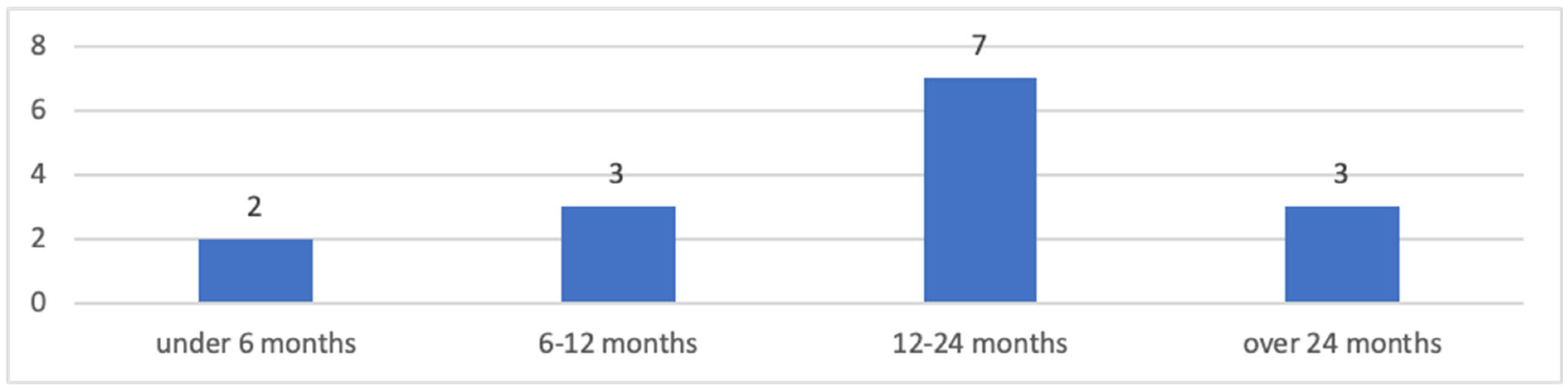
There were seven boys and eight girls. The average age was 22.3 ± 5.6 months (from 1 month to 7 years). Most of the children (70%) were aged 6–24 months, which corresponds to the peak of registration of primary HHV-6 infection. Two patients were younger than 6 months (28 days and 5 months, respectively). Only three patients were older than 2 years (Figure 3).
The anamnesis of the majority of the examined patients was not complicated. Three patients were born prematurely (35–36 weeks), but with normal weight. Two children were born via caesarean section; others were born naturally. At the time of admission, two infants were breastfed. One child, 5 months of age, underwent surgery for congenital hydronephrosis of the kidney.
Meningeal symptoms (occipital muscle rigidity, Kernig’s symptom) and/or symptoms of encephalitis (impaired consciousness, repeated convulsions, focal neurological symptoms) were recorded in all patients, which served as the indication for performing a lumbar puncture. Recurrent and/or prolonged seizures were observed in five (33%) patients.
White blood count of HHV-6 patients revealed four cases of leukopenia and four cases of leukocytosis. Seven patients had no abnormalities in the white blood count.
