

Oral Diseases and Adverse Pregnancy Outcomes in Sub-Saharan Africa: A Scoping Review

 , , , , , ,
, , , , , ,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Identifying Research Questions
2.2. Eligibility Criteria
2.3. Search Strategy
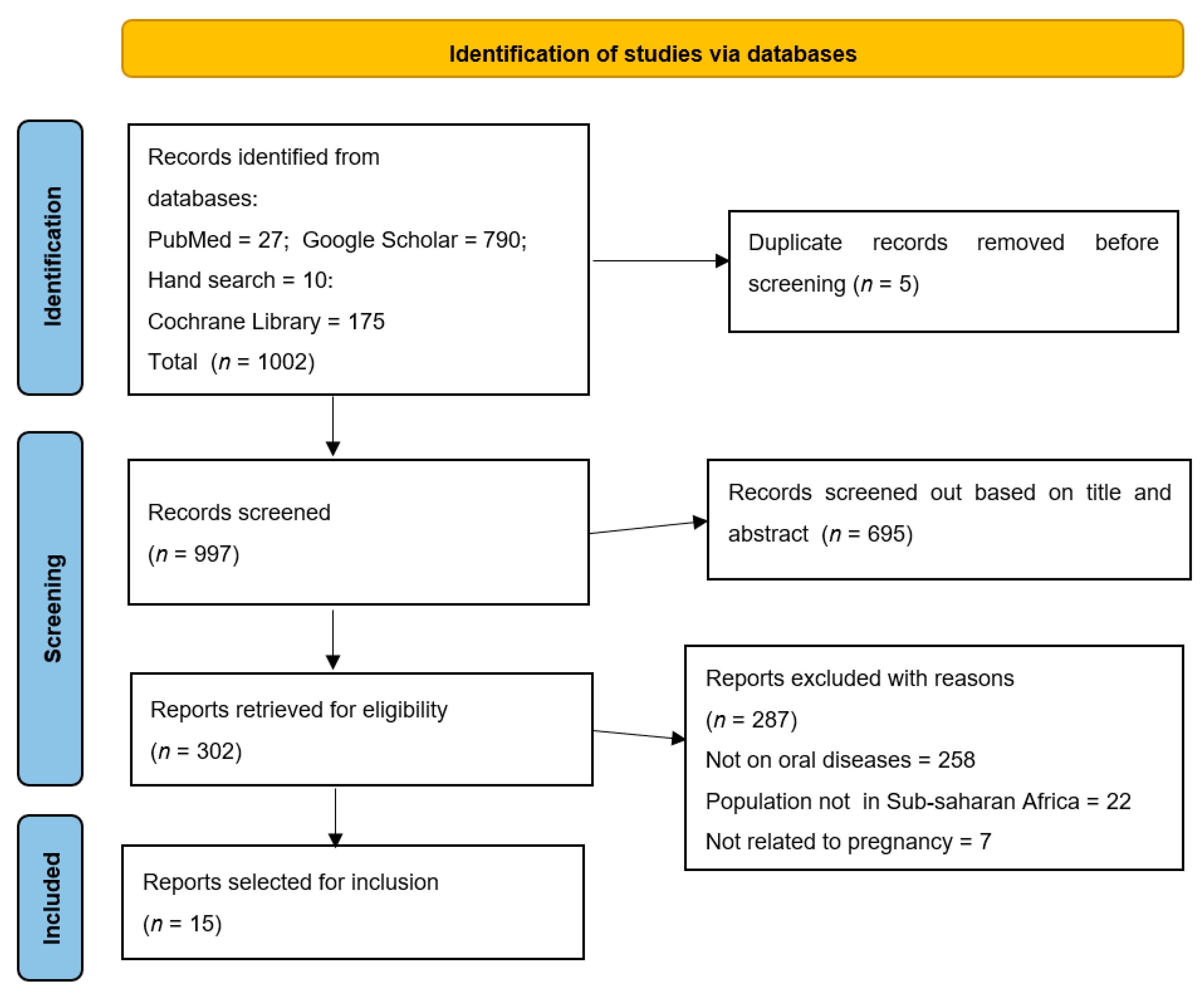
2.4. Study Selection
2.5. Data-Charting Process
2.6. Data Analysis
3. Results
3.1. Study Characteristics
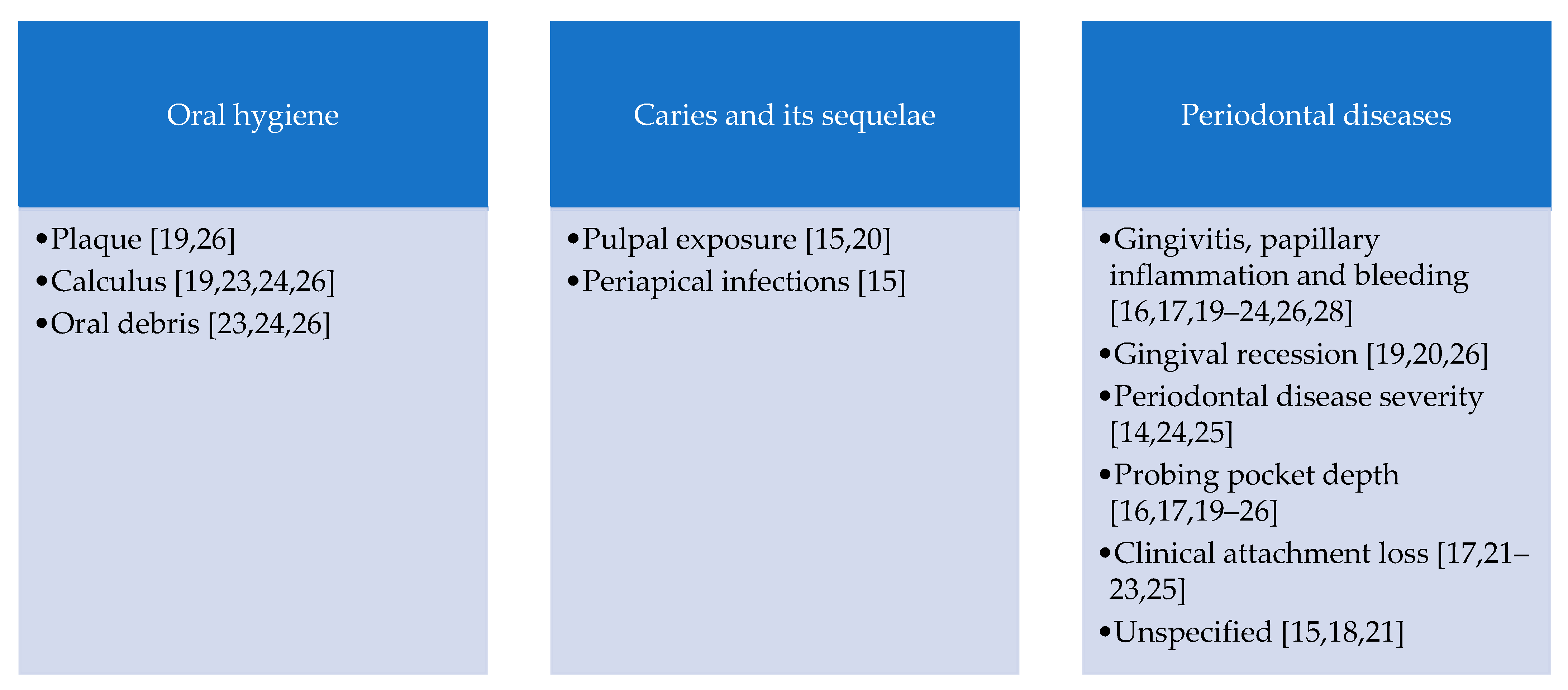
3.2. Oral Disease Conditions Assessed for the Association with Adverse Pregnancy Events
3.3. Indices Used to Measure Oral Disease Status
3.4. Adverse Pregnancy Events Observed
3.5. Links between Oral Disease Status and Child-Related Pregnancy Events
3.6. Links between Oral Disease Status and Maternal-Related Pregnancy Events
3.7. The Effect of Oral Health Interventions on Adverse Pregnancy Events
3.8. Point-of-Care Diagnostic Measure
3.9. Gaps in Knowledge on the Link between Oral Disease Status and Adverse Pregnancy Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Search Strategy for PubMed
| SEARCH STRATEGY | |||
| #1 | “oral health”[MeSH Terms] OR “dental clinics”[MeSH Terms] OR “dental health surveys”[MeSH Terms] OR “diagnosis, oral”[MeSH Terms] OR “mouth diseases”[MeSH Terms] OR “mouth rehabilitation”[MeSH Terms] | 255,419 | |
| #2 | “periodontitis”[MeSH Terms] OR “chronic periodontitis”[MeSH Terms] OR “aggressive periodontitis”[MeSH Terms] OR “periapical periodontitis”[MeSH Terms] OR “periapical abscess”[MeSH Terms] OR “periapical granuloma”[MeSH Terms] OR “aggressive periodontitis”[MeSH Terms] | 27,217 | |
| #3 | “gingivitis”[MeSH Terms] OR “gingivitis, necrotizing ulcerative”[MeSH Terms] OR “gingival diseases”[MeSH Terms] OR “granuloma, giant cell”[MeSH Terms] OR “gingival neoplasms”[MeSH Terms] | 17,213 | |
| #4 | “dental caries”[MeSH Terms] OR “dental caries”[MeSH Terms] OR “dental caries”[MeSH Terms] OR “dental caries”[MeSH Terms] OR “dental caries”[MeSH Terms] OR “dental caries”[MeSH Terms] OR “dental caries”[MeSH Terms] OR “dental caries”[MeSH Terms] OR “dental caries”[MeSH Terms] OR “dental caries”[MeSH Terms] OR “dental caries”[MeSH Terms] OR “dental caries”[MeSH Terms] | 29,789 | |
| #5 | “xerostomia”[MeSH Terms] OR “xerostomia”[MeSH Terms] OR “xerostomia”[MeSH Terms] OR “xerostomia”[MeSH Terms] OR “xerostomia”[MeSH Terms] | 15,069 | |
| #6 | #1 OR #2 OR #3 OR #4 OR #5 | (((((((((oral health[MeSH Terms]) OR (dental clinics[MeSH Terms])) OR (Dental health surveys[MeSH Terms])) OR (Diagnosis, Oral[MeSH Terms])) OR (Mouth diseases[MeSH Terms])) OR (Mouth rehabilitation[MeSH Terms])) OR (((((((Periodontitis[MeSH Terms]) OR (Chronic periodontitis[MeSH Terms])) OR (Aggressive periodontitis[MeSH Terms])) OR (Periapical periodontitis[MeSH Terms])) OR (Periapical abscess[MeSH Terms])) OR (Periapical granuloma[MeSH Terms])) OR (Periodontitis, aggressive[MeSH Terms]))) OR (((((Gingivitis[MeSH Terms]) OR (Gingivitis, necrotizing ulcerative[MeSH Terms])) OR (Gingival diseases[MeSH Terms])) OR (Granuloma, giant cell[MeSH Terms])) OR (Gingival neoplasms[MeSH Terms]))) OR ((((((((((((Caries, dental[MeSH Terms]) OR (Dental cavity[MeSH Terms])) OR (Dental decay[MeSH Terms])) OR (Dental cavities[MeSH Terms])) OR (Cavities, dental[MeSH Terms])) OR (Cavity, dental[MeSH Terms])) OR (Carious lesions[MeSH Terms])) OR (Carious lesion[MeSH Terms])) OR (Lesion, carious[MeSH Terms])) OR (Lesions, carious[MeSH Terms])) OR (Decay, dental[MeSH Terms])) OR (Dental white spot[MeSH Terms]))) OR (((((Xerostomia[MeSH Terms]) OR (Hyposalivation[MeSH Terms])) OR (Hyposalivations[MeSH Terms])) OR (Mouth dryness[MeSH Terms])) OR (Dryness, mouth[MeSH Terms])) | 272,124 |
| #7 | “pregnancy outcome”[MeSH Terms] OR “pregnancy outcome”[MeSH Terms] OR “pregnancy outcome”[MeSH Terms] OR “pregnancy complications”[MeSH Terms] OR “abortion, induced”[MeSH Terms] OR “live birth”[MeSH Terms] OR “stillbirth”[MeSH Terms] OR “fetal death”[MeSH Terms] | 359,101 | |