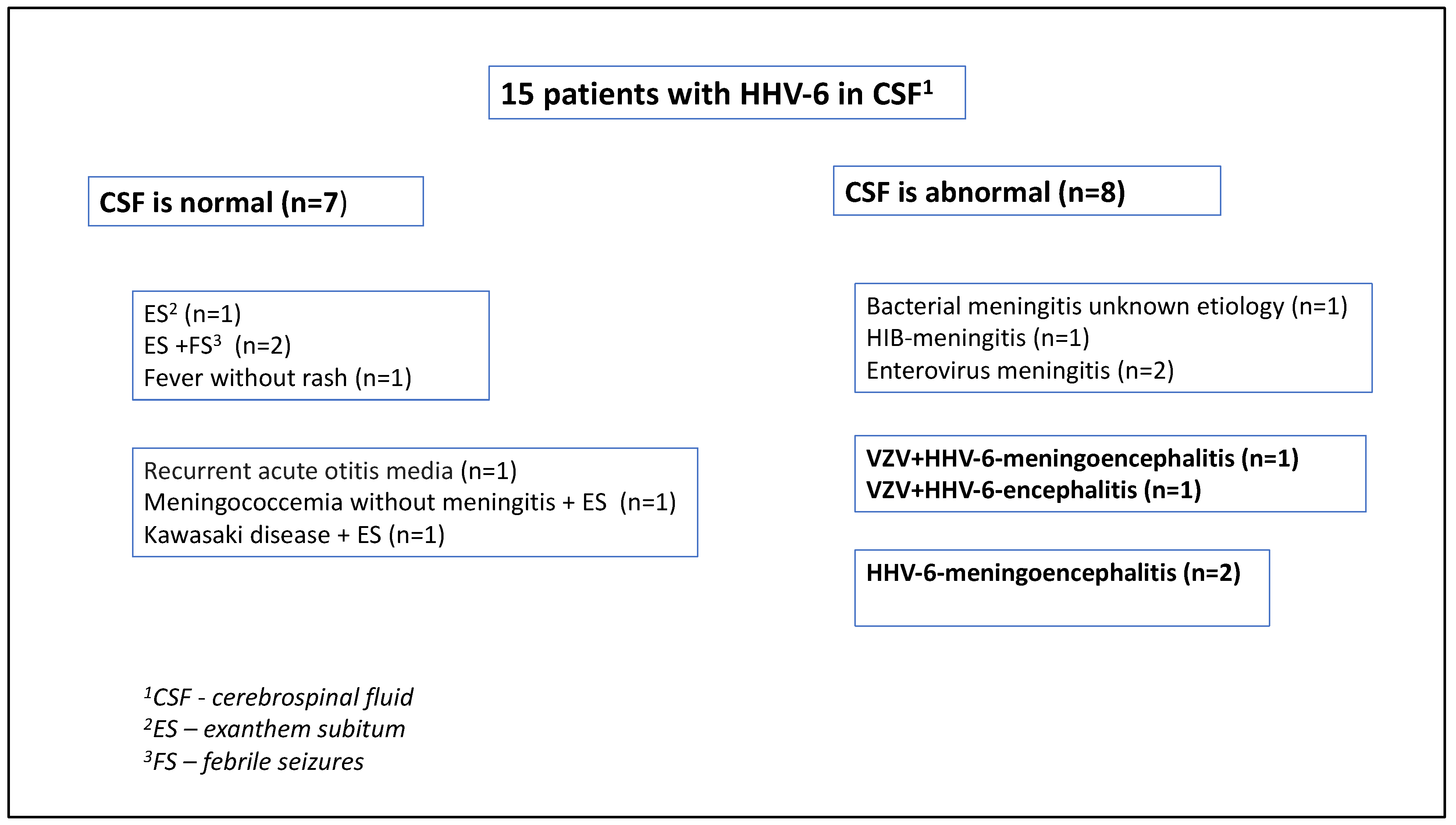
The CSF analysis demonstrated pathological changes in 8 of 15 (53%) patients (Figure 4). Two children had typical clinical and laboratory signs of bacterial meningitis (Hib and unknown etiology, respectively). Enterovirus meningitis was also confirmed in two cases. The role of HHV-6 in these patients remained unclear, given the absence of typical clinical manifestations of this infection and the impossibility of excluding ciHHV-6.
Diagnosis of HHV-6 meningoencephalitis was confirmed in four immunocompetent patients, while two children had coinfection with VZV. They were two boys and two girls, aged from 1 to 22 months, with an average age of 9.0 ± 1.9 months. Three cases occurred in the summer and one in May. All patients had fever and lethargy; three had repeated prolonged febrile convulsions; and one had hallucinations, grimaces, and hand twitching. The most serious condition was in a young patient with combined HHV-6 + VZV, who was on respiratory support for six days in the intensive care unit. None of these patients had a rash specific to exanthem subitum. All children with HHV-6 encephalitis had inflammatory changes in the CSF (Table 1). In half of the cases, HHV-6 was also detected in the blood plasma. Complete blood counts were without pathological abnormalities in all these cases. Only one five-month-old patient had IgG to HHV-6, considered to be of maternal origin. Two patients were seronegative for HHV-6 and one 1-month-old child was not tested for IgG. In summary, four patients had primary HHV-6 infection, which occurred in the form of meningoencephalitis. Etiotropic antiviral therapy was performed with acyclovir in patients with concomitant VZV infection. The average length of hospitalization in this group was 19 ± 0.7 days. All patients recovered and were discharged, but no follow-up history for isolated neurological complications was collected.