| #8 | “pre eclampsia”[MeSH Terms] OR “pre eclampsia”[MeSH Terms] OR “pre eclampsia”[MeSH Terms] OR “pre eclampsia”[MeSH Terms] OR “pre eclampsia”[MeSH Terms] | 24,824 | |
| #9 | “premature birth”[MeSH Terms] OR “premature birth”[MeSH Terms] OR “premature birth”[MeSH Terms] OR “premature birth”[MeSH Terms] OR “premature birth”[MeSH Terms] OR “premature birth”[MeSH Terms] | 20,123 | |
| #10 | “infant, premature”[MeSH Terms] OR “obstetric labor, premature”[MeSH Terms] OR ((“obstetric”[All Fields] OR “obstetrically”[All Fields] OR “obstetrics”[MeSH Terms] OR “obstetrics”[All Fields] OR “obstetrical”[All Fields]) AND “obstetric labor, premature”[MeSH Terms]) OR “infant, extremely premature”[MeSH Terms] | 74,368 | |
| #11 | #7 OR #8 OR #9 OR #10 | “pregnancy outcome”[MeSH Terms] OR “pregnancy outcome”[MeSH Terms] OR “pregnancy outcome”[MeSH Terms] OR “pregnancy complications”[MeSH Terms] OR “abortion, induced”[MeSH Terms] OR “live birth”[MeSH Terms] OR “stillbirth”[MeSH Terms] OR “fetal death”[MeSH Terms] OR (“pre eclampsia”[MeSH Terms] OR “pre eclampsia”[MeSH Terms] OR “pre eclampsia”[MeSH Terms] OR “pre eclampsia”[MeSH Terms] OR “pre eclampsia”[MeSH Terms]) OR (“premature birth”[MeSH Terms] OR “premature birth”[MeSH Terms] OR “premature birth”[MeSH Terms] OR “premature birth”[MeSH Terms] OR “premature birth”[MeSH Terms] OR “premature birth”[MeSH Terms]) OR (“infant, premature”[MeSH Terms] OR “obstetric labor, premature”[MeSH Terms] OR ((“obstetric”[All Fields] OR “obstetrically”[All Fields] OR “obstetrics”[MeSH Terms] OR “obstetrics”[All Fields] OR “obstetrical”[All Fields]) AND “obstetric labor, premature”[MeSH Terms]) OR “infant, extremely premature”[MeSH Terms]) | 400,414 |
| #12 | (“BENIN”[Title/Abstract] OR “BOTSWANA”[Title/Abstract] OR “burkina faso”[Title/Abstract] OR “BURUNDI”[Title/Abstract] OR “cabo verde”[Title/Abstract] OR “CAMEROON”[Title/Abstract] OR “central african republic”[Title/Abstract] OR “CHAD”[Title/Abstract] OR “COMOROS”[Title/Abstract] OR ((“congo”[MeSH Terms] OR “congo”[All Fields]) AND “dem rep”[Title/Abstract]) OR ((“congo”[MeSH Terms] OR “congo”[All Fields]) AND “rep”[Title/Abstract]) OR “cote d ivoire”[Title/Abstract] OR “equatorial guinea”[Title/Abstract] OR “ERITREA”[Title/Abstract] OR “ESWATINI”[Title/Abstract] OR “ETHIOPIA”[Title/Abstract] OR “GABON”[Title/Abstract] OR “GAMBIA”[Title/Abstract] OR “GHANA”[Title/Abstract] OR “GUINEA”[Title/Abstract] OR “GUINEA-BISSAU”[Title/Abstract] OR “KENYA”[Title/Abstract] OR “LESOTHO”[Title/Abstract] OR “LIBERIA”[Title/Abstract] OR “MADAGASCAR”[Title/Abstract] OR “MALAWI”[Title/Abstract] OR “MALI”[Title/Abstract] OR “MAURITANIA”[Title/Abstract] OR “MAURITIUS”[Title/Abstract] OR “MOZAMBIQUE”[Title/Abstract] OR “NAMIBIA”[Title/Abstract] OR “NIGER”[Title/Abstract] OR “NIGERIA”[Title/Abstract] OR “RWANDA”[Title/Abstract] OR (“sao tome”[Title/Abstract] AND “PRINCIPE”[Title/Abstract]) OR “SENEGAL”[Title/Abstract] OR “SEYCHELLES”[Title/Abstract] OR “sierra leone”[Title/Abstract] OR “SOMALIA”[Title/Abstract] OR “south africa”[Title/Abstract] OR “south sudan”[Title/Abstract] OR “SUDAN”[Title/Abstract] OR “TANZANIA”[Title/Abstract] OR “TOGO”[Title/Abstract] OR “UGANDA”[Title/Abstract] OR “ZAMBIA”[Title/Abstract] OR “ZIMBABWE”[Title/Abstract] | 283,964 | |
| #13 | #6 AND #11 AND #12 | ((“oral health”[MeSH Terms] OR “dental clinics”[MeSH Terms] OR “dental health surveys”[MeSH Terms] OR “diagnosis, oral”[MeSH Terms] OR “mouth diseases”[MeSH Terms] OR “mouth rehabilitation”[MeSH Terms] OR (“periodontitis”[MeSH Terms] OR “chronic periodontitis”[MeSH Terms] OR “aggressive periodontitis”[MeSH Terms] OR “periapical periodontitis”[MeSH Terms] OR “periapical abscess”[MeSH Terms] OR “periapical granuloma”[MeSH Terms] OR “aggressive periodontitis”[MeSH Terms]) OR (“gingivitis”[MeSH Terms] OR “gingivitis, necrotizing ulcerative”[MeSH Terms] OR “gingival diseases”[MeSH Terms] OR “granuloma, giant cell”[MeSH Terms] OR “gingival neoplasms”[MeSH Terms]) OR (“dental