The clinical manifestations of seven patients without inflammatory changes in the CSF were considered as meningism. Five patients had a typical HHV-6 infection maculopapular rash (in two cases it debuted in the background of other diseases) and were diagnosed with exanthem subitum. One patient had HHV-6 fever without a rash. But since MRI was not performed, it is possible that there were cases of undiagnosed HHV-6 encephalitis in this group. One patient in this group had purulent otitis without clinical signs of HHV-6-infection.
4. Discussion
Primary infection caused by HHV-6 is a ubiquitous disease in children in the first three years of life. The difficulty of identifying a specific pathology caused by HHV-6 is associated with its ubiquity and lifelong persistence in the latent form; the possibility of reactivation; the possibility of a child being infected with several pathogens at the same time; and the possibility of ciHHV-6.
Despite the benign course, primary HHV-6 infection often leads to hospitalization, and CNS infection is often suspected in patients. The neurotropic properties of the virus are manifested in many patients as an increased irritability on the day preceding the rash; another typical manifestation is a febrile seizure. It is very likely that the cause of FS is the direct effect of the virus on the central nervous system. HHV-6 causes neuroinflammation, hyperexcitability of neurons, and convulsions. Convulsions by themselves increase neuroinflammation—this is how the vicious cycle completes [10].
Nevertheless, HHV-6 encephalitis extremely rarely affects immunocompetent children. Most cases occur in the first two years of life as a primary infection. It is often difficult to conclude whether HHV-6 encephalitis is a complication of ES or an independent severe form of primary infection, since it sometimes occurs without a rash [24].
PCR diagnostics expands the possibilities of etiological identification of viral encephalitis. CSF testing for HHV-6 has been routine in our hospital since 2007, and the frequency of analyses has increased from year to year. CSF samples are sent to the laboratory evenly throughout the year, but all positive HHV-6 cases were documented from April to November.
The results of our study confirm that the detection of HHV-6 DNA in the cerebrospinal fluid is rare (2.8%) and, in most cases, does not indicate brain infection.
Over 12 years, out of 712 patients at our hospital with suspicion for CNS infection, HHV-6 meningoencephalitis was confirmed only in 4 children under 2 years of age (0.66%), with 2 patients registered as having combined (HHV-6+VZV) infection. The data obtained on the incidence of the disease correspond to the results of studies from other countries [17,18]. The seasonality of the HHV-6 encephalitis manifestations was noted in our study—most of the cases occurred in the summer, although some researchers reported the diseases in the winter [16]. The course of HHV-6 encephalitis was generally benign; patients fully recovered and were discharged 2–4 weeks after admission.
Coinfection of herpesviruses and other agents has been described by a number of authors [39,40]. Our study also revealed coinfection of HHV-6 and other pathogens. In most cases of coinfection, we decided on the role of a particular pathogen in CNS infection based on the clinical course of the disease.
Due to the difficulties of diagnosing HHV-6, there are controversial data on the criteria for diagnosis, which can lead to both underdiagnosis, due to the lack of MRI data, and overdiagnosis, when the detection of HHV-6 DNA is considered as confirmation of an acute infection. Our study confirmed that in primary HHV-6 infection, there is a possibility of detecting HHV-6 DNA in the CSF in patients without signs of brain damage, which should be taken into account when making a diagnosis and choosing treatment. In addition, asymptomatic reactivation of the latent virus in intercurrent diseases is also possible. Another problem is the persistent presence of HHV-6 in the cerebrospinal fluid of patients with ciHHV-6, which takes place, according to various sources, in 0.5–1% of the world’s population [26].
Thus, it is necessary to develop clear diagnostic criteria for confirming HHV-6 encephalitis in immunocompetent children. In our opinion, the algorithm for confirming HHV-6 encephalitis is as follows. In a patient with suspected meningoencephalitis (fever, convulsions, impaired consciousness, neurological focal symptoms), perform CSF analysis. If HHV-6 is detected in the CSF, it is necessary to determine HHV-6 DNA and its amount in the blood two times in dynamics after a week and/or to study the presence of HHV-6 DNA in the nail plates or hair follicles to exclude ciHHV-6. To clarify the nature of brain damage, it is necessary to use an MRI scan, which can confirm the diagnosis of encephalitis even in the absence of pleocytosis.
The frequency, mechanisms of lesion, clinical course, and therapeutic approaches in immunocompetent children with HHV-6 encephalitis are in need of further study, especially if considering the risks of long-term neurological complications.
The limitation of our work was the lack of the possibility to perform an MRI. Also, we did not genotype HHV-6 and did not estimate the viral load of HHV-6 in the cerebrospinal fluid and blood to exclude ciHHV-6.
Author Contributions
M.A.N.: conceptualization, methodology, writing (original draft preparation, review and editing), formal analysis, visualization. D.A.L.: methodology, writing—review and editing, validation. E.U.G.: investigation, data curation, supervision. T.V.V.: investigation, resources, project administration. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and was approved by the Local Ethics Committee of Pavlov First Saint Petersburg State Medical University (Approval Code: 04/2019, Approval Date: 29 April 2019) for studies involving humans.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data available on request from the authors.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Zerr, D.M.; Meier, A.S.; Selke, S.S.; Frenkel, L.M.; Huang, M.L.; Wald, A.; Rhoads, M.P.; Nguy, L.; Bornemann, R.; Morrow, R.A.; et al. A population-based study of primary human herpesvirus 6 infection. N. Engl. J. Med. 2005, 352, 768–776. [Google Scholar] [CrossRef] [PubMed]
- Nikolsky, M.; Vyazovaya, A.; Vedernikov, V.; Narvskaya, O.; Lioznov, D.; Smirnova, N.; Polunina, A.; Burmistrova, A.; Zolotova, M.; Bio, L.A.; et al. Molecular and biological characteristics of human herpes virus type 6 in patients with different variants of the disease course. Pediatrics 2019, 98, 53–56. [Google Scholar] [CrossRef]
- Ward, K.N.; Andrews, N.J.; Verity, C.M.; Miller, E.; Ross, E.M. Human herpesviruses-6 and -7 each cause significant neurological morbidity in Britain and Ireland. Arch. Dis. Child. 2005, 90, 619–623. [Google Scholar] [CrossRef] [PubMed]
- Sloan, P.E.; Rodriguez, C.; Holtz, L.R. Viral prevalence by gestational age and season in a large neonatal cord blood cohort. J. Matern. Neonatal Med. 2021, 35, 8482–8487. [Google Scholar] [CrossRef] [PubMed]
- Mannonen, L.; Herrgård, E.; Valmari, P.; Rautiainen, P.; Uotila, K.; Aine, M.-R.; Karttunen-Lewandowski, P.; Sankala, J.; Wallden, T.; Koskiniemi, M. Primary Human Herpesvirus-6 Infection in the Central Nervous System Can Cause Severe Disease. Pediatr. Neurol. 2007, 37, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Touserkani, F.M.; Gaínza-Lein, M.; Jafarpour, S.; Brinegar, K.; Kapur, K.; Loddenkemper, T. HHV-6 and seizure: A systematic review and meta-analysis. J. Med. Virol. 2016, 89, 161–169. [Google Scholar] [CrossRef]
- Nagasawa, T.; Kimura, I.; Abe, Y.; Oka, A. HHV-6 Encephalopathy with Cluster of Convulsions during Eruptive Stage. Pediatr. Neurol. 2007, 36, 61–63. [Google Scholar] [CrossRef]