caries”[MeSH Terms] OR “dental caries”[MeSH Terms] OR “dental caries”[MeSH Terms] OR “dental caries”[MeSH Terms] OR “dental caries”[MeSH Terms] OR “dental caries”[MeSH Terms] OR “dental caries”[MeSH Terms] OR “dental caries”[MeSH Terms] OR “dental caries”[MeSH Terms] OR “dental caries”[MeSH Terms] OR “dental caries”[MeSH Terms] OR “dental caries”[MeSH Terms]) OR (“xerostomia”[MeSH Terms] OR “xerostomia”[MeSH Terms] OR “xerostomia”[MeSH Terms] OR “xerostomia”[MeSH Terms] OR “xerostomia”[MeSH Terms])) AND (“pregnancy outcome”[MeSH Terms] OR “pregnancy outcome”[MeSH Terms] OR “pregnancy outcome”[MeSH Terms] OR “pregnancy complications”[MeSH Terms] OR “abortion, induced”[MeSH Terms] OR “live birth”[MeSH Terms] OR “stillbirth”[MeSH Terms] OR “fetal death”[MeSH Terms] OR (“pre eclampsia”[MeSH Terms] OR “pre eclampsia”[MeSH Terms] OR “pre eclampsia”[MeSH Terms] OR “pre eclampsia”[MeSH Terms] OR “pre eclampsia”[MeSH Terms]) OR (“premature birth”[MeSH Terms] OR “premature birth”[MeSH Terms] OR “premature birth”[MeSH Terms] OR “premature birth”[MeSH Terms] OR “premature birth”[MeSH Terms] OR “premature birth”[MeSH Terms]) OR (“infant, premature”[MeSH Terms] OR “obstetric labor, premature”[MeSH Terms] OR ((“obstetric”[All Fields] OR “obstetrically”[All Fields] OR “obstetrics”[MeSH Terms] OR “obstetrics”[All Fields] OR “obstetrical”[All Fields]) AND “obstetric labor, premature”[MeSH Terms]) OR “infant, extremely premature”[MeSH Terms])) AND 1990/01/01:2022/12/31[Date—Publication] AND ((“BENIN”[Title/Abstract] OR “BOTSWANA”[Title/Abstract] OR “burkina faso”[Title/Abstract] OR “BURUNDI”[Title/Abstract] OR “cabo verde”[Title/Abstract] OR “CAMEROON”[Title/Abstract] OR “central african republic”[Title/Abstract] OR “CHAD”[Title/Abstract] OR “COMOROS”[Title/Abstract] OR ((“congo”[MeSH Terms] OR “congo”[All Fields]) AND “dem rep”[Title/Abstract]) OR ((“congo”[MeSH Terms] OR “congo”[All Fields]) AND “rep”[Title/Abstract]) OR “cote d ivoire”[Title/Abstract] OR “equatorial guinea”[Title/Abstract] OR “ERITREA”[Title/Abstract] OR “ESWATINI”[Title/Abstract] OR “ETHIOPIA”[Title/Abstract] OR “GABON”[Title/Abstract] OR “GAMBIA”[Title/Abstract] OR “GHANA”[Title/Abstract] OR “GUINEA”[Title/Abstract] OR “GUINEA-BISSAU”[Title/Abstract] OR “KENYA”[Title/Abstract] OR “LESOTHO”[Title/Abstract] OR “LIBERIA”[Title/Abstract] OR “MADAGASCAR”[Title/Abstract] OR “MALAWI”[Title/Abstract] OR “MALI”[Title/Abstract] OR “MAURITANIA”[Title/Abstract] OR “MAURITIUS”[Title/Abstract] OR “MOZAMBIQUE”[Title/Abstract] OR “NAMIBIA”[Title/Abstract] OR “NIGER”[Title/Abstract] OR “NIGERIA”[Title/Abstract] OR “RWANDA”[Title/Abstract] OR (“sao tome”[Title/Abstract] AND “PRINCIPE”[Title/Abstract]) OR “SENEGAL”[Title/Abstract] OR “SEYCHELLES”[Title/Abstract] OR “sierra leone”[Title/Abstract] OR “SOMALIA”[Title/Abstract] OR “south africa”[Title/Abstract] OR “south sudan”[Title/Abstract] OR “SUDAN”[Title/Abstract] OR “TANZANIA”[Title/Abstract] OR “TOGO”[Title/Abstract] OR “UGANDA”[Title/Abstract] OR “ZAMBIA”[Title/Abstract] OR “ZIMBABWE”[Title/Abstract]) AND 1990/01/01:2022/12/31[Date—Publication] AND 1990/01/01:2022/12/31[Date—Publication])) AND (1990/1/1:2022/12/31[pdat]) | 27 |
Search Strategy for Cochrane
References
- American Dental Association. Council on Access, Prevention and Interprofessional Relations; American Dental Association: Niagara Falls, NY, USA, 2006. [Google Scholar]
- Hess, R.F.; Gililland, C.S.; Dembéle, J. Prevalence and predictors of periodontal disease among pregnant women in Mali, West Africa. Ann. Med. Health Sci. Res. 2017, 7, 263–270. [Google Scholar]
- Corbella, S.; Taschieri, S.; Del Fabbro, M.; Francetti, L.; Weinstein, R.; Ferrazi, E. Adverse pregnancy outcomes and periodontitis: A systematic review and meta-analysis exploring potential association. Quintessence Int. 2016, 47, 193–204. [Google Scholar] [PubMed]
- Yenen, Z.; Ataçag, T. Oral care in pregnancy. J. Tur. Ger. Gynecol. Assoc. 2019, 20, 264–268. [Google Scholar] [CrossRef] [PubMed]