- Zerr, D.M.; Yeung, L.C.; Obrigewitch, R.M.; Huang, M.-L.; Frenkel, L.M.; Corey, L. Primary human herpesvirus-6 associated with an afebrile seizure in a 3-week-old infant. J. Med. Virol. 2002, 66, 384–387. [Google Scholar] [CrossRef]
- Bartolini, L.; Theodore, W.H.; Jacobson, S.; Gaillard, W.D. Infection with HHV-6 and its role in epilepsy. Epilepsy Res. 2019, 153, 34–39. [Google Scholar] [CrossRef]
- Komaroff, A.L.; Pellett, P.E.; Jacobson, S. Human Herpesviruses 6A and 6B in Brain Diseases: Association versus Causation. Clin. Microbiol. Rev. 2020, 34, 2–36. [Google Scholar] [CrossRef]
- Fotheringham, J.; Donati, D.; Akhyani, N.; Fogdell-Hahn, A.; Vortmeyer, A.; Heiss, J.D.; Williams, E.; Weinstein, S.; A Bruce, D.; Gaillard, W.D.; et al. Association of Human Herpesvirus-6B with Mesial Temporal Lobe Epilepsy. PLoS Med. 2007, 4, e180. [Google Scholar] [CrossRef] [PubMed]
- Romanescu, C.; Schreiner, T.G.; Mukovozov, I. The Role of Human Herpesvirus 6 Infection in Alzheimer’s Disease Pathogenicity—A Theoretical Mosaic. J. Clin. Med. 2022, 11, 3061. [Google Scholar] [CrossRef]
- Berzero, G.; Campanini, G.; Vegezzi, E.; Paoletti, M.; Pichiecchio, A.; Simoncelli, A.M.; Colombo, A.A.; Bernasconi, P.; Borsani, O.; Di Matteo, A.; et al. Human Herpesvirus 6 Encephalitis in Immunocompetent and Immunocompromised Hosts. Neurol. Neuroimmunol. Neuroinflammation 2021, 8, e942. [Google Scholar] [CrossRef]
- Eliassen, E.; Hemond, C.C.; Santoro, J.D. HHV-6-Associated Neurological Disease in Children: Epidemiologic, Clinical, Diagnostic, and Treatment Considerations. Pediatr. Neurol. 2020, 105, 10–20. [Google Scholar] [CrossRef] [PubMed]
- Raspall-Chaure, M.; Armangué, T.; Elorza, I.; Sanchez-Montanez, A.; Vicente-Rasoamalala, M.; Macaya, A. Epileptic encephalopathy after HHV6 post-transplant acute limbic encephalitis in children: Confirmation of a new epilepsy syndrome. Epilepsy Res. 2013, 105, 419–422. [Google Scholar] [CrossRef]
- Yavarian, J.; Gavvami, N.; Mamishi, S. Detection of Human Herpesvirus 6 in Cerebrospinal Fluid of Children with Possible Encephalitis. Jundishapur J. Microbiol. 2014, 7, e11821. [Google Scholar] [CrossRef]
- Yoshikawa, T.; Ohashi, M.; Miyake, F.; Fujita, A.; Usui, C.; Sugata, K.; Suga, S.; Hashimoto, S.; Asano, Y. Exanthem Subitum-Associated Encephalitis: Nationwide Survey in Japan. Pediatr. Neurol. 2009, 41, 353–358. [Google Scholar] [CrossRef] [PubMed]
- Parisi, S.G.; Basso, M.; Del Vecchio, C.; Andreis, S.; Franchin, E.; Bello, F.D.; Pagni, S.; Biasolo, M.A.; Manganelli, R.; Barzon, L.; et al. Virological testing of cerebrospinal fluid in children aged less than 14 years with a suspected central nervous system infection: A retrospective study on 304 consecutive children from January 2012 to May 2015. Eur. J. Paediatr. Neurol. 2016, 20, 588–596. [Google Scholar] [CrossRef]
- Winestone, L.E.; Punn, R.; Tamaresis, J.S.; Buckingham, J.; Pinsky, B.A.; Waggoner, J.J.; Kharbanda, S. High human herpesvirus 6 viral load in pediatric allogeneic hematopoietic stem cell transplant patients is associated with detection in end organs and high mortality. Pediatr. Transplant. 2017, 22, e13084. [Google Scholar] [CrossRef]