- Tadese, M.; Dagne, K.; Wubetu, A.D.; Abeway, S.; Bekele, A.; Misganaw Kebede, W.; Baye Mulu, G. Assessment of the adverse pregnancy outcomes and its associated factors among deliveries at Debre Berhan Comprehensive Specialized Hospital, Northeast Ethiopia. PLoS ONE 2022, 17, e0271287. [Google Scholar] [CrossRef] [PubMed]
- Cho, G.J.; Kim, S.; Lee, H.C.; Kim, H.Y.; Lee, K.-M.; Han, S.W.; Oh, M.J. Association between dental caries and adverse pregnancy outcomes. Sci. Rep. 2020, 10, 5309. [Google Scholar] [CrossRef] [PubMed]
- Heimonen, A.; Rintamäki, H.; Furuholm, J.; Janket, S.-J.; Kaaja, R.; Meurman, J.H. Postpartum oral health parameters in women with preterm birth. Acta Odontol. Scand. 2008, 6, 334–341. [Google Scholar] [CrossRef] [PubMed]
- Teshome, A.; Yitayeh, A. Relationship between periodontal disease and preterm low birth weight: Systematic review. Pan Afr. Med. J. 2016, 24, 215. [Google Scholar] [CrossRef] [PubMed]
- Oleribe, O.O.; Momoh, J.; Uzochukwu, B.S.C.; Mbofana, F.; Adebiyi, A.; Barbera, T.; Williams, R.; Taylor-Robinson, S.D. Identifying Key Challenges Facing Healthcare Systems in Africa and Potential Solutions. Int. J. Gen. Med. 2019, 12, 395–403. [Google Scholar] [CrossRef]
- Al Agili, D.E.; Khalaf, Z.I. The role of oral and prenatal healthcare providers in the promotion of oral health for pregnant women. BMC Pregnancy Childbirth 2023, 313, 23. [Google Scholar] [CrossRef]
- Tamirat, K.S.; Sisay, M.M.; Tesema, G.A.; Tessema, Z.T. Determinants of adverse birth outcome in Sub-Saharan Africa: Analysis of recent demographic and health surveys. BMC Public Health 2021, 21, 1092. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Int. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Turton, M.S.; Henkel, R.R.; Africa, C.W.J. A Simple Point of Care Test Can Indicate the Need for Periodontal Therapy to Reduce the Risk for Adverse Pregnancy Outcomes in Mothers Attending Antenatal Clinics. Biomarkers 2017, 22, 740–746. [Google Scholar] [CrossRef] [PubMed]
- Harjunmaa, U.; Järnstedt, J.; Alho, L.; Dewey, K.G.; Cheung, Y.B.; Deitchler, M.; Ashorn, U.; Maleta, K.; Klein, N.J.; Ashorn, P. Association between Maternal Dental Periapical Infections and Pregnancy Outcomes: Results from a Cross-Sectional Study in Malawi. Trop. Med. Intern. Health 2015, 20, 1549–1558. [Google Scholar] [CrossRef] [PubMed]
- Gesase, N.; Miranda-Rius, J.; Brunet-Llobet, L.; Lahor-Soler, E.; Mahande, M.J.; Masenga, G. The Association between Periodontal Disease and Adverse Pregnancy Outcomes in Northern Tanzania: A Cross-Sectional Study. Afr. Health Sci. 2018, 18, 601–611. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pmc/articles/PMC6307003/ (accessed on 17 December 2023). [CrossRef] [PubMed]
- Turton, M.; Africa, C.W.J. Further Evidence for Periodontal Disease as a Risk Indicator for Adverse Pregnancy Outcomes. Int. Dent. J. 2017, 67, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Miranda-Rius, J.; Brunet-Llobet, L.; Blanc, V.; Álvarez, G.; Moncunill-Mira, J.; Mashala, E.I.; Kasebele, Y.; Masenga, G.; Nadal, A.; León, R. Microbial Profile of Placentas from Tanzanian Mothers with Adverse Pregnancy Outcomes and Periodontitis. Oral Dis. 2021, 29, 772–785. [Google Scholar] [CrossRef] [PubMed]
- Muwazi, L.; Rwenyonyi, C.M.; Nkamba, M.; Kutesa, A.; Kagawa, M.; Mugyenyi, G.; Kwizera, G.; Okullo, I. Periodontal Conditions, Low Birth Weight and Preterm Birth among Postpartum Mothers in Two Tertiary Health Facilities in Uganda. BMC Oral Health 2014, 14, 1. [Google Scholar] [CrossRef]
- Mumghamba, E.G.S.; Manji, K.P. Maternal Oral Health Status and Preterm Low Birth Weight at Muhimbili National Hospital, Tanzania: A Case-Control Study. BMC Oral Health 2007, 7, 1. [Google Scholar] [CrossRef]
- Uwambaye, P.; Munyanshongore, C.; Rulisa, S.; Shiau, H.; Nuhu, A.; Kerr, M.S. Assessing the Association between Periodontitis and Premature Birth: A Case-Control Study. BMC Pregnancy Childbirth 2021, 21, 1. [Google Scholar] [CrossRef]
- Cissé, D.F.; Diouf, M.; Faye, A.; Diadhiou, M.; Tal-Dia, A. Periodontal Disease of Pregnant Women and Low Weight Newborn in Senegal: A Case-Control Study. Open J. Epidemiol. 2015, 5, 1–8. [Google Scholar] [CrossRef]
- Wanjohi, R. Preterm Low Birth Weight and Maternal Periodontal Status among Mothers Attending Puwani Maternity Hospital Nairobi, Kenya. Master’s Thesis, University of Nairobi, Nairobi, Kenya, 2020. [Google Scholar]
- Wandera, M.; Åstrøm, A.N.; Okullo, I.; Tumwine, J.K. Determinants of Periodontal Health in Pregnant Women and Association with Infants’ Anthropometric Status: A Prospective Cohort Study from Eastern Uganda. BMC Pregnancy Childbirth 2012, 12, 1. [Google Scholar] [CrossRef] [PubMed]
- Pockpa, Z.A.D.; Soueidan, A.; Koffi-Coulibaly, N.T.; Mobio, G.S.; Pere, M.; Badran, Z.; Struillou, X. Association between periodontitis and preterm birth in a cohort of pregnant women in Ivory Coast. Oral Health Prev. Dent. 2022, 20, 363–368. [Google Scholar] [CrossRef] [PubMed]
- Soroye, M.O.; Ayanbadejo, P.O.; Savage, K.O.; Oluwole, A.A. Association between Periodontal Disease and Pregnancy Outcomes. Trop. Dent. J. 2015, 38, 5–16. [Google Scholar]
- Umoh, A.O.; Savage, K.O.; Ojehanon, P.I. Association between Maternal Gingivitis, Low Birth Weight and Preterm Delivery. J. Med. Biomed. Res. 2013, 12, 65–75. [Google Scholar]
- Umoh, A.O.; Ojehanon, P.I.; Savage, K.O. Effect of Maternal Periodontal Status on Birth Weight. Euro J. Gen. Dent. 2013, 2, 158. [Google Scholar] [CrossRef]
- World Health Organization. Global Oral Health Status Report: Towards Universal Health Coverage for Oral Health by 2030; World Health Organization: Geneva, Switzerland, 2022; License: CC BY-NC-SA 3.0 IGO. [Google Scholar]
- World Health Organization; World Bank; United Nations Population Fund; United Nations Children’s Fund. Maternal Mortality in 2005: Estimates Developed by WHO, UNICEF, UNFPA and the World Bank; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Dhalia, N.; Patil, S.; Chaubey, K.K.; Narula, I.S. The detection of BANA micro-organisms in adult periodontitis before and after scaling and root planning by BANA-EnzymaticTM test kit: An in vivo study. J. Indian Soc. Periodontol. 2015, 19, 401–405. [Google Scholar] [CrossRef] [PubMed]
- Andrade, J.A.; Feres, M.; Figueiredo, L.C.; Salvador, S.L.; Cortelli, S.C. The ability of the BANA test to detect different levels of P. gingivalis, T. denticola, and T. forsythia. Braz. Oral Res. 2010, 24, 224–230. [Google Scholar] [CrossRef]
- Hexagon International (GB) Limited. User Instructions on BANA-Zyme. Available online: http://www.hexagonlimited.com/dental_banaz.htm (accessed on 22 September 2023).
- Broadbent, J.M.; Thomson, W.M. For debate: Problems with the DMF index pertinent to dental caries data analysis. Community Dent. Oral Epidemiol. 2005, 33, 400–409. [Google Scholar] [CrossRef]
- Uwitonze, A.M.; Uwambaye, P.; Isyagi, M.; Mumena, C.H.; Hudder, A.; Haq, A.; Nessa, K.; Razzaque, M.S. Periodontal Diseases and Adverse Pregnancy Outcomes: Is There a Role for Vitamin D? J. Steroid Biochem. Mol. Biol. 2018, 180, 65–72. [Google Scholar] [CrossRef]
- Venkatesh, K.K.; Glover, A.V.; Vladutiu, C.J.; Stamilio, D.M. Association of chorioamnionitis and its duration with adverse maternal outcomes by mode of delivery: A cohort study. BJOG 2019, 126, 719–727. [Google Scholar] [CrossRef] [PubMed]
- Perry, A.K.; Rossi, R.M.; DeFranco, E.A. Severe adverse maternal outcomes associated with chorioamnionitis. Am. J. Obstet. Gynecol. MFM 2019, 1, 100027. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Feng, W.; Li, J.; Cui, L.; Chen, Z.-L. Periodontal disease and adverse neonatal outcomes: A systematic review and meta-analysis. Front. Pediatr. 2022, 10, 799740. [Google Scholar] [CrossRef] [PubMed]
- Menon, R.; Taylor, B.D. Exploring inflammatory mediators in fetal and maternal compartments during human parturition. Obstet. Gynecol. 2019, 134, 765–773. [Google Scholar] [CrossRef] [PubMed]