- Kawamura, Y.; Sugata, K.; Ihira, M.; Mihara, T.; Mutoh, T.; Asano, Y.; Yoshikawa, T. Different characteristics of human herpesvirus 6 encephalitis between primary infection and viral reactivation. J. Clin. Virol. 2011, 51, 12–19. [Google Scholar] [CrossRef]
- Fotheringham, J.; Akhyani, N.; Vortmeyer, A.; Donati, D.; Williams, E.; Oh, U.; Bishop, M.; Barrett, J.; Gea-Banacloche, J.; Jacobson, S. Detection of Active Human Herpesvirus–6 Infection in the Brain: Correlation with Polymerase Chain Reaction Detection in Cerebrospinal Fluid. J. Infect. Dis. 2007, 195, 450–454. [Google Scholar] [CrossRef] [PubMed]
- Shakhgildyan, V.I.; Yadrikhinskaya, M.S.; Domonova, E.A.; Orlovsky, A.A.; Tishkevich, O.A.; Yarovaya, E.B. Novel approaches to etiological diagnosis of central nervous system lesions in patients with HIV. Epidemiol. Infect. Dis. 2023, 13, 46–54. [Google Scholar] [CrossRef]
- Hennus, M.P.; van Montfrans, J.M.; van Vught, A.J.; Tesselaar, K.; Boelens, J.-J.; Jansen, N.J. Life-threatening human herpes virus-6 infection in early childhood: Presenting symptom of a primary immunodeficiency? Pediatr. Crit. Care Med. 2009, 10, e16–e18. [Google Scholar] [CrossRef] [PubMed]
- Ward, K.N.; Leong, H.N.; Thiruchelvam, A.D.; Atkinson, C.E.; Clark, D.A. Human Herpesvirus 6 DNA Levels in Cerebrospinal Fluid Due to Primary Infection Differ from Those Due to Chromosomal Viral Integration and Have Implications for Diagnosis of Encephalitis. J. Clin. Microbiol. 2007, 45, 1298–1304. [Google Scholar] [CrossRef] [PubMed]
- Mamishi, S.; Kamrani, L.; Mohammadpour, M.; Yavarian, J. Prevalence of HHV-6 in cerebrospinal fluid of children younger than 2 years of age with febrile convulsion. Iran. J. Microbiol. 2014, 6, 87–90. [Google Scholar]
- Pellett, P.E.; Ablashi, D.V.; Ambros, P.F.; Agut, H.; Caserta, M.T.; Descamps, V.; Flamand, L.; Gautheret-Dejean, A.; Hall, C.B.; Kamble, R.T.; et al. Chromosomally integrated human herpesvirus 6: Questions and answers. Rev. Med. Virol. 2011, 22, 144–155. [Google Scholar] [CrossRef]
- Esposito, L.; Drexler, J.F.; Braganza, O.; Agut, H.; Caserta, M.T.; Descamps, V.; Flamand, L.; Gautheret-Dejean, A.; Hall, C.B.; Kamble, R.T.; et al. Large-scale analysis of viral nucleic acid spectrum in temporal lobe epilepsy biopsies. Epilepsia 2015, 56, 234–243. [Google Scholar] [CrossRef]
- Kawamura, Y.; Nakai, H.; Sugata, K.; Asano, Y.; Yoshikawa, T. Serum biomarker kinetics with three different courses of HHV-6B encephalitis. Brain Dev. 2013, 35, 590–595. [Google Scholar] [CrossRef]
- Matsumoto, H.; Hatanaka, D.; Ogura, Y.; Chida, A.; Nakamura, Y.; Nonoyama, S. Severe human herpesvirus 6-associated encephalopathy in three children: Analysis of cytokine profiles and the carnitine palmitoyltransferase 2 gene. Pediatr. Infect. Dis. J. 2011, 30, 999–1001. [Google Scholar] [CrossRef]
- Tadokoro, R.; Okumura, A.; Nakazawa, T.; Hara, S.; Yamakawa, Y.; Kamata, A.; Kinoshita, K.; Obinata, K.; Shimizu, T. Acute encephalopathy with biphasic seizures and late reduced diffusion associated with hemophagocytic syndrome. Brain Dev. 2010, 32, 477–481. [Google Scholar] [CrossRef]