- Madianos, P.N.; Bobetsis, Y.A.; Offenbacher, S. Adverse pregnancy outcomes (APOs) and periodontal disease: Pathogenic mechanisms. J. Periodontol. 2013, 84, S170–S180. [Google Scholar] [CrossRef] [PubMed]
- Reyes, L.; Phillips, P.; Wolfe, B.; Golos, T.G.; Walkenhorst, M.; Progulske-Fox, A.; Brown, M. Porphyromonas gingivalis and adverse pregnancy outcome. J. Oral Microbiol. 2017, 9, 1374153. [Google Scholar] [CrossRef] [PubMed]
- Kadhim, H.N. Dental caries among pregnant women in Basrah. Int. J. Oral. Dental Health 2022, 8, 1–5. [Google Scholar] [CrossRef]
- Song, I.S.; Han, K.; Park, Y.M.; Ryu, J.J.; Park, J.B. Type 2 diabetes as a risk factor for dental caries in Korean adults: The 2011–2012 Korean National Health and Nutrition survey. Community Dent. Health 2017, 34, 169–175. [Google Scholar]
- Alswat, K.; Mohammed, W.S.; Wahab, M.A.; Aboelil, A.A. The association between body mass index and dental caries. Cross-sectional study. J. Clin. Med. Res. 2016, 8, 147–152. [Google Scholar] [CrossRef]
- Zi, M.Y.; Longo, P.L.; Bueno-Silva, B.; Mayer, M.P. Mechanisms Involved in the Association between Periodontitis and Complications in Pregnancy. Front. Public Health 2014, 2, 290. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author/Year of Publication | Study Design | Study Population/Sample Size | Study Objective | Pregnancy Status | Oral Disease Status | Study Events |
|---|---|---|---|---|---|---|
| Turton et al., 2017/South Africa [14] | Cross-sectional | Patients attending antenatal care clinics in one hospital/443 | To test the hypothesis that BANA, a diagnostic test for periodontal diseases, can predict the risk of adverse pregnancy outcomes in mothers attending antenatal clinics | LBW: 24.6% PTB: 32.0% PTLBW: 16.0% | Periodontal disease severity Absent: 7.8% Mild: 43.5% Moderate: 18.3% Severe:10.4%. | Highly significant differences in PTB and LBW of children born of BANA-positive and BANA-negative mothers. LBW and PTB increased significantly with periodontal disease severity. |
| Harjunmaa et al., 2015/Malawi [15] | Nested cross-sectional study. | Patients attending antenatal clinics in four hospitals/1024 | To test the hypothesis that mothers who have dental caries, periapical infection, or periodontitis have associated adverse pregnancy outcomes. | PTB: 7.9% LBW:12.0% Neonatal stunting:12.0% Small head circumference:3.8% | Caries: 63.1% Pulpal exposure:27.8% Periapical infection:23.5%; Periodontitis: 31.9% | Periapical infection was associated with PTB, LBW, neonatal stunting, and smaller head circumference. Caries and pulpal exposure had no association. |
| Mumghamba and Manji, 2007/Tanzania [20] | Case-control | Postpartum mothers attending one national hospital/373 | To examine the relationship between oral disease status (periodontal disease and carious pulpal exposure) and preterm low-birth-weight infant deliveries | PTLBW: 150 cases TNBW: 223 cases | PTLBW vs. TNBW Gingival bleeding on gentle probing (37.3% vs. 36.3%) Gingival recession (42.7% vs. 36.3%) Periodontal pocket 4 + mm (28.7% vs. 30.0%) Periodontal pocket 6 + mm (3.3% vs. 2.7%) Severity of periodontal disease (0.13 vs. 0.11) Carious pulpal exposure (18.7% vs. 19.7%) | No association between oral parameters and PTLBW. |
| Gesase et al., 2018/Tanzania [16] | Cross-sectional | Pregnant women at the labor ward of one university hospital/1117 | To determine the relationship between periodontal disease and adverse pregnancy outcomes | pPROM: 9.0% Preeclampsia:9.9% Eclampsia: 1.4% PTB: 9.8%, LBW: 11.0%, Overweight: 4.7%, | Periodontal disease: 14.2% | Periodontal disease was significantly associated with preeclampsia, PTB, and LBW but not with pPROM, eclampsia, and overweight. |
| Uwambaye et al., 2021/Rwanda [21] | Case control | Postpartum women with singleton delivery at multiple hospitals/555 | To assess the association between periodontitis and premature birth. | PTB: 185 cases TNBW: 370 cases | Cases vs. control Periodontitis (83.2% vs. 8.1%) | Women with periodontitis had a six-fold higher risk of PTB than women without periodontitis. |
| Soroye et al., 2015/Nigeria [26] | Clinical trial S&P + root planning +OHI before delivery (intervention) vs. S&P + root planning +OHI after delivery (control 1) vs. no periodontal disease (control 2) | Pregnant women attending antenatal clinic at a university hospital/423 | To evaluate the association between periodontal disease and pregnancy outcomes like preterm birth and low birth weight | PTB: 12.5% LBW: 12.1% Spontaneous abortion: 1.4%. | Intervention vs. control 1 vs. control 2 Oral hygiene (0.86 vs. 2.62 vs. 2.34) Pockets (1.3% vs. 5.5% vs. 0.0%) Periodontal status measured by CPI score 3 (9.2% vs. 32.6% vs. 0.0%) | PTB was significantly higher among mothers in control group 1 (31.2%) than those in control group 2 (5.0%) compared to the intervention group (1.4%). LBW was significantly higher among mothers in control group 1 (28.4%) compared to those in control group 2 (7.8%) than those in the intervention group (0%). |
| Turton and Africa, 2017/South Africa [17] | Cross-sectional | Pregnant women attending antenatal clinics/443 | To investigate the relationship between oral disease status and the adverse pregnancy outcomes of mothers | TNBW: 68.0% PTB: 32.0% LBW: 75.5% in | Clinical attachment loss: 1.7 mm Severe periodontal disease: 10.1% DMFT: 7.2 Plaque index: 2.2 Gingival index: 2.4 | Periodontal disease severity was significantly associated with PTB and LBW. The Gingival index was significantly associated with LBW. DMFT and Plaque index were not associated with pregnancy events. |
| Umoh et al., 2013/Nigeria [27] | Clinical trial S&P done before delivery (test group) vs. S&P done after delivery (control group) | Primigravida women, singleton, and spontaneous vaginal delivery at a university hospital/288 | To determine the association between maternal gingivitis and adverse pregnancy outcome. | PTB: 11.8% LBW: 12.3% | Test group vs. control Gingival bleeding at 12 weeks intrapartum test group 63.3%; control group 43.1%; Gingival bleeding at 28 weeks intrapartum test group 29.1%. | Gingival bleeding was not associated with PTB. The test group with reduced gingival bleeding did not have LBW. All LBWs were from the control. |
| Umoh et al., 2021/Nigeria [28] | Clinical trial S&P done before delivery (test) vs. S&P done after delivery (control) | Primigravida women, singleton, and spontaneous vaginal delivery at a university hospital/288 | To evaluate the effect of maternal periodontal disease on the birth weight of babies and the effect of intervention during periodontal disease on the birth weight of babies | LBW: 6.2% | Test group vs. control CPI grade (2.2% vs. 7.6% at 28 weeks) | Significantly lower number of LBWs in the test group |
| Miranda- Ruis et al., 2021/Tanzania [18] | Laboratory study | Placentae collected from postpartum women with singleton pregnancy at a hospital/36 | To relate microbial profiles in human placentae with the risk of adverse pregnancy outcomes and maternal periodontal disease status | Microbial composition of the placenta using 16 S rRNA metagenomicsHistologic assessment for chorioamnionitis: 27.8% | Periodontitis: 10 cases | Chorioamnionitis was more frequent in the placentae of mothers with periodontitis but the difference was not significant. |
| Muwazi et al., 2014/Uganda [19] | Cross-sectional | Postpartum women with singletons who delivered in two hospitals/400 | To assess the association between periodontal diseases in postpartum mothers and the incidence of PTB and LBW. | PTB:48.5% LBW:8.7% pPROM: 3.8% Vaginal bleeding:3% Features of chorioamnionitis | Gingivitis: 26% Periodontal pockets ≥ 4 mm:33%; Calculus and plaque:86.0%Gingival recession: 9% | - Gingival recession was significantly correlated and associated with LBW. - Probing pocket depth, bleeding on probing, and calculus with plaque deposits were not associated with LBW. - Other periodontal indices were not associated with PTB. Features of chorioamnionitis were significantly correlated and associated with LBW and PTB. |