- Akasaka, M.; Sasaki, M.; Ehara, S.; Kamei, A.; Chida, S. Transient decrease in cerebral white matter diffusivity on MR imaging in human herpes virus-6 encephalopathy. Brain Dev. 2005, 27, 30–33. [Google Scholar] [CrossRef]
- Sadighi, Z.; Sabin, N.D.; Hayden, R.; Stewart, E.; Pillai, A. Diagnostic Clues to Human Herpesvirus 6 Encephalitis and Wernicke Encephalopathy After Pediatric Hematopoietic Cell Transplantation. J. Child Neurol. 2015, 30, 1307–1314. [Google Scholar] [CrossRef] [PubMed]
- Olli-Lähdesmäki, T.; Haataja, L.; Parkkola, R.; Waris, M.; Bleyzac, N.; Ruuskanen, O. High-Dose Ganciclovir in HHV-6 Encephalitis of an Immunocompetent Child. Pediatr. Neurol. 2010, 43, 53–56. [Google Scholar] [CrossRef] [PubMed]
- Ogata, M.; Kikuchi, H.; Satou, T.; Kawano, R.; Ikewaki, J.; Kohno, K.; Kashima, K.; Ohtsuka, E.; Kadota, J. Human Herpesvirus 6 DNA in Plasma after Allogeneic Stem Cell Transplantation: Incidence and Clinical Significance. J. Infect. Dis. 2006, 193, 68–79. [Google Scholar] [CrossRef] [PubMed]
- Ohsaka, M.; Houkin, K.; Takigami, M.; Koyanagi, I. Acute Necrotizing Encephalopathy Associated with Human Herpesvirus-6 Infection. Pediatr. Neurol. 2006, 34, 160–163. [Google Scholar] [CrossRef]
- Hoshino, A.; Saitoh, M.; Oka, A.; Okumura, A.; Kubota, M.; Saito, Y.; Takanashi, J.-I.; Hirose, S.; Yamagata, T.; Yamanouchi, H.; et al. Epidemiology of acute encephalopathy in Japan, with emphasis on the association of viruses and syndromes. Brain Dev. 2012, 34, 337–343. [Google Scholar] [CrossRef]
- Spatola, M.; Petit-Pedrol, M.; Simabukuro, M.M.; Armangue, T.; Castro, F.J.; Artigues, M.I.B.; Benique, M.R.J.; Benson, L.; Gorman, M.; Felipe, A.; et al. Investigations in GABAA receptor antibody-associated encephalitis. Neurology 2017, 88, 1012–1020. [Google Scholar] [CrossRef]
- Liu, D.; Wang, X.; Wang, Y.; Wang, P.; Fan, D.; Chen, S.; Guan, Y.; Li, T.; An, J.; Luan, G. Detection of EBV and HHV6 in the Brain Tissue of Patients with Rasmussen’s Encephalitis. Virol. Sin. 2018, 33, 402–409. [Google Scholar] [CrossRef]
- Yamamoto, T.; Nakamura, Y. A single tube PCR assay for simultaneous amplification of HSV-1/-2, VZV, CMV, HHV-6A/-6B, and EBV DNAs in cerebrospinal fluid from patients with virus-related neurological diseases. J. Neurovirology 2000, 6, 410–417. [Google Scholar] [CrossRef]
- Calvario, A.; Bozzi, A.; Scarasciulli, M.; Ventola, C.; Seccia, R.; Stomati, D.; Brancasi, B. Herpes Consensus PCR test: A useful diagnostic approach to the screening of viral diseases of the central nervous system. J. Clin. Virol. 2002, 25, 71–78. [Google Scholar] [CrossRef]
Figure 1.
Number of CSF examinations for HHV-6 in different years.

Figure 2.
CSF testing for HHV-6 depending on the month of the year.

Figure 3.
Distribution of patients with detected HHV-6 in the cerebrospinal fluid by age.

Figure 4.
Diagnoses of patients with HHV-6 in CSF.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
The summary data for patients with HHV-6 in the CSF.