| Wandera et al., 2012/Uganda [24] | Clinical trial | Multi-center community recruitment of women at seven months of gestational age/877 | To study the connection between periodontal issues at seven months of pregnancy and the anthropometric measurements of the infants | Wasting: 2.0%, Stunting: 10.0%, Underweight: 6.9% | CPI ≥ 1 = 67.0% Fair to poor oral hygiene:12.1% Severe periodontal symptoms: 65.4% | CPI ≥ 1 was significantly associated with stunting and wasting. Oral hygiene scores >1.2 are significantly associated with stunting. |
| Cisse et al., 2015/Senagal [22] | Case-control | Postpartum women at a “kangaroo unit” hospital with babies with LBW/378 | To study the connection between women’s periodontal disease during their pregnancy and the weight of newborn infants. | LBW: 126 cases Control: 252 cases | Case vs. control Periodontitis (70% vs. 33%)Gingival index | Periodontitis and Gingival index were significantly associated with increased odds of LBW. The plaque index was not significantly associated with LBW. |
| Wanjohi 2020/Uganda [23] | Case-control | Postpartum women who delivered singleton via spontaneous vaginal delivery at a hospital/235 | To determine whether there is an association between maternal periodontal disease and PTLBW. | PTLBW: 61 cases Control: 174 cases | Case vs. control Periodontitis (19.7% vs.27.0%) Gingivitis (59.0% vs. 71.8%) | Gingivitis and periodontitis were not associated with PTLBW |
| Pockpa et al., 2022/Ivory Coast [25] | Cohort | Pregnant women attending antenatal care at a university hospital/338. | To determine the association between maternal periodontitis and PTB. | PTB 18.3% | Prevalence of Periodontitis 59.4% Stage I: 41.4%; Stage II: 11.2%; Stage III/IV: 6.8% | PTB was significantly higher among pregnant women with periodontitis. Periodontitis is a risk factor for PTB. |
| Adverse Pregnancy Events | Gingivitis | Moderate and Severe Periodontal Disease | Probing Pocket Depth | Calculus | Gingival Recession | CAL | Periapical Infections | Caries | Pulpal Exposure | Oral Hygiene Status |
|---|---|---|---|---|---|---|---|---|---|---|
| LBW | X | X/- | X | X | X | X | - | |||
| PTB | - | X/- | X | - | - | X | X | - | ||
| PTLBW | - | X/- | - | - | ||||||
| Neonatal stunting | X | X | - | X | ||||||
| Wasting | X | |||||||||
| Underweight | X | |||||||||
| Overweight | ||||||||||
| Small head circumference | X | - | ||||||||
| pPROM | ||||||||||
| Preeclampsia | X | |||||||||
| Eclampsia | ||||||||||
| Spontaneous abortion | ||||||||||
| Vaginal bleeding | ||||||||||
| Chorioamnionitis | X | X |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adebayo, E.T.; Abodunrin, O.R.; Adewole, I.E.; Salako, A.O.; Lusher, J.; Akinsolu, F.T.; El Tantawi, M.; Alade, O.T.; Eleje, G.U.; Ezechi, O.C.; et al. Oral Diseases and Adverse Pregnancy Outcomes in Sub-Saharan Africa: A Scoping Review. BioMed 2024, 4, 1-18. https://0-doi-org.brum.beds.ac.uk/10.3390/biomed4010001
Adebayo ET, Abodunrin OR, Adewole IE, Salako AO, Lusher J, Akinsolu FT, El Tantawi M, Alade OT, Eleje GU, Ezechi OC, et al. Oral Diseases and Adverse Pregnancy Outcomes in Sub-Saharan Africa: A Scoping Review. BioMed. 2024; 4(1):1-18. https://0-doi-org.brum.beds.ac.uk/10.3390/biomed4010001
Chicago/Turabian StyleAdebayo, Ezekiel Taiwo, Olunike Rebecca Abodunrin, Ifeoluwa E. Adewole, Abideen Olurotimi Salako, Joanne Lusher, Folahanmi Tomiwa Akinsolu, Maha El Tantawi, Omolola Titilayo Alade, George Uchenna Eleje, Oliver Chukwujekwu Ezechi, and et al. 2024. "Oral Diseases and Adverse Pregnancy Outcomes in Sub-Saharan Africa: A Scoping Review" BioMed 4, no. 1: 1-18. https://0-doi-org.brum.beds.ac.uk/10.3390/biomed4010001