| Age, Months | Gender | Symptoms | CSF | Plasma | WBC | Diagnosis | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| HHV-6 | Cell Count (Cell/3 Mics) | Protein (g/L) | Glucose (mmol/L) | Another Agent in CSF | HHV-6 | Another Agent | |||||
| 23 | m | Fever, lethargy, rash | Positive | 3 | 0.08 | 4.2 | Negative | Not tested | Negative | Leucopenia | ES ** |
| 14 | m | Fever, repeated seizures, rash | Positive | 1 | 0.05 | 3.8 | Negative | Not tested | Negative | Normal | ES + FS *** |
| 26 | f | Fever, repeated seizures, headache, vomiting, nuchal rigidity, Kernig’s sign, rash | Positive | 3 | 0.2 | 3.3 | Negative | Positive | Negative | Leucopenia | ES + FS |
| 7 | m | Fever, refusal to eat, irritability, mild transaminitis (ALT = 370) | Positive | 6 | 0.2 | 3.0 | Negative | Positive | Negative | Leucopenia | Fever without rash |
| 15 | f | Repeated fever, drowsiness, rash | Positive | 18 (PMN * 5) | 0.19 | 3.5 | Negative | Not tested | Meningococcus B | Leucopenia | Meningococcal B inf. + ES |
| 17 | f | Prolonged fever, drowsiness, rash | Positive | 3 | 0.12 | 3.8 | Negative | Negative | Negative | Leukocytosis, lymphocytosis | Kawasaki disease + ES |
| 5 | m | Fever, prolonged repeated seizures, lethargy, unconsciousness | Positive | 176 (PMN 90) | 0.22 | 4.9 | Negative | Negative | Bordetella pertussis | Leukocytosis, lymphocytosis | HHV-6-meningoencephalitis + Pertussis |
| 8 | f | Fever, repeated seizures, lethargy | Positive | 16 (PMN 10) | 1.2 | 2.9 | Negative | Positive | Negative | Normal | HHV-6-meningoencephalitis |
| 22 | f | Fever, lethargy, vomiting, hallucinations, grimaces, hand twitching, rash | Positive | 590 (PMN 550) | 0.26 | 2.6 | VZV | Negative | VZV | Normal | HHV-6 + VZV-meningoencephalitis |
| 1 | m | Fever, prolonged repeated seizures, lethargy, general cerebral symptoms, rash | Positive | 3 | 0.44 | 1 | Negative | Positive | VZV | Normal | HHV-6 + VZV-encephalitis |
| 19 | m | Fever, vomiting, nuchal rigidity, Kernig’s sign | Positive | 2780 (PMN 95%) | 0.35 | 2.1 | Negative | Not tested | Negative | Normal | Bacterial meningitis unknown etiology |
| 12 | f | Fever, vomiting, nuchal rigidity, Kernig’s sign | Positive | 23,296 (PMN 98%) | 1.4 | 0.5 | Hib | Not tested | Negative | Leukocytosis, neutrophilia | Hib-meningitis |
| 92 | m | Fever, photophobia, Kernig’s sign | Positive | 870 (PMN 263) | 0.3 | 5.3 | Enterovirus | Not tested | Enterovirus | Normal | Enterovirus meningitis |
| 62 | f | Fever, headache, vomiting, nuchal rigidity | Positive | 542 (PMN 15) | 0.44 | 2.5 | Enterovirus | Negative | Negative | Normal | Enterovirus meningitis |
| 11 | f | Fever, nuchal rigidity, lethargy, rash | Positive | 80 (PMN 61) | 1.6 | 4.1 | Pneumococcus | Not tested | Negative | Leukocytosis, neutrophilia | Recurrent acute otitis media |
* PMN—polymorphonuclear neutrophil. ** ES—exanthem subitem. *** FS—febrile seizures.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Nikolskiy, M.A.; Lioznov, D.A.; Gorelik, E.U.; Vishnevskaya, T.V. HHV-6 in Cerebrospinal Fluid in Immunocompetent Children. BioMed 2023, 3, 420-430. https://0-doi-org.brum.beds.ac.uk/10.3390/biomed3030034
AMA Style
Nikolskiy MA, Lioznov DA, Gorelik EU, Vishnevskaya TV. HHV-6 in Cerebrospinal Fluid in Immunocompetent Children. BioMed. 2023; 3(3):420-430. https://0-doi-org.brum.beds.ac.uk/10.3390/biomed3030034
Chicago/Turabian StyleNikolskiy, Mikhail A., Dmitriy A. Lioznov, Evgeniy U. Gorelik, and Tatyana V. Vishnevskaya. 2023. "HHV-6 in Cerebrospinal Fluid in Immunocompetent Children" BioMed 3, no. 3: 420-430. https://0-doi-org.brum.beds.ac.uk/10.3390/biomed3030034